Acute Care and the HCA Program
This section outlines key information on acute care for instructors to share with students. It has been updated to align with the language changes reflected in the 2023 HCA Program Provincial Curriculum.
The acute care content was originally added to the Health Care Assistant Provincial Curriculum Guide in 2015. The accompanying HCA Supplement provided an instructor guide to support faculty in incorporating the acute care content into the HCA program courses. This guide was based on materials developed by Island Health. Instructors were encouraged to adapt and integrate the content into their instructional activities, such as PowerPoint slides, student handouts, course manuals, and lab practice scenarios.
In 2023, the HCA Provincial Program Provincial Curriculum was updated to include the option of sending students to units such as acute care, transitional care, discharge planning, rehabilitation, and alternate levels of care. These clinical experiences are acceptable, provided the program learning outcomes can be met in these settings, and the placements do not replace the minimum 150 hours of instructor-led clinical required in complex care.
Note: This section is adapted from Island Health. (2012). Transitional Learning Continuum, Health Care Assistant in Acute Care Curriculum with permission from the Island Health Authority, B.C. Health Education Foundation, and the Ministry of Health Services.
1. Supervision Structures in Acute Care
Course: Introduction to Practice
Estimated time: 30 minutes
- Every health authority and unit has an organizational structure that outlines the supervision and reporting structure.
- Within a unit structure, there are members of the health care team that will guide the role of the HCA. This includes the team members the HCA will report to when supporting client care and unit operations. These team members may include, but are not limited to, Registered Nurses (RNs), Licensed Practical Nurses (LPNs), Registered Psychiatric Nurses (RPNs), Clinical Nurse Leads (CNLs) and Unit Managers.
- Supervisors can help determine which team members HCAs will regularly work with.
- Depending on who assigns tasks or delegates restricted activities, different team members need to establish supervision plans for the care activities that HCAs will support.
- Communication is essential when reporting to and collaborating with other health care team members.
- As an HCA, there will be times when different types of questions and concerns should be brought to different members of the health care team. HCAs can also talk to their unit supervisors/leaders for guidance.
2. Characteristics of Clients in Acute Care
Course: Common Health Challenges
Estimated time: 1 hour 30 minutes
- In most instances, acute care settings will be very different from complex and home or community care settings. The pace of activities and the variety of sights, sounds, and smells can be overwhelming for a new HCA. However, similar to a beehive, the activity is purposeful and coordinated. All interprofessional team members work collaboratively in a variety of different ways to meet diverse client and family care needs every day.
- As HCAs become acquainted with the acute care setting, they will start to notice that, in many instances, acute care and complex care settings will share the same clients along their health and wellness journey. Many of these clients will be elderly clients who have been admitted into acute care units for some type of medical intervention, such as surgery, or clients who have a chronic condition that requires symptom control or readjustment. The care needs of these types of clients will be very familiar to HCAs who have practised in other settings. In these instances, HCAs can offer significant support to these clients, families, and other members of the health care team.
- There are some important considerations for HCAs to keep in mind when working in an acute care setting.
- HCAs will never be working independently. Instead, HCAs will draw upon the knowledge, skills, and resources of a variety of interprofessional care team members who will work collaboratively with them in caring for each client.
- As a member of the interprofessional care team, HCAs also bring with them a wealth of knowledge and skills in caring for elderly clients. These skills and knowledge in caring for elderly clients add strength to the interprofessional team and can contribute to the care planning process.
- Acute care is an intricate and diverse working environment. HCAs have many skills that contribute to providing quality care in this setting but may not be familiar with some of the unique aspects of the acute care environment.
- Clients may be admitted to acute care in the following circumstances. If the client:
- Has had a stroke or a heart attack
- Has acute congestive heart failure
- Has uncontrolled pain
- Requires surgical intervention
- Is frail, elderly, and has a fractured hip
- Has a crisis in their caregiving supports
- Most clients in acute care will have different medical needs than those in complex or community settings. For example, they may:
- Have had recent surgery
- Have lines and tubes
- Have new incisions, wounds, or dressings
- Be experiencing acute mental health issues
- Be admitted for alcohol and drug detoxification
- Be acutely palliative
3. Elements of the Acute Care Environment
Courses: Common Health Challenges and Personal Care and Assistance
Estimated time: covered in 2 and 5
Examples of environmental aspects more often encountered in the acute care setting may include:
- Additional forms of documentation, or documentation that the HCA will access more often than they might in other settings
- Increased technology, such as various pumps, monitors, etc.
