57 Review of Cell Cycling, DNA duplication, Cell Differentiation and Errors that can lead to Cancer
Zoë Soon
Review of Cell Cycling and DNA duplication
Cell cycling in humans begins right away, starting with a fertilized egg. Undoubtedly you don’t remember when you were this young, however, your first act as a fertilized egg was to grow larger in size and then get divide from 1 cell into 2 identical cells. This process is termed cell cycling. During cell cycling a cell becomes larger, duplicates its organelles and DNA and then divides into two identical daughter cells. This process of cell duplication is also sometimes called cell division, or cell proliferation or simply mitosis.
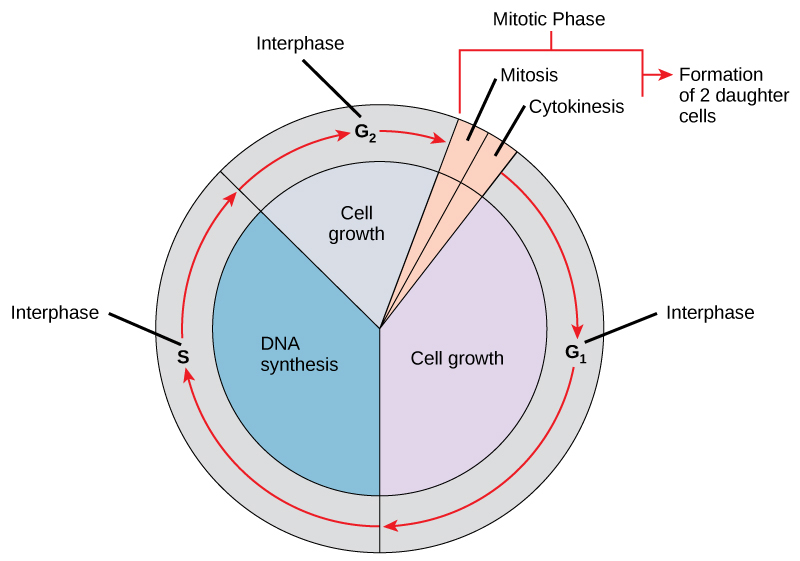
The steps of cell cycling are all equally important. The process begins in Interphase and there are three distinct stages within Interphase: G1, S and G2. In G1, the cell is growing in size and is duplicating its organelles. In S phase, DNA duplication occurs and in G2, the cell grows a bit more. After interphase is complete, the cell enters Mitosis. Within mitosis the enlarged cell divides into two cells, with half of its organelles and one set of DNA ending up in each daughter cell.
Review of Cell Differentiation
As the fertilized egg grows, and repeatedly goes through cell cycling, a ball of identical cells called a blastocyst is created. At this point in time cells begin to mature and differentiate slightly to form 3 unique cell lineages (endoderm, mesoderm, and ectoderm). Within each of these cell types, cells continue to go through cell cycling and the embryo gets larger and larger in total size. Eventually these cells will become even further differentiated forming lineages for all 200 cell types of the human body (e.g. epithelial cells, cardiomyocytes, hepatocytes, etc.). Organs will form with unique sets of cell types becoming more and more functional. Wtihin each organ and tissue, some daughter cells (termed stem cells) continue to cell cycle, producing more cells, allowing the embryo to get larger, while other daughter cells exit the cell cycle and full mature or differentiate. These fully mature cells can no longer cell cycle and divide, and instead express specific proteins and enzymes to become more and more functional. This process continues through all stages of development from embryo to fetus to newborn to child to teenager. Even as a full-size adult, many tissues contain stem cells that divide in order to allow for the replacement of mature cells that get old and die. However most cells have exited the cell cycle and have fully differentiated to ensure that each organ and tissue is functional.
Cellular Review of Cellular proliferation and differentiation begin with a fertilized egg.
During embryogenesis, the fertilized egg undergoes mitosis, leading to cell division.
Cells differentiate into various types, such as epithelial, connective, muscle, and neural tissue.
Stem cells undergo mitosis to produce daughter cells, which may differentiate into functional cells.
During mitosis, organelles double, and DNA duplication occurs during the S phase of the cell cycle.
Enzymes check DNA for errors during duplication, triggering apoptosis if mutations are found.
Telomeres, end caps of chromosomes, shorten with each cell division, acting as a safety net to limit division.
Telomere shortening helps prevent excessive divisions, reducing the risk of mutations and cancer development.
