Unit 9.6: Diseases of the Urogenital System
Outline
Part 1: Anatomy and Normal Microbiota of the Urogenital Tract
General Signs and Symptoms of Urogenital Infections
General Causes and Modes of Transmission of Urogenital Infections
Part 2: Bacterial Infections of the Urinary System
Learning Objectives
After reading the following, you should be able to:
- Describe the basic structure of the urogenital system, including protective features and defenses.
- Describe any features that promote microbial growth and give one example of a bacterial species that is part of the normal flora.
- Describe any general features of infections of the urogenital system.
- Describe cystitis, including its causative organisms and possible complications.
- Describe kidney infections, including its causative organisms and possible complications.
- Describe gonorrhea, including its causative organism and possible complications.
- Describe syphilis, including its causative organism and possible complications.
- Describe genital warts, including its causative organism and possible complications.
- For all the diseases in this section, describe mode of transmission, portal of entry, modes of detection (where discussed) and treatments (in general, e.g. antiviral medication, vaccine, etc)
The urogenital system is a combination of the urinary tract and reproductive system. Because both systems are open to the external environment, they are prone to infections. Some infections are introduced from outside, whereas others result from imbalances in the microbiota of the urogenital tract.
Urinary tract infections (UTIs) are one the most common bacterial infections worldwide, affecting over 100 million people each year. During 2007 in the United States, doctor office visits for UTIs exceeded 10 million, and an additional 2–3 million emergency department visits were attributed to UTIs. Sexually transmitted infections (STIs) also primarily affect the urogenital system and are an important cause of patient morbidity. The Centers for Disease Control and Prevention (CDC) estimates that there are approximately 20 million new cases of reportable STIs annually in the United States, half of which occur in people aged 15–24 years old. When STIs spread to the reproductive organs, they can be associated with severe morbidity and loss of fertility
Part 1: Anatomy and Normal Microbiota of the Urogenital Tract
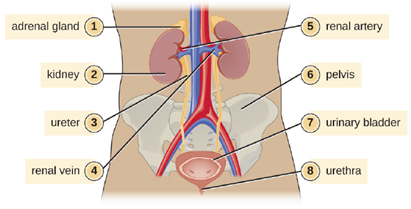
The basic structures of the urinary tract are common in males and females. However, there are unique locations for these structures in females and males, and there is a significant amount of overlap between the urinary and genital structures in males. Figure 9.52 illustrates the urinary anatomy common to females and males.
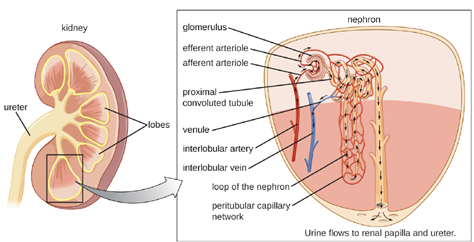
The kidneys carry out the urinary system’s primary functions of filtering the blood and maintaining water and electrolyte balance. The kidneys are composed of millions of filtration units called nephrons. Each nephron is in intimate contact with blood through a specialized capillary bed called the glomerulus (plural glomeruli). Fluids, electrolytes, and molecules from the blood pass from the glomerulus into the nephron, creating the filtrate that becomes urine (Figure 9.53). Urine that collects in each kidney empties through a ureter and drains to the urinary bladder, which stores urine. Urine is released from the bladder to the urethra, which transports it to be excreted from the body through the urinary meatus, the opening of the urethra.
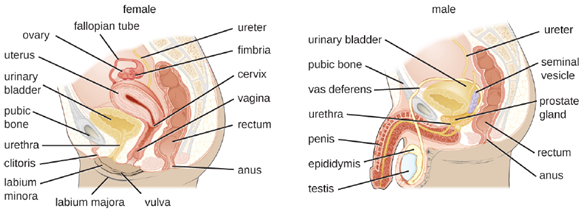
Anatomy of the Reproductive System: The male reproductive system (Figure 9.54) is located in close proximity to the urinary system, and the urethra is part of both systems. The testes are responsible for the production of sperm. The epididymis is a coiled tube that collects sperm from the testes and passes it on to the vas deferens. The epididymis is also the site of sperm maturation after they leave the testes. The seminal vesicles and prostate are accessory glands that produce fluid that supports sperm. During ejaculation, the vas deferens releases this mixture of fluid and sperm, called semen, into the urethra, which extends to the end of the penis.
