Unit 3.1: Eukaryotic pathogens.
Outline
Learning Objectives
After reading the following, you should be able to:
- Describe the defining characteristics of fungi, and the two basic forms of fungi.
- Describe the five types of mycoses: systemic, subcutaneous, cutaneous, superficial and opportunistic and describe a common type of fungal skin infection.
- Name two toxins that are produced by fungi, and their effects.
- Describe the defining characteristics of algae.
- Name and describe two algal diseases.
- Describe the defining characteristics of protozoa.
- Describe the life cycles of three pathogenic protozoa and the illnesses they causes.
- Describe the defining characteristics of helminthes
- Describe how parasitic helminthes differ from free living helminthes.
- Describe the life cycle and characteristics of two flatworm species.
- Describe the life cycle and characteristics of two roundworm species.
Fungi
Fungi are important to humans in a variety of ways. Both microscopic and macroscopic fungi have medical relevance, with some pathogenic species that can cause mycoses (illnesses caused by fungi). Some pathogenic fungi are opportunistic, meaning that they mainly cause infections when the host’s immune defenses are compromised and do not normally cause illness in healthy individuals. Fungi are important in other ways. They act as decomposers in the environment, and they are critical for the production of certain foods such as cheeses.
Fungi have well-defined characteristics that set them apart from other organisms. Most multicellular fungal bodies, commonly called molds, are made up of filaments called hyphae. Hyphae can form a tangled network called a mycelium and form the thallus (body) of fleshy fungi. In contrast to molds, yeasts are unicellular fungi. The budding yeasts reproduce asexually by budding off a smaller daughter cell; the resulting cells may sometimes stick together as a short chain or pseudohypha. Candida albicans is a common yeast that forms pseudohyphae; it is associated with various infections in humans, including vaginal yeast infections, oral thrush, and candidiasis of the skin.
There are notable unique features in fungal cell walls and membranes. Fungal cell walls contain chitin, as opposed to the cellulose found in the cell walls of plants and many protists. Additionally, whereas animals have cholesterol in their cell membranes, fungal cell membranes have different sterols called ergosterols. Ergosterols are often exploited as targets for antifungal drugs.
Fungal life cycles are unique and complex. Fungi reproduce sexually either through cross- or self-fertilization. Fungi may also exhibit asexual reproduction by mitosis, mitosis with budding, fragmentation of hyphae, and formation of asexual spores by mitosis (Figure 3.1). These spores are specialized cells that, depending on the organism, may have unique characteristics for survival, reproduction, and dispersal.

Fungal Skin Infections: Fungi often cause skin infections. Many fungal infections of the skin involve fungi that are found in the normal skin microbiota. Some of these fungi can cause infection when they gain entry through a wound; others mainly cause opportunistic infections in immunocompromised patients. Other fungal pathogens primarily cause infection in unusually moist environments that promote fungal growth; for example, sweaty shoes, communal showers, and locker rooms provide excellent breeding grounds that promote the growth and transmission of fungal pathogens.
Fungal infections, also called mycoses, can be divided into classes based on their invasiveness. Mycoses that cause infections of the epidermis, hair, and nails, are called cutaneous mycoses, if the fungi digest the keratin, or superficial, if there is no keratin digestion. Mycoses that penetrate the epidermis and the dermis to infect deeper tissues are called subcutaneous mycoses. Mycoses that spread throughout the body are called systemic mycoses.
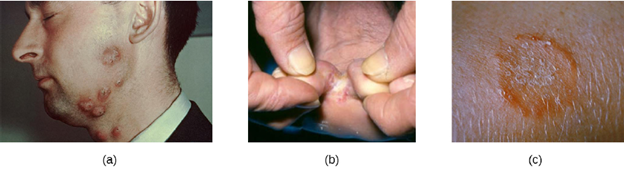
A group of cutaneous mycoses called tineas are caused by dermatophytes, fungal molds that require keratin, a protein found in skin, hair, and nails, for growth. There are three genera of dermatophytes, all of which can cause cutaneous mycoses: Trichophyton, Epidermophyton, and Microsporum. Tineas on most areas of the body are generally called ringworm, but tineas in specific locations may have distinctive names and symptoms (see Table 3.1 and Figure 3.2). Keep in mind that these names—even though they are Latinized—refer to locations on the body, not causative organisms. Tineas can be caused by different dermatophytes in most areas of the body.
