Unit 9.1: Diseases of the Skin
Outline
Part 1: Anatomy and Normal Microbiota of the Skin
Part 2: Bacterial Infections of the Skin
- Staphylococcal Infections of the Skin
- Superficial Staphylococcal Infections
- Impetigo
- Streptococcal Infections of the Skin
- Necrotizing Fasciitis
- Acne
Learning Objectives
After reading the following, you should be able to:
- Describe the basic structure of the skin, including protective features and defenses.
- Describe features that promote microbial growth and give one example of a bacterial species that is part of the normal flora.
- Describe the general features of infections of the skin including the types of rashes that can result.
- Describe the features of the skin diseases caused by S. aureus, including any specific virulence factors involved.
- Describe the features of the skin diseases caused by S. pyogenes, including any specific virulence factors involved.
- Explain how bacteria can cause acne.
- Compare and contrast infections caused by HSV-1 and HSV-2.
- Describe the causes and symptoms of candidiasis.
- For all the diseases in this section, describe mode of transmission, portal of entry, modes of detection (where discussed) and treatments (in general, e.g. antiviral medication, vaccine, etc)
The human body is covered in skin, and like most coverings, skin is designed to protect what is underneath. One of its primary purposes is to prevent microbes in the surrounding environment from invading underlying tissues and organs. But in spite of its role as a protective covering, skin is not itself immune from infection. Certain pathogens and toxins can cause severe infections or reactions when they come in contact with the skin. Other pathogens are opportunistic, breaching the skin’s natural defenses through cuts, wounds, or a disruption of normal microbiota resulting in an infection in the surrounding skin and tissue. Still other pathogens enter the body via different routes—through the respiratory or digestive systems, for example—but cause reactions that manifest as skin rashes or lesions.
Nearly all humans experience skin infections to some degree. Many of these conditions are, as the name suggests, “skin deep,” with symptoms that are local and non-life-threatening. At some point, almost everyone must endure conditions like acne, athlete’s foot, and minor infections of cuts and abrasions, all of which result from infections of the skin. But not all skin infections are quite so innocuous. Some can become invasive, leading to systemic infection or spreading over large areas of skin, potentially becoming life-threatening.
Part 1: Anatomy and Normal Microbiota of the Skin
Human skin is an important part of the innate immune system. In addition to serving a wide range of other functions, the skin serves as an important barrier to microbial invasion. Not only is it a physical barrier to penetration of deeper tissues by potential pathogens, but it also provides an inhospitable environment for the growth of many pathogens. In this section, we will provide a brief overview of the anatomy and normal microbiota of the skin and eyes, along with general symptoms associated with skin and eye infections.
Layers of the Skin: Human skin is made up of several layers and sub-layers. The two main layers are the epidermis and the dermis. These layers cover a third layer of tissue called the hypodermis, which consists of fibrous and adipose connective tissue (Figure 9.1).
The epidermis is the outermost layer of the skin, and it is relatively thin. The exterior surface of the epidermis, called the stratum corneum, primarily consists of dead skin cells. This layer of dead cells limits direct contact between the outside world and live cells. The stratum corneum is rich in keratin, a tough, fibrous protein that is also found in hair and nails. Keratin helps make the outer surface of the skin relatively tough and waterproof. It also helps to keep the surface of the skin dry, which reduces microbial growth. However, some microbes are still able to live on the surface of the skin, and some of these can be shed with dead skin cells in the process of desquamation, which is the shedding and peeling of skin that occurs as a normal process but that may be accelerated when infection is present.
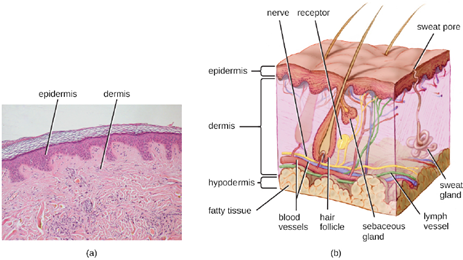
Beneath the epidermis lies a thicker skin layer called the dermis. The dermis contains connective tissue and embedded structures such as blood vessels, nerves, and muscles. Structures called hair follicles (from which hair grows) are located within the dermis, even though much of their structure consists of epidermal tissue. The dermis also contains the two major types of glands found in human skin: sweat glands (tubular glands that produce sweat) and sebaceous glands (which are associated with hair follicles and produce sebum, a lipid-rich substance containing proteins and minerals).
