128
Jen to check DHPLC for gross & histopath specimens
Gross anatomy and histopathology specimens for:
- Traumatic brain injury
- Ischemic stroke
- MS
- Diabetic neuropathy
Learning Objectives
By the end of this chapter, you will be able to:
- List key observations from anatomical specimens of traumatic brain injury, ischemic stroke, multiple sclerosis, and diabetic neuropathy
- Correlate observations from anatomical specimens to patient histories
- Identify findings from histopathological slides of traumatic brain injury, ischemic stroke, multiple sclerosis, and diabetic neuropathy
In this section, we’ll further explore the neuromuscular diseases outlined in our pathophysiology chapter by presenting some anatomical specimens and images of histopathology slides. A brief summary of each disease will also be provided, but please refer to the pathophysiology chapter (add hyperlink) for in-depth information as needed.
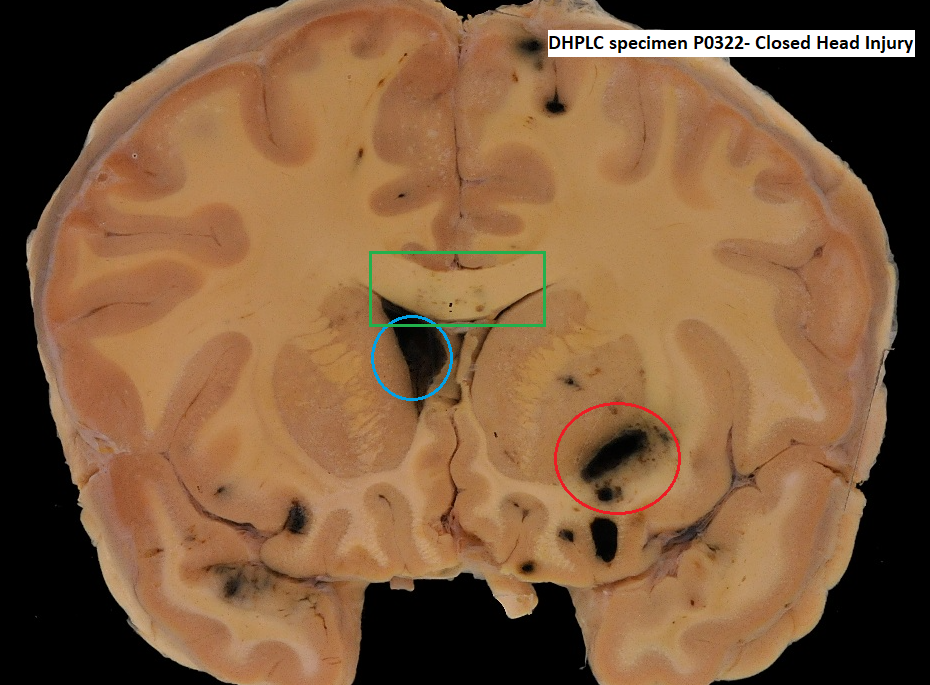
Closed Head Traumatic Brain Injury
Traumatic brain injury (TBI) is an injury to the brain caused by an external force to the head or neck. The initial primary trauma to the brain as well as the subsequent delayed pathophysiological changes can lead to neuron cell damage and death. TBI results in impaired physical and/or cognitive functioning, which may or may not be reversible. In a closed-head injury, the skull remains intact.
