Unit 9.3: Diseases of the Circulatory and Lymphatic Systems
Outline
Part 1: Anatomy of the Circulatory and Lymphatic Systems
Infections of the Circulatory System
Infections of the Lymphatic System
Part 2: Bacterial Infections of the Circulatory and Lymphatic Systems
Part 3: Viral Infections of the Circulatory and Lymphatic Systems
Part 4: Helminths Infections of the of the Circulatory and Lymphatic Systems
Learning Objectives
After reading the following, you should be able to:
- Describe the basic structure of the circulatory and lymphatic systems, including protective features and defenses.
- Describe any general features of infections of the circulatory and lymphatic systems.
- Describe toxic shock syndrome, including its causative organism and possible complications.
- Describe gas gangrene, including its causative organism and possible complications.
- Describe infectious mononucleosis, including its causative organism and possible complications.
- Describe the features of a Hantavirus infection, including any possible complications.
- Describe the features of an HIV, including any possible complications.
- Describe lymphatic filariasis, including its most common causative organism and possible complications.
- For all the diseases in this section, describe mode of transmission, portal of entry, modes of detection (where discussed) and treatments (in general, e.g. antiviral medication, vaccine, etc)
Yellow fever was once common in the southeastern US, with annual outbreaks of more than 25,000 infections in New Orleans in the mid-1800s. In the early 20th century, efforts to eradicate the virus that causes yellow fever were successful thanks to vaccination programs and effective control (mainly through the insecticide dichlorodiphenyltrichloroethane [DDT]) of Aedes aegypti, the mosquito that serves as a vector. Today, the virus has been largely eradicated in North America.
Like yellow fever, many of the circulatory and lymphatic diseases discussed in this chapter are emerging or reemerging worldwide. Despite medical advances, diseases like malaria, Ebola, and others could become endemic in the US given the right circumstances.
Part 1: Anatomy of the Circulatory and Lymphatic Systems
The circulatory and lymphatic systems are networks of vessels and a pump that transport blood and lymph, respectively, throughout the body. When these systems are infected with a microorganism, the network of vessels can facilitate the rapid dissemination of the microorganism to other regions of the body, sometimes with serious results. In this section, we will review some of the key anatomical features of the circulatory and lymphatic systems, as well as general signs and symptoms of infection.
The Circulatory System: The circulatory (or cardiovascular) system is a closed network of organs and vessels that moves blood around the body (Figure 9.26). The primary purposes of the circulatory system are to deliver nutrients, immune factors, and oxygen to tissues and to carry away waste products for elimination. The heart is a four-chambered pump that propels the blood throughout the body. Deoxygenated blood enters the right atrium through the superior vena cava and the inferior vena cava after returning from the body. The blood next passes through the tricuspid valve to enter the right ventricle. When the heart contracts, the blood from the right ventricle is pumped through the pulmonary arteries to the lungs. There, the blood is oxygenated at the alveoli and returns to the heart through the pulmonary veins. The oxygenated blood is received at the left atrium and proceeds through the mitral valve to the left ventricle. When the heart contracts, the oxygenated blood is pumped throughout the body via a series of thick-walled vessels called arteries. The first and largest artery is called the aorta. The arteries sequentially branch and decrease in size (and are called arterioles) until they end in a network of smaller vessels called capillaries. The capillary beds are located in the interstitial spaces within tissues and release nutrients, immune factors, and oxygen to those tissues. The capillaries connect to a series of vessels called venules, which increase in size to form the veins. The veins join together into larger vessels as they transfer blood back to the heart. The largest veins, the superior and inferior vena cava, return the blood to the right atrium.