Apoptosis is triggered if telomeres reach a certain length, preventing further cell division and potential cancerous growth
DNA mutations and Cancer
Unfortunately during S phase, as DNA is duplicated there is a chance for errors in sequencing together the correct strands of nucleotides. Luckily there are several enzymes that check the DNA for errors during duplication and will trigger apoptosis if mutations are found that can not be fixed. It is known that mutations that occur in DNA (depending on the location) can cause cancer. It is also known that inevitably DNA errors do occur during duplication just due to the shear number of times DNA is duplicated, not to mention the number of nucleotides within each of the 23 pairs of chromosomes. It may seem obvious that the more DNA duplication events there are, the more risk there is for DNA errors to occur. Therefore a person’s age becomes a risk factor for DNA mutations (and the possibility that these mutations may give rise to cancer). One can also imagine that if any of the enzymes responsible for checking DNA for errors in S phase is damaged or mutated or absent, that again person has an increased risk of accumulating mutations and therefore susceptibility to cancer.
Role of Telomeres and Telomerase in Cancer
Telomeres, the end caps of chromosomes, which are maintained through childhood and adolescence through the enzymatic action of telomerase which continues to add telomere to the ends of chromosome. Telomerase is inactivated in adulthood and the telomeres begin to shorten with each cell division, acting as a safety net to limit division. At a certain length, a critical point is reached, and the cell becomes dormant or dies. This telomere shortening helps prevent excessive divisions, reducing the risk of mutations and cancer development. Additionally, at a certain age the cell has likely become less functional or dysfunctional, potentially accumulating waste products or abnormalities and it would become detrimental to the body if it wasn’t inactivated or removed. In tissue that is regenerative, old cells can be replaced through the division of tissue-specific stem cells. In cells that die when telomeres reach a certain length, apoptosis is triggered and macrophages engulf and recycle their components. Interestingly it has been found that in 90% of cancers, telomerase has been re-activated in the cancerous cells (which helps them to become immortal – continually adding telomere length and thereby permitting continual cell cycling).
Welcome to Lesson 3. Today we’re going to talk about neoplasia, which we introduced in Lesson 2, so we know what that means new growth. Here’s of course our important copyright information and some cartoons to get us started. In the first slide, I just wanted to remind us of some terms and I’m sure you’re remembering the word differentiation. And of course you can’t remember being a fertilized egg. But what happened, of course, while you were growing in your mom’s womb during embryogenesis, that cell started dividing. You went through rounds of mitosis. And these cells then started to go down different pathways, becoming more and more differentiated to give rise to tissues such as epithelial tissue, connective tissue, muscle tissue, and neural tissue, our four tissue types, ok that we know the word differentiation. And hopefully you remember the word cell cycle and mitosis as well. This is a great figure again from anatomy and physiology. And of course with cell cycle and mitosis, we’re talking about typically stem cells that are going through rounds of mitosis producing daughter cells. This is in this diagram. And these daughter cells may well then differentiate and become functional. So in this process of cell division or mitosis, we know that this original cell has to of course, double its organelles and it also helps to duplicate its DNA. You might remember that during cell cycle or mitosis, DNA duplication occurs during the S phase of the cell cycle. And this is again another figure from anatomy and physiology. And it’s showing you that this parent strand of DNA is of course getting duplicated into two identical strands in preparation for going through with mitosis. So you can imagine that creating an exact duplicate is very important and when this process goes through, the DNA is checked by enzymes for any errors that might have occurred during this duplication process. And you might remember from lesson two that if those enzymes sense any or find any DNA errors, they will trigger that cell to go through apoptosis. And the reason for that, of course, that if a DNA strand has a mutation, it may well give rise to a non-functional cell or it might give rise to a cancerous cell. In both cases, of course, we want to go through apoptosis. If that DNA checking enzyme does not detect that DNA mutation, that mutation is going to be passed down to the daughter cells. Okay, So it’s good to keep in mind that we do have enzymes to check this process for DNA mutation. And another safety net we have in our cells is what’s called this telomere shortening that takes place with every round of cell division and the telomeres are these end caps of chromosomes. And you can see that every time a cell goes through mitosis, that those telomeres get shorter and shorter. And this is another safety net, like I said, in order to make sure that a cell only goes through a certain number of divisions before that cell becomes either dormant or dies. So you can imagine every time it’s replicated, when that DNA is duplicated, there might be another chance for an error