Anatomical Specimens
This specimen demonstrates a case of closed-head TBI.
| Patient history: |
| A previously healthy young male was found with a fixed dilated right pupil, non-reacting left pupil, flaccid paralysis (absent muscle tone) and areflexia (absent reflexes) at the scene of a motor vehicle accident. In hospital, the patient was placed on a respirator and x-ray imaging revealed an intact skull. CT imaging showed a swollen brain with intraventricular bleeding (bleeding into the ventricles). |
| Key Observations |
|
Stroke
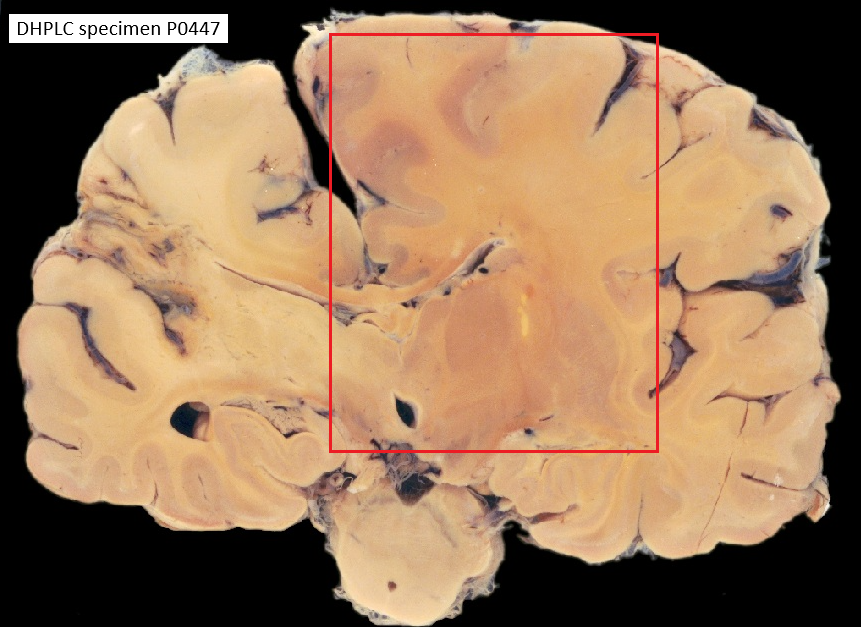
Anatomical Specimens
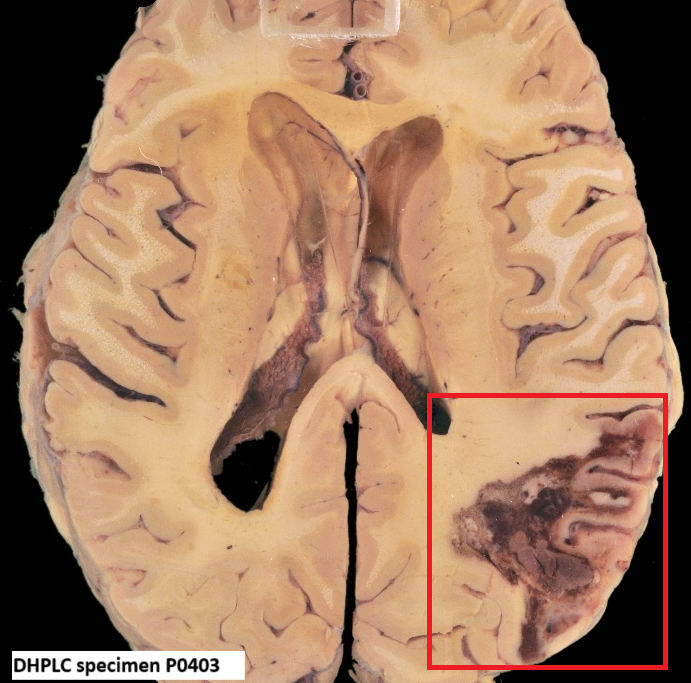
This specimen demonstrates a case of a previous ischemic stroke (specimen P0447- add)