The female reproductive system is located near the urinary system (Figure 9.54). The external genitalia (vulva) in females open to the vagina, a muscular passageway that connects to the cervix. The cervix is the lower part of the uterus (the organ where a fertilized egg will implant and develop). The cervix is a common site of infection, especially for viruses that may lead to cervical cancer. The uterus leads to the fallopian tubes and eventually to the ovaries. Ovaries are the site of ova (egg) production, as well as the site of estrogen and progesterone production that are involved in maturation and maintenance of reproductive organs, preparation of the uterus for pregnancy, and regulation of the menstrual cycle.
Normal Microbiota of the Urogenital System: The normal microbiota of different body sites provides an important nonspecific defense against infectious diseases, and the urogenital tract is no exception. In both men and women, however, the kidneys are sterile. Although urine does contain some antibacterial components, bacteria will grow in urine left out at room temperature. Therefore, it is primarily the flushing action that keeps the ureters and bladder free of microbes.
Below the bladder, the normal microbiota of the male urogenital system is found primarily within the distal urethra and includes bacterial species that are commonly associated with the skin microbiota. In women, the normal microbiota is found within the distal one third of the urethra and the vagina. The normal microbiota of the vagina becomes established shortly after birth and is a complex and dynamic population of bacteria that fluctuates in response to environmental changes. Members of the vaginal microbiota play an important role in the nonspecific defense against vaginal infections and sexually transmitted infections by occupying cellular binding sites and competing for nutrients. In addition, the production of lactic acid by members of the microbiota provides an acidic environment within the vagina that also serves as a defense against infections. For the majority of women, the lactic-acid–producing bacteria in the vagina are dominated by a variety of species of Lactobacillus. For women who lack sufficient lactobacilli in their vagina, lactic acid production comes primarily from other species of bacteria such as Leptotrichia spp., Megasphaera spp., and Atopobium vaginae. Lactobacillus spp. use glycogen from vaginal epithelial cells for metabolism and production of lactic acid. This process is tightly regulated by the hormone estrogen. Increased levels of estrogen correlate with increased levels of vaginal glycogen, increased production of lactic acid, and a lower vaginal pH. Therefore, decreases in estrogen during the menstrual cycle and with menopause are associated with decreased levels of vaginal glycogen and lactic acid, and a higher pH. In addition to producing lactic acid, Lactobacillus spp. also contribute to the defenses against infectious disease through their production of hydrogen peroxide and bacteriocins (antibacterial peptides).
General Signs and Symptoms of Urogenital Infections: Infections of the urinary tract most commonly cause inflammation of the bladder (cystitis) or of the urethra (urethritis). Urethritis can be associated with cystitis, but can also be caused by sexually transmitted infections. Symptoms of urethritis in men include burning sensation while urinating, discharge from the penis, and blood in the semen or the urine. In women, urethritis is associated with painful and frequent urination, vaginal discharge, fever, chills, and abdominal pain. The symptoms of cystitis are similar to those of urethritis. When urethritis is caused by a sexually transmitted pathogen, additional symptoms involving the genitalia can occur. These can include painful vesicles (blisters), warts, and ulcers. Ureteritis, a rare infection of the ureter, can also occur with cystitis. These infections can be acute or chronic.
Pyelonephritis and glomerulonephritis are infections of the kidney that are potentially serious. Pyelonephritis is an infection of one or both of the kidneys and may develop from a lower urinary tract infection; the upper urinary tract, including the ureters, is often affected. Signs and symptoms of pyelonephritis include fever, chills, nausea, vomiting, lower back pain, and frequent painful urination. Pyelonephritis usually only becomes chronic in individuals who have malformations in or damage to the kidneys.
