Unit 9.2: Diseases of the Respiratory system
Outline
Part 1: Anatomy and Normal Microbiota of the Respiratory Tract
- Anatomy of the Upper Respiratory System
- Anatomy of the Lower Respiratory System
- Defenses of the Respiratory System
- Normal Microbiota of the Respiratory System
- Signs and Symptoms of Respiratory Infection
Learning Objectives
After reading the following, you should be able to:
- Describe the basic structure of the respiratory system, including protective features and defenses.
- Describe any features that promote microbial growth and give one example of a bacterial species that is part of the normal flora.
- Describe any general features of infections of the respiratory system.
- Describe strep throat, including its causative organism and possible complications.
- Describe bacterial pneumonia and compare and contrast its three main causative species.
- Describe tuberculosis, including its causative organism and possible complications.
- Describe whooping cough, including its causative organism and possible complications.
- Describe the common cold, including its causative organism and possible complications.
- Describe influenza, including its causative organism and possible complications.
- Explain the difference between antigenic shift and antigenic drift
- Describe measles, including its causative organism and possible complications.
- Describe chicken pox, including its causative organism and possible complications.
- Explain the connection between chicken pox and shingles
- For all the diseases in this section, describe mode of transmission, portal of entry, modes of detection (where discussed) and treatments (in general, e.g. antiviral medication, vaccine, etc)
The respiratory tract is one of the main portals of entry into the human body for microbial pathogens. On average, a human takes about 20,000 breaths each day. This roughly corresponds to 10,000 liters, or 10 cubic meters, of air. Suspended within this volume of air are millions of microbes of terrestrial, animal, and human origin—including many potential pathogens. A few of these pathogens will cause relatively mild infections like sore throats and colds. Others, however, are less benign. According to the World Health Organization, respiratory tract infections such as tuberculosis, influenza, and pneumonia were responsible for more than 4 million deaths worldwide in 2012.
At one time, it was thought that antimicrobial drugs and preventive vaccines might hold respiratory infections in check in the developed world, but recent developments suggest otherwise. The rise of multiple-antibiotic resistance in organisms like Mycobacterium tuberculosis has rendered many of our modern drugs ineffective. In addition, there has been a recent resurgence in diseases like whooping cough and measles, once-common childhood illnesses made rare by effective vaccines. Despite advances in medicine and public health programs, it is likely that respiratory pathogens will remain formidable adversaries for the foreseeable future.
Part 1: Anatomy and Normal Microbiota of the Respiratory Tract
The primary function of the respiratory tract is to exchange gases (oxygen and carbon dioxide) for metabolism. However, inhalation and exhalation (particularly when forceful) can also serve as a vehicle of transmission for pathogens between individuals.
Anatomy of the Upper Respiratory System: The respiratory system can be conceptually divided into upper and lower regions at the point of the epiglottis, the structure that seals off the lower respiratory system from the pharynx during swallowing (Figure 9.14). The upper respiratory system is in direct contact with the external environment. The nares (or nostrils) are the external openings of the nose that lead back into the nasal cavity, a large air-filled space behind the nares. These anatomical sites constitute the primary opening and first section of the respiratory tract, respectively. The nasal cavity is lined with hairs that trap large particles, like dust and pollen, and prevent their access to deeper tissues. The nasal cavity is also lined with a mucous membrane and Bowman’s glands that produce mucus to help trap particles and microorganisms for removal. The nasal cavity is connected to several other air-filled spaces. The sinuses, a set of four, paired small cavities in the skull, communicate with the nasal cavity through a series of small openings. The nasopharynx is part of the upper throat extending from the posterior nasal cavity. The nasopharynx carries air inhaled through the nose. The middle ear is connected to the nasopharynx through the eustachian tube. The middle ear is separated from the outer ear by the tympanic membrane, or ear drum. And finally, the lacrimal glands drain to the nasal cavity through the nasolacrimal ducts (tear ducts). The open connections between these sites allow microorganisms to move from the nasal cavity to the sinuses, middle ears (and back), and down into the lower respiratory tract from the nasopharynx.
The oral cavity is a secondary opening for the respiratory tract. The oral and nasal cavities connect through the fauces to the pharynx, or throat. The pharynx can be divided into three regions: the nasopharynx, the oropharynx, and the laryngopharynx. Air inhaled through the mouth does not pass through the nasopharynx; it proceeds first through the oropharynx and then through the laryngopharynx. The palatine tonsils, which consist of lymphoid tissue, are located within the oropharynx. The laryngopharynx, the last portion of the pharynx, connects to the larynx, which contains the vocal fold (Figure 9.14).