| Patient history: |
| 6 years ago, this 81 year old man suffered an ischemic stroke resulting in left hemiplegia (one-sided paralysis) and hemianesthesia (one-sided loss of sensation) but no speech disturbance. |
| Key Observations |
|
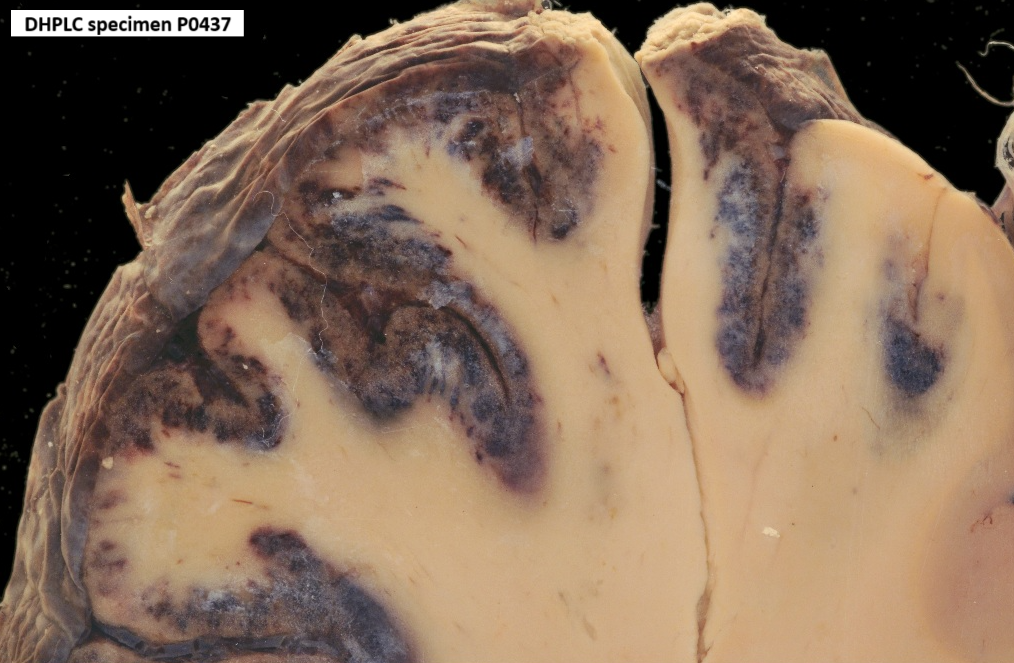
This specimen demonstrates a case of a hemorrhagic stroke
| Patient history: |
| This elderly man suffered a sudden-onset severe headache which progressed to weakness of the right arm and leg and eventual complete paralysis. |
| Key Observations |
|
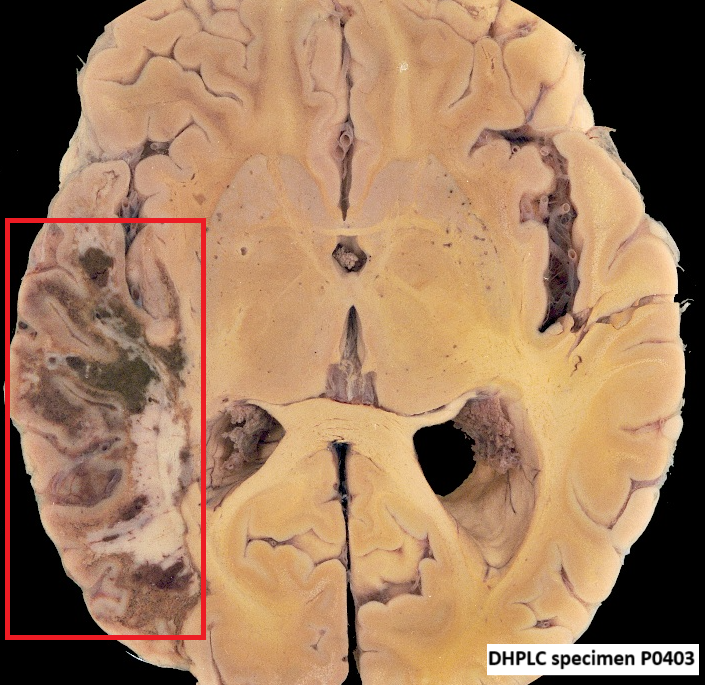
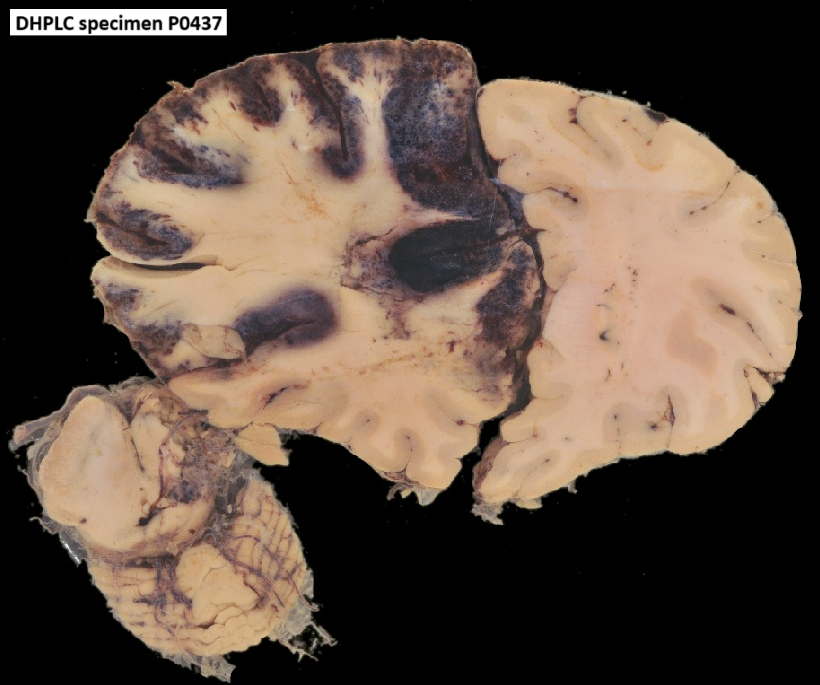
This specimen demonstrates a case of a hemorrhagic stroke