Dermatophytes are commonly found in the environment and in soils and are frequently transferred to the skin via contact with other humans and animals. Fungal spores can also spread on hair. Many dermatophytes grow well in moist, dark environments. For example, tinea pedis (athlete’s foot) commonly spreads in public showers, and the causative fungi grow well in the dark, moist confines of sweaty shoes and socks. Likewise, tinea cruris (jock itch) often spreads in communal living environments and thrives in warm, moist undergarments. Tineas on the body (tinea corporis) often produce lesions that grow radially and heal towards the center. This causes the formation of a red ring, leading to the misleading name of ringworm.
| Tinea corporis (ringworm) | Body |
| Tinea capitis (ringworm)Tinea | Scalp |
| Tinea pedis (athlete’s foot) | Feet |
| Tinea barbae (barber’s iitch) | Beard |
| Tinea cruris (jock itch) | Groin |
| Tinea unguium (onychomycosis) | Toenails, fingernails |
Fungal Toxins: Some fungi a pathogenic due to the toxins they produce. Fungal toxins are called mycotoxins. Claviceps purpurea, a fungus that grows on rye and related grains, produces a mycotoxin called ergot toxin, an alkaloid responsible for the disease known as ergotism. There are two forms of ergotism: gangrenous and convulsive. In gangrenous ergotism, the ergot toxin causes vasoconstriction, resulting in improper blood flow to the extremities, eventually leading to gangrene. A famous outbreak of gangrenous ergotism occurred in Eastern Europe during the 5th century AD due to the consumption of rye contaminated with C. purpurea. In convulsive ergotism, the toxin targets the central nervous system, causing mania and hallucinations.
The mycotoxin aflatoxin is a virulence factor produced by the fungus Aspergillus, an opportunistic pathogen that can enter the body via contaminated food or by inhalation. Inhalation of the fungus can lead to the chronic pulmonary disease aspergillosis, characterized by fever, bloody sputum, and/or asthma. Aflatoxin acts in the host as both a mutagen (a substance that causes mutations in DNA) and a carcinogen (a substance involved in causing cancer), and has been associated with the development of liver cancer. Aflatoxin has also been shown to cross the blood-placental barrier.
Algae
The algae are autotrophic protists that can be unicellular or multicellular. They are important ecologically and environmentally because they are responsible for the production of approximately 70% of the oxygen and organic matter in aquatic environments. Some types of algae, even those that are microscopic, are regularly eaten by humans and other animals. Additionally, algae are the source for agar, agarose, and carrageenan, solidifying agents used in laboratories and in food production. Although algae are typically not pathogenic, some produce toxins. Harmful algal blooms, which occur when algae grow quickly and produce dense populations, can produce high concentrations of toxins that impair liver and nervous-system function in aquatic animals and humans.
All algae are photosynthetic. Their cells can have one or more chloroplasts that contain structures called pyrenoids to synthesize and store starch. Different algal groups have different pigments, which are reflected in common names such as red algae, brown algae, and green algae. Some algae, the seaweeds, are macroscopic and may be confused with plants. Seaweeds can be red, brown, or green, depending on their photosynthetic pigments. Green algae, in particular, share some important similarities with land plants; however, there are also important distinctions. For example, seaweeds do not have true tissues or organs like plants do. Additionally, seaweeds do not have a waxy cuticle to prevent desiccation. Algae can also be confused with cyanobacteria, photosynthetic bacteria that bear a resemblance to algae; however, cyanobacteria are prokaryotes. Two examples of pathogenic algae are diatoms and dinoflagellates.
- Diatoms: Diatoms have flagella and frustules, which are outer cell walls of crystallized silica; their fossilized remains are used to produce diatomaceous earth, which has a range of uses such as filtration and insulation. Additionally, diatoms can reproduce sexually or asexually. Certain diatoms produce a toxin called domoic acid. Organisms that eat diatoms, such as clams, oysters, mussels and shrimp, accumulate domoic acid in their tissues. Other animals that go on to eat these organisms are thus exposed to the toxins. At each step along a food chain, the concentration of the toxin increases through a process known as bioaccumulation. In high enough concentrations, domoic acid causes domoic acid toxicosis, a neurological disease with symptoms including diarrhea and memory loss. An outbreak of domoic acid toxicosis in Canada in 1987 resulted in more than 100 affected individuals and 3 deaths. While large outbreaks are uncommon in human, domoic acid toxicosis has been found to be the culprit in the deaths of hundreds of birds and marine mammals, including the deaths of several baleen whales.
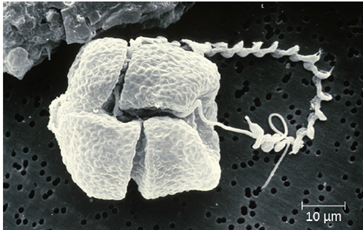
- Dinoflagellates: The dinoflagellates are mostly marine organisms and are an important component of plankton. They have a variety of nutritional types and may be phototrophic, heterotrophic, or mixotrophic. They generally have two flagella, causing them to whirl (in fact, the name dinoflagellate comes from the Greek word for “whirl”: dini). Some have cellulose plates forming a hard outer covering, or theca, as armor (Figure 3.3). When a population of dinoflagellates becomes particularly dense, a red tide (a type of harmful algal bloom) can occur. Exposure can occur through contact with water containing the dinoflagellate toxins or by feeding on organisms that have eaten dinoflagellates.
