Unit 7.1: Mechanisms of Disease Part 1
Outline
Classifications of Diseases: Behaviour in a Population
Classifications of Diseases: Severity
Learning Objectives
After reading the following, you should be able to:
- Define: pathology, etiology, stages of pathogenesis, infection, disease, normal flora, transient flora.
- Identify regions of the body that possess normal flora, giving specific examples.
- Define symbiotic, commensalistic, mutualistic and parasitic relationships.
- What is meant by the term “competitive inhibition” and why is that an advantage to a host?
- Describe (with examples): symptom, sign and syndrome.
- Describe the terms used for disease classification.
- Be able to draw a diagram with labels to describe the stages of disease.
A disease is any condition in which the normal structure or functions of the body are damaged or impaired. Physical injuries or disabilities are not classified as disease, but there can be several causes for disease, including infection by a pathogen, genetics (as in many cancers or deficiencies), noninfectious environmental causes, or inappropriate immune responses. Our focus in this chapter will be on infectious diseases, although when diagnosing infectious diseases, it is always important to consider possible noninfectious causes.
Symbiotic Relationships: As we have learned, prokaryotic microorganisms can associate with plants and animals. Often, this association results in unique relationships between organisms. For example, bacteria living on the roots or leaves of a plant get nutrients from the plant and, in return, produce substances that protect the plant from pathogens. On the other hand, some bacteria are plant pathogens that use mechanisms of infection similar to bacterial pathogens of animals and humans.
Prokaryotes live in a community, or a group of interacting populations of organisms. A population is a group of individual organisms belonging to the same biological species and limited to a certain geographic area. Populations can have cooperative interactions, which benefit the populations, or competitive interactions, in which one population competes with another for resources. The study of these interactions between populations is called microbial ecology.
Any interaction between different species within a community is called symbiosis. Such interactions fall along a continuum between opposition and cooperation. Interactions in a symbiotic relationship may be beneficial or harmful, or have no effect on one or both of the species involved.
When two species benefit from each other, the symbiosis is called mutualism (or syntropy, or crossfeeding). For example, humans have a mutualistic relationship with certain strains of Escherichia coli, another bacterium found in the gut. E. coli relies on intestinal contents for nutrients, and humans derive certain vitamins from E. coli, particularly vitamin K, which is required for the formation of blood clotting factors. (This is only true for some strains of E. coli, however. Other strains are pathogenic and do not have a mutualistic relationship with humans.)
In another type of symbiosis, called commensalism, one organism benefits while the other is unaffected. This occurs when the bacterium Staphylococcus epidermidis uses the dead cells of the human skin as nutrients. Billions of these bacteria live on our skin, but in most cases (especially when our immune system is healthy), we do not react to them in any way.
A type of symbiosis in which one organism benefits while harming the other is called parasitism. The relationship between humans and many pathogenic prokaryotes can be characterized as parasitic because these organisms invade the body, producing toxic substances or infectious diseases that cause harm. Diseases such as tetanus, diphtheria, pertussis, tuberculosis, and leprosy all arise from interactions between bacteria and humans.
Scientists have coined the term microbiome to refer to all prokaryotic and eukaryotic microorganisms that are associated with a certain organism. Within the human microbiome, there are resident microbiota and transient microbiota. The resident microbiota consists of microorganisms that constantly live in or on our bodies. The term transient microbiota refers to microorganisms that are only temporarily found in the human body, and these may include pathogenic microorganisms. Hygiene and diet can alter both the resident and transient microbiota.
The resident microbiota is amazingly diverse, not only in terms of the variety of species but also in terms of the preference of different microorganisms for different areas of the human body. For example, in the human mouth, there are thousands of commensal or mutualistic species of bacteria. Some of these bacteria prefer to inhabit the surface of the tongue, whereas others prefer the internal surface of the cheeks, and yet others prefer the front or back teeth or gums. The inner surface of the cheek has the least diverse microbiota because of its exposure to oxygen. By contrast, the crypts of the tongue and the spaces between teeth are two sites with limited oxygen exposure, so these sites have more diverse microbiota, including bacteria living in the absence of oxygen (e.g., Bacteroides, Fusobacterium).