Perspiration (sweat) provides some moisture to the epidermis, which can increase the potential for microbial growth. For this reason, more microbes are found on the regions of the skin that produce the most sweat, such as the skin of the underarms and groin. However, in addition to water, sweat also contains substances that inhibit microbial growth, such as salts, lysozyme, and antimicrobial peptides. Sebum also serves to protect the skin and reduce water loss. Although some of the lipids and fatty acids in sebum inhibit microbial growth, sebum contains compounds that provide nutrition for certain microbes.
Normal Microbiota of the Skin: The skin is home to a wide variety of normal microbiota, consisting of commensal organisms that derive nutrition from skin cells and secretions such as sweat and sebum. The normal microbiota of skin tends to inhibit transient microbe colonization by producing antimicrobial substances and out-competing other microbes that land on the surface of the skin. This helps to protect the skin from pathogenic infection. The skin’s properties differ from one region of the body to another, as does the composition of the skin’s microbiota.
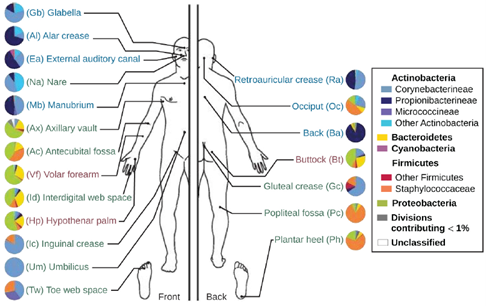
The availability of nutrients and moisture partly dictates which microorganisms will thrive in a particular region of the skin. Relatively moist skin, such as that of the nares (nostrils) and underarms, has a much different microbiota than the dryer skin on the arms, legs, hands, and top of the feet. Some areas of the skin have higher densities of sebaceous glands. These sebum-rich areas, which include the back, the folds at the side of the nose, and the back of the neck, harbor distinct microbial communities that are less diverse than those found on other parts of the body.
Different types of bacteria dominate the dry, moist, and sebum-rich regions of the skin. The most abundant microbes typically found in the dry and sebaceous regions are Betaproteobacteria and Propionibacteria, respectively. In the moist regions, Corynebacterium and Staphylococcus are most commonly found (Figure 9.2). Viruses and fungi are also found on the skin, with Malassezia being the most common type of fungus found as part of the normal microbiota. The role and populations of viruses in the microbiota, known as viromes, are still not well understood, and there are limitations to the techniques used to identify them. However, Circoviridae, Papillomaviridae, and Polyomaviridae appear to be the most common residents in the healthy skin virome.
Infections of the Skin: While the microbiota of the skin can play a protective role, it can also cause harm in certain cases. Often, an opportunistic pathogen residing in the skin microbiota of one individual may be transmitted to another individual more susceptible to an infection. For example, methicillin-resistant Staphylococcus aureus (MRSA) can often take up residence in the nares of health care workers and hospital patients; though harmless on intact, healthy skin, MRSA can cause infections if introduced into other parts of the body, as might occur during surgery or via a post-surgical incision or wound. This is one reason why clean surgical sites are so important.
Injury or damage to the skin can allow microbes to enter deeper tissues, where nutrients are more abundant and the environment is more conducive to bacterial growth. Wound infections are common after a puncture or laceration that damages the physical barrier of the skin. Microbes may infect structures in the dermis, such as hair follicles and glands, causing a localized infection, or they may reach the bloodstream, which can lead to a systemic infection.