to occur, right? So of course, if it’s gone through 50 divisions, there’s a higher chance there could be a mutation. And it could be a non-functional cell or dysfunctional cell or it could become a cancerous cell. So it’s best to program that cell to go through apoptosis once the telomeres are a certain length, right? So those are a couple of things the cell can do to try and reduce the risk of cancer from developing. And of course, cancer is a huge problem everywhere in the world it touches lives. And I don’t need you to memorize any of this, but it’s always good to know the top three. Let’s say. Cancers that affects Canadians So you can see (biological XY) men and (biological XX) women with prostate cancer and breast cancer affecting quite a large percentage of people, followed by lung cancer and then colorectal cancer. You’ll notice actually on this list that skin cancers such as basal cell and squamous cell skin cancers are not listed. Skin cancer unfortunately, is a very common cause of cancer as well. Okay. So just things to keep in mind. Don’t need to know the order or anything, but as long as you are familiar with the top three and of course, you can see that if we’re thinking of the number one cause of cancer. Most people would say smoking. And you might be interested to know that in everyone – including(biological XY) males and (biological XX) females. That not only does it cause lung cancer, the different nasty chemicals in smoke can also be risk factors for other types of cancer as well. Okay. So one of the best ways to prevent cancer is of course not to smoke or expose yourself to second hand smoke. Okay, so what is cancer? How does cells become cancerous? Let’s go through this. You probably know that cell growth or mitosis becomes uncontrolled in cancerous cells. So that’s part of its definition. And of course I’ve got this cell cycle picture here. And you can imagine the cells going through G1, S-phase, G2 phase, and then of course our mitosis phase prophase, metaphase, anaphase and telophase. You probably remember that. And as the cell goes through this cell cycling, you probably can imagine that this process is tightly regulated, right? The rate at which the cell goes through mitosis is tightly regulated. And there are some specific genes that regulate, control the rate of mitosis. And they’re nicely called regulator genes. And they would code for things like growth factors and growth inhibiting factors. So you can imagine that growth factors are the ones that will increase the rate of mitosis. And growth inhibiting factors are going to be the ones that promote that cell from exiting that cell cycling pattern. And they will either become then functional cells or perhaps they will become old and when they’re old and they’ll die, right? So there’s tight control over the rate of mitosis. So not only is it important to control the rate of mitosis of a cell, it’s also of course important to control the rate of apoptosis, right? We, we know that we need to get rid of cells when they become old, or potentially their DNA becomes mutated, or they become dysfunctional. And ideally in a tissue, you want the same rate of mitosis as apoptosis. And we’re talking about an adult here, so their organs are fully, full size. So for example, blood cells or the liver, et cetera. You want the same amount of mitosis as there is a apoptosis, so that organ maintains its function. Right? Now, you can imagine that if the DNA sequences for any of these regulatory genes are mutated, so if it’s say the growth factors are mutated or the growth inhibiting factors are mutated. Or maybe it’s the genes that control the rate of apoptosis. If any of those genes is mutated, that might result in either excessive mitosis or a lack of apoptosis to occur, right? And those of course, are the two scenarios that we see in cancer. Now, we could brainstorm and think about what can cause DNA mutation. You might remember from lesson two that we know certain viruses can lead to DNA mutation which can give rise to cancer. We talked about human papilloma virus or HPV, which can convert or mutate DNA. And that could end up in cervical cancer. You probably know that radiation or exposure to gamma radiation or excessive x-rays can also cause damage to DNA. Here’s a photo of a UV, UV light, and you can see there’s some damage done to our our DNA right here. And of course that’s one of the leading causes of skin cancer is excessive UV causing DNA damage in skin cells. You can imagine that different chemicals such as asbestos or the chemicals in cigarette smoking also can cause DNA mutation. And then of course, we talked a little bit off the top about, there can be spontaneous errors that occur during normal DNA synthesis. So every time that cell goes through mitosis and they have to duplicate their DNA. If the DNA is not duplicated perfectly and the DNA checker enzymes miss that error, then that error could be passed down to a daughter cell without apoptosis happening. And that could well, any of these of course, could well lead to mutation that gives rise to, if it’s in these regulatory genes, could give rise to excessive mitosis or a lack of apoptosis, right? Hopefully that makes sense. This last line is really interesting as well. And this is something that Terry Fox actually speculated about. And this last line says. Rapid rates of mitosis during injury repair may increase the risk of errors occurring. And I just want you to think about that for a minute and I’ll tell you the story of Terry Fox. And you can see why all of a sudden he speculated that this