Differences in the oral microbiota between randomly chosen human individuals are also significant. Studies have shown, for example, that the prevalence of such bacteria as Streptococcus, Haemophilus, Neisseria, and others was dramatically different when compared between individuals.
There are also significant differences between the microbiota of different sites of the same human body. The inner surface of the cheek has a predominance of Streptococcus, whereas in the throat, the palatine tonsil, and saliva, there are two to three times fewer Streptococcus, and several times more Fusobacterium. In the plaque removed from gums, the predominant bacteria belong to the genus Fusobacterium. However, in the intestine, both Streptococcus and Fusobacterium disappear, and the genus Bacteroides becomes predominant.
Not only can the microbiota vary from one body site to another, the microbiome can also change over time within the same individual. Humans acquire their first inoculations of normal flora during natural birth and shortly after birth. Before birth, there is a rapid increase in the population of Lactobacillus spp. in the vagina, and this population serves as the first colonization of microbiota during natural birth. After birth, additional microbes are acquired from healthcare providers, parents, other relatives, and individuals who come in contact with the baby. This process establishes a microbiome that will continue to evolve over the course of the individual’s life as new microbes colonize and are eliminated from the body. For example, it is estimated that within a 9-hour period, the microbiota of the small intestine can change so that half of the microbial inhabitants will be different. The importance of the initial Lactobacillus colonization during vaginal child birth is highlighted by studies demonstrating a higher incidence of diseases in individuals born by cesarean section, compared to those born vaginally. Studies have shown that babies born vaginally are predominantly colonized by vaginal lactobacillus, whereas babies born by cesarean section are more frequently colonized by microbes of the normal skin microbiota, including common hospital-acquired pathogens.
Throughout the body, resident microbiotas are important for human health because they occupy niches that might be otherwise taken by pathogenic microorganisms, through a process called competitive inhibition. Through their occupation of cellular binding sites and competition for available nutrients, the resident microbiota prevent the critical early steps of pathogen attachment and proliferation required for the establishment of an infection. For instance, Lactobacillus spp. are the dominant bacterial species of the normal vaginal microbiota for most women. Lactobacillus produces lactic acid, contributing to the acidity of the vagina and inhibiting the growth of pathogenic yeasts. However, when the population of the resident microbiota is decreased for some reason (e.g., because of taking antibiotics), the pH of the vagina increases, making it a more favorable environment for the growth of yeasts such as Candida albicans. Antibiotic therapy can also disrupt the microbiota of the intestinal tract and respiratory tract, increasing the risk for secondary infections and/or promoting the long-term carriage and shedding of pathogens.
Signs and Symptoms of Disease: An infection is the successful colonization of a host by a microorganism. Infections can lead to disease, which causes signs and symptoms resulting in a deviation from the normal structure or functioning of the host. Microorganisms that can cause disease are known as pathogens
The signs of disease are objective and measurable, and can be directly observed by a clinician. Vital signs, which are used to measure the body’s basic functions, include body temperature (normally 37 °C [98.6 °F]), heart rate (normally 60–100 beats per minute), breathing rate (normally 12–18 breaths per minute), and blood pressure (normally between 90/60 and 120/80 mm Hg). Changes in any of the body’s vital signs may be indicative of disease. For example, having a fever (a body temperature significantly higher than 37 °C or 98.6 °F) is a sign of disease because it can be measured.
In addition to changes in vital signs, other observable conditions may be considered signs of disease. For example, the presence of antibodies in a patient’s serum (the liquid portion of blood that lacks clotting factors) can be observed and measured through blood tests and, therefore, can be considered a sign. However, it is important to note that the presence of antibodies is not always a sign of an active disease. Antibodies can remain in the body long after an infection has resolved; also, they may develop in response to a pathogen that is in the body but not currently causing disease.