Glomerulonephritis is an inflammation of the glomeruli of the nephrons. Symptoms include excessive protein and blood in urine, increased blood pressure, and fluid retention leading to edema of face, hands, and feet. Glomerulonephritis may be an acute infection or it can become chronic.
Infections occurring within the reproductive structures of males include epididymitis, orchitis, and prostatitis. Bacterial infections may cause inflammation of the epididymis, called epididymitis. This inflammation causes pain in the scrotum, testicles, and groin; swelling, redness, and warm skin in these areas may also be observed. Inflammation of the testicle, called orchitis, is usually caused by a bacterial infection spreading from the epididymis, but it can also be a complication of mumps, a viral disease. The symptoms are similar to those of epididymitis, and it is not uncommon for them both to occur together, in which case the condition is called epididymo-orchitis. Inflammation of the prostate gland, called prostatitis, can result from a bacterial infection. The signs and symptoms of prostatitis include fever, chills, and pain in the bladder, testicles, and penis. Patients may also experience burning during urination, difficulty emptying the bladder, and painful ejaculation.
Because of its proximity to the exterior, the vagina is a common site for infections in women. The general term for any inflammation of the vagina is vaginitis. Vaginitis often develops as a result of an overgrowth of bacteria or fungi that normally reside in the vaginal microbiota, although it can also result from infections by transient pathogens. Bacterial infections of the vagina are called bacterial vaginosis, whereas fungal infections (typically involving Candida spp.) are called yeast infections. Dynamic changes affecting the normal microbiota, acid production, and pH variations can be involved in the initiation of the microbial overgrowth and the development of vaginitis. Although some individuals may have no symptoms, vaginosis and vaginitis can be associated with discharge, odor, itching, and burning.
Pelvic inflammatory disease (PID) is an infection of the female reproductive organs including the uterus, cervix, fallopian tubes, and ovaries. The two most common pathogens are the sexually transmitted bacterial pathogens Neisseria gonorrhoeae and Chlamydia trachomatis. Inflammation of the fallopian tubes, called salpingitis, is the most serious form of PID. Symptoms of PID can vary between women and include pain in the lower abdomen, vaginal discharge, fever, chills, nausea, diarrhea, vomiting, and painful urination.
General Causes and Modes of Transmission of Urogenital Infections: Hormonal changes, particularly shifts in estrogen in women due to pregnancy or menopause, can increase susceptibility to urogenital infections. As discussed earlier, estrogen plays an important role in regulating the availability of glycogen and subsequent production of lactic acid by Lactobacillus species. Low levels of estrogen are associated with an increased vaginal pH and an increased risk of bacterial vaginosis and yeast infections. Estrogen also plays a role in maintaining the elasticity, strength, and thickness of the vaginal wall, and keeps the vaginal wall lubricated, reducing dryness. Low levels of estrogen are associated with thinning of the vaginal wall. This thinning increases the risk of tears and abrasions, which compromise the protective barrier and increase susceptibility to pathogens.
Another common cause of urogenital infections in females is fecal contamination that occurs because of the close proximity of the anus and the urethra. Escherichia coli, an important member of the digestive tract microbiota, is the most common cause of urinary tract infections (urethritis and cystitis) in women; it generally causes infection when it is introduced to the urethra in fecal matter. Good hygiene can reduce the risk of urinary tract infections by this route. In men, urinary tract infections are more commonly associated with other conditions, such as an enlarged prostate, kidney stones, or placement of a urinary catheter. All of these conditions impair the normal emptying of the bladder, which serves to flush out microbes capable of causing infection.
Infections that are transmitted between individuals through sexual contact are called sexually transmitted infections (STIs) or sexually transmitted diseases (STDs). (The CDC prefers the term STD, but WHO prefers STI, which encompasses infections that result in disease as well as those that are subclinical or asymptomatic.) STIs often affect the external genitalia and skin, where microbes are easily transferred through physical contact. Lymph nodes in the genital region may also become swollen as a result of infection. However, many STIs have systemic effects as well, causing symptoms that range from mild (e.g., general malaise) to severe (e.g., liver damage or serious immunosuppression).