- Positive/negative pressure rooms for isolation
- Call bell systems
4. HCA Role in Acute Care Settings
Courses: Common Health Challenges, Introduction to Practice, and Concepts for Practice
Estimated time: 1 hour for Common Health Challenges, 15 minutes in Introduction to Practice, and 30 minutes in Concepts for Practice (recording/reporting)
The HCA roles in acute care settings depend on client acuity, intensity, and complexity. When assigning care activities, the health care professional considers such factors as client stability and the probability of an adverse event. HCAs are generally assigned care activities where the impact and probability of an adverse event are lower.
- “Acuity” refers to the level of care a client requires based on the severity of their condition or symptoms. High acuity clients are those who experience an event that is characterized by having a sudden onset, a sharp rise, having severe symptoms, and lasting a short time. Examples of clients with high acuity needs are those with:
- Respiratory distress (using high flow oxygen)
- Active gastrointestinal bleeding
- Unstable vital signs
- Low acuity clients are those who have become more stable in their health concerns, the prescribed medical treatment is working, and they are demonstrating improvements in their health status. Examples of clients with low acuity care needs are those:
- Who are progressing as expected three days after an operation
- With pneumonia, requiring IV antibiotics
- With influenza (the flu)
- With C. difficile
- “Intensity” refers to the volume of work that may be required from the health care team to meet the care needs of a particular client. Examples of clients with high-intensity and complicated care needs are those who require:
- Complete ADL support, total care client
- Care of more than one health care team member (e.g., mechanical lifts, bariatric clients)
- Complex wound management (e.g., Vacuum-Assisted Closure (VAC) dressings, ulcers, infected surgical wounds)
- Support to manage complex family dynamics
- Examples of clients with low-intensity/complex care needs are those who require:
- Minimal ADL support for client care
- Basic meal tray set up (clients who are able to feed themselves)
- Limited support as they are stable and waiting to be discharged or transferred
- “Complexity” refers to the range of variables, such as multiple medical diagnosis or challenging family dynamics, which may influence the care needs of a particular client.
- HCAs help care for clients in the acute care setting by helping with:
- Bathing and washing
- Toileting
- Meal assistance
- Basic treatments (as identified by site-specific role and responsibilities)
- Ambulation, mobilization, and transfer of stable clients
5. IV Lines, Tubes, Wounds, and Surgical Incisions
Course: Personal Care and Assistance
Estimated time: 2 hours theory/lab
- Most clients in acute care will have medical needs that require interventions through the use of IV lines or tubes. These interventions are crucial for delivering medications, nutrients and fluids, maintaining bodily functions, and promoting healing after surgeries or injuries. To provide care to clients, HCAs must be able to safely work around and with these interventions.
- Examples of lines and tubes in acute care are:
- Intravenous (IV) lines
- Oxygen tubing
- Surgical drains
- Chest tubes
- Catheters
- Prior to interacting with the client, HCAs must:
- Observe the client carefully, looking for surgical or medical lines.
- Ask the RN/LPN if there is anything special that they need to know or do related to this client’s tubing and receive instructions about any specific approaches or care plan interventions.
- Make considerations for giving daily care, such as changing a gown.
- Seek assistance if there are any concerns or questions before proceeding with care and care-related activities.
IV Lines
Ask: What is an IV?
Answer: An IV or intravenous catheter is a small plastic cannula that is inserted in the vein with the use of a needle. After the plastic cannula is secure within the vein, the needle is removed. They are most commonly inserted in the hand or forearm but can be located in other areas such as the foot. IV catheters are used to supply a client with additional fluids or medications.
Ask: What does an HCA need to do when providing care to a client with an IV?
Answer: When providing care to a client with an IV, the HCA should:
- Never remove the IV bag from the pole it is situated on.
- Never disconnect a tube or unplug equipment from the wall without having permission from the RN to do so.
- Notify an RN if:
- They observe blood in the IV tubing or the IV site is leaking
- They accidentally dislodge the IV during care
- The client is complaining about pain in the area
- Avoid getting the dressing or insertion site wet during care
- If available, use an IV gown to dress the client (IV gowns will have snaps on the sleeves of the gown).
- Check with the RN or team leader about specific client information or instructions before mobilizing a client. Clients who are allowed to be up and walking and have an IV can generally be mobilized, but there are a few exceptions.
