Alan Jenks
In your career as a health practitioner, it is very likely that one day you will encounter someone who tells you they are ‘short of breath’. This very ambiguous statement will set off alarm bells in your head as your mind races to find the appropriate follow up questions. Is it difficult to inhale? To exhale? Is the force of inhalation or exhalation compromised? Given the long list of things that can cause shortness of breath, you may decide to test this patient’s lung function to rule out some common pulmonary disorders and move forward with treatment.
Or, perhaps you are working in an exercise metabolism lab and want to test the impact of a common bronchodilatory drug on exercise capacity in people with asthma. In both of these scenarios you have the opportunity to employ pulmonary function tests. These tests, especially spirometry, play important roles in screening and diagnosing patients with respiratory disorders and are very popular in the exercise science world as a research modality.
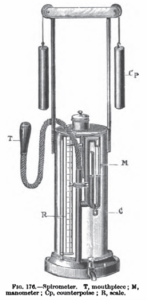
A surgeon named John Hutchinson invented spirometry in 1846, but prior to this, in 1813 E. Kentish used a ‘pulmometer’ to study the effect of diseases on pulmonary lung volume. Both Kentish and Hutchinson realized if a bell-shaped jar was inverted in water, it could be used to capture the volume of exhaled air by a person. From there, Hutchinson described a direct relationship between vital capacity (the maximum amount of air a person can exhale after a maximal inhale) and height, and an indirect relationship between vital capacity and age. Hutchinson also used the machine to predict premature mortality, and we still use vital capacity today as an important measure of pulmonary and cardiovascular health.
Gas exchange occurs between the air and the blood in the alveolar sacs. The efficiency of gas exchange is dependant on ventilation, that is, the cyclical breathing movements that alternately inflate and deflate the alveolar sacs. Many important aspects of lung function can be determined by measuring airflow and in the past, this was done using a bell spirometer very similar to Hutchinson’s (in fact some university labs still have bell spirometers!).
In today’s lab we will be using a pneumotachometer with an attached spirometer to test the breathing of a participant. Modern spirometry allows for many components of pulmonary function to be visualized, not just vital capacity (VC). During the respiratory cycle (inhale to exhale) a specific volume of air is drawn into the lungs and then expired out.
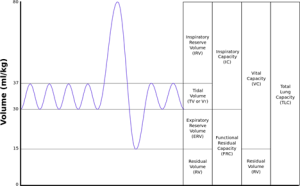 This is called Tidal Volume (VT). When tidal volume is multiplied by the frequency of breathing (normal is around 15 breaths per minute) the product is the Expired Minute Volume (VE), or amount of air expired in one minute. IRV and ERV are the inhaled and exhaled reserve volume (respectively). Each of these are the amount that can be maximally inhaled or exhaled after a normal inhale or exhale. Functional residual capacity (FRC) is the volume in the lungs after a normal exhale and RV, residual volume, is the amount of air that stays in the lungs even after maximal exhalation. Recall this is required to keep the lungs inflated and aid in pressure differentials that allow air to be drawn into the lungs at inhalation.
This is called Tidal Volume (VT). When tidal volume is multiplied by the frequency of breathing (normal is around 15 breaths per minute) the product is the Expired Minute Volume (VE), or amount of air expired in one minute. IRV and ERV are the inhaled and exhaled reserve volume (respectively). Each of these are the amount that can be maximally inhaled or exhaled after a normal inhale or exhale. Functional residual capacity (FRC) is the volume in the lungs after a normal exhale and RV, residual volume, is the amount of air that stays in the lungs even after maximal exhalation. Recall this is required to keep the lungs inflated and aid in pressure differentials that allow air to be drawn into the lungs at inhalation.
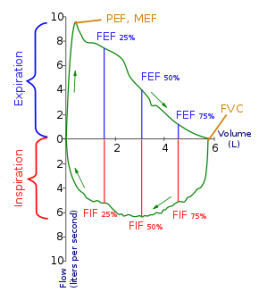
With spirometry, sometimes breathing will be displayed with a Flow-Volume Loop rather than a volume vs. time pulmonary function graph as above. The Flow-Volume loop plots inspiratory and expiratory air flow against volume during maximally forced inspiratory and expiratory maneuvers. Many clinicians and scientists prefer this way of displaying data collected as the shape, size and ‘shift’ of the loop all give indication of pulmonary functioning of the patient.