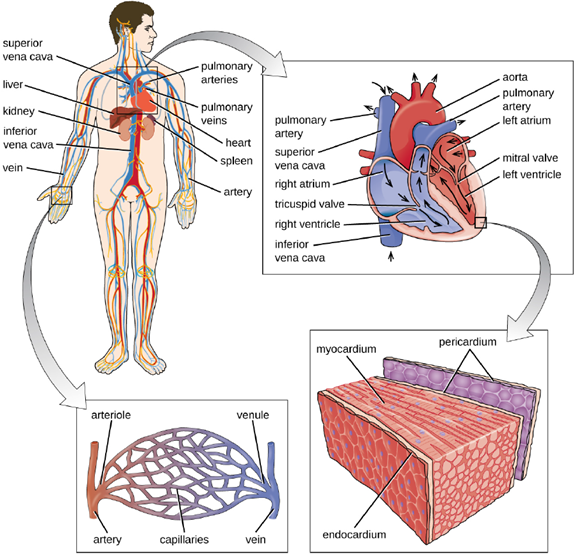
Other organs play important roles in the circulatory system as well. The kidneys filter the blood, removing waste products and eliminating them in the urine. The liver also filters the blood and removes damaged or defective red blood cells. The spleen filters and stores blood, removes damaged red blood cells, and is a reservoir for immune factors. All of these filtering structures serve as sites for entrapment of microorganisms and help maintain an environment free of microorganisms in the blood.
The Lymphatic System: The lymphatic system is also a network of vessels that run throughout the body (Figure 9.27). However, these vessels do not form a full circulating system and are not pressurized by the heart. Rather, the lymphatic system is an open system with the fluid moving in one direction from the extremities toward two drainage points into veins just above the heart. Lymphatic fluids move more slowly than blood because they are not pressurized. Small lymph capillaries interact with blood capillaries in the interstitial spaces in tissues. Fluids from the tissues enter the lymph capillaries and are drained away. These fluids, termed lymph, also contain large numbers of white blood cells.
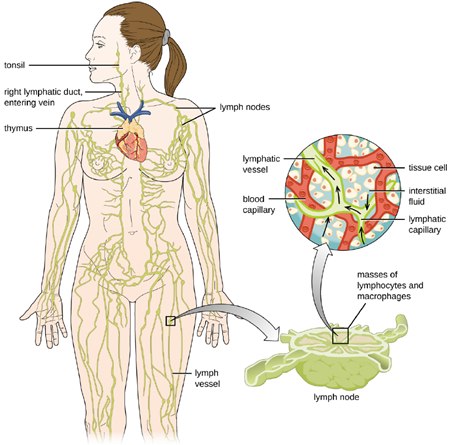
Recall that the lymphatic system contains two types of lymphoid tissues. The primary lymphoid tissue includes bone marrow and the thymus. Bone marrow contains the hematopoietic stem cells (HSC) that differentiate and mature into the various types of blood cells and lymphocytes. The secondary lymphoid tissues include the spleen, lymph nodes, and several areas of diffuse lymphoid tissues underlying epithelial membranes. The spleen, an encapsulated structure, filters blood and captures pathogens and antigens that pass into it. The spleen contains specialized macrophages and dendritic cells that are crucial for antigen presentation, a mechanism critical for activation of T lymphocytes and B lymphocytes.
Lymph nodes are bean-shaped organs situated throughout the body. These structures contain areas called germinal centers that are rich in B and T lymphocytes. The lymph nodes also contain macrophages and dendritic cells for antigen presentation. Lymph from nearby tissues enters the lymph node through afferent lymphatic vessels and encounters these lymphocytes as it passes through; the lymph exits the lymph node through the efferent lymphatic vessels.
Infections of the Circulatory System: Under normal circumstances, the circulatory system and the blood should be sterile; the circulatory system has no normal microbiota. Because the system is closed, there are no easy portals of entry into the circulatory system for microbes. Those that are able to breach the body’s physical barriers and enter the bloodstream encounter a host of circulating immune defenses, such as antibodies, complement proteins, phagocytes, and other immune cells. Microbes often gain access to the circulatory system through a break in the skin (e.g., wounds, needles, intravenous catheters, insect bites) or spread to the circulatory system from infections in other body sites. For example, microorganisms causing pneumonia or renal infection may enter the local circulation of the lung or kidney and spread from there throughout the circulatory network.
If microbes in the bloodstream are not quickly eliminated, they can spread rapidly throughout the body, leading to serious, even life-threatening infections. Various terms are used to describe conditions involving microbes in the circulatory system. The term bacteremia refers to bacteria in the blood. If bacteria are reproducing in the blood as they spread, this condition is called septicemia. The presence of viruses in the blood is called viremia. Microbial toxins can also be spread through the circulatory system, causing a condition termed toxemia.