Oxygen Tubing
Ask: What does an HCA need to know about providing care to a client with oxygen tubing?
Explain: Clients may require oxygen therapy as either a short-term intervention (clients with pneumonia, for example) or for long-term use (such as COPD clients). How much oxygen therapy is required and what method of delivery is used will depend on the client’s condition and may change as the client improves or deteriorates. Chronic conditions, such as COPD, will require consistent oxygen therapy at all times.
Describe the different methods of delivering oxygen, such as nasal prongs or facial masks.
Ask: What does an HCA need to do when providing care to a client on oxygen?
Answer: When providing care to a client on oxygen, the HCA should:
- Never adjust the flow rate of the oxygen.
- Check with the RN or team leader about whether the client requires oxygen before and during mobilization.
- Check with the RN or LPN if they find oxygen tubing laying on the floor in rooms where there is more than one client, to ensure that the nasal prongs are replaced before being reapplied to the correct client.
- Reapply nasal prongs to a client if the prongs become dislodged during care.
- Check with the RN or team leader about specific client information before mobilizing a client.
- Clients who are ambulatory and on oxygen generally can be mobilized, but there are a few exceptions.
Surgical Drains
Ask: What is a surgical drain?
Answer: Surgical drains are external drainage systems that are used to collect and drain internal fluids after a surgical procedure.
- There are many different types of surgical drains, and HCAs must always confirm instructions with the health care team prior to providing care for clients with surgical drains.
- They are often pinned to gowns to prevent them from accidentally becoming dislodged.
- They are often covered by dressings.
Ask: What does an HCA need to do when providing care to a client with a surgical drain?
Answer: When providing care to a client with a surgical drain, the HCA should:
- Use caution when removing a client’s gown, as some drains may be pinned to the gown.
- Safely remove safety pins from the old gown and secure them to the new gown when care is complete.
- Never remove a dressing that may be oozing. HCAs may place a gauze over the site and must report it to the RN or team leader immediately.
- Avoid getting the dressing around the drain wet during care. Wash and dry around the dressing site.
- Report any pain or discomfort a client may experience during care and care-related activities.
- Read the client’s care plan and/or talk to their RN or team leader to determine if the client is allowed to sit/get up and walk if they have a surgical drain. HCAs should also have the RN or team leader check the client prior to getting out of bed to ensure the drainage system is secure.
Chest Tubes
Ask: What does an HCA need to know about providing care to a client with a chest tube?
Answer: HCAs need to know that:
- Chest tubes are used when a client’s lung cannot inflate and deflate on its own. This may be the result of an external trauma such as an accident, or as a result of a fluid buildup in the lung that has caused it to collapse.
- Chest tubes are secured with a lot of tape.
Ask: What does an HCA need to do when providing care to a client with a chest tube?
Answer: When providing care to a client with a chest tube, the HCA should:
- Avoid getting too much moisture around the chest tube dressing. Wash around the tape with a moist washcloth.
- Report any drainage that may be observed during care to the RN or team leader.
- Report any pain or discomfort a client may experience during care and care-related activities.
- Always check with the RN prior to mobilizing a client with a chest tube. Accidentally dislodging or withdrawing the chest tube may cause the client to go into respiratory distress and requires immediate medical intervention.
Catheters
Ask: What does an HCA need to know about providing care to a client with a catheter?
Answer: HCAs need to know that:
- Catheters in acute care settings are inserted as a short-term medical intervention. This may include surgical clients both pre-operatively and post-operatively to facilitate bladder drainage during surgery. Unless otherwise indicated, catheters in acute care settings should only be used for short periods of time.
- Although clients who are allowed to be up and walking and have catheters can generally be mobilized, there are a few exceptions. HCAs must check with the RN or team leader about specific client information.
Ask: What does an HCA need to do when providing care to a client with a catheter?
Answer: When providing care to a client with a catheter, the HCA should:
- Confirm instructions and gather information regarding anything that may be different in providing care for a specific client with a catheter.
- Observe the site of insertion for discharge, swelling and/or redness.
- Observe the catheter and tubing to ensure that the catheter is properly secured to the patient and that the tubing is not obstructed.
- Avoid lifting the catheter above the client’s waist level.
- Ensure that the bag and tubing are not touching the floor.
- Report any pain or discomfort a client may experience during care or care-related activities.
Surgical Incisions
In addition to lines and tubes, clients in acute care may have incisions from treatment procedures or wounds. Prior to interacting with the client, HCAs must ask the RN/LPN if there is anything special they need to know or do related to the client’s surgical incisions or wounds.