Unlike signs, symptoms of disease are subjective. Symptoms are felt or experienced by the patient, but they cannot be clinically confirmed or objectively measured. Examples of symptoms include nausea, loss of appetite, and pain. Such symptoms are important to consider when diagnosing disease, but they are subject to memory bias and are difficult to measure precisely. Some clinicians attempt to quantify symptoms by asking patients to assign a numerical value to their symptoms. For example, the Wong-Baker Faces pain-rating scale asks patients to rate their pain on a scale of 0–10. An alternative method of quantifying pain is measuring skin conductance fluctuations. These fluctuations reflect sweating due to skin sympathetic nerve activity resulting from the stressor of pain.
A specific group of signs and symptoms characteristic of a particular disease is called a syndrome. Many syndromes are named using a nomenclature based on signs and symptoms or the location of the disease. Table 7.1 lists some of the prefixes and suffixes commonly used in naming syndromes.
| Suffix / Prefix | Meaning | Example |
|---|---|---|
| cyto – | cells | cytopenia: reduction in the number of blood cells |
| hepat – | of the liver | hepatitis: inflammation of the liver |
| – pathy | disease | neuropathy: a disease affecting nerves |
| – emia | of the blood | bacteremia: presence of bacteria in blood |
| -itis | inflammation | colitis: inflammation of the colon |
| -lysis | destruction | hemolysis: destruction of red blood cells |
| – oma | tumour | lymphoma: cancer of the lymphatic system |
| – osis | diseased or abnormal condition | leukocytosis: abnormally high number of white blood cells |
| – derma | of the skin | keratoderma: a thickening of the skin |
Clinicians must rely on signs and on asking questions about symptoms, medical history, and the patient’s recent activities to identify a particular disease and the potential causative agent. Diagnosis is complicated by the fact that different microorganisms can cause similar signs and symptoms in a patient. For example, an individual presenting with symptoms of diarrhea may have been infected by one of a wide variety of pathogenic microorganisms. Bacterial pathogens associated with diarrheal disease include Vibrio cholerae, Listeria monocytogenes, Campylobacter jejuni, and enteropathogenic Escherichia coli (EPEC). Viral pathogens associated with diarrheal disease include norovirus and rotavirus. Parasitic pathogens associated with diarrhea include Giardia lamblia and Cryptosporidium parvum. Likewise, fever is indicative of many types of infection, from the common cold to the deadly Ebola hemorrhagic fever.
Finally, some diseases may be asymptomatic or subclinical, meaning they do not present any noticeable signs or symptoms. For example, most individual infected with herpes simplex virus remain asymptomatic and are unaware that they have been infected.
Classifications of Diseases: Behavior in a Population: An infectious disease is any disease caused by the direct effect of a pathogen. A pathogen may be cellular (bacteria, parasites, and fungi) or acellular (viruses and prions). Some infectious diseases are also communicable, meaning they are capable of being spread from person to person through either direct or indirect mechanisms. Some infectious communicable diseases are also considered contagious diseases, meaning they are easily spread from person to person. Not all contagious diseases are equally so; the degree to which a disease is contagious usually depends on how the pathogen is transmitted. For example, measles is a highly contagious viral disease that can be transmitted when an infected person coughs or sneezes and an uninfected person breathes in droplets containing the virus. Gonorrhea is not as contagious as measles because transmission of the pathogen (Neisseria gonorrhoeae) requires close intimate contact (usually sexual) between an infected person and an uninfected person.
Certain infectious diseases are not transmitted between humans directly but can be transmitted from animals to humans. Such a disease is called zoonotic disease (or zoonosis). According to WHO, a zoonosis is a disease that occurs when a pathogen is transferred from a vertebrate animal to a human; however, sometimes the term is defined more broadly to include diseases transmitted by all animals (including invertebrates). For example, rabies is a viral zoonotic disease spread from animals to humans through bites and contact with infected saliva.