would happen. Now of course, we know Terry Fox, a Canadian hero who attempted to run across Canada in order to raise money in support of cancer research. Of course, we know he was stopped short in Thunder Bay when the cancer had spread to his lungs. And he could no longer run his one marathon per day, if you can imagine him performing that feat on one leg. Now, I’m not sure if you know what kind of cancer Terry had, but he had a cancer called osteosarcoma, which is cancer of the bone, which is why his leg had to be removed, it was actually cancer that was found in one of his leg bones. Now, before he was diagnosed with cancer in that that bone, he’d actually been in a in a vehicle accident and had sustained some damage to that same leg. So of course, when he was diagnosed with cancer in that leg, he thought it was quite the coincidence. And he started speculating this, hey, maybe during this healing of my leg, where obviously there was rapid rates of mitosis. Perhaps there was more chance that there was a DNA error during DNA duplication and that error gave rise to cancer. Okay, so I’m hoping that helps explain that sentence and that’s actually found to be true. Now I wanted to put this up at the top too, because I think it kind of blows people’s mind when they think that cancer is actually a genetic disease. I think for most of us, when we hear the word genetic disease, we assume that that means it’s an inherited disease. And certainly there are genetic diseases that can be inherited. And definitely not all genetic diseases are cancer. Really what a genetic disease means is there’s a mutation in that genome. And so of course you can see, yes, that’s exactly what happens when cancer occurs, is a regulatory gene is mutated. Now of course, you don’t have to be born with that. You can develop cancer later in life as a result of any one of these things we’ve just listed, you can certainly be born with cancer. It can be inherited. You can be born with a gene mutation that’s likely in one of these regulatory genes that gives rise to cancer for you. But we also know that you can be born with other inherited genetic mutations that don’t give rise to cancer, but give rise to other diseases such as cystic fibrosis or Huntington’s disease for example. And we also know that not all diseases you’re born with you you inherit through your genome. Some diseases that you’re born with can be things like cerebral palsy. You’re born with that, but it’s not genetic at all. All right, so moving on, I’m hoping you’re getting the sense as to those words and how biologists use them. Again, these are probably big reminder pictures from anatomy and physiology. And I just wanted to put this out there, just to get our minds back in the swing of thinking of DNA and what DNA in the cell is used for. So remember, you’ve got 23 pairs of chromosomes. And along those chromosomes, of course you’ve got thousands of different genes and each gene codes for a different protein. So we’ve got Gene 1 here, coding for one protein, Gene 2 coding for another protein. And we know what happens is say we wants to make more of this protein that’s coded by Gene 1. This gene one would be transcribed into messenger RNA. And then that messenger RNA it would be used in a translation process in order to string amino acids together to form that protein that we need. Okay, so let’s take a look at what happens when a gene is mutated. Say it’s mutated by a virus or by asbestos, or by cigarette smoke. Now of course, there’s three types of different mutations that can happen to DNA. And a lot of these mutations don’t actually give rise to cancer. A lot of them will just give rise to actually nonfunctional products. So let’s take a look. One type of mutation is an insertion, and it’s just what it sounds like. We can see that we have a nucleotide that’s being inserted. So here’s our starting sequence of nucleobases. So you probably remember guanine and adenine and cytosine and thiamine. So here’s our order. And you can see with an insertion mutation, what happens is we’re inserting and I just put a highlight, an additional nucleobase in there, an adenine, ok. So now we have 10 bases instead of nine. And so you can see that that’s going to actually shift – do remember that basically it’s codons or triplets that code for specific amino acids. So you can imagine if we’ve all of a sudden added a nucleobase right in the middle that the rest of our codons are going to be out of sequence now. So it means every amino acid after that insertion is now going to code for something different. Instead of glycine, maybe all of a sudden, now it’s going to code for valine, et cetera. So the first half of the protein is going to be correct, but the second half will not be. So this will likely result in either a dysfunctional protein that doesn’t work, might be completely non-functional. Or if it happens to be in a regulatory gene it might well give rise to cancer. A substitution mutation. So you can see here, instead of cytosine, adenine is getting put in its place, so it’s a mistake, we end up with nine bases still. So that means the sequence of triplets is still on target. And that means again, the first triplets are going to be fine. We still get tryptophan and phenylalanine. But this middle one say this is where the mutation was and so that triplet is going to have an adenine now instead of cytosine. So it would code for a different amino acid here instead of the one it’s supposed to. So basically just be one amino acid in that whole protein that might be wrong. And that might not actually