Ask: What types of surgical incisions would HCAs expect to see in acute care?
Answer: In acute care, HCAs may encounter a wide variety of incisions. Incisions are generally covered with a dressing/bandage. Common surgical incisions include:
- Abdominal incisions
- Hip or knee incisions
Ask: What does an HCA need to do when providing care to a client with a surgical incision?
Answer: When providing care to a client with a surgical incision, the HCA should:
- Confirm instructions with the RN/LPN.
- Gather information and supplies for care.
- Seek permission from the client to look at the bandage over the incision and to perform care.
- Notify an RN immediately if there is a large amount of drainage on the bandage over the incision.
- Never remove a dressing that may be oozing. HCAs may place a gauze over the site and must report it to the RN or team leader immediately.
- Avoid getting a dressing wet during care. Wash and dry around the dressing site.
- Report any pain or discomfort a client may experience during care and care-related activities.
6. Time Management, Problem-Solving, and Decision-Making in Acute Care
Courses: Concepts for Practice, Common Health Challenges, and Personal Care and Assistance
Estimated time: 1 hour for theory/lab
Although HCAs may not be assigned to specific client assignments or teams, they may be required to support specific aspects of daily care under the direction of another health care team member. This will require a level of flexibility and adaptability from the HCA to meet client care needs in the rapidly changing environment of acute care. Case studies or lab scenarios could be used to give students an opportunity to apply critical thinking and problem-solving skills to acute care settings or to compare and contrast acute care and other settings.
Ask: What does an HCA need to know to prioritize care activities when providing care in acute care settings?
Answer: When providing care in acute settings, HCAs need to know that acute care environments and client assignments can change rapidly due to:
- Client admissions and discharges
- Moving clients from one room to another
- Transferring clients from one unit to another
- Changing acuity of clients
- Clients developing infections that require special precautions
Ask: What does an HCA need to do to prioritize care activities when providing care in acute care settings?
Answer: When providing care in acute care settings, HCAs need to:
- Attend huddles/shift reports or seek information from the other members of the health care team about changing priorities throughout the day.
- Seek guidance and direction from the RN related to their responsibilities.
- Communicate clearly with the health care team to identify what care activities have or have not yet been completed.
- Anticipate that they will need to be flexible in their client care assignment based on the clients’ needs. Although they may have been given assignments, they may be reassigned during their work days due to unforeseen circumstances.
7. Interprofessional Collaborative Practice in Acute Care Settings
Course: Introduction to Practice
Estimated time: Not applicable, as already covered in program
Interprofessional collaborative practice is important because it meets the following needs in providing client care:
- Improving client outcomes, care, and services
- Reducing medical error
- Ensuring knowledge transfer and communication between and to relevant professionals
- Informing government policy and leadership at all levels
- Addressing health and human resource shortages
Describe when teams work interprofessionally:
- Decision-making is shared
- Leadership is shared
- The role of each health care provider is understood, and the client and family are included in the process
- Team communication is efficient, open, respectful, and client-centred, in which the client and family are integrated into the care process
Highlight the outcomes of interprofessional collaboration. Clients and families have:
- Expressed more satisfaction and identified a more positive experience
- Enhanced self-care and health condition knowledge and skills
- Improved health outcomes
- More timely referrals to other team members
- More comprehensive care
Health care providers:
- Are more satisfied and have a more positive experience
- Develop enhanced knowledge and skills
- Experience improved communication between providers
- Can offer a broader range of services and more efficient use of resources
- Provides improved access to services and shorter wait times
Reference
Barrett, J., Curran, V., Glynn, L., & Godwin, M. (2007). CHSRF synthesis: interprofessional collaboration and quality primary healthcare. Canadian Health Services Research Foundation.
8. Communication in Acute Care Settings
Courses: Interpersonal Communications and Introduction to Practice
Estimated time: 30 minutes
Communication processes within acute care settings require the full and active participation of all interprofessional team members. It is important to consider the urgency for information (how quickly something is needed) as well as the frequency required of communication (how regularly information is needed). Critical decisions regarding such factors as hospital admissions and discharges, client care routines, diagnostic assessments, medical treatments, and access to supplies depend on clear and timely communication between team members.
