Information on Mandatory Reporting
This section begins with a brief description of how child welfare legislation in Canada has evolved and outlines how legislation is differentiated amongst the provinces and territories. The definitions of child maltreatment are expanded upon as well as the circumstances in which these various forms of maltreatment are often found. In addition, this section will provide a brief list of the occupations that are required to report to Child Protection Services.
Click on the different sub-sections below to navigate the page!
- History of Child Maltreatment Legislation in Canada
- Definitions of Child Maltreatment
- Mandatory Reporters
- Canadian Association of Social Workers
- Proactive Strategies to Avoid Potential Relationship Rupture
History of Child Maltreatment Legislation in Canada
Canadian child welfare legislation grew from the concept of parens patriae, a Latin term for “protector” or “father of the country” whereby the court may substitute as a benevolent parent on behalf of the state (Bala & Clark, 1981). Although interventions originally focused on enforcing standards of care as opposed to the caring aspects of parenting, the parens patriae framework served to inform Ontario’s 1893 Act for the Prevention of Cruelty to and Better Protection of Children and the 1908 federal Juvenile Delinquents Act (MacIntyre, 1993). The latter legislation was designed to protect children from their or others’ “evil tendencies” through providing state representatives to offer guidance and assistance.
Juvenile and family court judges were charged with the responsibility of acting in the role of the benevolent parent on behalf of the state and render their decisions for the child’s best interests accordingly. Amendments to provincial child welfare and federal juvenile delinquent acts throughout most of the 20th century were based on the concept of parens patriae, which provided the state with the right to remove some authority from the family, define good and bad parents’ behaviour, articulate safe living conditions for children, propose possible outcomes for young persons involved, and establish services for children believed to be in need of state intervention (MacIntyre, 1993).
In Canada, child welfare falls under provincial and territorial matters. With the enactment of child welfare legislation, arose the establishment and growth of Child Protection Services (CPS) and provincial departments of child welfare. Early legislation did not concern itself with societal issues of poverty, exploitation of children, or other social issues which resulted in neglected, abandoned, or maltreated children, but did enforce that parents no longer had the right to absolute power over their children (MacIntyre, 1993). Child welfare legislation continued to expand and refine in scope throughout the 21st century. In the 1960s, provinces began introducing mandatory reporting legislation (Mathews & Kenny, 2008) and since 1980, every province and territory has enacted some form of this legislation (Walters, 1995).
Definitions of Child Maltreatment
Legislation differs across provinces, territories, and states in the definition of maltreatment. At the federal level, the Public Health Agency of Canada (2006) stipulates that “child maltreatment refers to the harm, or risk of harm, that a child or youth may experience while in the care of a person they trust or depend on, including a parent, sibling, other relative, teacher, parent or guardian. Harm may occur through direct actions by the person (acts of commission) or through the person’s neglect to provide a component of care necessary for healthy child growth and development (acts of omission)” or “psychological harm, or serious risk of harm to the child.”
Physical maltreatment involves actions such as: shaking, pushing, grabbing, throwing, hitting with a hand, punching, kicking, biting, hitting with an object, or other forms such as choking, strangling, stabbing, burning, shooting, poisoning, and the abusive use of restraints (Trocmé et al., 2010). Emotional maltreatment has vague definitions due to a lack of a specific incident or visible injury and tends to become apparent over time. This type of maltreatment includes threatening, belittling or defamation, inadequate nurturance / affection, invasion of privacy, negligence, and exposure to non-intimate violence such as between adults other than parents (Trocmé et al., 2010).
Neglect includes omissions in care by parents or legal guardians resulting in significant or, the risk of significant, harm and involves failing to provide for a child’s basic needs (i.e., food, clothing, shelter, supervision, medical care, emotional care, education, psychological / psychiatric treatment, a hazard free home, affection) (Dubowitz, 1997; Trocmé et al., 2010). Neglect is often found in families living at or below the poverty level who are struggling with economic issues to provide for necessities such as food (Trocmé et al., 2010).
Sexual maltreatment encompasses acts involving physical contact including penetration, attempted penetration, oral sex, fondling, sex talk, voyeurism, exhibitionism, exploitation, inappropriate touching of genitalia as well as those of non-contact including exposure to pornography or sexual acts (Trocmé et al., 2010).
Exposure to intimate partner violence is an addition to mandatory reporting legislation in the Canadian context and involves a child either directly witnessing violence between parents or indirectly witnessing the violence, such as through seeing the physical injuries on the parent or overhearing the violence. Within the previous decade, seven jurisdictions have included exposure to intimate partner violence as a circumstance where a child is in need of protection (Newfoundland and Labrador, Alberta, Manitoba, the Northwest Territories, Nova Scotia, Prince Edward Island, and Saskatchewan) (Mathews & Kenny, 2008). Ontario does not currently have this legislation; however, these cases are processed as child protection services based on the Ontario Child Welfare Eligibility Spectrum (2021) and some municipal police protocols.