Microbes and microbial toxins in the blood can trigger an inflammatory response so severe that the inflammation damages host tissues and organs more than the infection itself. This counterproductive immune response is called systemic inflammatory response syndrome (SIRS), and it can lead to the life-threatening condition known as sepsis. Sepsis is characterized by the production of excess cytokines that leads to classic signs of inflammation such as fever, vasodilation, and edema. In a patient with sepsis, the inflammatory response becomes dysregulated and disproportionate to the threat of infection. Critical organs such as the heart, lungs, liver, and kidneys become dysfunctional, resulting in increased heart and respiratory rates, and disorientation. If not treated promptly and effectively, patients with sepsis can go into shock and die.
Certain infections can cause inflammation in the heart and blood vessels. Inflammation of the endocardium, the inner lining of the heart, is called endocarditis and can result in damage to the heart valves severe enough to require surgical replacement. Inflammation of the pericardium, the sac surrounding the heart, is called pericarditis. The term myocarditis refers to the inflammation of the heart’s muscle tissue. Pericarditis and myocarditis can cause fluid to accumulate around the heart, resulting in congestive heart failure. Inflammation of blood vessels is called vasculitis. Although somewhat rare, vasculitis can cause blood vessels to become damaged and rupture; as blood is released, small red or purple spots called petechiae appear on the skin. If the damage of tissues or blood vessels is severe, it can result in reduced blood flow to the surrounding tissues. This condition is called ischemia, and it can be very serious. In severe cases, the affected tissues can die and become necrotic; these situations may require surgical debridement or amputation.
Infections of the Lymphatic System: Like the circulatory system, the lymphatic system does not have a normal microbiota, and the large numbers of immune cells typically eliminate transient microbes before they can establish an infection. Only microbes with an array of virulence factors are able to overcome these defenses and establish infection in the lymphatic system. However, when a localized infection begins to spread, the lymphatic system is often the first place the invading microbes can be detected.
Infections in the lymphatic system also trigger an inflammatory response. Inflammation of lymphatic vessels, called lymphangitis, can produce visible red streaks under the skin. Inflammation in the lymph nodes can cause them to swell. A swollen lymph node is referred to as a bubo, and the condition is referred to as lymphadenitis.
Part 2: Bacterial Infections of the Circulatory and Lymphatic Systems
Bacteria can enter the circulatory and lymphatic systems through acute infections or breaches of the skin barrier or mucosa. Breaches may occur through fairly common occurrences, such as insect bites or small wounds. Even the act of tooth brushing, which can cause small ruptures in the gums, may introduce bacteria into the circulatory system. In most cases, the bacteremia that results from such common exposures is transient and remains below the threshold of detection. In severe cases, bacteremia can lead to septicemia with dangerous complications such as toxemia, sepsis, and septic shock. In these situations, it is often the immune response to the infection that results in the clinical signs and symptoms rather than the microbes themselves.
Septic and Toxic Shock: At low concentrations, pro-inflammatory cytokines such as interleukin 1 (IL-1) and tumor necrosis factor-α (TNF-α) play important roles in the host’s immune defenses. When they circulate systemically in larger amounts, however, the resulting immune response can be life threatening. IL-1 induces vasodilation (widening of blood vessels) and reduces the tight junctions between vascular endothelial cells, leading to widespread edema. As fluids move out of circulation into tissues, blood pressure begins to drop. If left unchecked, the blood pressure can fall below the level necessary to maintain proper kidney and respiratory functions, a condition known as septic shock. In addition, the excessive release of cytokines during the inflammatory response can lead to the formation of blood clots. The loss of blood pressure and occurrence of blood clots can result in multiple organ failure and death.
Toxemia associated with infections caused by Staphylococcus aureus can cause staphylococcal toxic shock syndrome (TSS). Some strains of S. aureus produce a superantigen called toxic shock syndrome toxin-1 (TSST-1). TSS may occur as a complication of other localized or systemic infections such as pneumonia, osteomyelitis, sinusitis, and skin wounds (surgical, traumatic, or burns). Those at highest risk for staphylococcal TSS are women with preexisting S. aureus colonization of the vagina who leave tampons, contraceptive sponges, diaphragms, or other devices in the vagina for longer than the recommended time.