Communication principles in acute care for HCAs:
- Who to communicate with: know the interprofessional team that is involved in client care
- What to communicate: the methods of gathering, reporting, and recording information
- When to communicate: the urgency and frequency of communication required
- Where to communicate: whiteboards, client charts, huddles, meetings
- Why communication is important
- How to communicate: unit processes and technology
Reinforce the importance of frequent communication in acute care settings.
Emphasize that the other members of the health care team will base their analysis, synthesis, and evaluation of client care on their observations and information (such as care planning or physician’s orders).
Explain that other members of the health care team will base their client access and flow decisions on the most recent client information (such as who can be discharged or who can be admitted to a room and when).
Identify any specific protocols or site-specific processes that HCAs may encounter that will highlight the need for urgent and frequent communication processes (such as reduced staffing levels and high client acuity levels). Explain what the HCA role and responsibilities will be within these processes (such as re-prioritizing care and care activities to attend to different unit requirements).
Reinforce that HCAs should:
- Report any client care information during regular communication processes (in huddles, for example).
- Report any observations or concerns with client care, such as changes in client condition or bleeding, to the health care team leader immediately.
- Record any client care information they perform, such as bowel record or recording food or fluids, immediately after completing the care activity.
Acknowledge that sometimes communication processes do not go well. Explain the reporting structure that HCAs may use as a guide to facilitate difficult communication processes. Highlight any specific protocols, policies, or procedures that may be used at this site to address ongoing or unresolved communication difficulties (such as respectful workplace policies).
9. Role of the HCA in Responding to Emergency Codes in Acute Care
Courses: Concepts for Practice and Personal Care and Assistance
Estimated time: 30 minutes
Content related to codes is covered in the online orientation for students doing placements at health region sites. However, the following codes could be discussed regarding the differences in policy and protocols between acute care and complex care/community settings.
Code Blue
- Activate help (this may simply involve notifying the unit clerk, LPN, or RN nearest to the phone system, or emergency call button).
- Remove all obstructions from the client’s bedside and room (bedside table, chairs, etc.).
- Close the privacy drapes of any clients in the same room.
- Stand in the hallway and direct emergency personnel to the correct room.
- Be available to retrieve supplies and equipment that the code response team may require.
- Comfort any clients who may be located in the same room.