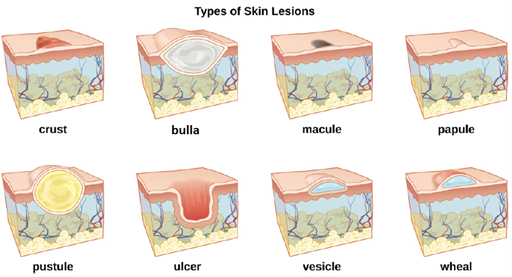
In some cases, infectious microbes can cause a variety of rashes or lesions that differ in their physical characteristics. These rashes can be the result of inflammation reactions or direct responses to toxins produced by the microbes. Table 9.1 lists some of the medical terminology used to describe skin lesions and rashes based on their characteristics; Figure 9.3 and Figure 9.4 illustrate some of the various types of skin lesions. It is important to note that many different diseases can lead to skin conditions of very similar appearance; thus the terms used in the table are generally not exclusive to a particular type of infection or disease.
Table 9.1: Some Medical Terms Associated with Skin Lesions and Rashes
| Term | Definition |
| abscess | localized collection of pus |
| bulla (pl., bullae) | fluid-filled skin lesion larger than 1cm |
| crust | dried fluids from a lesion on the surface of the skin |
| folliculitis | a localized rash due to inflammation of hair follicles |
| furuncle (boil) | pus-filled abscess due to infection of a hair follicle |
| macules | Flat discolored skin lesions |
| papules | small raised skin lesions |
| pustules | Raised, pus-filled skin lesions |
| pyoderma | any suppurative (pus-producing) infection of the skin |
| ulcer | break in the skin; open sore |
| vesicle | small, fluid-filled skin lesion smaller than 1cm |
| wheal | swollen, inflamed skin that itches or burns, such as from an insect bite |
Part 2: Bacterial Infections of the Skin
Despite the skin’s protective functions, infections are common. Gram-positive Staphylococcus spp. and Streptococcus spp. are responsible for many of the most common skin infections. However, many skin conditions are not strictly associated with a single pathogen. Opportunistic pathogens of many types may infect skin wounds, and individual cases with identical symptoms may result from different pathogens or combinations of pathogens.
Staphylococcal Infections of the Skin: Staphylococcus species are commonly found on the skin, with S. epidermidis and S. hominis being prevalent in the normal microbiota. S. aureus is also commonly found in the nasal passages and on healthy skin, but pathogenic strains are often the cause of a broad range of infections of the skin and other body systems.
S. aureus is quite contagious. It is spread easily through skin-to-skin contact, and because many people are chronic nasal carriers (asymptomatic individuals who carry S. aureus in their nares), the bacteria can easily be transferred from the nose to the hands and then to fomites or other individuals. Because it is so contagious, S. aureus is prevalent in most community settings. This prevalence is particularly problematic in hospitals, where antibiotic-resistant strains of the bacteria may be present, and where immunocompromised patients may be more susceptible to infection. Resistant strains include methicillin-resistant S. aureus (MRSA), which can be acquired through healthcare settings (hospital-acquired MRSA, or HA-MRSA) or in the community (community-acquired MRSA, or CAMRSA).
Hospital patients often arrive at health-care facilities already colonized with antibiotic-resistant strains of S. aureus that can be transferred to health-care providers and other patients.
Superficial Staphylococcal Infections: S. aureus is often associated with pyoderma, skin infections that are purulent. Pus formation occurs because many strains of S. aureus produce leukocidins, which kill white blood cells. These purulent skin infections may initially manifest as folliculitis, but can lead to furuncles or deeper abscesses called carbuncles.
Folliculitis generally presents as bumps and pimples that may be itchy, red, and/or pus-filled. If the follicle involved is an eyelash, the infection is called a stye. In some cases, folliculitis is self-limiting, in that it ultimately resolves itself without treatment, but if it continues for more than a few days, worsens, or returns repeatedly, it may require medical treatment. Sweat, skin injuries, ingrown hairs, tight clothing, irritation from shaving, and skin conditions can all contribute to folliculitis. Avoidance of tight clothing and skin irritation can help to prevent infection, but topical antibiotics (and sometimes other treatments) may also help. Folliculitis can be identified by skin inspection; treatment is generally started without first culturing and identifying the causative agent.