These categories should be analyzed within the context of their varied circumstances, for example, neglect may have different meanings and manifestations for a child aged four as opposed to an adolescent aged 14. Neglect may also have a different meaning for an upper middle-class family as opposed to a family living below the poverty level.
Mandatory Reporters
In addition to social workers, there are many professional groups who are considered mandatory reporters. Some of the professional groups include medical personnel (physicians, surgeons, osteopaths, resident interns, nurses, dentists, dental hygienists, medical examiners, pharmacists), mental health professionals (psychologists, social workers, marriage and family clinicians, family counsellors), educational personnel (teachers, teacher’s assistants, administrative officers, school principals), members of the clergy, employees of the justice system (probation officers, parole officers), and occupations specific to children / youth (operators or employees of a day-care facility, youth or recreation workers, employees of public or private day camps, foster parents, group home personnel). This list is not exhaustive, and those occupations with mandatory reporting obligations vary per provincial and territorial legislation.
Canadian Association of Social Workers
Despite the fact that mandatory reporting legislation is provincially and territorially directed, all registered social workers practicing in Canada are governed by The Canadian Association of Social Workers Code of Ethics, Values and Guiding Principles (2024). The Code of Ethics is not silent on the mandatory reporting of child maltreatment but speaks to this issue at various points:
- Guiding Principle 1.7: Social workers uphold the rights of every person, group, and community to be free from violence or threat of violence;
- 1.7.3 being knowledgeable about the signs of physical, emotional, and sexual abuse and the sexual exploitation of children and youth and taking the necessary measures to protect their safety and well-being and, where circumstances require, fulfil their professional duty to report specified under child protection legislation in their jurisdiction
The code also speaks about confidentiality:
- Guiding Principle 6.3: Social workers are transparent about the limits of confidentiality in their professional practice;
- Guidelines: Social workers inform service users of the limits to privacy and confidentiality related to:
- 6.3.1: the individual rights of children and adolescents, couples, families, or groups sharing information in service provision, which may or may not be respected by all
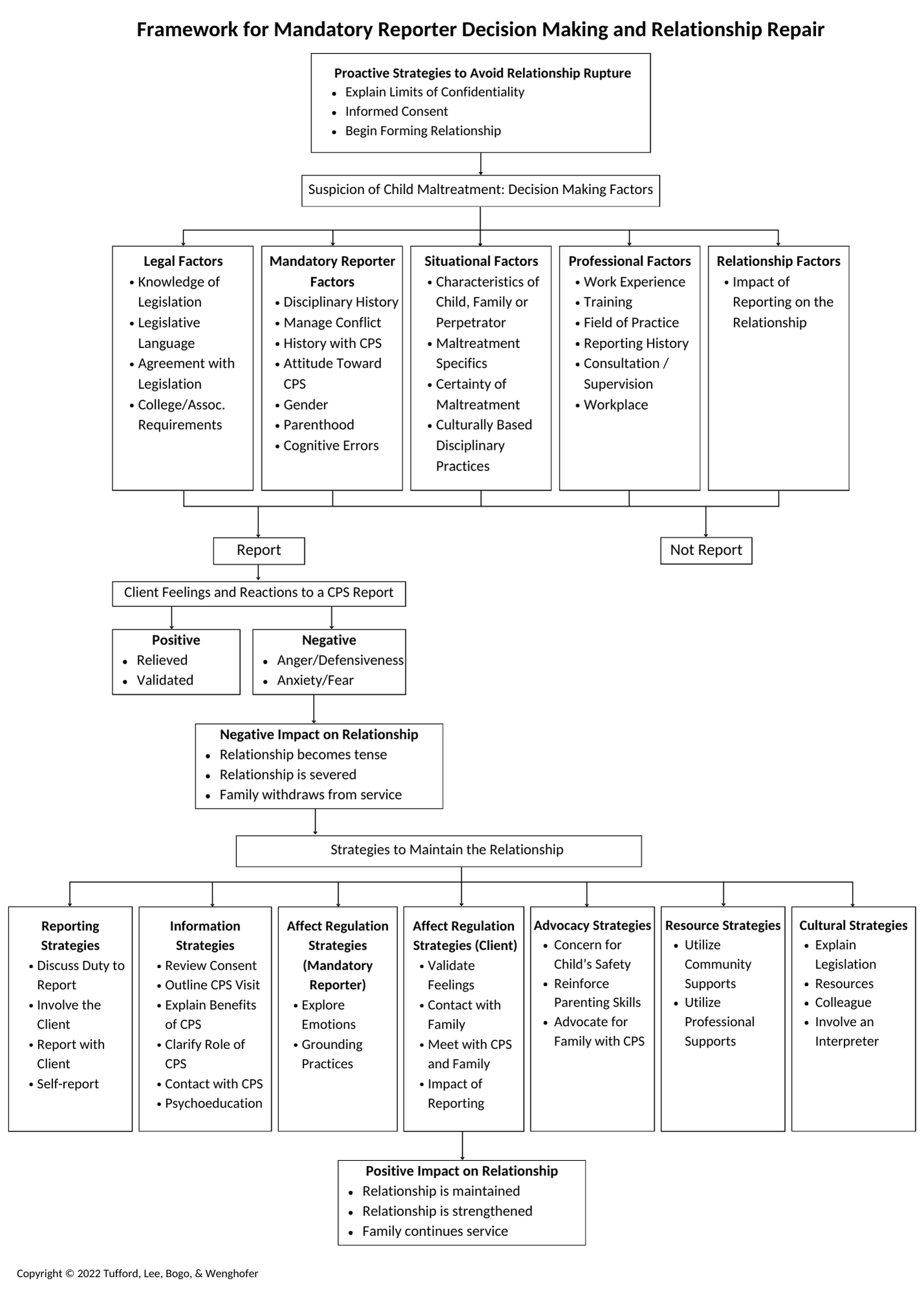
The framework of Figure 1 is based on Brosig and Kalichman’s (1992) model of practicing psychologists’ child maltreatment reporting decisions. This framework begins with the strategies respondents outlined qualitatively to avoid relationship ruptures prior to the disclosure of reportable material. Specifically, respondents noted explaining the limits of confidentiality at the start of counselling, asking clients to sign an informed consent statement, and building a therapeutic relationship early within counselling.
