196
Zoë Soon
Learning Objectives
By the end of this section, you will be able to:
- List and locate the anatomical structures associated with the immune system and lymphatic system.
- Describe the main functions of each structure (lymph capillaries, lymph vessels, lymph nodes, bone marrow, spleen, thymus, tonsils, BALT, and MALT) in terms of how it contributes to the immune system.
The immune system is vitally important in maintaining the health of an individual. The major tissues and organs of the immune system are involved in producing cells and chemicals that are capable of destroying pathogens and neutralizing toxins that would otherwise contribute to tissue damage or destruction. This section will focus on the biological components of the immune system, which is closely associated with the lymphatic system. The lymphatic system provides key structural components that are used by the immune system to defend the body (OpenStax Figure 21.2).
One may recall that the lymphatic system consists of lymphatic vessels (that transport lymph fluid), as well as lymph tissues (tonsils, Bronchus Associated Lymphoid Tissue, BALT and Mucosa Associated Lymphoid Tissue, MALT) and lymph organs (bone marrow, thymus, lymph nodes and spleen), which house lymphocytes (immune system cells) as well as other important cells and extracellular proteins that provide structure and function. Most lymph organs have capsules made of fibrous connective tissue (e.g. lymph nodes, thymus, and spleen). Lymph Tissues (e.g. tonsils and MALT) tend to be aggregates or clusters of lymphocytes within other organs or structures. GALT (Gut-Associated Lymphoid Tissue) and Peyer’s patches are components of MALT which helps to protect the intestines from pathogens.
Figure 21.2 Anatomy of the Lymphatic System Lymphatic vessels in the arms and legs convey lymph to the larger lymphatic vessels in the torso (OpenStax).
Lymph vessels are a pale golden colour and penetrate most tissues of the body intertwining with the capillaries therein. Their structure and role is quite different than blood vessels though, in that lymphatic vessels begin with blind-ends (or closed ends) and serve to recapture interstitial fluid (within the interstitial spaces) that is continuously leaked from capillaries (Figure 21.3). In total, approximately 3-4L is collected per day. To readily perform this function, the endothelial cells of a lymphatic capillary are not bound tightly and overlap, acting as one-way valves which permit the entrance only of fluid, solutes, proteins, viruses, bacteria, and cell debris. Once absorbed through these flap-like valves in the blind-ends of lymphatic capillaries, this fluid, now termed lymph fluid is strategically transported through lymph nodes before finally arriving at either the right or left subclavian vein into which the fluid is returned to the bloodstream.
Figure 21.3 Lymphatic Capillaries Lymphatic capillaries are interlaced with the arterioles and venules of the cardiovascular system. Collagen fibers anchor a lymphatic capillary in the tissue (inset). Interstitial fluid slips through spaces between the overlapping endothelial cells that compose the lymphatic capillary (OpenStax). The walls of lymph vessels are similar to veins in that there are 3 tunics, an inner endothelial layer, a middle smooth muscle layer, and an outer layer of connective tissue. However the basement membrane is incomplete and the endothelial cells are arranged as flap-valves. The smooth muscle layer is innervated and consists of an inner circular layer and an outer longitudinal layer of smooth muscle cells. The luminal diameter of lymphatic capillaries is larger than blood capillaries and their walls are thinner. Lymphatic capillaries have a lower hydrostatic pressure and higher osmotic pressure than blood capillaries.
Areas of the body that do not include lymphatic vessels include: the central nervous system, teeth, cornea and bone marrow. It is important to note that lymph is not pumped, as is blood by the heart, but is moved through lymphatic capillaries, into larger-diameter lymph vessels, through lymph nodes, and finally into lymphatic ducts through peristalsis. The rhythmic contraction of the smooth muscle lining of lymphatic vessels achieves this peristalsis which is particularly necessary as lymph is moved upwards against gravity. The flow rate is approximately 4-5mm/second. Compression of neighbouring skeletal muscle around lymph vessels also assists in the movement of lymph, as does the process of breathing which continuously introduces periods of lower thoracic pressure during inspiration that facilitate the upward movement of lymph through this region. This phenomenon of regular pressure changes within the thorax is often called the respiratory pump. Additionally, semi-lunar valves are strategically located along the length of lymphatic vessels which prevent back-flow. Lymph fluid from the right half of the thorax, right arm and right side of the head and neck are carried through lymph vessels that merge into the right lymphatic duct which drains into the right subclavian vein. Lymphatic vessels from the rest of the body eventually merge into the thoracic duct which drains into the left subclavian vein (Fig. 21.4).
Figure 21.4 Major Trunks and Ducts of the Lymphatic System The thoracic duct drains a much larger portion of the body than does the right lymphatic duct (OpenStax).
Lymph nodes are small bean-shaped organs that house immune cells, specifically B and T lymphocytes, in large quantity which function to screen this lymph fluid making sure to destroy any pathogens, neutralize any toxins, and launch a full immune response if required in order to protect the body. There are 500-600 lymph nodes in the body and there are clusters of lymph nodes in the groin (Inguinal Lymph Nodes), armpits (Axillary Lymph Nodes), neck (Cervical Lymph Nodes), chest, and surrounding the intestines. The 3 largest collection of lymph nodes are the Inguinal, Axillary, and Cervical. Lymph nodes can become swollen during infection as they trap incoming lymph while pathogens are destroyed.