Dinoflagellates responsible for red tides produce neurotoxins collectively called saxitoxins. Exposure to high concentrations of saxitoxins usually occurs through the ingestion of shellfish, due to bioaccumulation, as was the case with domoic acid. Exposure to saxitoxins can result in paralytic shellfish poisoning. In humans, symptoms include numbness, dizziness, nausea, vomiting, headaches and in severe cases, respiratory failure, leading to death. While reported cases in humans are rare, toxic plankton kills untold numbers of fish, and marine birds and mammals.
Protozoa
Eukaryotic microbes are an extraordinarily diverse group, including species with a wide range of life cycles, morphological specializations, and nutritional needs. Although more diseases are caused by viruses and bacteria than by microscopic eukaryotes, these eukaryotes are responsible for some diseases of great public health importance. For example, the protozoal disease malaria was responsible for 584,000 deaths worldwide (primarily children in Africa) in 2013, according to the World Health Organization (WHO).
Protozoans inhabit a wide variety of habitats, both aquatic and terrestrial. Many are free-living, while others are parasitic, carrying out a life cycle within a host or hosts and potentially causing illness. There are also beneficial symbionts that provide metabolic services to their hosts. During the feeding and growth part of their life cycle, they are called trophozoites; these feed on small particulate food sources such as bacteria. While some types of protozoa exist exclusively in the trophozoite form, others can develop from trophozoite to an encapsulated cyst stage when environmental conditions are too harsh for the trophozoite. A cyst is a cell with a protective wall, and the process by which a trophozoite becomes a cyst is called encystment. When conditions become more favorable, these cysts are triggered by environmental cues to become active again through excystment.
Protozoans have a variety of reproductive mechanisms. Some protozoans reproduce asexually and others reproduce sexually; still others are capable of both sexual and asexual reproduction. In protozoans, asexual reproduction occurs by binary fission, budding, or schizogony. In schizogony, the nucleus of a cell divides multiple times before the cell divides into many smaller cells. The products of schizogony are called merozoites and they are stored in structures known as schizonts. Protozoans may also reproduce sexually, which increases genetic diversity and can lead to complex life cycles.
Most pathogenic protozoa are parasites. Parasites live on or in another organism, called a host, causing harm to their hosts. In parasitic infections, the parasite’s preferred host is called the definitive host. In parasites with complex life cycles, the definitive host is the host in which the parasite reaches sexual maturity. Some parasites may also infect one or more intermediate hosts in which the parasite goes through several immature life cycle stages or reproduces asexually.
- Entamoeba histolytica: The protozoan parasite Entamoeba histolytica causes amoebiasis, which is known as amoebic dysentery in severe cases. E. histolytica is generally transmitted through water or food that has fecal contamination containing the amoebic cysts. The disease is most widespread in the developing world and is one of the leading causes of mortality from parasitic disease worldwide. Disease can be caused by as few as 10 cysts being transmitted. Humans are the definitive host for E. histolytica.
Signs and symptoms range from nonexistent to mild diarrhea to severe amoebic dysentery. Severe infection causes the abdomen to become distended and may be associated with fever. The parasite may live in the colon without causing signs or symptoms, producing cysts which are then excreted with the feces, or may invade the mucosa to cause colitis. In some cases, the disease spreads to the spleen, brain, genitourinary tract, or lungs. In particular, it may spread to the liver and cause an abscess. When a liver abscess develops, fever, nausea, liver tenderness, weight loss, and pain in the right abdominal quadrant may occur. Chronic infection may occur and is associated with intermittent diarrhea, mucus, pain, flatulence, and weight loss. Up to 500 million people may be infected with E. histolytica worldwide, with upwards of 100,000 deaths annually. E. histolytica is susceptible to several anti-protozoan medications and can be treated with the appropriate medications.
- Plasmodium: Despite more than a century of intense research and clinical advancements, malaria remains one of the most important infectious diseases in the world today. Its widespread distribution places more than half of the world’s population in jeopardy. In 2015, the WHO estimated there were about 214 million cases of malaria worldwide, resulting in about 438,000 deaths; about 88% of cases and 91% of deaths occurred in Africa. Although malaria is not currently a major threat in the US, the possibility of its reintroduction is a concern. Malaria is caused by several protozoan parasites in the genus Plasmodium: P. falciparum, P. knowlesi, P. malariae, P. ovale, and P. vivax. Plasmodium primarily infects red blood cells and are transmitted through the bite of Anopheles mosquitoes. Currently, P. falciparum is the most common and most lethal cause of malaria, often called falciparum malaria.