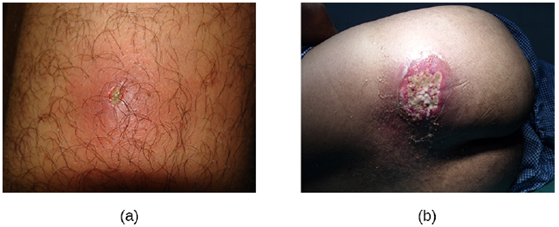
In contrast, furuncles (boils) are deeper infections (Figure 9.5). They are most common in those individuals (especially young adults and teenagers) who play contact sports, share athletic equipment, have poor nutrition, live in close quarters, or have weakened immune systems. Good hygiene and skin care can often help to prevent furuncles from becoming more infective, and they generally resolve on their own. However, if furuncles spread, increase in number or size, or lead to systemic symptoms such as fever and chills, then medical care is needed. They may sometimes need to be drained (at which time the pathogens can be cultured) and treated with antibiotics.
When multiple boils develop into a deeper lesion, it is called a carbuncle (Figure 9.5). Because carbuncles are deeper, they are more commonly associated with systemic symptoms and a general feeling of illness. Larger, recurrent, or worsening carbuncles require medical treatment, as do those associated with signs of illness such as fever. Carbuncles generally need to be drained and treated with antibiotics. While carbuncles are relatively easy to identify visually, culturing and laboratory analysis of the wound may be recommended for some infections because antibiotic resistance is relatively common. Proper hygiene is important to prevent these types of skin infections or to prevent the progression of existing infections.
Staphylococcal scalded skin syndrome (SSSS) is another superficial infection caused by S. aureus that is most commonly seen in young children, especially infants. Bacterial exotoxins first produce erythema (redness of the skin) and then severe peeling of the skin, as might occur after scalding (Figure 9.6). SSSS is diagnosed by examining characteristics of the skin (which may rub off easily), using blood tests to check for elevated white blood cell counts, culturing, and other methods. Intravenous antibiotics and fluid therapy are used as treatment.

Impetigo: The skin infection impetigo causes the formation of vesicles, pustules, and possibly bullae, often around the nose and mouth. Impetigo can be diagnosed as either non-bullous or bullous. In non-bullous impetigo, vesicles and pustules rupture and become encrusted sores. Typically the crust is yellowish, often with exudate draining from the base of the lesion. In bullous impetigo, the bullae fill and rupture, resulting in larger, draining, encrusted lesions (Figure 9.7).
Especially common in children, impetigo is particularly concerning because it is highly contagious. Impetigo can be caused by S. aureus alone, by Streptococcus pyogenes alone, or by coinfection of S. aureus and S. pyogenes. Impetigo is often diagnosed through observation of its characteristic appearance, although culture and susceptibility testing may also be used.
Topical or oral antibiotic treatment is typically effective in treating most cases of impetigo. However, cases caused by S. pyogenes can lead to serious sequelae (pathological conditions resulting from infection, disease, injury, therapy, or other trauma) such as acute glomerulonephritis (AGN), which is severe inflammation in the kidneys.

Streptococcal Infections of the Skin: Streptococcus are gram-positive cocci with a microscopic morphology that resembles chains of bacteria. Colonies are typically small (1–2 mm in diameter), translucent, entire edge, with a slightly raised elevation that can be gamma-hemolytic, alpha-hemolytic, or beta-hemolytic when grown on blood agar. Additionally, they are facultative anaerobes that are catalase-negative.
The most clinically important streptococcal species in humans is S. pyogenes, also known as group A streptococcus (GAS). S. pyogenes produces a variety of extracellular enzymes, including streptolysins O and S, hyaluronidase, and streptokinase. These enzymes can aid in transmission and contribute to the inflammatory response. S. pyogenes also produces a capsule and M protein, a streptococcal cell wall protein. These virulence factors help the bacteria to avoid phagocytosis while provoking a substantial immune response that contributes to symptoms associated with streptococcal infections.