affect the protein itself. It may well still be able to carry on its function. Deletion is just what it sounds like. Where here we’re deleting cytosine in the sequence, so we’re ending up with eight bases. So again, you can see that the first few codons may well code for the correct amino acids, but everything past that deletion will code for the wrong amino acid now, so this protein is going to be quite messed up just as this one is. So it might well lead to just a non-functional enzyme can’t really do anything. If it happens to be one of those regulatory enzymes that we need. Then it may well give rise to cancer. Assuming that our DNA checker enzymes and the cell hasn’t gone through apoptosis, ok. So you get the sense that there’s quite a few things that could happen there. And again, just to give you a picture as to how this could play out. Like I was saying, this type of mutation, say here, where we only have one substitution event. It might well mean that the same, basically the same or similar protein is going to be coded for us. So here we’ve got a red amino acid, a green one, and a blue one. Here’s a red, a green and a blue one. So it might well be, and you might remember too that there’s quite a few codons. There’s about three codons that code for glycine. And if saves this one that’s been affected and it happens to be basically maybe this cytosine is switched out for a different amino acid. And that sequence of three still codes for glycine, then we’re still going to have glycine put in. Even though the sequence is slightly different. So it might mean that nothing actually ends up happening and we have a normal happy protein. So we’ve had a mutation because we end up with the same product. We call it synonymous, just like synonym if you’re thinking of words. So for example, two words that mean the same thing. Okay, and then over here we’ve got a mutation that’s created. You can see that instead of the blue amino acid, we’ve got a purple one. And it pulls our protein into a different shape. And now our protein is likely not functional. So that mutation of course, is called nonsynonymous. And this, again, there’s basically three scenarios that could play out for it. It may well have no effect on the cell. Maybe the cell doesn’t really use much of this protein, so it doesn’t actually affect it at all. A lot of proteins aren’t used that much. Or sometimes there’s back-up proteins, right? Where if this one is messed up, there’s other proteins that do the same job, so there’s no real net effect on the cell. So that might be a scenario or it might mean that that cell becomes slightly dysfunctional but not cancerous just less functional than normal. Or it might be in one of those regulatory genes that controls the rate of mitosis or the rate of apoptosis. And therefore it might give rise to cancer. Okay, so we know this word neoplasm means new growth. And of course, if we’ve got new growth, that cell is no longer responding to normal genetic controls. It continues to reproduce, even though there’s no need for that cell to reproduce, we’ve got sufficient cells in that tissue. And when it does so, of course it’s going to start depriving other cells, presumably more functional cells in that tissue, of nutrition. These cells, when they go through mitosis like this, they become basically nutrition hogs. And so that means the healthy cells nearby become a bit starved and of course that’s going to reduce their ability to function properly. Neoplasms consist of atypical immature cells, which we saw in the last lesson. We notice they became an undifferentiated and their morphology changed. In a young healthy person, usually abnormal or cancerous cells will be recognized by the immune system and destroyed. You probably remember the natural killer cells are really good at doing this. However, of course, at times cancerous cells evade or sneak by the immune system. And of course that’s how some people do you end up with cancer. Now, the characteristics of each tumor that grows really depend on the type of cell from which the tumor arises. So a lab technician, when they are looking at a biopsy that’s taken from a tumor, let’s say they’re looking at a biopsy that’s been removed from the lung. They can tell whether this cell came from the lung. Is it a lung cell cancer? It’s in the lung. But sometimes of course, cancers spread through the body. So perhaps that tumor that’s in the lung, it’s actually got thyroid cells. And this person has thyroid cancer that has spread to the lung. So a lab technician would be able to tell that based on what they can see under the microscope, where that cell came from. Each cell has a unique structure and growth pattern. And now, when we talk about cancer, sometimes we say cells go through rapid rates of mitosis and that’s not actually accurate. In cancer. It’s not a faster rate of mitosis that each cell does. It’s just that more cells are going through mitosis at the same time. So of course you can picture, our abnormal cell and one of its regulatory genes is mutated. So it’s going through these rounds of division with fewer cells going through apoptosis. And as a result, this mass grows. Okay? Now you can see that it’s still within our tissue, it hasn’t spread out. So we would say this is a tumor at this point. And we talked about this in lesson 2, that basically there’s two types of tumors. There’s benign tumors, which are not considered cancer, they are slow-growling, and the cells are still fairly differentiated. However, they’re growing faster than normal. Tumors are benign tumors are often