Falciparum malaria is widespread in highly populated regions of Africa and Asia, putting many people at risk for the most severe form of the disease.
The classic signs and symptoms of malaria are cycles of extreme fever and chills. The sudden, violent symptoms of malaria start with malaise, abrupt chills, and fever (39–41° C [102.2–105.8 °F]), rapid and faint pulse, polyuria, headache, myalgia, nausea, and vomiting. After 2 to 6 hours of these symptoms, the fever falls, and profuse sweating occurs for 2 to 3 hours, followed by extreme fatigue. These symptoms are a result of Plasmodium emerging from red blood cells synchronously, leading to simultaneous rupture of a large number of red blood cells, resulting in damage to the spleen, liver, lymph nodes, and bone marrow. The organ damage resulting from hemolysis causes patients to develop sludge blood (i.e., blood in which the red blood cells agglutinate into clumps) that can lead to lack of oxygen, necrosis of blood vessels, organ failure, and death. In established infections, malarial cycles of fever and chills typically occur every 2 days in the disease described as tertian malaria, which is caused by P. vivax and P. ovale. The cycles occur every 3 days in the disease described as quartan malaria, which is caused by P. malariae. These intervals may vary among cases.
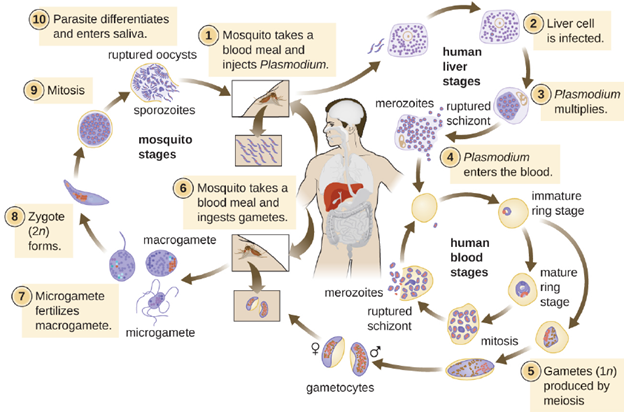
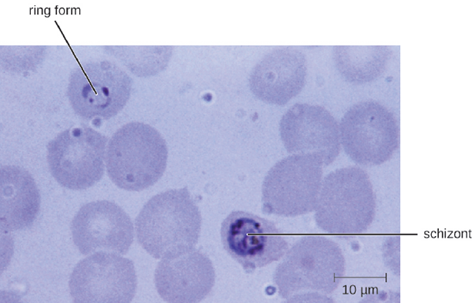
Plasmodium has a complex life cycle that includes several developmental stages alternately produced in mosquitoes, which are the definitive hosts, and humans which are the intermediate hosts (Figure 3.4). When an infected mosquito takes a blood meal, sporozoites in the mosquito salivary gland are injected into the host’s blood. These parasites circulate to the liver, where they develop into schizonts. The schizonts then undergo schizogony, resulting in the release of many merozoites at once. The merozoites move to the bloodstream and infect red blood cells. Inside red blood cells, merozoites develop into trophozoites that produce more merozoites. The synchronous release of merozoites from red blood cells in the evening leads to the symptoms of malaria.
In addition, some trophozoites alternatively develop into male and female gametocytes. The gametocytes are taken up when the mosquito takes a blood meal from an infected individual. Sexual sporogony occurs in the gut of the mosquito. The gametocytes fuse to form zygotes in the insect gut. The zygotes become motile and elongate into an ookinete. This form penetrates the midgut wall and develops into an oocyst. Finally, the oocyst releases new sporozoites that migrate to the mosquito salivary glands to complete the life cycle.
Diagnosis of malaria can be done by microscopic observation of developmental forms of Plasmodium in blood smears (Figure 3.5). Drugs such as chloroquine, atovaquone , artemether, and lumefantrine may be prescribed for both acute and prophylactic therapy, although some Plasmodium spp. have shown resistance to antimalarial drugs. Use of insecticides and insecticide-treated bed nets can limit the spread of malaria. Despite efforts to develop a vaccine for malaria, none is currently available.
- Toxoplasma gondii: The disease toxoplasmosis is caused by the protozoan Toxoplasma gondii. T. gondii is found in a wide variety of birds and mammals, and human infections are common. The Centers for Disease Control and Prevention (CDC) estimates that 22.5% of the population 12 years and older has been infected with T. gondii; but immunocompetent individuals are typically asymptomatic, however. Domestic cats are the only known definitive hosts for the sexual stages of T. gondii and, thus, are the main reservoirs of infection. Infected cats shed T. gondii oocysts in their feces, and these oocysts typically spread to humans through contact with fecal matter on cats’ bodies, in litter boxes, or in garden beds where outdoor cats defecate.