Staphylococcal TSS is characterized by sudden onset of vomiting, diarrhea, myalgia, body temperature higher than 38.9 °C (102.0 °F), and rapid-onset hypotension with a systolic blood pressure less than 90 mm Hg for adults; a diffuse erythematous rash that leads to peeling and shedding skin 1 to 2 weeks after onset; and additional involvement of three or more organ systems. The mortality rate associated with staphylococcal TSS is less than 3% of cases.
Diagnosis of staphylococcal TSS is based on clinical signs, symptoms, serologic tests to confirm bacterial species, and the detection of toxin production from staphylococcal isolates. Cultures of skin and blood are often negative; less than 5% are positive in cases of staphylococcal TSS. Treatment for staphylococcal TSS includes decontamination, debridement, vasopressors to elevate blood pressure, and antibiotic therapy with clindamycin plus vancomycin or daptomycin pending susceptibility results.
Gas Gangrene: Traumatic injuries or certain medical conditions, such as diabetes, can cause damage to blood vessels that interrupts blood flow to a region of the body. When blood flow is interrupted, tissues begin to die, creating an anaerobic environment in which anaerobic bacteria can thrive. This condition is called ischemia. Endospores of the anaerobic bacterium Clostridium perfringens (along with a number of other Clostridium spp. from the gut) can readily germinate in ischemic tissues and colonize the anaerobic tissues.
The resulting infection, called gas gangrene, is characterized by rapidly spreading myonecrosis (death of muscle tissue). The patient experiences a sudden onset of excruciating pain at the infection site and the rapid development of a foul-smelling wound containing gas bubbles and a thin, yellowish discharge tinged with a small amount of blood. As the infection progresses, edema and cutaneous blisters containing bluish-purple fluid form. The infected tissue becomes liquefied and begins sloughing off. The margin between necrotic and healthy tissue often advances several inches per hour even with antibiotic therapy. Septic shock and organ failure frequently accompany gas gangrene; when patients develop sepsis, the mortality rate is greater than 50%.
α-Toxin and theta (θ) toxin are the major virulence factors of C. perfringens implicated in gas gangrene. α-Toxin is a lipase responsible for breaking down cell membranes; it also causes the formation of thrombi (blood clots) in blood vessels, contributing to the spread of ischemia. θ-Toxin forms pores in the patient’s cell membranes, causing cell lysis. The gas associated with gas gangrene is produced by Clostridium’s fermentation of butyric acid, which produces hydrogen and carbon dioxide that are released as the bacteria multiply, forming pockets of gas in tissues (Figure 9.28). Treatment typically involves surgical debridement of any necrotic tissue; advanced cases may require amputation. Surgeons may also use vacuum-assisted closure (VAC), a surgical technique in which vacuum-assisted drainage is used to remove blood or serous fluid from a wound or surgical site to speed recovery. The most common antibiotic treatments include penicillin G and clindamycin. Some cases are also treated with hyperbaric oxygen therapy because Clostridium spp. are incapable of surviving in oxygen-rich environments.

Part 3: Viral Infections of the Circulatory and Lymphatic Systems
Viral pathogens of the circulatory system vary tremendously both in their virulence and distribution worldwide. Some of these pathogens are practically global in their distribution. Fortunately, the most ubiquitous viruses tend to produce the mildest forms of disease. In the majority of cases, those infected remain asymptomatic. On the other hand, other viruses are associated with life-threatening diseases that have impacted human history.
Infectious Mononucleosis and Burkitt Lymphoma: Human herpesvirus 4, also known as Epstein-Barr virus (EBV), has been associated with a variety of human diseases, such as mononucleosis and Burkitt lymphoma. Exposure to the human herpesvirus 4 (HHV-4) is widespread and nearly all people have been exposed at some time in their childhood, as evidenced by serological tests on populations. The virus primarily resides within B lymphocytes and, like all herpes viruses, can remain dormant in a latent state for a long time.