From these initial strategies, the framework proceeds to outline the decision-making factors to consider when faced with suspected child maltreatment. These include legal, mandatory reporter, situational, professional, and relationship factors. Based on these discrete but interrelated factors, the mandatory reporter decides to report or not report to CPS. In the event of reporting, the family may have a positive or negative reaction to the report or somewhere in between. A positive reaction could include that the family feels heard and understood and is appreciative of the report. A negative reaction could include that the family feels afraid, angered, and betrayed by the mandatory reporter. This could then lead to the relationship becoming strained and tense and possibly resulting in the family withdrawing from treatment. In the event that the family’s reaction is negative, the mandatory reporter can draw from a number of relationship repair strategies, specifically reporting, information, affect regulation, advocacy, resource, and cultural strategies. Emerging from these strategies is the impact on the relationship which can be maintained or strengthened leading to continued treatment.
In presenting this framework, some mandatory reporters may have been trained to not tell the client they are reporting, or their workplace policy is not to tell clients while other readers may have been trained to discuss reporting with the client prior to doing so. The framework is predicated on discussing the report with the client, but this may not be the case for all mandatory reporters. However, the relationship repair strategies can still be useful for mandatory reporters who do not discuss reporting with clients prior to filing a report.
Proactive Strategies to Avoid Potential Relationship Rupture
At the top of the framework are the proactive strategies to avoid potential relationship rupture. The first strategy involves explaining the limits of confidentiality, which will look different depending on the geographic region. When explaining the limits of confidentiality, it is recommended to discuss the different types of abuse and neglect, namely physical, sexual, emotional, intimate partner violence, and neglect. This lets the client know that there are different types of abuse as often clients may think of only physical abuse.
It is also important to discuss any legal reasons why confidentiality cannot be maintained, for example, there may be situations where client notes must be submitted for court proceedings. There may be other situations, for example, in Ontario, if a client discloses they are being treated in an unethical manner by a regulated health care provider such as an occupational therapist, physiotherapist, teacher, or doctor, the mandatory reporter is obligated to contact that professional’s college. Should the client have any questions about any aspect of confidentiality, their questions and the social worker’s responses should be documented and remain in the client file.
The second strategy is informed consent. This involves asking a client to sign an informed consent statement that would explain the limits to confidentiality as well as other information such as fees, cancelation procedures etc. Some clients may not feel comfortable signing an informed consent statement and may wish to give oral consent. In this situation it is important to document that the informed consent statement was explained in detail and the client chose not to sign but gave oral consent. The final strategy involves beginning to form the therapeutic relationship with the client. This will be demonstrated in the simulation videos which are part of the educational toolkit. Building the relationship can take place by asking how the client is doing, expressing concern for their wellbeing, offering condolences when a loss has occurred, and treating them not just as a parent but as an individual. It is important to remember that most clients are trying to parent the best they can often under challenging circumstances such as inadequate housing, poverty, disability, illness, and bereavement.
Summary
Section One provided critical information on the legal and ethical aspects of mandatory reporting in Canada as well as information on CPS. Social workers new to the practice are advised to familiarize themselves with this information and to stay current with legislative and ethical revisions which may impact their practice. Section Two outlines the empirical literature on decision making concerning the mandatory reporting of child maltreatment.
Reference: Tufford, L., Lee, B., Bogo, M., & Wenghofer, E. (2022). Maintaining a working relationship with clients when reporting suspected child maltreatment: Using simulation in education. Laurentian University, University of British Columbia, & University of Toronto.