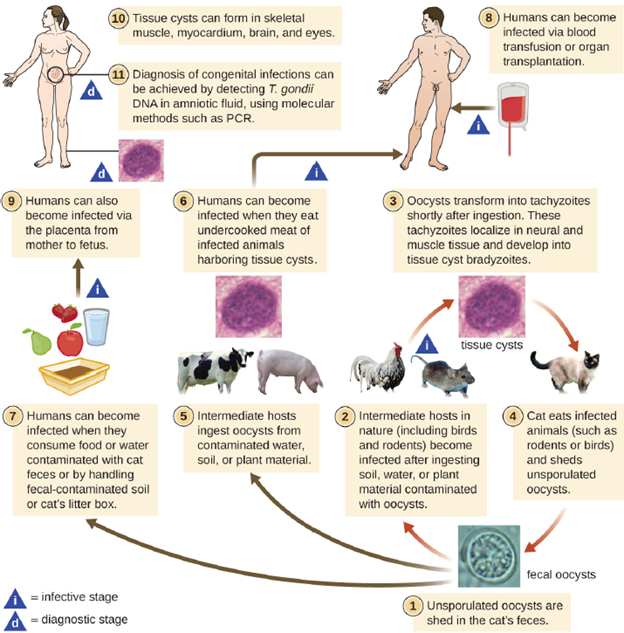
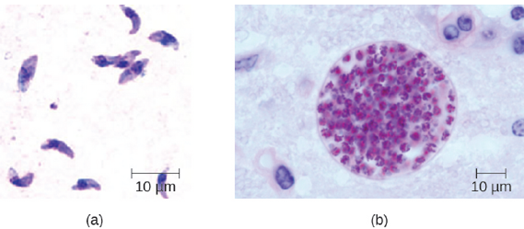
T. gondii has a complex life cycle that involves multiple hosts. The T. gondii life cycle begins when unsporulated oocysts are shed in the cat’s feces. These oocysts take 1–5 days to sporulate in the environment and become infective. Intermediate hosts in nature include birds and rodents, which become infected after ingesting soil, water, or plant material contaminated with the infective oocysts. Once ingested, the oocysts transform into tachyzoites that localize in the bird or rodent neural and muscle tissue, where they develop into tissue cysts. Cats may become infected after consuming birds and rodents harboring tissue cysts. Cats and other animals may also become infected directly by ingestion of sporulated oocysts in the environment. Interestingly, Toxoplasma infection appears to be able to modify the host’s behavior. Mice infected by Toxoplasma lose their fear of cat pheromones. As a result, they become easier prey for cats, facilitating the transmission of the parasite to the cat definitive host (Figure 3.6).
Toxoplasma infections in humans are extremely common, but most infected people are asymptomatic or have subclinical symptoms. Some studies suggest that the parasite may be able to influence the personality and psychomotor performance of infected humans, similar to the way it modifies behavior in other mammals. When symptoms do occur, they tend to be mild and similar to those of mononucleosis. However, asymptomatic toxoplasmosis can become problematic in certain situations. Cysts can lodge in a variety of human tissues and lie dormant for years. Reactivation of these quiescent infections can occur in immunocompromised patients following transplantation, cancer therapy, or the development of an immune disorder such as AIDS. In patients with AIDS who have toxoplasmosis, the immune system cannot combat the growth of T. gondii in body tissues; as a result, these cysts can cause encephalitis, retinitis, pneumonitis, cognitive disorders, and seizures that can eventually be fatal.
Toxoplasmosis can also pose a risk during pregnancy because tachyzoites can cross the placenta and cause serious infections in the developing fetus. The extent of fetal damage resulting from toxoplasmosis depends on the severity of maternal disease, the damage to the placenta, the gestational age of the fetus when infected, and the virulence of the organism. Congenital toxoplasmosis often leads to fetal loss or premature birth and can result in damage to the central nervous system, manifesting as mental retardation, deafness, or blindness. Consequently, pregnant women are advised by the CDC to take particular care in preparing meat, gardening, and caring for pet cats. Diagnosis of toxoplasmosis infection during pregnancy is usually achieved by serology including TORCH testing (the “T” in TORCH stands for toxoplasmosis). Diagnosis of congenital infections can also be achieved by detecting T. gondii DNA in amniotic fluid, using molecular methods.
In adults, diagnosis of toxoplasmosis can include observation of tissue cysts in tissue specimens. Tissue cysts may be observed in stained biopsy specimens, and CT, magnetic resonance imaging, and lumbar puncture can also be used to confirm infection (Figure 3.7).