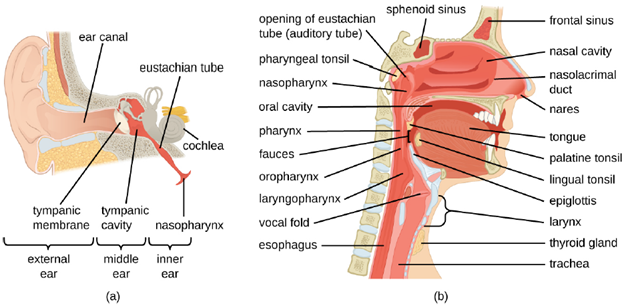
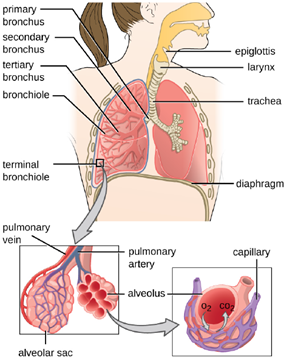
Anatomy of the Lower Respiratory System: The lower respiratory system begins below the epiglottis in the larynx or voice box (Figure 9.14). The trachea, or windpipe, is a cartilaginous tube extending from the larynx that provides an unobstructed path for air to reach the lungs. The trachea bifurcates into the left and right bronchi as it reaches the lungs. These paths branch repeatedly to form smaller and more extensive networks of tubes, the bronchioles. The terminal bronchioles formed in this treelike network end in cul-de-sacs called the alveoli. These structures are surrounded by capillary networks and are the site of gas exchange in the respiratory system. Human lungs contain on the order of 400,000,000 alveoli. The outer surface of the lungs is protected with a double-layered pleural membrane. This structure protects the lungs and provides lubrication to permit the lungs to move easily during respiration.
Defenses of the Respiratory System: The inner lining of the respiratory system consists of mucous membranes and is protected by multiple immune defenses. The goblet cells within the respiratory epithelium secrete a layer of sticky mucus. The viscosity and acidity of this secretion inhibits microbial attachment to the underlying cells. In addition, the respiratory tract contains ciliated epithelial cells. The beating cilia dislodge and propel the mucus, and any trapped microbes, upward to the epiglottis, where they will be swallowed. Elimination of microbes in this manner is referred to as the mucociliary escalator effect and is an important mechanism that prevents inhaled microorganisms from migrating further into the lower respiratory tract.
The upper respiratory system is under constant surveillance by mucosa-associated lymphoid tissue (MALT), including the adenoids and tonsils. Other mucosal defenses include secreted antibodies (IgA), lysozyme, surfactant, and antimicrobial peptides called defensins. Meanwhile, the lower respiratory tract is protected by alveolar macrophages. These phagocytes efficiently kill any microbes that manage to evade the other defenses. The combined action of these factors renders the lower respiratory tract nearly devoid of colonized microbes.
Normal Microbiota of the Respiratory System: The upper respiratory tract contains an abundant and diverse microbiota. The nasal passages and sinuses are primarily colonized by members of the Firmicutes, Actinobacteria, and Proteobacteria. The most common bacteria identified include Staphylococcus epidermidis, viridans group streptococci (VGS), Corynebacterium spp. (diphtheroids), Propionibacterium spp., and Haemophilus spp. The oropharynx includes many of the same isolates as the nose and sinuses, with the addition of variable numbers of bacteria like species of Prevotella, Fusobacterium, Moraxella, and Eikenella, as well as some Candida fungal isolates. In addition, many healthy humans asymptomatically carry potential pathogens in the upper respiratory tract. As much as 20% of the population carry Staphylococcus aureus in their nostrils. The pharynx, too, can be colonized with pathogenic strains of Streptococcus, Haemophilus, and Neisseria.
The lower respiratory tract, by contrast, is scantily populated with microbes. Of the organisms identified in the lower respiratory tract, species of Pseudomonas, Streptococcus, Prevotella, Fusobacterium, and Veillonella are the most common. It is not clear at this time if these small populations of bacteria constitute a normal microbiota or if they are transients.
Signs and Symptoms of Respiratory Infection: Microbial diseases of the respiratory system typically result in an acute inflammatory response. These infections can be grouped by the location affected and have names ending in “itis”, which literally means inflammation of. For instance, rhinitis is an inflammation of the nasal cavities, often characteristic of the common cold. Rhinitis may also be associated with hay fever allergies or other irritants. Inflammation of the sinuses is called sinusitis. Inflammation of the ear is called otitis. Otitis media is an inflammation of the middle ear. A variety of microbes can cause pharyngitis, commonly known as a sore throat. An inflammation of the larynx is called laryngitis. The resulting inflammation may interfere with vocal cord function, causing voice loss. When tonsils are inflamed, it is called tonsillitis. Chronic cases of tonsillitis may be treated surgically with tonsillectomy. More rarely, the epiglottis can be infected, a condition called epiglottitis. In the lower respiratory system, the inflammation of the bronchial tubes results in bronchitis. Most serious of all is pneumonia, in which the alveoli in the lungs are infected and become inflamed. Pus and edema accumulate and fill the alveoli with fluids (called consolidations). This reduces the lungs’ ability to exchange gases and often results in a productive cough expelling phlegm and mucus. Cases of pneumonia can range from mild to life-threatening, and remain an important cause of mortality in the very young and very old.