| Patient history: |
| This previously healthy 70 year old man was found conscious but unable to produce or understand speech and right hemiparalysis. |
| Key Observations |
|
Histopathological Specimen- Jen to look:
VALERIE: You can look at PATH 425-135 (cerebral anoxia), PATH 425-134 (old infarct), or PATH 425-133 (recent infarct). But i don’t have the microscopic descriptions on hand right now….
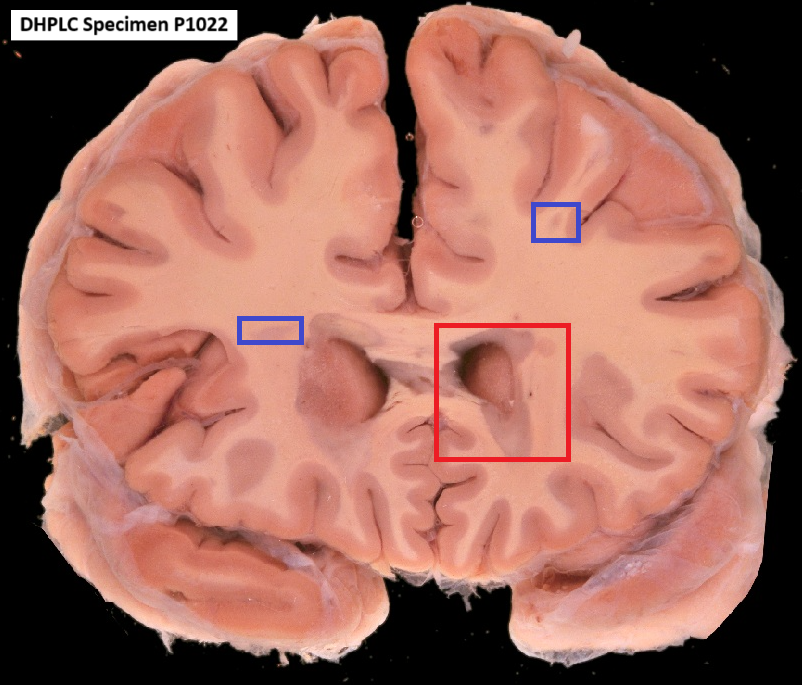
Multiple Sclerosis
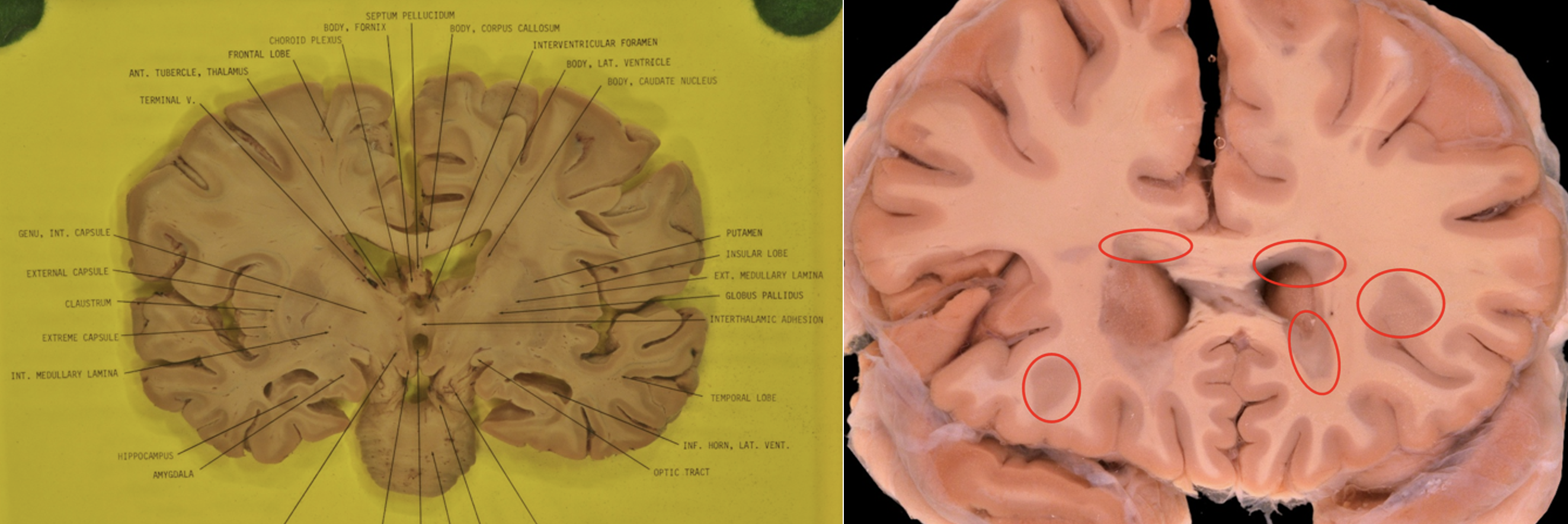
Figure XYZ. Normal coronal brain gross anatomy specimen (left) compared to a specimen showing MS lesions (right). Prominent sharply outlined grey plaques of demyelination surround the anterior horns of the lateral ventricles, as outlined by the red circles. Since MS plaques are areas of demyelination, they resemble the colour of the grey matter in the cortex. Smaller plaques are also visible scattered along the margin of cortex and white matter. (P Brain Normal Coronal # 5_DSC2622)
Anatomical Specimens
This specimen demonstrates a case of MS
| Patient history: |
| This 36 year old man had suffered from multiple sclerosis for 7 years. It began with transient blindness in one eye, followed by paresthesia (tingling) and spasticity of one, then both legs. Next the left arm became atactic (clumsy with poor muscle control). Bladder disturbances followed. |
| Key Observations |
|