When uninfected young adults are exposed to EBV, they may experience infectious mononucleosis. The virus is mainly spread through contact with body fluids (e.g., saliva, blood, and semen). The main symptoms include pharyngitis, fever, fatigue, and lymph node swelling. Abdominal pain may also occur as a result of spleen and liver enlargement in the second or third week of infection. The disease typically is self-limiting after about a month. The main symptom, extreme fatigue, can continue for several months, however. Complications in immunocompetent patients are rare but can include jaundice, anemia, and possible rupture of the spleen caused by enlargement.
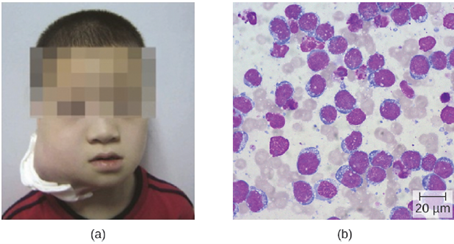
In patients with malaria or HIV, Epstein-Barr virus can lead to a fast-growing malignant cancer known as Burkitt lymphoma (Figure 9.29). This condition is a form of non-Hodgkin lymphoma that produces solid tumors chiefly consisting of aberrant B cells. Burkitt lymphoma is more common in Africa, where prevalence of HIV and malaria is high, and it more frequently afflicts children. Repeated episodes of viremia caused by reactivation of the virus are common in immunocompromised individuals. In some patients with AIDS, EBV may induce the formation of malignant B-cell lymphomas or oral hairy leukoplakia. Immunodeficiency-associated Burkitt lymphoma primarily occurs in patients with HIV. HIV infection, similar to malaria, leads to polyclonal B-cell activation and permits poorly controlled proliferation of EBV+ B cells, leading to the formation of lymphomas.
Because the disease is self-limiting, antiviral treatments are rare for mononucleosis. Cases
of Burkitt lymphoma are diagnosed from a biopsy specimen from a lymph node or tissue from a suspected tumor. Because the tumors grow so rapidly, staging studies must be expedited and treatment must be initiated promptly. Earlier diagnosis and treatment results in a cure rate greater than 90% for children and adults.
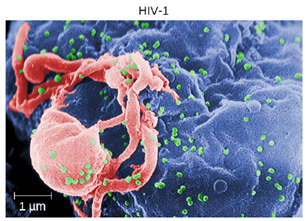
Human Immunodeficiency Virus: Human T-lymphotropic viruses (HTLV), also called human immunodeficiency viruses (HIV) are retroviruses that are the causative agent of acquired immune deficiency syndrome (AIDS). There are two main variants of human immunodeficiency virus (HIV). HIV-1 (Figure 9.30) occurs in human populations worldwide, whereas HIV-2 is concentrated in West Africa. Currently, the most affected region in the world is sub-Saharan Africa, with an estimated 25.6 million people living with HIV in 2015. Sub-Saharan Africa also accounts for two-thirds of the global total of new HIV infections.
HIV is spread through direct contact with body fluids. Casual contact and insect vectors are not sufficient for disease transmission; common modes of transmission include sexual contact and sharing of needles by intravenous (IV) drug users. It generally takes many years before the effects of an HIV infection are detected. HIV infections are not dormant during this period: virions are continually produced, and the immune system continually attempts to clear the viral infection, while the virus persistently infects additional CD4 T cells. Over time, the CD4 T-cell population is devastated, ultimately leading to AIDS.
When people are infected with HIV, their disease progresses through three stages based on CD4 T-cell counts and the presence of clinical symptoms.
- Stage 1: Acute HIV infection. Two to 4 weeks after infection with HIV, patients may experience a flulike illness, which can last for a few weeks. Patients with acute HIV infection have more than 500 cells/μL CD4 T cells and a large amount of virus in their blood. Patients are very contagious during this stage. To confirm acute infection, either a fourth-generation antibody-antigen test or a nucleic acid test (NAT) must be performed.