Part 2: Bacterial Infections of the Respiratory Tract
The respiratory tract can be infected by a variety of bacteria, both gram positive and gram negative. Although the diseases that they cause may range from mild to severe, in most cases, the microbes remain localized within the respiratory system. Fortunately, most of these infections also respond well to antibiotic therapy.
Streptococcal Infections: A common upper respiratory infection, streptococcal pharyngitis (strep throat) is caused by Streptococcus pyogenes. Rebecca Lancefield serologically classified streptococci in the 1930s using carbohydrate antigens from the bacterial cell walls. S. pyogenes is the sole member of the Lancefield group A streptococci and is often referred to as GAS, or group A strep.
Similar to streptococcal infections of the skin, the mucosal membranes of the pharynx are damaged by the release of a variety of exoenzymes and exotoxins by this extracellular pathogen. Many strains of S. pyogenes can degrade connective tissues by using hyaluronidase, collagenase and streptokinase. Streptokinase activates plasmin, which leads to degradation of fibrin and, in turn, dissolution of blood clots, which assists in the spread of the pathogen.
Released toxins include streptolysins that can destroy red and white blood cells. The classic signs of streptococcal pharyngitis are a fever higher than 38 °C (100.4 °F); intense pharyngeal pain; erythema associated with pharyngeal inflammation; and swollen, dark-red palatine tonsils, often dotted with patches of pus; and petechiae (microcapillary hemorrhages) on the soft or hard palate (roof of the mouth) (Figure 9.15). The submandibular lymph nodes beneath the angle of the jaw are also often swollen during strep throat.
S. pyogenes can be easily spread by direct contact or droplet transmission through coughing and sneezing. The disease can be diagnosed quickly using a rapid enzyme immunoassay for the group A antigen. However, due to a significant rate of false-negative results (up to 30%), culture identification is still the gold standard to confirm pharyngitis due to S. pyogenes. S. pyogenes can be identified as a catalase-negative, beta hemolytic bacterium that is susceptible to 0.04 units of bacitracin. Antibiotic resistance is limited for this bacterium, so most β-lactams remain effective; oral amoxicillin and intramuscular penicillin G are those most commonly prescribed.

One reason strep throat infections are aggressively treated with antibiotics is because they can lead to serious sequelae, later clinical consequences of a primary infection. It is estimated that 1%–3% of untreated S. pyogenes infections can be followed by non-suppurative (without the production of pus) sequelae that develop 1–3 weeks after the acute infection has resolved. Two such sequelae are acute rheumatic fever and acute glomerulonephritis.
Acute rheumatic fever can follow pharyngitis caused by specific rheumatogenic strains of S. pyogenes. Although the exact mechanism responsible for this sequela remains unclear, molecular mimicry between the M protein of rheumatogenic strains of S. pyogenes and heart tissue is thought to initiate the autoimmune attack. The most serious and lethal clinical manifestation of rheumatic fever is damage to and inflammation of the heart (carditis). Acute glomerulonephritis also results from an immune response to streptococcal antigens following pharyngitis and cutaneous infections. Acute glomerulonephritis develops within 6–10 days after pharyngitis, but can take up to 21 days after a cutaneous infection. Similar to acute rheumatic fever, there are strong associations between specific nephritogenic strains of S. pyogenes and acute glomerulonephritis, and evidence suggests a role for antigen mimicry and autoimmunity. However, the primary mechanism of acute glomerulonephritis appears to be the formation of immune complexes between S. pyogenes antigens and antibodies, and their deposition between endothelial cells of the glomeruli of kidney. Inflammatory response against the immune complexes leads to damage and inflammation of the glomeruli (glomerulonephritis).
Bacterial Pneumonia: Pneumonia is a general term for infections of the lungs that lead to inflammation and accumulation of fluids and white blood cells in the alveoli. Pneumonia can be caused by bacteria, viruses, fungi, and other organisms, although the vast majority of pneumonias are bacterial in origin. Bacterial pneumonia is a prevalent, potentially serious infection; it caused more 50,000 deaths in the United States in 2014. As the alveoli fill with fluids and white blood cells (consolidation), air exchange becomes impaired and patients experience respiratory distress (Figure 9.16). In addition, pneumonia can lead to pleurisy, an infection of the pleural membrane surrounding the lungs, which can make breathing very painful. Although many different bacteria can cause pneumonia under the right circumstances, three bacterial species cause most clinical cases: Streptococcus pneumoniae, Haemophilus influenzae, and Mycoplasma pneumoniae.
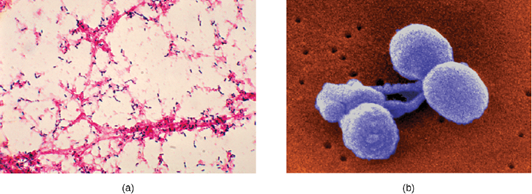
1. Pneumococcal Pneumonia: The most common cause of community-acquired bacterial pneumonia is Streptococcus pneumoniae. This gram-positive, alpha hemolytic streptococcus is commonly found as part of the normal microbiota of the human respiratory tract. The cells tend to be somewhat lancet-shaped and typically appear as pairs (Figure 9.17). The pneumococci initially colonize the bronchioles of the lungs. Eventually, the infection spreads to the alveoli, where the microbe’s polysaccharide capsule interferes with phagocytic clearance. Other virulence factors include autolysins like Lyt A, which degrade the microbial cell wall, resulting in cell lysis and the release of cytoplasmic virulence factors. One of these factors, pneumolysin O, is important in disease progression; this pore-forming protein damages host cells, promotes bacterial adherence, and enhances pro-inflammatory cytokine production. The resulting inflammatory response causes the alveoli to fill with exudate rich in neutrophils and red blood cells. As a consequence, infected individuals develop a productive cough with bloody sputum.