Part 2: Bacterial Infections of the Urinary System
Urinary tract infections (UTIs) include infections of the urethra, bladder, and kidneys, and are common causes of urethritis, cystitis, pyelonephritis, and glomerulonephritis. Bacteria are the most common causes of UTIs, especially in the urethra and bladder.
Cystitis: Cystitis is most often caused by a bacterial infection of the bladder, but it can also occur as a reaction to certain treatments or irritants such as radiation treatment, hygiene sprays, or spermicides. Common symptoms of cystitis include dysuria (urination accompanied by burning, discomfort, or pain), pyuria (pus in the urine), hematuria (blood in the urine), and bladder pain.
In women, bladder infections are more common because the urethra is short and located in close proximity to the anus, which can result in infections of the urinary tract by fecal bacteria. Bladder infections are also more common in the elderly because the bladder may not empty fully, causing urine to pool; the elderly may also have weaker immune systems that make them more vulnerable to infection. Conditions such as prostatitis in men or kidney stones in both men and women can impact proper drainage of urine and increase risk of bladder infections. Catheterization can also increase the risk of bladder infection.
Gram-negative bacteria such as Escherichia coli (most commonly), Proteus vulgaris, Pseudomonas aeruginosa, and Klebsiella pneumoniae cause most bladder infections. Gram-positive pathogens associated with cystitis include the coagulase-negative Staphylococcus saprophyticus, Enterococcus faecalis, and Streptococcus agalactiae. Routine manual urinalysis using a urine dipstick or test strip can be used for rapid screening of infection. These test strips are either held in a urine stream or dipped in a sample of urine to test for the presence of nitrites, leukocyte esterase, protein, or blood that can indicate an active bacterial infection. The presence of nitrite may indicate the presence of E. coli or K. pneumonia; these bacteria produce nitrate reductase, which converts nitrate to nitrite.
Low specificity, sensitivity, or both, associated with these rapid screening tests require that care be taken in interpretation of results and in their use in diagnosis of urinary tract infections. Therefore, positive LE or nitrite results are followed by a urine culture to confirm a bladder infection. Urine culture is generally accomplished using blood agar and MacConkey agar, and it is important to culture a clean catch of urine to minimize contamination with normal microbiota of the penis and vagina. A clean catch of urine is accomplished by first washing the labia and urethral opening of female patients or the penis of male patients. The patient then releases a small amount of urine into the toilet bowl before stopping the flow of urine. Finally, the patient resumes urination, this time filling the container used to collect the specimen.
Bacterial cystitis is commonly treated with fluoroquinolones, nitrofurantoin, cephalosporins, or a combination of trimethoprim and sulfamethoxazole. Pain medications may provide relief for patients with dysuria. Treatment is more difficult in elderly patients, who experience a higher rate of complications such as sepsis and kidney infections.
Kidney Infections (Pyelonephritis and Glomerulonephritis): Pyelonephritis, an inflammation of the kidney, can be caused by bacteria that have spread from other parts of the urinary tract (such as the bladder). In addition, pyelonephritis can develop from bacteria that travel through the bloodstream to the kidney. When the infection spreads from the lower urinary tract, the causative agents are typically fecal bacteria such as E. coli. Common signs and symptoms include back pain (due to the location of the kidneys), fever, and nausea or vomiting. Gross hematuria (visible blood in the urine) occurs in 30–40% of women but is rare in men. The infection can become serious, potentially leading to bacteremia and systemic effects that can become life-threatening. Scarring of the kidney can occur and persist after the infection has cleared, which may lead to dysfunction.