Necrotizing Fasciitis: Streptococcal infections that start in the skin can sometimes spread elsewhere, resulting in a rare but potentially life-threatening condition called necrotizing fasciitis, sometimes referred to as flesh-eating bacterial syndrome. S. pyogenes is one of several species that can cause this rare but potentially-fatal condition.
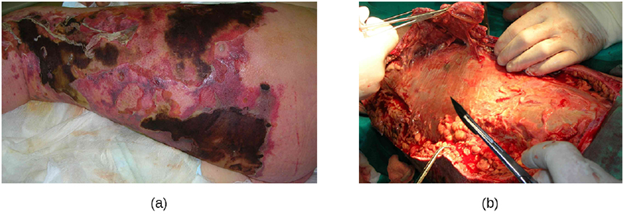
Necrotizing fasciitis occurs when the fascia, a thin layer of connective tissue between the skin and muscle, becomes infected. Severe invasive necrotizing fasciitis due to Streptococcus pyogenes occurs when virulence factors that are responsible for adhesion and invasion overcome host defenses. S. pyogenes adhesins allow bacterial cells to adhere to tissues and establish infection. Bacterial proteases unique to S. pyogenes aggressively infiltrate and destroy host tissues, inactivate complement, and prevent neutrophil migration to the site of infection. The infection and resulting tissue death can spread very rapidly, as large areas of skin become detached and die. Treatment generally requires debridement (surgical removal of dead or infected tissue) or amputation of infected limbs to stop the spread of the infection; surgical treatment is supplemented with intravenous antibiotics and other therapies (Figure 9.8).
Necrotizing fasciitis does not always originate from a skin infection; in some cases there is no known portal of entry. Some studies have suggested that experiencing a blunt force trauma can increase the risk of developing streptococcal necrotizing fasciitis.
: One of the most ubiquitous skin conditions is acne. Acne afflicts nearly 80% of teenagers and young adults, but it can be found in individuals of all ages. Higher incidence among adolescents is due to hormonal changes that can result in overproduction of sebum.
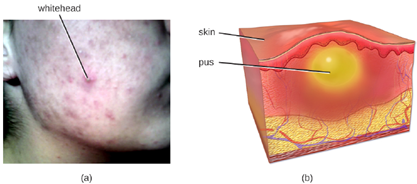
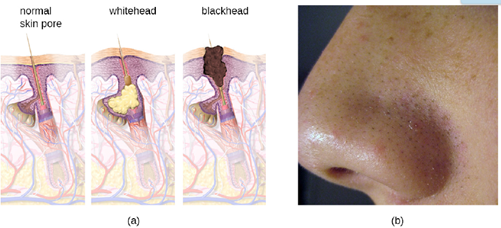
Acne occurs when hair follicles become clogged by shed skin cells and sebum, causing non-inflammatory lesions called comedones. Comedones (singular “comedo”) can take the form of whitehead and blackhead pimples. Whiteheads are covered by skin, whereas blackhead pimples are not; the black color occurs when lipids in the clogged follicle become exposed to the air and oxidize (Figure 9.9).
Often comedones lead to infection by Cutibacterium acnes, a gram-positive, non-spore-forming, aerotolerant anaerobic bacillus found on skin that consumes components of sebum. C. acnes digests triglycerides in the sebum. It uses the glycerol for nutrition and secretes free fatty acids. These fatty acids stimulate inflammatory pathways, causing inflammatory lesions that may include papules, pustules, or nodules, depending on their size and severity.
Treatment of acne depends on the severity of the case. There are multiple ways to grade acne severity, but three levels are usually considered based on the number of comedones, the number of inflammatory lesions, and the types of lesions. Mild acne is treated with topical agents that may include salicylic acid (which helps to remove old skin cells) or retinoids (which have multiple mechanisms, including the reduction of inflammation). Moderate acne may be treated with antibiotics (erythromycin, clindamycin), acne creams (e.g., benzoyl peroxide), and hormones. Severe acne may require treatment using strong medications such as isotretinoin (a retinoid that reduces oil buildup, among other effects, but that also has serious side effects such as photosensitivity). Other treatments, such as phototherapy and laser therapy to kill bacteria and possibly reduce oil production, are also sometimes used.