Pneumococci can be presumptively identified by their distinctive gram-positive, lancet-shaped cell morphology and diplococcal arrangement. In blood agar cultures, the organism demonstrates alpha hemolytic colonies that are autolytic after 24 to 48 hours. Antibiotics remain the mainstay treatment for pneumococci. β-Lactams like penicillin are the first-line drugs, but resistance to β-lactams is a growing problem. When β-lactam resistance is a concern, macrolides and fluoroquinolones may be prescribed. There are currently two pneumococcal vaccines available: pneumococcal conjugate vaccine (PCV13) and pneumococcal polysaccharide vaccine (PPSV23). These are generally given to the most vulnerable populations of individuals: children younger than 2 years and adults older than 65 years.
2. Haemophilus Pneumonia: Encapsulated strains of Haemophilus influenzae are known for causing meningitis, but non-encapsulated strains are important causes of pneumonia. This small, gram-negative coccobacillus is found in the pharynx of the majority of healthy children; however, Haemophilus pneumonia is primarily seen in the elderly. Like other pathogens that cause pneumonia, H. influenzae is spread by droplets and aerosols produced by coughing. A fastidious organism, H. influenzae will only grow on media with available factor X (hemin) and factor V (NAD), like chocolate agar. Serotyping must be performed to confirm identity of H. influenzae isolates.
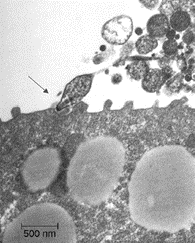
3. Mycoplasma Pneumonia (Walking Pneumonia): Primary atypical pneumonia is caused by Mycoplasma pneumoniae. This bacterium is not part of the respiratory tract’s normal microbiota and can cause epidemic disease outbreaks. Also known as walking pneumonia, Mycoplasma pneumonia infections are common in crowded environments like college campuses and military bases. It is spread by aerosols formed when coughing or sneezing. The disease is often mild, with a low fever and persistent cough. These bacteria, which do not have cell walls, use a specialized attachment organelle to bind to ciliated cells. In the process, epithelial cells are damaged and the proper function of the cilia is hindered (Figure 9.18).
Mycoplasma grow very slowly when cultured. Therefore, penicillin and thallium acetate are added to agar to prevent the overgrowth by faster-growing potential contaminants. Since M. pneumoniae does not have a cell wall, it is resistant to these substances. Without a cell wall, the microbial cells appear pleomorphic. M. pneumoniae infections tend to be self-limiting, in that it ultimately resolves itself without treatment, but may also respond well to macrolide antibiotic therapy. β-lactams, which target cell wall synthesis, cannot be used for treatment of infections with this pathogen.
Tuberculosis: Tuberculosis (TB) is one of the deadliest infectious diseases in human history. Although tuberculosis infection rates in the United States are extremely low, the CDC estimates that about one-third of the world’s population is infected with Mycobacterium tuberculosis, the causal organism of TB, with 9.6 million new TB cases and 1.5 million deaths worldwide in 2014.
M. tuberculosis is an acid-fast, gram-positive, nonspore-forming rod. Its cell wall is rich in waxy mycolic acids, which make the cells impervious to polar molecules (this prevents proper gram staining, so other methods must be used). It also causes these organisms to grow slowly. M. tuberculosis causes a chronic granulomatous disease that can infect any area of the body, although it is typically associated with the lungs. M. tuberculosis is spread by inhalation of respiratory droplets or aerosols from an infected person. The infectious dose (ID50) of M. tuberculosis is only 10 cells.
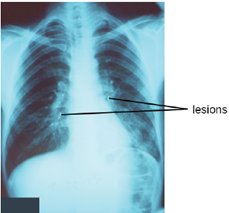
After inhalation, the bacteria enter the alveoli (Figure 9.19). The cells are phagocytized by macrophages but can survive and multiply within these phagocytes because of the protection by the waxy mycolic acid in their cell walls. If not eliminated by macrophages, the infection can progress, causing an inflammatory response and an accumulation of neutrophils and macrophages in the area. Several weeks or months may pass before an immunological response is mounted by T cells and B cells. Eventually, the lesions in the alveoli become walled off, forming small round lesions called tubercles. Bacteria continue to be released into the center of the tubercles and the chronic immune response results in tissue damage and induction of apoptosis (programmed host-cell death) in a process called liquefaction.