Diagnosis of pyelonephritis is made using microscopic examination of urine, culture of urine, testing for leukocyte esterase and nitrite levels, and examination of the urine for blood or protein. It is also important to use blood cultures to evaluate the spread of the pathogen into the bloodstream. Imaging of the kidneys may be performed in high-risk patients with diabetes or immunosuppression, the elderly, patients with previous renal damage, or to rule out an obstruction in the kidney. Pyelonephritis can be treated with either oral or intravenous antibiotics, including penicillins, cephalosporins, vancomycin, fluoroquinolones, carbapenems, and aminoglycosides.
Glomerulonephritis occurs when the glomeruli of the nephrons are damaged from inflammation. Whereas pyelonephritis is usually acute, glomerulonephritis may be acute or chronic. The most well-characterized mechanism of glomerulonephritis is the post-streptococcal sequelae associated with Streptococcus pyogenes throat and skin infections. Although S. pyogenes does not directly infect the glomeruli of the kidney, immune complexes that form in blood between S. pyogenes antigens and antibodies lodge in the capillary endothelial cell junctions of the glomeruli and trigger a damaging inflammatory response. Glomerulonephritis can also occur in patients with bacterial endocarditis (infection and inflammation of heart tissue); however, it is currently unknown whether glomerulonephritis associated with endocarditis is also immune-mediated.
Part 3: Bacterial Infections of the Reproductive System
In addition to infections of the urinary tract, bacteria commonly infect the reproductive tract. As with the urinary tract, parts of the reproductive system closest to the external environment are the most likely sites of infection. Often, the same microbes are capable of causing urinary tract and reproductive tract infections.
Gonorrhea: Also known as the clap, gonorrhea is a common sexually transmitted disease of the reproductive system that is especially prevalent in individuals between the ages of 15 and 24. It is caused by Neisseria gonorrhoeae, which have fimbriae that allow the cells to attach to epithelial cells. It also has a type of lipopolysaccharide endotoxin called lipooligosaccharide as part of the outer membrane structure that enhances its pathogenicity. In addition to causing urethritis, N. gonorrhoeae can infect other body tissues such as the skin, meninges, pharynx, and conjunctiva.
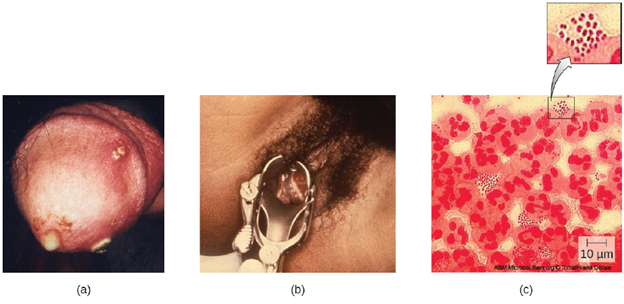
Many infected individuals (both men and women) are asymptomatic carriers of gonorrhea. When symptoms do occur, they manifest differently in males and females. Males may develop pain and burning during urination and discharge from the penis that may be yellow, green, or white (Figure 9.55). Less commonly, the testicles may become swollen or tender. Over time, these symptoms can increase and spread. In some cases, chronic infection develops. The disease can also develop in the rectum, causing symptoms such as discharge, soreness, bleeding, itching, and pain (especially in association with bowel movements).
Women may develop pelvic pain, discharge from the vagina, intermenstrual bleeding (i.e., bleeding not associated with normal menstruation), and pain or irritation associated with urination. As with men, the infection can become chronic. In women, however, chronic infection can cause increases in menstrual flow. Rectal infection can also occur, with the symptoms previously described for men. Infections that spread to the endometrium and fallopian tubes can cause pelvic inflammatory disease (PID), characterized by pain in the lower abdominal region, dysuria, vaginal discharge, and fever. PID can also lead to infertility through scarring and blockage of the fallopian tubes (salpingitis); it may also increase the risk of a life-threatening ectopic pregnancy, which occurs when a fertilized egg begins developing somewhere other than the uterus (e.g., in the fallopian tube or ovary).
When a gonorrhea infection disseminates throughout the body, serious complications can develop. The infection may spread through the blood (bacteremia) and affect organs throughout the body, including the heart (gonorrheal endocarditis), joints (gonorrheal arthritis), and meninges encasing the brain (meningitis).