Primary Lymphoid Organs
Both bone marrow and the thymus are considered to be primary lymphoid organs as they are the primary sites of B and T lymphocyte maturation, proliferation and clonal selection (Fig. 21.6). B and T lymphocytes become immunocompetent (capable of mounting an immune response in these two primary lymphoid organs.
Of the three types of lymphocytes (Natural Killer cells, B cell and T cells), all 3 originate in the bone marrow and are daughter cells of hematopoietic stem cells. Natural Killer (NK) cells and B lymphocytes (B cells) complete nearly all of their maturation within bone marrow. While some NK cells stay to complete differentiation within the bone marrow, other NK cells migrate to other lymphatic tissues and organs including the lymph nodes, the spleen, thymus, and tonsils before fully maturing and entering circulation.
B lymphocytes leave the bone marrow as transitional B cells and migrate to the spleen where they fully mature and become naïve B cells. These naive B cells can either remain in the spleen or travel to other secondary lymphoid organs (e.g. lymph nodes) and lymphoid tissues (e.g. tonsils and MALT). B cells will remain in this naïve state until they become sensitized through direct interactions with foreign antigens and activated Helper T lymphocytes (Helper T cells also known as CD4 cells).
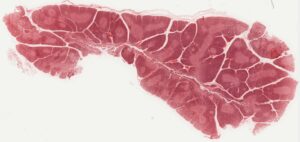
Figure 21.6 Bone Marrow Red bone marrow fills the head of the femur, and a spot of yellow bone marrow is visible in the center. The white reference bar is 1 cm (OpenStax).
Immature T lymphocytes (T cells) leave the bone marrow migrate to the thymus and the exposure to thymosin facilitates their maturation into naïve T cells. The thymus gland has two lobes and is located between the aorta and the sternum (Fig. 21.7). At first
Aging and the Immune System
The loss of immune function with age is called immunosenescence. To treat the growing aging populations in Canada and the USA, medical professionals must better understand the aging process. One major cause of age-related immune deficiencies is thymic involution, the shrinking of the thymus gland that begins at birth, at a rate of about three percent tissue loss per year, and continues until 35–45 years of age, when the rate declines to about one percent loss per year for the rest of one’s life. At that pace, the total loss of thymic epithelial tissue and thymocytes would occur at about 120 years of age. Thus, this age is a theoretical limit to a healthy human lifespan.
Thymic involution has been observed in all vertebrate species that have a thymus gland. Animal studies have shown that transplanted thymic grafts between inbred strains of mice involuted according to the age of the donor and not of the recipient, implying the process is genetically programmed. There is evidence that the thymic microenvironment, so vital to the development of naïve T cells, loses thymic epithelial cells according to the decreasing expression of the FOXN1 gene with age.
It is also known that thymic involution can be altered by hormone levels. Sex hormones such as estrogen and testosterone enhance involution, and the hormonal changes during pregnancy cause a temporary thymic involution that reverses itself, when the size of the thymus and its hormone levels return to normal, usually after lactation ceases.
What does all this tell us? Can we reverse immunosenescence, or at least slow it down? The potential is there for using thymic transplants from younger donors to keep thymic output of naïve T cells high. Gene therapies that target gene expression are also seen as future possibilities. The more we learn through immunosenescence research, the more opportunities there will be to develop therapies, even though these therapies will likely take decades to develop. The ultimate goal is for everyone to live and be healthy longer, but there may be limits to immortality imposed by our genes and hormones (OpenStax).

Figure 21.10 Locations and Histology of the Tonsils (a) The pharyngeal tonsil is located on the roof of the posterior superior wall of the nasopharynx. The palatine tonsils lay on each side of the pharynx. (b) A micrograph shows the palatine tonsil tissue. LM × 40. (Micrograph provided by the Regents of the University of Michigan Medical School © 2012) (OpenStax)
Mucosa-associated lymphoid tissue (MALT) is composed of lymphoid follicles overlaid with mucosal epithelial cells and is found in the gastrointestinal tract, breast tissue, lungs, and eyes. Peyer’s patches are located in the small intestinal walls and contain specialized endothelial M (microfold) cells that sample material from the lumen and transport it to nearby lymphoid follicles which are capable of launching specific (adaptive) immune responses. Similar processes have been found to occur in the MALT of the appendix.
Figure 21.11 Mucosa-associated Lymphoid Tissue (MALT) Nodule LM × 40. (Micrograph provided by the Regents of the University of Michigan Medical School © 2012) (OpenStax)
Bronchus-associated lymphoid tissue (BALT) is composed of lymphoid follicles overlaid with epithelial cells and is found along the bifurcations of the bronchi, and between bronchi and arteries. BALT provides protection against inhaled pathogens.
Pre/Post-Test Questions:
- What would happen if the lymphatic vessels are damaged or scarred?
A. Lymphatic vessels can be damaged as a result of trauma or inadvertently removed/disrupted during surgical procedures. When this occurs the vessels can become severed or scarred resulting in either partial or full occlusion. As such interstitial fluid is no longer drained appropriately and can accumulate leading to regional swelling known as lymphedema.
Adaption
The figures, figure captions, and Aging in the Immune System textbox in this chapter are adapted from the following text:
Anatomy of the Lymphatic and Immune Systems in Anatomy and Physiology by OSCRiceUniversity is licensed under a Creative Commons Attribution 4.0 International License