This creates a caseous center, or air pocket, where the aerobic M. tuberculosis can grow and multiply. Tubercles may eventually rupture and bacterial cells can invade pulmonary capillaries; from there, bacteria can spread through the bloodstream to other organs, a condition known as miliary tuberculosis. The rupture of tubercles also facilitates transmission of the bacteria to other individuals via droplet aerosols that exit the body in coughs. Because these droplets can be very small and stay aloft for a long time, special precautions are necessary when caring for patients with TB, such as the use of face masks and negative-pressure ventilation and filtering systems.
Eventually, most lesions heal to form calcified Ghon complexes. These structures are visible on chest radiographs and are a useful diagnostic feature. But even after the disease has apparently ended, viable bacteria remain sequestered in these locations. Release of these organisms at a later time can produce reactivation tuberculosis (or secondary TB). This is mainly observed in people with alcoholism, the elderly, or in otherwise immunocompromised individuals.
Because TB is a chronic disease, chemotherapeutic treatments often continue for months or years. Multidrug resistant (MDR-TB) and extensively drug-resistant (XDR-TB) strains of M. tuberculosis are a growing clinical concern. These strains can arise due to misuse or mismanagement of antibiotic therapies. Therefore, it is imperative that proper multidrug protocols are used to treat these infections. Common antibiotics included in these mixtures are isoniazid, rifampin, ethambutol, and pyrazinamide.
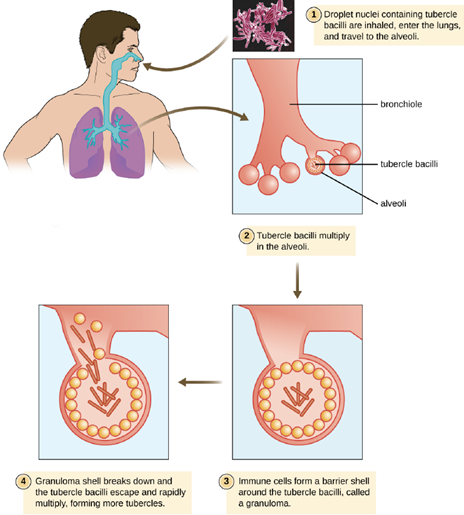
(approximately 90%) results in the formation of tubercles in which the infection is walled off. The remainder will suffer progressive primary tuberculosis. The sequestered bacteria may be reactivated to form secondary tuberculosis in immunocompromised patients at a later time. (credit: modification of work by Centers for Disease Control and Prevention)
A TB vaccine is available that is based on the so-called bacillus Calmette-Guérin (BCG) strain of M. bovis commonly found in cattle. In the United States, the BCG vaccine is only given to health-care workers and members of the military who are at risk of exposure to active cases of TB. It is used more broadly worldwide. Many individuals born in other countries have been vaccinated with BCG strain. BCG is used in many countries with a high prevalence of TB, to prevent childhood tuberculous meningitis and miliary disease.
The Mantoux tuberculin skin test (Figure 9.20) is regularly used in the United States to screen for potential TB exposure. However, prior vaccinations with the BCG vaccine can cause false-positive results. Chest radiographs to detect Ghon complex formation are required, therefore, to confirm exposure.

Pertussis (Whooping Cough): The causative agent of pertussis, commonly called whooping cough, is Bordetella pertussis, a gram-negative coccobacillus. The disease is characterized by mucus accumulation in the lungs that leads to a long period of severe coughing. Sometimes, following a bout of coughing, a sound resembling a “whoop” is produced as air is inhaled through the inflamed and restricted airway—hence the name whooping cough. Although adults can be infected, the symptoms of this disease are most pronounced in infants and children. Pertussis is highly communicable through droplet transmission, so the uncontrollable coughing produced is an efficient means of transmitting the disease in a susceptible population.
Following inhalation, B. pertussis specifically attaches to epithelial cells using an adhesin, filamentous
hemagglutinin. The bacteria then grow at the site of infection and cause disease symptoms through the production of exotoxins. One of the main virulence factors of this organism is an A-B exotoxin called the pertussis toxin (PT). PT is known to enhance inflammatory responses involving histamine and serotonin. In addition to PT, B. pertussis produces a tracheal cytotoxin that damages ciliated epithelial cells and results in accumulation of mucus in the lungs, due to the disruption of the mucociliary escalator. The mucus can support the colonization and growth of other microbes and, as a consequence, secondary infections are common. Together, the effects of these factors produce the cough that characterizes this infection.
A pertussis infection can be divided into three distinct stages. The initial infection, termed the catarrhal stage, is relatively mild and unremarkable. The signs and symptoms may include nasal congestion, a runny nose, sneezing, and a low-grade fever. This, however, is the stage in which B. pertussis is most infectious. In the paroxysmal stage, mucus accumulation leads to uncontrollable coughing spasms that can last for several minutes and frequently induce vomiting. The paroxysmal stage can last for several weeks. A long convalescence stage follows the paroxysmal stage, during which time patients experience a chronic cough that can last for up to several months. In fact, the disease is sometimes called the 100-day cough. In infants, coughing can be forceful enough to cause fractures to the ribs, and prolonged infections can lead to death. The CDC reported 20 pertussis-related deaths in 2012, but that number had declined to five by 2015.