encapsulated. They’re freely movable on palpation. So when you move them with your finger, say near the surface of your body. And a benign tumor hasn’t metastasized. And of course once removed, if the doctor performed some surgery, removes it, it won’t reoccur. The only time that really damage takes place, it is when that tumor compresses on adjacent structures. So perhaps blood vessels. And of course, if this is in the brain, that would be quite unfortunate, is that tumor were to grow, as you can imagine, it would then start compressing the neurons of the brain and taking up volume. And as it takes up volume, it’s going to increase the intracranial pressure in the brain. And what that can do is it can basically start pinching off capillaries. And when you pinch off capillaries to the brain, there’s less blood flow to the brain. Your neurons, of course, need a constant supply of oxygen and glucose and nutrients in order to stay alive. And if it becomes deprive, then you’re going to see neurons start dying. Okay? So that’s one area of the body where benign tumor can have really serious consequences. Now in terms of naming, biologists tend to use the suffix -oma to indicate a benign tumor. So for example, an adenoma would be an epithelial tumor. There are some exceptions. Glioma or a lymphoma. These are actually malignant tumors, can tell this is in the neuroglial cells. And this is talking about white blood cells. Where unfortunately they’ve been given the ending -oma. Even though they’re cancerous. The second type of tumor we talked about in Lesson 2 as well. This is a malignant tumor and its term malignant when it invades surrounding tissues. So we know that those cells are immature, they’ve undifferentiated. They’ve become more like stem cells, instead of functional cells, they’ve become non-functional. They’re dysplastic or they’re anaplastic cells. They’re going through rapid reproduction. And normally cells have what we call cell-to-cell contact inhibition, which means that when a cell comes close to its neighbouring cell, that’s a stimulus for it to stop growing and stop going through mitosis. So that would normally be what happens. But if a cell is cancerous, it’s lost that ability. It comes right up close to its neighbouring cell and it still goes through mitosis, even though it’s quite close to the neighbouring cell. So yeah, we’re going through rapid reproduction and we’ve lost the ability to go through the same rate of apoptosis. The other thing that cancerous cells typically have are abnormal cell membranes. They may have altered surface antigens, which of course is helpful for natural killer cells. to sense, detect and then signal them to of course, destroy these cancerous cells. These cells don’t tend to adhere to each other like normal cells in a tissue do, which is problematic. And it means that it’s easy for them to break off and start spreading to other areas of the body. Now of course, they typically spread to other tissues through the bloodstream or through the lymph vessels. Now biologists tend to use the suffix -carcinoma, such as adenocarcinoma. Here’s adenoma, benign tumor, adenocarcinoma for a malignant tumor. And of course, if the surgeon isn’t able to get all of the cells of that malignant tumor, some of them have spread, so they’re not able to remove all of them. Then that cancer, of course, can reoccur. It’s still present. And once it gets big enough again, again, there will be more signs and symptoms. This is a really nice cartoon to show the difference between benign and malignant tumors. So you can see the benign tumor is capsulated. It’s more slowly growing and the cells are more normal. They’re less anaplastic, they’re little bit more differentiated. Our malignant tumor. You can see that it is not capsulated. Some of these cells can freely break off. And you can see that of course, you’ve got blood vessels throughout all of your tissues. Some will, some may well break off and then travel through the bloodstream. And then you can see that some of the healthy cells surrounding started perhaps dying. maybe, they’re getting starved for nutrient and oxygen. Or perhaps they’re cancer cells that have stopped that are, that are dying as well. Again, for similar reasons. Here is a benign tumor of the breast, so you can actually see the capsule. And you can see that this malignant tumor over here is quite a bit different in its shape. I love this summary table. I think we’ve gone through all the differences now of benign and malignant tumors. So this is just a handy table to maybe cover up and use as you’re studying to see if you can remember the big differences. And I’m wondering if you’re, you know, kinda contemplating, I don’t know if you’re into astrology. But of course, the, the cancer sign is a crab right. And this actually dates back to Hippocrates, the Greek physician who lived 460 BC. He’s considered the father of medicine. He actually, he coined the term carcinos. It’s a Greek term, carcinos and used it to describe tumors. And he noticed that the tumor is that we’re spreading had these finger-like projections that were reminiscent of the shape of a crab. And so later, like 500 years later, they’d been using the word carcinos, which became carcinoma of course. And the Romans actually started using the words cancer from the Latin word for a crab to describe the same thing. Let’s talk about malignant tumors now. So carcinomas. When we talk about carcinomas, we’re talking about epithelial cancers. This accounts for 90 percent of cancer is that humans are affected with. So arising from epithelial