Preventing infection is the best first-line defense against toxoplasmosis. Preventive measures include washing hands thoroughly after handling raw meat, soil, or cat litter, and avoiding consumption of vegetables possibly contaminated with cat feces. Most immunocompetent patients do not require clinical intervention for Toxoplasma infections. However, neonates, pregnant women, and immunocompromised patients can be treated with pyrimethamine and sulfadiazine—except during the first trimester of pregnancy, because these drugs can cause birth defects.
Multicellular Animal Parasites
Parasitic helminths are animals that are often included within the study of microbiology because many species of these worms are identified by their microscopic eggs and larvae. There are two major groups of parasitic helminths: the roundworms (Nematoda) and flatworms (Platyhelminthes). Of the many species that exist in these groups, about half are parasitic and some are important human pathogens. As animals, they are multicellular and have organ systems. However, the parasitic species often have limited digestive tracts, nervous systems, and locomotor abilities, due to the fact that they don’t have to search for food, regulate body temperature, perform their own digestion or avoid predation. Compared to free living worms, parasitic worms may have complex reproductive systems, often producing hundreds of thousands of eggs per day. Some are monoecious, having both male and female reproductive organs in a single individual, while others are dioecious, each having either male or female reproductive organs.
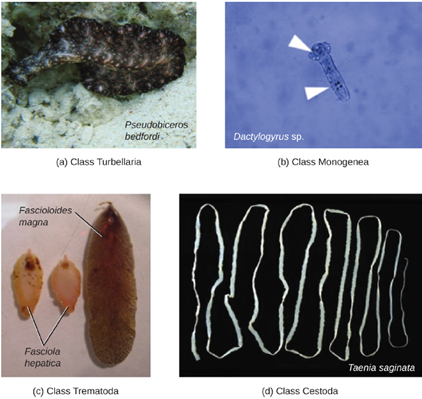
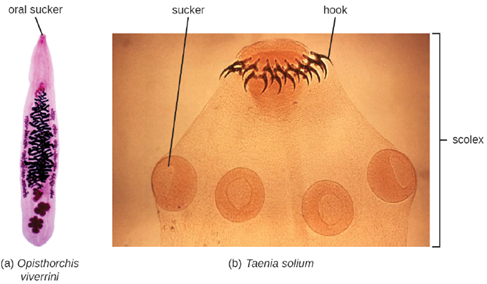
- Platyhelminthes: Phylum Platyhelminthes (the platyhelminths) are flatworms. This group includes the flukes, tapeworms, and the turbellarians, which include planarians. The flukes and tapeworms are medically important parasites (Figure 3.8). The flukes (trematodes) are nonsegmented flatworms that have an oral sucker (Figure 3.9) (and sometimes a second ventral sucker) and attach to the inner walls of intestines, lungs, large blood vessels, or the liver. The other medically important group of platyhelminths are commonly known as tapeworms (cestodes) and are segmented flatworms that may have suckers or hooks at the scolex (head region) (Figure 3.9). Tapeworms use these suckers or hooks to attach to the wall of the small intestine. The body of the worm is made up of segments called proglottids that contain reproductive structures; these detach when the gametes are fertilized, releasing gravid proglottids with eggs. Tapeworms often have an intermediate host that consumes the eggs, which then hatch into a larval form called an oncosphere. The oncosphere migrates to a particular tissue or organ in the intermediate host, where it forms cysticerci. After being eaten by the definitive host, the cysticerci develop into adult tapeworms in the host’s digestive system.
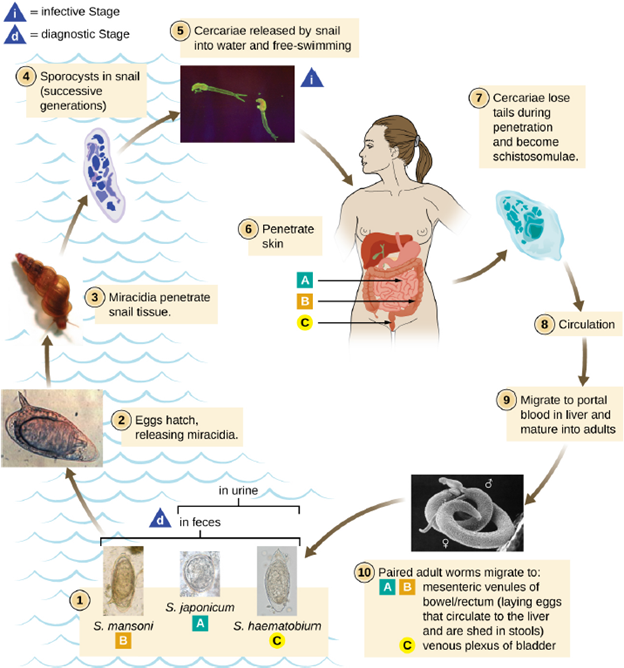
- Schistosoma: Schistosomiasis is an disease caused by blood flukes in the genus Schistosoma that are native to the Caribbean, South America, Middle East, Asia, and Africa. Most human schistosomiasis cases are caused by Schistosoma mansoni, S. haematobium, or S. japonicum. Schistosoma are the only trematodes that invade through the skin; all other trematodes infect by ingestion. WHO estimates that at least 258 million people required preventive treatment for schistosomiasis in 2014.