Urethritis caused by N. gonorrhoeae can be difficult to treat due to antibiotic resistance.
Some strains have developed resistance to the fluoroquinolones, so cephalosporins are often a first choice for treatment. Treatment of sexual partners is also recommended to avoid reinfection and spread of infection to others.
Syphilis: Syphilis is spread through direct physical (generally sexual) contact, and is caused by the gram-negative spirochete Treponema pallidum. T. pallidum has a relatively simple genome and lacks lipopolysaccharide endotoxin characteristic of gram-negative bacteria. However, it does contain lipoproteins that trigger an immune response in the host, causing tissue damage that may enhance the pathogen’s ability to disseminate while evading the host immune system.
After entering the body, T. pallidum moves rapidly into the bloodstream and other tissues. If not treated effectively, syphilis progresses through three distinct stages: primary, secondary, and tertiary. Primary syphilis appears as a single lesion on the cervix, penis, or anus within 10 to 90 days of transmission. Such lesions contain many T. pallidum cells and are highly infectious. The lesion, called a hard chancre, is initially hard and painless, but it soon develops into an ulcerated sore (Figure 9.56). Localized lymph node swelling may occur as well. In some cases, these symptoms may be relatively mild, and the lesion may heal on its own within two to six weeks. Because the lesions are painless and often occur in hidden locations (e.g., the cervix or anus), infected individuals sometimes do not notice them.
The secondary stage generally develops once the primary chancre has healed or begun to heal. Secondary syphilis is characterized by a rash that affects the skin and mucous membranes of the mouth, vagina, or anus. The rash often begins on the palms or the soles of the feet and spreads to the trunk and the limbs (Figure 9.55). The rash may take many forms, such as macular or papular. On mucous membranes, it may manifest as mucus patches or white, wart-like lesions called condylomata lata. The rash may be accompanied by malaise, fever, and swelling of lymph nodes. Individuals are highly contagious in the secondary stage, which lasts two to six weeks and is recurrent in about 25% of cases.
After the secondary phase, syphilis can enter a latent phase, in which there are no symptoms but microbial levels remain high. Blood tests can still detect the disease during latency. The latent phase can persist for years.
Tertiary syphilis, which may occur 10 to 20 years after infection, produces the most severe symptoms and can be fatal. Granulomatous lesions called gummas may develop in a variety of locations, including mucous membranes, bones, and internal organs (Figure 9.56). Gummas can be large and destructive, potentially causing massive tissue damage. The most deadly lesions are those of the cardiovascular system (cardiovascular syphilis) and the central nervous system (neurosyphilis). Cardiovascular syphilis can result in a fatal aortic aneurysm (rupture of the aorta) or coronary stenosis (a blockage of the coronary artery). Damage to the central nervous system can cause dementia, personality changes, seizures, general paralysis, speech impairment, loss of vision and hearing, and loss of bowel and bladder control.

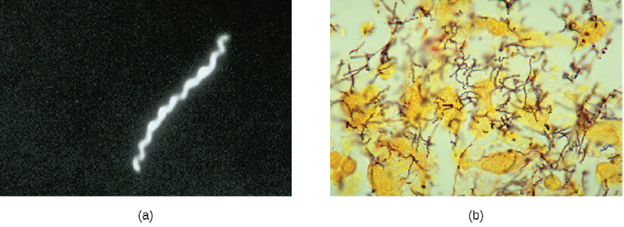
The recommended methods for diagnosing early syphilis are darkfield or brightfield (silver stain) microscopy of tissue or exudate from lesions to detect T. pallidum (Figure 9.57). The recommended treatment for syphilis is parenteral penicillin G (especially long-acting benzathine penicillin, although the exact choice depends on the stage of disease). Other options include tetracycline and doxycycline.