cells – do you remember from anatomy and physiology that you have four tissue types? You have epithelial cells, connective tissue cells, muscle cells, and neural cells. Okay, so epithelial cancers are the most common. And so this is just to practice out your vocabulary. So adenocarcinoma, you would say, Okay, this is a malignant tumor of the epithelial cells of the gland. Adeno, meaning gland. Squamous cell carcinoma Squamous cells that they’re talking about are in the skin. You might remember epithelial cells of the skin are squamous. Melanoma. You’ve probably heard that one before too. So you know that it’s the melanocytes of the skin that have become cancerous. And those melanocytes are epithelial cells, specialized epithelial cells. Okay, So if we move on to connective tissue and muscle tissue, so remember your connective tissue as bone and cartilage and blood – is connective tissue. And of course, muscle tissue is your third tissue type. Now altogether, connective tissue and muscle tissue is called mesenchymal tissue. because they both come from the mesenchymal stem cell lineage actually gives rise to all of these things. So if there’s a cell that has become cancerous in this lineage is called a sarcoma. So Terry Fox, I mentioned had osteosarcomas. So you could tell this is cancer of the bone. Rhabdomyosarcoma. This refers to cancer of striated muscle. Chondrosarcomere. You could probably picture chondrocytes, you know that’s cartilage. Glioma. We talked about that a few slides back. So this is cancer of the neuroglial cells. So you could think of your, you know, you’ve got six types of neuroglial cells. You probably remember astrocytes, ependymal cells, microglial cells. These two are the most common astrocytoma and ependymoma. Now, you might think, well, what about cancer of the brain? Is that neurons have become cancerous. And no, it’s not actually brain cancer is typically a neuroglial cancer. And that might make sense because we know neurons don’t go through mitosis. So it’s less likely that they’re going to become cancerous. And then lastly, you’ve probably heard of different cancers that have unique names that had been possibly named after someone such as Hodgkin’s disease, Wilms tumor, or some that don’t follow that naming pattern with carcinoma sarcoma as the suffix. They might be things like leukemia. And again, you could probably figure this out. This is cancer of the white blood cells or lymphoma as well. Specific type of white blood cell lymphocyte. Again, don’t feel you have to remember names (e.g. Wilms) That’s not important. Basically, we’re just learning how these things are called. The next slide, beautiful diagram just illustrating how metastasis occurs. And of course, you likely know that cells basically break off that primary tumor and start spreading through the bloodstream or through the lymph vessels. Now, it might astound you that actually most cells die on route. And I didn’t know that myself. Actually most cells die on route. But unfortunately of course, some do make it. And they store it again, they lodge into a different tissue. Say the, the lung or the liver or bone tends to be popular secondary sites for cancer. And it starts, of course, growing, creating secondary tumors. Here’s another table from one of the textbooks that lets you practice that nomenclature. So fatty tissue, it’s a benign tumor, lipoma. If it’s a gland tissue adeno, but it’s malignant adenocarcinoma. If it’s a fibrous tissue, sometimes it’s used fibro prefix, fibrous sarcoma. What is oncology again, you probably know this. The study of malignant tumors or cancer. So a malignant tumor – what’s so bad? Why does it kill you? Firstly, a lot of things, of course start going wrong. One can be the mass compresses blood vessels as we talked about in different brain cancers, pinching of capillaries and oxygen and nutrients to healthy tissue. So healthy tissue cell start dying, inflammation of course, would start occurring in that zone because of course, anywhere where cells are dying, inflammation is going to occur. And both those things can again mean that there’s a lack of oxygen. And nutrients going to those tissues, and those tissues become less and less functional. So of course, that’s a huge problem. The second huge problem is that some tumor cells secrete enzymes, and this is pretty nasty. So this one here, collegenase, you can again picture what it does. Basically it breaks down proteins. Remember a lot of your connective tissue actually has collagen as a supporting protein. So if you break down that supporting tissue or a supporting protein, it’s easier for that cancer cell to infiltrate that tissue and spread and spread and spread. So that’s a problem of course. And of course it means that tissue loses its integrity. Some tumor cells secrete hormones which create really weird effects depending on which hormone is being secreted. So you can imagine if, say this, all of a sudden this tumor cell starts to secrete calcitonin or maybe it starts accreting parathyroid hormone at an abnormal level, you can start changing things in the body. You can start changing blood calcium levels. You might not think that would occur with cancer, but it can, when they start producing hormones at weird levels like that, you can have endocrine side effects. Then some tumor cells start secreting their own growth factors which promote their own growth, basically stimulating them go to go through more and more cell cycling and can also actually encourage, let me put this one up. Encourage the growth of blood vessels, which we’ll get to