Infected human hosts shed Schistosoma eggs in urine and feces, which can contaminate freshwater habitats of snails that serve as intermediate hosts. The eggs hatch in the water, releasing miracidia, an intermediate growth stage of the Schistosoma that infect the snails. The miracidia mature and multiply inside the snails, transforming into cercariae that leave the snail and enter the water, where they can penetrate the skin of swimmers and bathers. The cercariae migrate through human tissue and enter the bloodstream, where they mature into adult male and female worms that mate and release fertilized eggs. The eggs travel through the bloodstream and penetrate various body sites, including the bladder or intestine, from which they are excreted in urine or stool to start the life cycle over again (Figure 3.10).
A few days after infection, patients may develop a rash or itchy skin associated with the site of cercariae penetration. Within 1–2 months of infection, symptoms may develop, including fever, chills, cough, and myalgia, as eggs that are not excreted circulate through the body. After years of infection, the eggs become lodged in tissues and trigger inflammation and scarring that can damage the liver, central nervous system, intestine, spleen, lungs, and bladder. This may cause abdominal pain, enlargement of the liver, blood in the urine or stool, and problems passing urine. Increased risk for bladder cancer is also associated with chronic Schistosoma infection. In addition, children who are repeatedly infected can develop malnutrition, anemia, and learning difficulties.
Diagnosis of schistosomiasis is made by the microscopic observation of eggs in feces or urine, intestine or bladder tissue specimens, or serologic tests. The drug praziquantel is effective for the treatment of all schistosome infections. Improving wastewater management and educating at-risk populations to limit exposure to contaminated water can help control the spread of the disease.
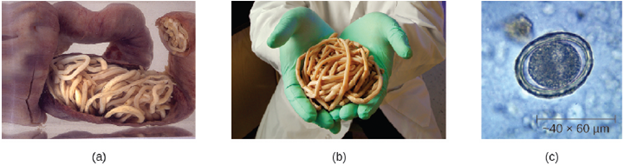
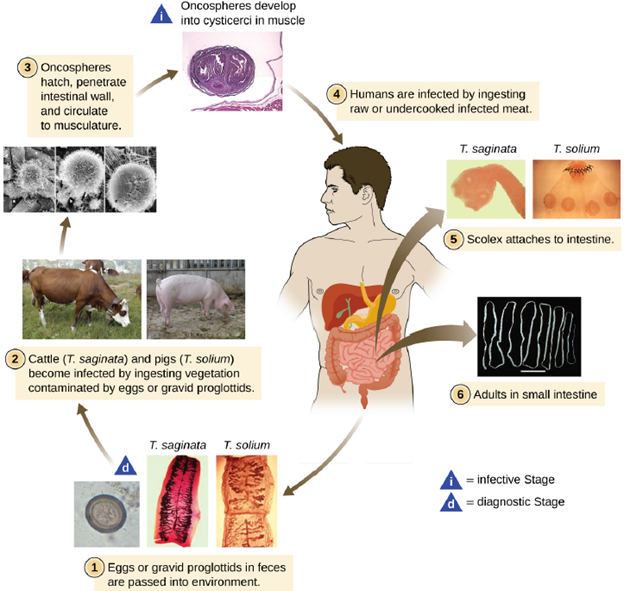
- Taenia solium: Taeniasis is a tapeworm infection, generally caused by pork (Taenia solium), beef (Taenia saginata), and Asian (Taenia asiatica) tapeworms found in undercooked meat. Humans are the definitive hosts for these parasites and pass the parasite onto other animals via our waste products. Consumption of raw or undercooked fish, including contaminated sushi, can also result in infection from the fish tapeworm (Diphyllobothrium latum). Tapeworms are flatworms (cestodes) with multiple body segments and a head called a scolex that attaches to the intestinal wall. Tapeworms can become quite large, reaching 4 to 8 meters long Figure 3.11 illustrates the life cycle of a tapeworm.