During the first 2 weeks of infection, laboratory diagnosis is best performed by culturing the organism directly from a nasopharyngeal (NP) specimen collected from the posterior nasopharynx. Pertussis is generally a self-limiting disease. Antibiotic therapy with erythromycin or tetracycline is only effective at the very earliest stages of disease. Antibiotics given later in the infection, and prophylactically to uninfected individuals, reduce the rate of transmission. Active vaccination is a better approach to control this disease. The DPT vaccine was once in common use in the United States. In that vaccine, the P component consisted of killed whole-cell B. pertussis preparations. Because of some adverse effects, that preparation has now been superseded by the DTaP and Tdap vaccines. In both of these new vaccines, the “aP” component is a pertussis toxoid.
Part 3: Viral Infections of the Respiratory Tract
Viruses are the most frequent cause of respiratory tract infections. Unlike the bacterial pathogens, we have few effective therapies to combat viral respiratory infections. Fortunately, many of these diseases are mild and self-limiting. A few respiratory infections manifest their primary symptoms at other locations in the body.
The Common Cold: The common cold is a generic term for a variety of mild viral infections of the nasal cavity. More than 200 different viruses are known to cause the common cold. The most common groups of cold viruses include rhinoviruses, coronaviruses, and adenoviruses. These infections are widely disseminated in the human population and are transmitted through direct contact and droplet transmission. Coughing and sneezing efficiently produce infectious aerosols, and rhinoviruses are known to persist on environmental surfaces for up to a week.
Viral contact with the nasal mucosa or eyes can lead to infection. Rhinoviruses tend to replicate best between 33 °C (91.4 °F) and 35 °C (95 °F), somewhat below normal body temperature (37 °C [98.6 °F]). As a consequence, they tend to infect the cooler tissues of the nasal cavities. Colds are marked by an irritation of the mucosa that leads to an inflammatory response. This produces common signs and symptoms such as nasal excess nasal secretions (runny nose), congestion, sore throat, coughing, and sneezing. The absence of high fever is typically used to differentiate common colds from other viral infections, like influenza. Some colds may progress to cause otitis media, pharyngitis, or laryngitis, and patients may also experience headaches and body aches. The disease, however, is self-limiting and typically resolves within 1–2 weeks.
There are no effective antiviral treatments for the common cold and antibacterial drugs should not be prescribed unless secondary bacterial infections have been established. Many of the viruses that cause colds are related, so immunity develops throughout life. Given the number of viruses that cause colds, however, individuals are never likely to develop immunity to all causes of the common cold.
Influenza: Commonly known as the flu, influenza is a common viral disease of the lower respiratory system. Influenza is pervasive worldwide and causes 3,000–50,000 deaths each year in the United States. The annual mortality rate can vary greatly depending on the virulence of the strain(s) responsible for seasonal epidemics.
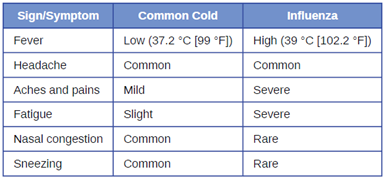
Influenza infections are most typically characterized by fever, chills, and body aches. This is followed by symptoms similar to the common cold that may last a week or more. Table 9.1 compares the signs and symptoms of influenza and the common cold.
In general, influenza is self-limiting. However, serious cases can lead to pneumonia and other complications that can be fatal. Such cases are more common in the very young and the elderly; however, certain strains of influenza virus are more lethal to young adults than to the very young or old. Strains that affect young adults are believed to involve a cytokine storm—a positive feedback loop that forms between cytokine production and leukocytes. This cytokine storm produces an acute inflammatory response that leads to rapid fluid accumulation in the lungs, culminating in pulmonary failure. In such cases, the ability to mount a vigorous immune response is actually detrimental to the patient. The very young and very old are less susceptible to this effect because their immune systems are less robust.
A complication of influenza that occurs primarily in children and teenagers is Reye syndrome. This sequela causes swelling in the liver and brain, and may progress to neurological damage, coma, or death. Reye syndrome may follow other viral infections, like chickenpox, and has been associated with the use of aspirin. For this reason, the CDC and other agencies recommend that aspirin and products containing aspirin never be used to treat viral illnesses in children younger than age 19 years.
The influenza virus is primarily transmitted by direct contact and inhalation of aerosols. The RNA genome of this virus exists as seven or eight segments, each coated with ribonucleoprotein and encoding one or two specific viral proteins. The influenza virus is surrounded by a lipid membrane envelope, and two of the main antigens of the influenza virus are the spike proteins hemagglutinin (H) and neuraminidase (N), as shown in Figure 9.21. These spike proteins play important roles in the viral infectious cycle.