- Clean and tidy the area after the event.
Discuss the site policy and protocol for both witnessed and unwitnessed cardiac arrests and the importance of being aware of the DNR/code status.
Code White
A call for help due to a potentially violent situation or a violent or escalating incident.
- Call for help (this may simply involve notifying co-workers, the unit clerk, LPN, or RN nearest to the phone system or emergency call button). 911 may have to be called.
- Always maintain personal safety, removing yourself and any clients who may be at risk.
- Be available to provide support to those responding to the code white.
- Seek first aid if you were injured.
- Participate in any review of the incident.
- Provide support to those who may have been affected by the incident. Be aware of your own internal responses to the event and seek help if you are experiencing unhealthy reactions.
- Recognizing that a member of the interprofessional care team may not be available as a resource for HCA practice during the time they are responding to an event, identify the next appropriate care provider who will provide guidance and direction.
Discuss the differences between a code white response in AM acute care, complex care facility, or community setting.
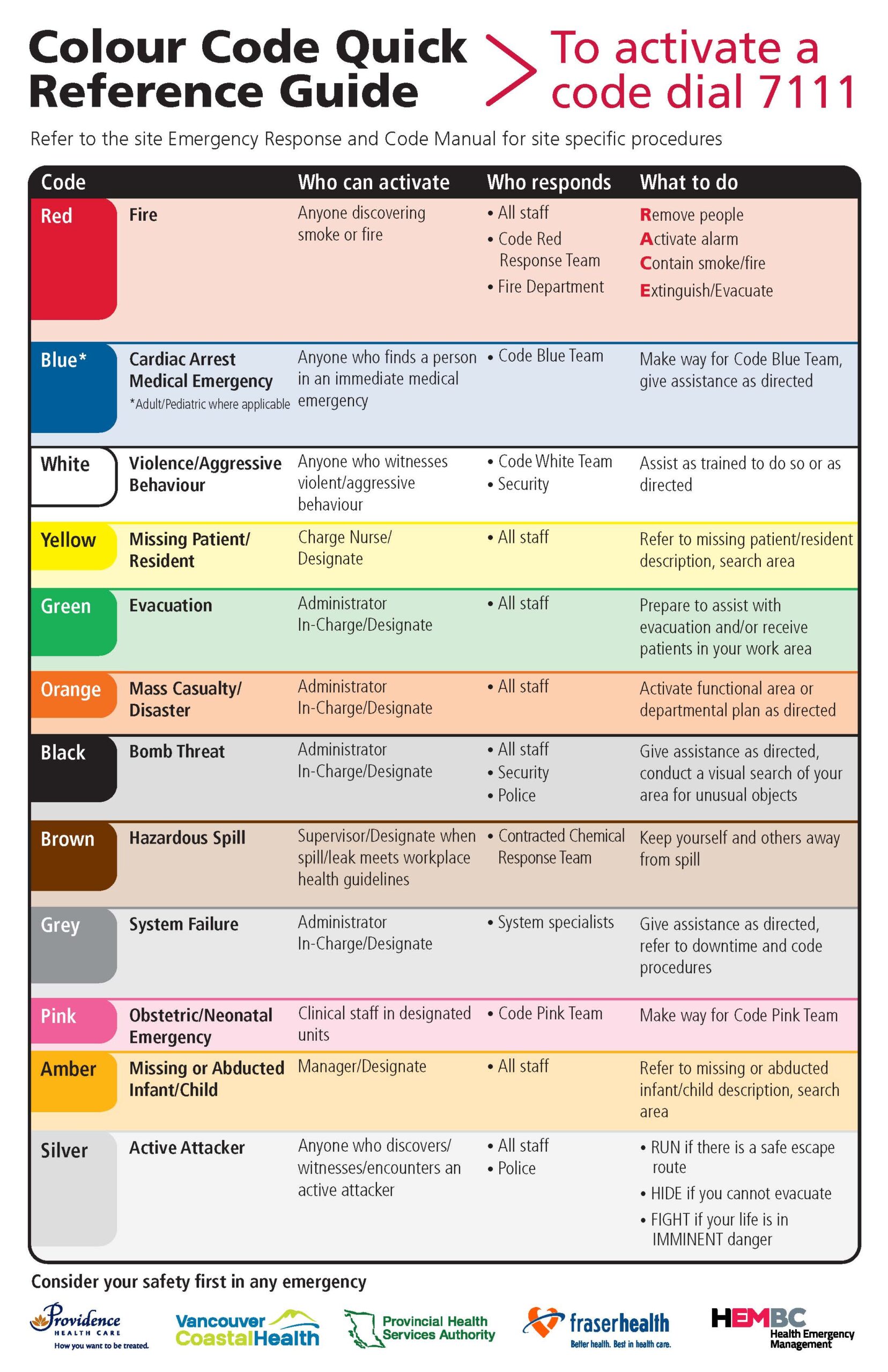
Image Description
Colour Codes Quick Reference Guide
To activate a code, dial 7111. Refer to the site Emergency Response and Code Manual for site specific procedures.
| Code | Who can activate | Who responds | What to do |
|---|---|---|---|
| Red: Fire | Anyone discovering smoke or fire |
|
|
| Blue: Cardiac Arrest Medical Emergency (Adult/Pediatric when applicable) | Anyone who finds a person in an immediate medical emergency |
|
Make way for the Code Blue Team, give assistance as directed. |
| White: Violence/Aggressive Behaviour | Anyone who witnesses violent/aggressive behaviour |
|
Assist as trained to do so or as directed |
| Yellow: Missing Patient/Resident | Charge Nurse/Designate |
|
Refer to missing patient/resident description, search area |
| Green: Evacuation | Administrator In-Charge/Designate |
|
Prepare to assist with evacuation and/or receive patients in your work area |
| Orange: Mass Casualty/Disaster | Administrator In-Charge/Designate |
|
Activate functional area or departmental plan as directed |
| Black: Bomb Threat | Administrator In-Charge/Designate |
|
Give assistance as directed, conduct a visual search of your area for unusual objects |
| Brown: Hazardous Spill | Supervisor/Designate when spill/leak meets workplace health guidelines |
|
Keep yourself and others away from spill |
| Grey: System Failure | Administrator In-Charge/Designate |
|
Give assistance as directed, refer to downtime and code procedures |
| Pink: Obstetric/Neonatal Emergency | Clinical staff in designated units |
|
Make way for Code Pink Team |
| Amber: Missing or Abducted Infant/Child | Manager/Designate |
|
Refer to missing or abducted infant/child description. search area |
| Silver: Active Attacker | Anyone who discovers/witnesses/encounters an active attacker |
|
|