In contrast to communicable infectious diseases, a noncommunicable infectious disease is not spread from one person to another. One example is tetanus, caused by Clostridium tetani, a bacterium that produces endospores that can survive in the soil for many years. This disease is typically only transmitted through contact with a skin wound; it cannot be passed from an infected person to another person. Similarly, Legionnaires disease is caused by Legionella pneumophila, a bacterium that lives within amoebae in moist locations like water-cooling towers. An individual may contract Legionnaires disease via contact with the contaminated water, but once infected, the individual cannot pass the pathogen to other individuals.
In addition to the wide variety of noncommunicable infectious diseases, noninfectious diseases (those not caused by pathogens) are an important cause of morbidity and mortality worldwide. Noninfectious diseases can be caused by a wide variety factors, including genetics, the environment, or immune system dysfunction, to name a few.
Periods of Disease: The five periods of disease (sometimes referred to as stages or phases) include the incubation, prodromal, illness, decline, and convalescence periods (Figure 7.1). The incubation period occurs in an acute disease after the initial entry of the pathogen into the host (patient). It is during this time the pathogen begins multiplying in the host. However, there are insufficient numbers of pathogen particles (cells or viruses) present to cause signs and symptoms of disease. Incubation periods can vary from a day or two in acute disease to months or years in chronic disease, depending upon the pathogen. Factors involved in determining the length of the incubation period are diverse, and can include strength of the pathogen, strength of the host immune defenses, site of infection, type of infection, and the size infectious dose received. During this incubation period, the patient is unaware that a disease is beginning to develop.
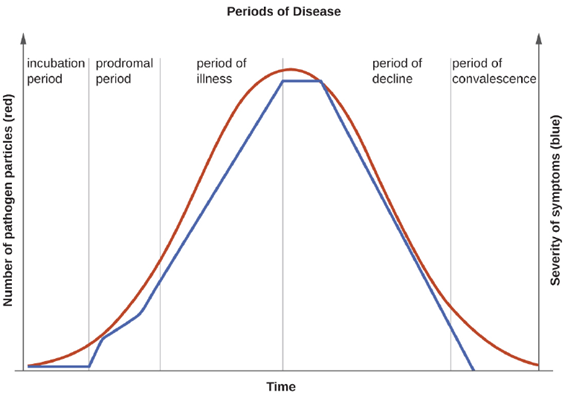
The prodromal period occurs after the incubation period. During this phase, the pathogen continues to multiply and the host begins to experience general signs and symptoms of illness, which typically result from activation of the immune system, such as fever, pain, soreness, swelling, or inflammation. Usually, such signs and symptoms are too general to indicate a particular disease. Following the prodromal period is the period of illness, during which the signs and symptoms of disease are most obvious and severe.
The period of illness is followed by the period of decline, during which the number of pathogen particles begins to decrease, and the signs and symptoms of illness begin to decline. However, during the decline period, patients may become susceptible to developing secondary infections because their immune systems have been weakened by the primary infection. The final period is known as the period of convalescence. During this stage, the patient generally returns to normal functions, although some diseases may inflict permanent damage that the body cannot fully repair.
Infectious diseases can be contagious during all five of the periods of disease. Which periods of disease are more likely to associate with transmissibility of an infection depends upon the disease, the pathogen, and the mechanisms by which the disease develops and progresses. For example, with meningitis (infection of the lining of brain), the periods of infectivity depend on the type of pathogen causing the infection. Patients with bacterial meningitis are contagious during the incubation period for up to a week before the onset of the prodromal period, whereas patients with viral meningitis become contagious when the first signs and symptoms of the prodromal period appear. With many viral diseases associated with rashes (e.g., chickenpox, measles, rubella, roseola), patients are contagious during the incubation period up to a week before the rash develops. In contrast, with many respiratory infections (e.g., colds, influenza, diphtheria, strep throat, and pertussis) the patient becomes contagious with the onset of the prodromal period. Depending upon the pathogen, the disease, and the individual infected, transmission can still occur during the periods of decline, convalescence, and even long after signs and symptoms of the disease disappear. For example, an individual recovering from a diarrheal disease may continue to carry and shed the pathogen in feces for some time, posing a risk of transmission to others through direct contact or indirect contact (e.g., through contaminated objects or food).