Following inhalation, the influenza virus uses the hemagglutinin protein to bind to sialic acid receptors on host respiratory epithelial cells. This facilitates endocytosis of the viral particle. Once inside the host cell, the negative strand viral RNA is replicated by the viral RNA polymerase to form mRNA, which is translated by the host to produce viral proteins. Additional viral RNA molecules are transcribed to produce viral genomic RNA, which assemble with viral proteins to form mature virions. Release of the virions from the host cell is facilitated by viral neuraminidase, which cleaves sialic-acid receptors to allow progeny viruses to make a clean exit when budding from an infected cell.
There are three genetically related influenza viruses, called A, B, and C. The influenza A viruses have different subtypes based on the structure of their hemagglutinin and neuraminidase proteins. There are currently 18 known subtypes of hemagglutinin and 11 known subtypes of neuraminidase. Influenza viruses are serologically characterized by the type of H and N proteins that they possess. Of the nearly 200 different combinations of H and N, only a few, such as the H1N1 strain, are associated with human disease. The influenza viruses A, B, and C make up three of the five major groups of orthomyxoviruses.
The most virulent group is the influenza A viruses, which cause seasonal pandemics of influenza each year. Influenza A virus can infect a variety of animals, including pigs, horses, pigs, and even whales and dolphins. Influenza B virus is less virulent and is sometimes associated with epidemic outbreaks. Influenza C virus generally produces the mildest disease symptoms and is rarely connected with epidemics. Neither influenza B virus nor influenza C virus has significant animal reservoirs.
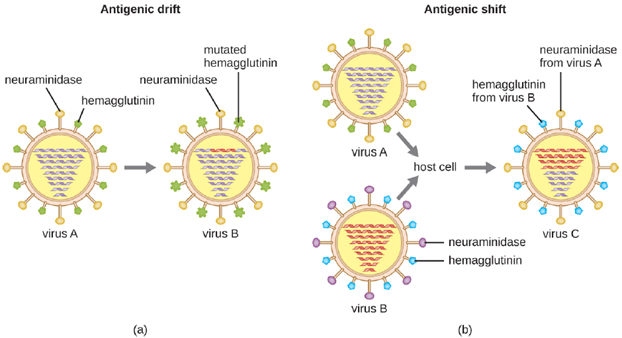
Influenza virus infections elicit a strong immune response, particularly to the hemagglutinin protein, which would protect the individual if they encountered the same virus. Unfortunately, the antigenic properties of the virus change relatively rapidly, so new strains are evolving that immune systems previously challenged by influenza virus cannot recognize. When an influenza virus gains a new hemagglutinin or neuraminidase type, it is able to evade the host’s immune response and be successfully transmitted, often leading to an epidemic.
There are two mechanisms by which these evolutionary changes may occur: antigenic drift and antigenic shift (Figure 9.22). Antigenic drift is the result of point mutations causing slight changes in the spike proteins hemagglutinin (H) and neuraminidase (N). On the other hand, antigenic shift is a major change in spike proteins due to gene reassortment. This reassortment for antigenic shift occurs typically when two different influenza viruses infect the same host.
The rate of antigenic variation in influenza viruses is very high, making it difficult for the immune system to recognize the many different strains of Influenzavirus. Although the body may develop immunity to one strain through natural exposure or vaccination, antigenic variation results in the continual emergence of new strains that the immune system will not recognize. This is the main reason that vaccines against Influenzavirus must be given annually. Each year’s influenza vaccine provides protection against the most prevalent strains for that year, but new or different strains may be more prevalent the following year.
Three drugs that inhibit influenza neuraminidase activity are available: inhaled zanamivir, oral oseltamivir, and intravenous peramivir. If taken at the onset of symptoms, these drugs can shorten the course of the disease. These drugs are thought to impair the ability of the virus to efficiently exit infected host cells. A more effective means of controlling influenza outbreaks, though, is vaccination. Every year, new influenza vaccines are developed to be effective against the strains expected to be predominant. This is determined in February by a review of the dominant strains around the world from a network of reporting sites; their reports are used to generate a recommendation for the vaccine combination for the following winter in the northern hemisphere. In September, a similar recommendation is made for the winter in the southern hemisphere. These recommendations are used by vaccine manufacturers to formulate each year’s vaccine. In most cases, three or four viruses are selected—the two most prevalent influenza A strains and one or two influenza B strains. The chosen strains are typically cultivated in eggs and used to produce either an inactivated or a live attenuated vaccine (e.g., FluMist). For individuals 18 years or older with an allergy to egg products, a recombinant egg-free trivalent vaccine is available. Most of the influenza vaccines over the past decade have had an effectiveness of about 50%.
Viral Pneumonia: Viruses cause fewer cases of pneumonia than bacteria; however, several viruses can lead to pneumonia in children and the elderly. The most common sources of viral pneumonia are adenoviruses, influenza viruses, parainfluenza viruses, and respiratory syncytial viruses. The signs and symptoms produced by these viruses can range from mild cold-like symptoms to severe cases of pneumonia, depending on the virulence of the virus strain and the strength of the host defenses of the infected individual. Occasionally, infections can result in otitis media (ear infections).
Viral Respiratory Diseases Causing Skin Rashes: Measles and chickenpox are two important viral diseases often associated with skin rashes. However, their symptoms are systemic, and because their portal of entry is the respiratory tract, they can be considered respiratory infections.