Part 3: Viral Infections of the Skin
Until recently, it was thought that the normal microbiota of the body consisted primarily of bacteria and some fungi. However, in addition to bacteria, the skin is colonized by viruses, and recent studies suggest that Papillomaviridae, Polyomaviridae and Circoviridae also contribute to the normal skin microbiota. However, some viruses associated with skin are pathogenic, and these viruses can cause diseases with a wide variety of presentations.
Numerous types of viral infections cause rashes or lesions on the skin; however, in many cases these skin conditions result from infections that originate in other body systems. In this chapter, we will limit the discussion to viral skin infections that use the skin as a portal of entry. Later on we will discuss viral infections such as chickenpox and measles, diseases that cause skin rashes but invade the body through portals of entry other than the skin.
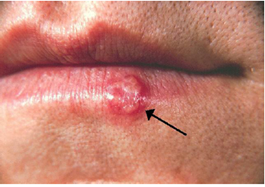
: A common skin virus is herpes simplex virus (HSV). HSV has historically been divided into two types, HSV-1 and HSV-2. HSV-1 is typically transmitted by direct oral contact between individuals, and is usually associated with oral herpes. HSV-2 is usually transmitted sexually and is typically associated with genital herpes. However, both HSV-1 and HSV-2 are capable of infecting any mucous membrane, and the incidence of genital HSV-1 and oral HSV-2 infections has been increasing in recent years.
Infection by HSV-1 commonly manifests as cold sores or fever blisters, usually on or around the lips (Figure 9.10). HSV-1 is highly contagious, with some studies suggesting that up to 65% of the US population is infected; however, many infected individuals are asymptomatic. Moreover, the virus can be latent for long periods, residing in the trigeminal nerve ganglia between recurring bouts of symptoms. Recurrence can be triggered by stress or environmental conditions (systemic or affecting the skin). When lesions are present, they may blister, break open, and crust. The virus can be spread through direct contact, even when a patient is asymptomatic.
HSV-1 infections are commonly diagnosed from their appearance, although laboratory testing can confirm the diagnosis. There is no cure, but antiviral medications such as acyclovir, penciclovir, famciclovir, and valacyclovir are used to reduce symptoms and risk of transmission. Topical medications, such as creams with n-docosanol and penciclovir, can also be used to reduce symptoms such as itching, burning, and tingling.
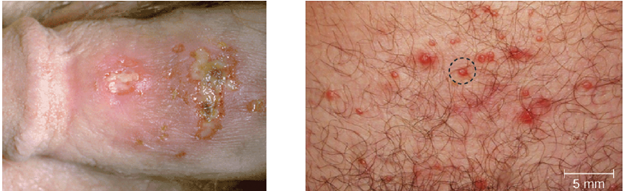
HSV-2 is usually associated with genital herpes. However, both viruses can infect either location as well as other parts of the body. Oral-genital contact can spread either virus from the mouth to the genital region or vice versa.
Many infected individuals do not develop symptoms, and thus do not realize that they carry the virus. However, in some infected individuals, fever, chills, malaise, swollen lymph nodes, and pain precede the development of fluid-filled vesicles that may be irritating and uncomfortable. When these vesicles burst, they release infectious fluid and allow transmission of HSV. In addition, open herpes lesions can increase the risk of spreading or acquiring HIV.
In men, the herpes lesions typically develop on the penis and may be accompanied by a watery discharge. In women, the vesicles develop most commonly on the vulva, but may also develop on the vagina or cervix (Figure 9.11).
The symptoms are typically mild, although the lesions may be irritating or accompanied by urinary discomfort. Use of condoms may not always be an effective means of preventing transmission of genital herpes since the lesions can occur on areas other than the genitals.