- Stage 2: Clinical latency. During this period, HIV enters a period of dormancy. Patients have between 200 and 499 cells/μL CD4 T cells; HIV is still active but reproduces at low levels, and patients may not experience any symptoms of illness. For patients who are not taking medicine to treat HIV, this period can last a decade or longer. For patients receiving antiretroviral therapy, the stage may last for several decades, and those with low levels of the virus in their blood are much less likely to transmit HIV than those who are not virally suppressed. Near the end of the latent stage, the patient’s viral load starts to increase and the CD4 T-cell count begins to decrease, leading to the development of symptoms and increased susceptibility to opportunistic infections.
- Stage 3: Acquired immunodeficiency syndrome (AIDS). Patients are diagnosed with AIDS when their CD4 T-cell count drops below 200 cells/μL or when they develop certain opportunistic illnesses. During this stage, the immune system becomes severely damaged by HIV. Common symptoms of AIDS include chills, fever, sweats, swollen lymph glands, weakness, and weight loss; in addition, patients often develop rare cancers such as Kaposi’s sarcoma and opportunistic infections such as Pneumocystis pneumonia, tuberculosis, cryptosporidiosis, and toxoplasmosis. This is a fatal progression that, in the terminal stages, includes wasting
As a consequence of provirus formation, it is currently not possible to eliminate HIV from an infected patient’s body. Elimination by specific antibodies is ineffective because the virus mutates rapidly—a result of the error-prone reverse transcriptase and the inability to correct errors. Antiviral treatments, however, can greatly extend life expectancy.
To combat the problem of drug resistance, combinations of antiretroviral drugs called antiretroviral therapy (ART), sometimes called highly active ART or combined ART, are used. There are several different targets for antiviral drug action (and a growing list of drugs for each of these targets). One class of drugs inhibits HIV entry; other classes inhibit reverse transcriptase by blocking viral RNA-dependent and DNA-dependent DNA polymerase activity; and still others inhibit one of the three HIV enzymes needed to replicate inside human cells.
Part 4: Helminths Infections of the of the Circulatory and Lymphatic Systems
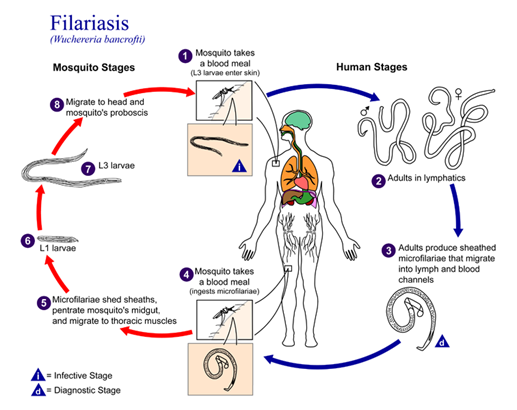
Lymphatic Filariasis: Lymphatic filariasis is caused by microscopic nematodes (parasitic worms) whose larvae are transmitted between human hosts by mosquitoes (figure 9.30). It is caused by three main species of nematodes, Wuchereria bancrofti (most frequent), Brugia malayi and Brugia timori. Male worms are about 3–4 centimeters in length, and female worms 8–10 centimeters. The male and female worms together form “nests” in lymphatic vessels, where their presence stimulates infiltration by lymphocytes, plasma cells, eosinophils, and thrombocytes (a condition known as lymphangitis). Because of the chronic nature of the illness, granulomas, fibrosis, and blocking of the lymphatic system may eventually occur.
Over time, these blockages may worsen with repeated infections over decades, leading to skin thickened with edema and fibrosis. Lymph (extracellular tissue fluid) may spill out of the lymphatic areas and back into tissues, causing extreme swelling (Figure 9.31). Secondary bacterial infections commonly follow. Because it is a disease caused by a parasite, eosinophilia (a dramatic rise in the number of eosinophils in the blood) is characteristic of acute infection. However, this increase in antiparasite granulocytes is not sufficient to clear the infection in many cases.

Lymphatic filariasis affects an estimated 120 million people worldwide, mostly concentrated in Africa and Asia. Improved sanitation and mosquito control can reduce transmission rates. Anti-helminths medication can stop the progression of the disease, but not reverse the swelling. Due to this, early detection and treatment is essential.