Measles (Rubeola): The measles virus (MeV) causes the highly contagious disease measles, also known as rubeola, which is a major cause of childhood mortality worldwide. Although vaccination efforts have greatly reduced the incidence of measles in much of the world, epidemics are still common in unvaccinated populations in certain countries.
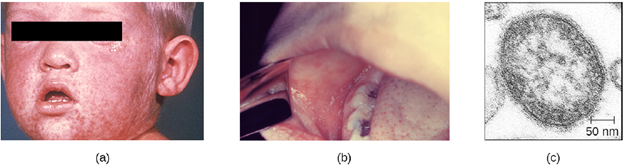
The measles virus is a single-stranded, negative-strand RNA virus and, like the influenza virus, it possesses an envelope with spikes of embedded hemagglutinin. The infection is spread by direct contact with infectious secretions or inhalation of airborne droplets spread by breathing, coughing, or sneezing. Measles is initially characterized by a high fever, conjunctivitis, and a sore throat. The virus then moves systemically through the bloodstream and causes a characteristic rash. The measles rash initially forms on the face and later spreads to the extremities. The red, raised macular rash will eventually become confluent and can last for several days. At the same time, extremely high fevers (higher than 40.6 °C [105 °F]) can occur. Another diagnostic sign of measles infections is Koplik’s spots, white spots that form on the inner lining of inflamed cheek tissues (Figure 9.23).
Although measles is usually self-limiting, it can lead to pneumonia, encephalitis, and death. In addition, the inhibition of immune system cells by the measles virus predisposes patients to secondary infections. In severe infections with highly virulent strains, measles fatality rates can be as high as 10% to 15%. There were more than 145,000 measles deaths (mostly young children) worldwide in 2013.
There are no effective treatments for measles. Vaccination is widespread in developed countries as part of the measles, mumps, and rubella (MMR) vaccine. As a result, there are typically fewer than 200 cases of measles in the United States annually. When it is seen, it is often associated with children who have not been vaccinated.
Chickenpox and Shingles: Chickenpox, also known as varicella, was once a common viral childhood disease. The causative agent of chickenpox, the varicella-zoster virus, is a member of the herpesvirus family. In children, the disease is mild and self-limiting, and is easily transmitted by direct contact or inhalation of material from the skin lesions. In adults, however, chickenpox infections can be much more severe and can lead to pneumonia and birth defects in the case of infected pregnant women. Reye syndrome, mentioned earlier, is also a serious complication associated with chickenpox, generally in children.
Once infected, most individuals acquire a lifetime immunity to future chickenpox outbreaks. For this reason, parents once held “chickenpox parties” for their children. At these events, uninfected children were intentionally exposed to an infected individual so they would contract the disease earlier in life, when the incidence of complications is very low, rather than risk a more severe infection later.
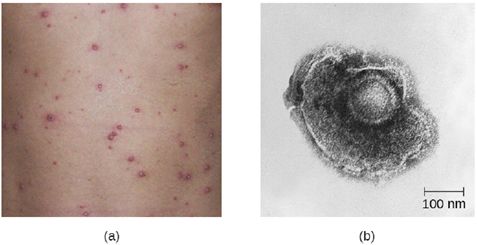
After the initial viral exposure, chickenpox has an incubation period of about 2 weeks. The initial infection of the respiratory tract leads to viremia and eventually produces fever and chills. A pustular rash then develops on the face, progresses to the trunk, and then the extremities, although most form on the trunk (Figure 9.24). Eventually, the lesions burst and form a crusty scab. Individuals with chickenpox are infectious from about 2 days before the outbreak of the rash until all the lesions have scabbed over.
Like other herpesviruses, the varicella-zoster virus can become dormant in nerve cells. While the pustular vesicles are developing, the virus moves along sensory nerves to the dorsal ganglia in the spinal cord. Once there, the varicella-zoster virus can remain latent for decades. These dormant viruses may be reactivated later in life by a variety of stimuli, including stress, aging, and immunosuppression. Once reactivated, the virus moves along sensory nerves to the skin of the face or trunk. This results in the production of the painful lesions in a condition known as shingles (Figure 9.25). These symptoms generally last for 2–6 weeks, and may recur more than once. Postherpetic neuralgia, pain signals sent from damaged nerves long after the other symptoms have subsided, is also possible. In addition, the virus can spread to other organs in immunocompromised individuals. A person with shingles lesions can transmit the virus to a non-immune contact, and the newly infected individual would develop chickenpox as the primary infection. Shingles cannot be transmitted from one person to another.

Treatment for chickenpox infections in children is usually not required. In patients with shingles, acyclovir treatment can often reduce the severity and length of symptoms, and diminish the risk of postherpetic neuralgia. An effective vaccine is now available for chickenpox. A vaccine is also available for adults older than 60 years who were infected with chickenpox in their youth. This vaccine reduces the likelihood of a shingles outbreak by boosting the immune defenses that are keeping the latent infection in check and preventing reactivation.