Classifications of Diseases: Severity: The duration of the period of illness can vary greatly, depending on the pathogen, effectiveness of the immune response in the host, and any medical treatment received. For an acute disease, pathologic changes occur over a relatively short time (e.g., hours, days, or a few weeks) and involve a rapid onset of disease conditions. For example, influenza (caused by Influenzavirus) is considered an acute disease because the incubation period is approximately 1–2 days. Infected individuals can spread influenza to others for approximately 5 days after becoming ill. After approximately 1 week, individuals enter the period of decline.
For a chronic disease, pathologic changes can occur over longer time spans (e.g., months, years, or a lifetime). For example, chronic gastritis (inflammation of the lining of the stomach) is caused by the gram-negative bacterium Helicobacter pylori. H. pylori is able to colonize the stomach and persist in its highly acidic environment by producing the enzyme urease, which modifies the local acidity, allowing the bacteria to survive indefinitely. Consequently, H. pylori infections can recur indefinitely unless the infection is cleared using antibiotics. Hepatitis B virus can cause a chronic infection in some patients who do not eliminate the virus after the acute illness. A chronic infection with hepatitis B virus is characterized by the continued production of infectious virus for 6 months or longer after the acute infection, as measured by the presence of viral antigen in blood samples.
In latent diseases, as opposed to chronic infections, the causal pathogen goes dormant for extended periods of time with no active replication. Examples of diseases that go into a latent state after the acute infection include herpes (herpes simplex viruses [HSV-1 and HSV-2]), chickenpox (varicella-zoster virus [VZV]), and mononucleosis (Epstein-Barr virus [EBV]). HSV-1, HSV-2, and VZV evade the host immune system by residing in a latent form within cells of the nervous system for long periods of time, but they can reactivate to become active infections during times of stress and immunosuppression. For example, an initial infection by VZV may result in a case of childhood chickenpox, followed by a long period of latency. The virus may reactivate decades later, causing episodes of shingles in adulthood. EBV goes into latency in B cells of the immune system and possibly epithelial cells; it can reactivate years later to produce B-cell lymphoma.
Analyzing Disease in a Population: Analysis of the spread of a disease is always carried out with reference to a population, which is the group of individuals that are at risk for the disease or condition. The population can be defined geographically, but if only a portion of the individuals in that area are susceptible, additional criteria may be required. Susceptible individuals may be defined by particular behaviors, such as intravenous drug use, owning particular pets, or membership in an institution, such as a college. Being able to define the population is important because most measures of interest in epidemiology are made with reference to the size of the population.
The state of being diseased is called morbidity. Morbidity in a population can be expressed in a few different ways. Morbidity or total morbidity is expressed in numbers of individuals without reference to the size of the population. The morbidity rate can be expressed as the number of diseased individuals out of a standard number of individuals in the population, such as 100,000, or as a percent of the population.