Part 4: Viral Infections of the Reproductive System
Several viruses can cause serious problems for the human reproductive system. Most of these viral infections are incurable, increasing the risk of persistent sexual transmission. In addition, such viral infections are very common in the United States. For example, human papillomavirus (HPV) is the most common STI in the country, with an estimated prevalence of 79.1 million infections in 2008; herpes simplex virus 2 (HSV-2) is the next most prevalent STI at 24.1 million infections.
Human Papillomas: Warts of all types are caused by a variety of strains of human papillomavirus (HPV). Condylomata acuminata, more commonly called genital warts or venereal warts (Figure 9.58), are an extremely prevalent STI caused by certain strains of HPV. Condylomata are irregular, soft, pink growths that are found on external genitalia or the anus.

HPV is a small, non-enveloped virus with a circular double-stranded DNA genome. Researchers have identified over 200 different strains (called types) of HPV, with approximately 40 causing STIs. While some types of HPV cause genital warts, HPV infection is often asymptomatic and self-limiting. However, genital HPV infection often co-occurs with other STIs like syphilis or gonorrhea. Additionally, some forms of HPV (not the same ones associated with genital warts) are associated with cervical cancers. At least 14 oncogenic (cancer-causing) HPV types are known to have a causal association with cervical cancers. Examples of oncogenic HPV are types 16 and 18, which are associated with 70% of cervical cancers. Oncogenic HPV types can also cause oropharyngeal cancer, anal cancer, vaginal cancer, vulvar cancer, and penile cancer. Most of these cancers are caused by HPV type 16. HPV virulence factors include proteins (E6 and E7) that are capable of inactivating tumor suppressor proteins, leading to uncontrolled cell division and the development of cancer.
HPV cannot be cultured, so molecular tests are the primary method used to detect HPV. While routine HPV screening is not recommended for men, it is included in guidelines for women. An initial screening for HPV at age 30, conducted at the same time as a Pap test, is recommended. If the tests are negative, then further HPV testing is recommended every five years. More frequent testing may be needed in some cases. The protocols used to collect, transport, and store samples vary based on both the type of HPV testing and the purpose of the testing. This should be determined in individual cases in consultation with the laboratory that will perform the testing.
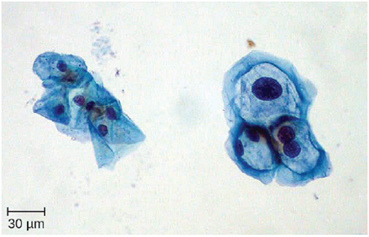
Because HPV testing is often conducted concurrently with Pap testing, the most common approach uses a single sample collection within one vial for both. This approach uses liquid-based cytology (LBC). The samples are then used for Pap smear cytology as well as HPV testing and genotyping. HPV can be recognized in Pap smears by the presence of cells called koilocytes (called koilocytosis or koilocytotic atypia). Koilocytes have a hyperchromatic atypical nucleus that stains darkly and a high ratio of nuclear material to cytoplasm. There is a distinct clear appearance around the nucleus called a perinuclear halo (Figure 9.59).
Most HPV infections resolve spontaneously; however, various therapies are used to treat and remove warts. Topical medications such as imiquimod (which stimulates the production of interferon), podofilox, or sinecatechins, may be effective. Warts can also be removed using cryotherapy or surgery, but these approaches are less effective for genital warts than for other types of warts. Electrocauterization and carbon dioxide laser therapy are also used for wart removal.
Regular Pap testing can detect abnormal cells that might progress to cervical cancer, followed by biopsy and appropriate treatment. Vaccines for some of the high risk HPV types are now available. Gardasil vaccine includes types 6, 11, 16 and 18 (types 6 and 11 are associated with 90% of genital wart infections and types 16 and 18 are associated with 70% of cervical cancers). Gardasil 9 vaccinates against the previous four types and an additional five high-risk types (31, 33, 45, 52, and 58). Cervarix vaccine includes just HPV types 16 and 18. Vaccination is the most effective way to prevent infection with oncogenic HPV, but it is important to note that not all oncogenic HPV types are covered by the available vaccines. It is recommended for both boys and girls prior to sexual activity (usually between the ages of nine and fifteen).