Tapeworms attached to the intestinal wall produce eggs that are excreted in feces. After ingestion by animals, the eggs hatch and the larvae emerge. They may take up residence in the intestine, but can sometimes move to other tissues, especially muscle or brain tissue. When T. solium larvae form cysts in tissue, the condition is called cysticercosis. This occurs through ingestion of eggs via the fecal-oral route, not through consumption of undercooked meat. It can develop in the muscles, eye (ophthalmic cysticercosis), or brain (neurocysticercosis).
Infections may be asymptomatic or they may cause mild gastrointestinal symptoms such as epigastric discomfort, nausea, diarrhea, flatulence, or hunger pains. It is also common to find visible tapeworm segments passed in the stool. In cases of cysticercosis, symptoms differ depending upon where the cysts become established. Neurocysticercosis can have severe, life-threatening consequences and is associated with headaches and seizures because of the presence of the tapeworm larvae encysted in the brain. Cysts in muscles may be asymptomatic, or they may be painful. To diagnose these conditions, microscopic analysis of stool samples from three separate days is generally recommended. Eggs or body segments, called proglottids, may be visible in these samples. Molecular methods have been developed but are not yet widely available. Imaging, such as CT and MRI, may be used to detect cysts. Anti-heminthes medications, such as praziquantel or niclosamide, are used for treatment.
- Nematodes: Phylum Nematoda (the roundworms) is a diverse group containing more than 15,000 species, of which several are important human parasites. These unsegmented worms have a full digestive system even when parasitic and in most case they are dioecious. Some are common intestinal parasites, and their eggs can sometimes be identified in feces or around the anus of infected individuals. Parasitic nematodes can be either egg infective, where ingestion of eggs is required for infection, or larva infective, where the larval worms are able to burrow directly into the host.
- Enterobius vermicularis: Enterobius vermicularis, commonly called pinworms, are tiny (2–13 mm) nematodes that cause enterobiasis. Of all helminthic infections, enterobiasis is the most common in the United States, affecting as many as one-third of American children. Although the signs and symptoms are generally mild, patients may experience abdominal pain and insomnia from itching of the perianal region, which frequently occurs at night when worms leave the anus to lay eggs. The itching contributes to transmission, as the disease is transmitted through the fecal-oral route. When an infected individual scratches the anal area, eggs may get under the fingernails and later be deposited near the individual’s mouth, causing reinfection, or on fomites, where they can be transferred to new hosts. After being ingested, the larvae hatch within the small intestine and then take up residence in the colon and develop into adults. From the colon, the female adult exits the body at night to lay eggs (Figure 6.28).
Infection is diagnosed in any of three ways. First, because the worms emerge at night to lay eggs, it is possible to inspect the perianal region for worms while an individual is asleep. An alternative is to use transparent tape to remove eggs from the area around the anus first thing in the morning for three days to yield eggs for microscopic examination. Finally, it may be possible to detect eggs through examination of samples from under the fingernails, where eggs may lodge due to scratching. Once diagnosis has been made drugs such as, mebendazole, albendazole, and pyrantel pamoate are effective for treatment.
- Ascaris lumbricoides: Infections caused by the large nematode roundworm Ascaris lumbricoides, a soil-transmitted helminth, are called ascariasis. Over 800 million to 1 billion people are estimated to be infected worldwide. Infections are most common in warmer climates and at warmer times of year. At present, infections are uncommon in the North America. The eggs of the worms are transmitted through contaminated food and water. This may happen if food is grown in contaminated soil, including when manure is used as fertilizer.
When an individual consumes embryonated eggs (those with a developing embryo), the eggs travel to the intestine and the larvae are able to hatch. Ascaris is able to produce proteases that allow for penetration and degradation of host tissue. The juvenile worms can then enter the circulatory system and migrate to the lungs where they enter the alveoli (air sacs). From here they crawl to the pharynx and then follow the gut lumen to return to the small intestine, where they mature into adult roundworms. Females in the host will produce and release eggs that leave the host via feces. In some cases, the worms can block ducts such as those of the pancreas or gallbladder.
The infection is commonly asymptomatic. When signs and symptoms are present, they include shortness of breath, cough, nausea, diarrhea, blood in the stool, abdominal pain, weight loss, and fatigue. The roundworms may be visible in the stool. In severe cases, children with substantial infections may experience intestinal blockage. The eggs can be identified by microscopic examination of the stool (Figure 3.12). In some cases, the worms themselves may be identified if coughed up or excreted in stool. They can also sometimes be identified by X-rays, ultrasounds, or MRIs. Ascariasis is usually self-limiting, but can last one to two years because the worms can inhibit the body’s inflammatory response. The first line of treatment is anti-helminths medication such as mebendazole or albendazole. In some severe cases, surgery may be required to remove worm masses.