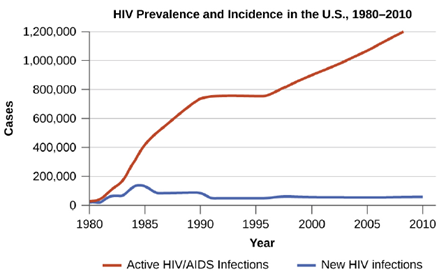
There are two aspects of morbidity that are relevant to an epidemiologist: a disease’s prevalence and its incidence. Prevalence is the number, or proportion, of individuals with a particular illness in a given population at a point in time. For example, the Centers for Disease Control and Prevention (CDC) estimated that in 2012, there were about 1.2 million people 13 years and older with an active human immunodeficiency virus (HIV) infection. Expressed as a proportion, or rate, this is a prevalence of 467 infected persons per 100,000 in the population. On the other hand, incidence is the number or proportion of new cases in a period of time. For the same year and population, the CDC estimates that there were 43,165 newly diagnosed cases of HIV infection, which is an incidence of 13.7 new cases per 100,000 in the population. The relationship between incidence and prevalence can be seen in Figure 7.2. For a chronic disease like HIV infection, prevalence will generally be higher than incidence because it represents the cumulative number of new cases over many years minus the number of cases that are no longer active (e.g., because the patient died or was cured).
In addition to morbidity rates, the incidence and prevalence of mortality (death) may also be reported. A mortality rate can be expressed as the percentage of the population that has died from a disease or as the number of deaths per 100,000 persons (or other suitable standard number).
Classifications of Diseases: Frequency of Occurrence: Diseases that are seen only occasionally, and usually without geographic concentration, are called sporadic diseases. Examples of sporadic diseases include tetanus, rabies, and plague. In the United States, Clostridium tetani, the bacterium that causes tetanus, is ubiquitous in the soil environment, but incidences of infection occur only rarely and in scattered locations because most individuals are vaccinated, clean wounds appropriately, or are only rarely in a situation that would cause infection. Likewise in the United States there are a few scattered cases of plague each year, usually contracted from rodents in rural areas in the western states.
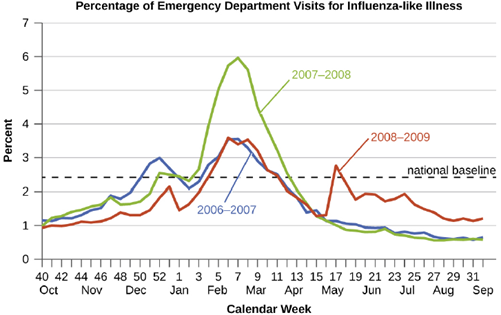
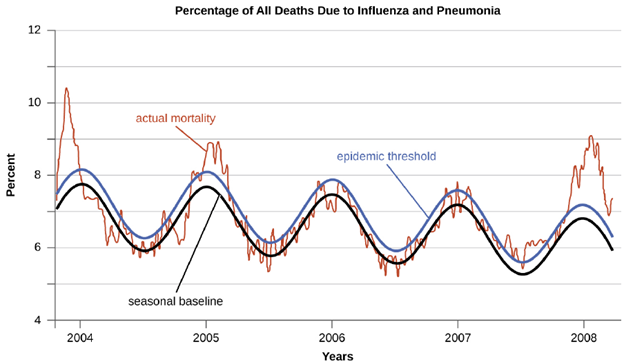
Diseases that are constantly present (often at a low level) in a population within a particular geographic region are called endemic diseases. For example, malaria is endemic to some regions of Brazil, but is not endemic to the United States. Diseases for which a larger than expected number of cases occurs in a short time within a geographic region are called epidemic diseases. Influenza is a good example of a commonly epidemic disease. Incidence patterns of influenza tend to rise each winter in the northern hemisphere. These seasonal increases are expected, so it would not be accurate to say that influenza is epidemic every winter; however, some winters have an unusually large number of seasonal influenza cases in particular regions, and such situations would qualify as epidemics (Figure 7.3 and Figure 7.4).
An epidemic disease signals the breakdown of an equilibrium in disease frequency, often resulting from some change in environmental conditions or in the population. An epidemic that occurs on a worldwide scale is called a pandemic disease. For example, HIV/AIDS is a pandemic disease and novel influenza virus strains often become pandemic.