Restrictive lung disease refers to a group of lung diseases that prevent the lungs from fully filling with air. As you can imagine this makes breathing difficult and, in some cases, can be fatal. Examples of restrictive lung diseases include pulmonary fibrosis, pneumoconiosis, and muscular dystrophy. In today’s lab you will mimic a restrictive lung disease by tightly binding the thoracic region of the torso such that the ribcage cannot expand fully.
Tidal Volume: (TV, 500 ml in both male and female). The amount of air inspired or expired during a single, quiet breath.
Inspiratory Reserve Volume: (IRV, 3,300 ml in male, 1,900 in female). The amount of air that can be forcibly inspired above a normal inspiration.
Expiratory Reserve Volume: (ERV, 1,000 ml in male, 700 in female). The amount of air that can be forcibly exhaled after a normal exhalation.
Residual Volume: (RV, 1,200 ml in male, 1,100 ml in female). The amount of air that remains trapped in the lungs after a maximal exhalation effort. Surfactant produced by the alveoli prevents the alveoli from collapsing completely during exhalation. Since the alveoli are not allowed to completely empty, they always maintain a resident volume of air.
In addition to the four volumes, there are four capacities, which are combinations of two or more volumes.
Total Lung Capacity: (TLC, 6,000 ml in male, 4,200 ml in female). The total amount of air the lungs can contain. TLC = IRV + TV + ERV + RV.
Vital Capacity: (VC, 4,800 ml in male, 3,100 ml in female). The maximal amount of air that can be forcefully expired after a maximal inspiration. VC = IRV + TV + ERV
Functional Residual Capacity: (FRC, 2,200 ml in male, 1,800 ml in female). The amount of air remaining in the lungs after a normal expiration. FRC = ERV + RV
Inspiratory Capacity: (IC, 3,800 ml in male, 2,400 ml in female). The maximal amount of air that can be inspired after a normal expiration. IC = TV + IRV
The values given above for respiratory volumes and capacities are for normal adults. The values for female are 20%-25% smaller than that in male. Why? A person’s size, age, and physical condition also produce variations in respiratory volumes and capacities.
Respiratory volumes and capacities are generally measured in the clinical assessment of a variety of pulmonary disorders. In general, chronic pulmonary diseases may be classified into two physiologic categories: (1) obstructive pulmonary disorder, such as emphysema and bronchial asthma, and (2) restrictive disorders, such as pulmonary fibrosis. Both obstructive and restrictive pulmonary diseases often coexist (e.g., combined pulmonary emphysema and fibrosis).
In restrictive pulmonary diseases, lung capacities and volumes are general reduced (e.g., decreased VC). For example, in silicosis (grinder’s disease), a disorder caused by chronic inhalation of stone dust, sand, or flint, the lungs lose dispensability and become stiff. Restrictive pulmonary diseases may be diagnosed by determining the respiratory volumes and capacities.
In obstructive pulmonary diseases, pulmonary air-flow is generally reduced. In a chronic obstructive pulmonary disease (COPD) such as bronchial asthma, excessive mucous secretion partially blocks airways, increasing airway resistance and thus making breathing more difficult. This results in reduction in the volume of air flowing per minute into and out of the lungs. The asthmatic may take longer to inspire and expire, but respiratory volumes may be normal or near normal. Therefore, measurements of respiratory volumes and capacities tell nothing about the ability to more air in and out of the lungs, a critical factor in the delivery of oxygen to the blood.
Forced Expiratory Volume (FEV), is a test in which a limit is placed on the length of time a subject has to expel VC air. Normal adults are able, with maximal effort, to expire about 83% of their VC in one second (FEV1.0 = 83% of VC in one second), 94% of their VC in the 2nd second (FEV2.0 = 94% of VC in 2nd second), and 97% of their VC by the end of the 3rd second (FEV3.0 = 97% of VC in 3rd second).
Media Attributions
- Picture3