Herpes simplex viruses can cause recurrent infections because the virus can become latent and then be reactivated. This occurs more commonly with HSV-2 than with HSV-1.[11] The virus moves down peripheral nerves, typically sensory neurons, to ganglia in the spine (either the trigeminal ganglion or the lumbar-sacral ganglia) and becomes latent. Reactivation can later occur, causing the formation of new vesicles. Not everyone infected with HSV-2 experiences reactivations, which are typically associated with stressful conditions, and the frequency of reactivation varies throughout life and among individuals. Between outbreaks or when there are no obvious vesicles, the virus can still be transmitted.
While there is no cure or vaccine for HSV-2 infections, antiviral medications are available that manage the infection by keeping the virus in its dormant or latent phase, reducing signs and symptoms. If the medication is discontinued, then the condition returns to its original severity.
Many fungal infections of the skin involve fungi that are found in the normal skin microbiota. Some of these fungi can cause infection when they gain entry through a wound; others mainly cause opportunistic infections in immunocompromised patients. Other fungal pathogens primarily cause infection in unusually moist environments that promote fungal growth; for example, sweaty shoes, communal showers, and locker rooms provide excellent breeding grounds that promote the growth and transmission of fungal pathogens.
Tineas: See unit 6 for a discussion of the cutaneous fungal infection known as tineas.
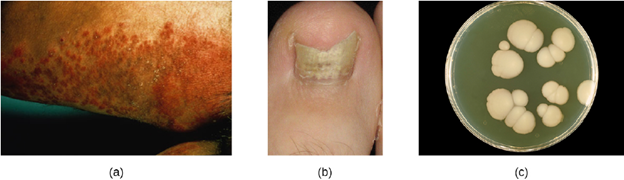
Candidiasis: Candida albicans and other yeasts in the genus Candida can cause skin infections referred to as cutaneous candidiasis. Candida spp. are sometimes responsible for intertrigo, a general term for a rash that occurs in a skin fold, or other localized rashes on the skin. Candida can also infect the nails, causing them to become yellow and harden (Figure 9.12).
Cutaneous candidiasis can be treated with topical or systemic antifungal medications. Because candidiasis can become invasive, patients suffering from HIV/AIDS, cancer, or other conditions that compromise the immune system may benefit from preventive treatment. Repeat infections often occur, but this risk can be reduced by carefully following treatment recommendations, avoiding excessive moisture, maintaining good health, practicing good hygiene, and having appropriate clothing (including footwear).
Candida also causes infections in other parts of the body besides the skin. These include vaginal yeast infections and oral thrush.
As discussed earlier, lactobacilli in the vagina inhibit the growth of other organisms, including bacteria and Candida, but disruptions can allow Candida to increase in numbers. Typical disruptions include antibiotic therapy, illness (especially diabetes), pregnancy, and the presence of transient microbes. Immunosuppression can also play a role, and the severe immunosuppression associated with HIV infection often allows Candida to thrive. This can cause genital or vaginal candidiasis, a condition characterized by vaginitis and commonly known as a yeast infection. When a yeast infection develops, inflammation occurs along with symptoms of pruritus (itching), a thick white or yellow discharge, and odor. Although Candida spp. are found in the normal microbiota, Candida spp. may also be transmitted between individuals. Sexual contact is a common mode of transmission, although candidiasis is not considered an STI.
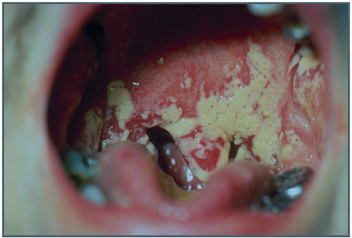
When Candida infection develops in the oral cavity, it is called oral thrush. Oral thrush is most common in infants because they do not yet have well developed immune systems and have not acquired the robust normal microbiota that keeps Candida in check in adults. Oral thrush is also common in immunodeficient patients and is a common infection in patients with AIDS. Oral thrush is characterized by the appearance of white patches and pseudomembranes in the mouth (Figure 9.13) and can be associated with bleeding.