in a sec. Inflammation we covered in lesson 2. So we know that it can be helpful, can bring in white blood cells, which of course will gobble up debris and can help set the stage for healing. And perhaps it’ll bring in some cells that will recognize that cancer and start to get rid of those cells. But we know that the downside of inflammation is it can mean that there is a bit of hypoxia, a bit of collateral damage done to some healthy tissue in that area. So it can and especially if it’s over a long period of time, chronic inflammation can lead to a progressive reduction in organ integrity and function. So I’m hoping you’re getting this says the big problem with cancer is our organs can become less and less and less functional until they can no longer sustain life. Now, I just mentioned this already that those growth factors at times can promote the development of new capillaries. That process is called angiogenesis. Angio meaning blood vessel genesis, meaning the creation of new blood vessels. And you’re thinking, well that’s weird. Why would a cancer want to promote the development of new capillaries? And it’s a great strategy actually because if you bring in a new capillaries to that tumor, then your bringing in a food supply, aren’t you? You’re bringing in more oxygen to that tumor. You’re bringing in more nutrients. And of course that tumor cells just going to, tumor is just going to thrive. Those cells, will, they need all of that energy in order to go through those rapid rounds of mitosis are with all those cells going through mitosis. And of course that’s just going to make the problem worse. That tumor is going to get bigger and bigger. Now, there are some new drugs out there that mimic what are called Anti-angiogenesis factors. And that’s a really good idea. If you use those drugs, then theoretically you would block angiogenesis. You would block the development of new capillaries. So you could basically starve out the tumor, prevent capillaries from going into it, and presumably that tumor would start dying. And so there is some research that shows at times it can be helpful. However, what they found to be a problem that goes along with this idea is that if you don’t have blood vessels going to that tumor, then the chemotherapy, which is drugs that are typically distributed through the body, through the blood vessels, wouldn’t get to the cancer. And you of course, need the chemotherapy drugs to get to the cancer in order to be able to kill the cancer. Now, how do you know you’ve got cancer? Now there’s eight warning signs. This one of course would be a red flag. Unusual bleeding or discharge anywhere in the body. A change in bowel or bladder habits. So prolonged diarrhea or discomfort. Okay. So maybe a blockage, even someone is constipated all the sudden. Change in wart or mole. So you should always be checking your skin, of course, to make sure that you don’t have any skin cancers developing. Sores that don’t heal. Okay. That’s something that should be checked out. Unexplained weight loss, anemia. So that might well mean that the person has, again, more bleeding internally or low hemoglobin. If there’s a persistent cough or hoarseness or even a solid lump, usually, that lump is painless at the beginning. And then when that lump gets bigger and bigger, that’s when it might start causing pain. But lumps definitely should get checked out, especially if they’re in the breast or testes. So you should be checking those things all the time. So here we’ve got someone doing a breast self exam which should be done. So look for lumps. So as mentioned at first, that lump might well be painless, but as it gets bigger, so you would see pain severity depends on the type of tumor and its location. So pain may be absent until very late stages, so that might be painless until it’s much bigger. And of course, once it’s much bigger, that’s when it starts pressing on sensory nerves and causing pain. And that, you know, when it’s bigger too, it starts stretching capsules. So if it’s in the kidney or liver, and the nociceptors in the kidney or liver tend to be in the capsules that surrounds them. So again, they have to get pretty stretched. So unfortunately the tumor is usually fairly well advanced before pain becomes a signal or a sign. Secondary causes of pain can be, of course, chemicals are mediators that are released by that cancer or from the inflammation that takes place around it. Remember, we talked about inflammatory chemicals and how some of them, such as bradykinin and prostataglandin can trigger nociceptors. If it’s an open wound, you may have an infection. And of course then that infection, if it’s bacterial or virus, is going to lead to inflammation and some of these painful pain inducing chemicals being released. Ischemia, so again, nociceptors are very sensitive to lack of oxygen and that can trigger them for sure. And they’re also irritated by blood. So nociceptors if they’re in contact with blood, will typically be triggered. We talked about obstructions. So again, that would be a local effect for sure. So if a tumor is compressing a duct or passageway, might be the blood vessels, that might be lymph vessels. So you don’t get proper lymphatic draining, for example, that could lead to swelling in the body. The lymph fluid isn’t able to drain. So that could be a sign. You’re getting swollen in a particular area. If it’s compressing the digestive tract, again, it could mean that you’re not able to swallow food properly if it’s near your esophagus or maybe become constipated if it’s lower down. If it’s blocking bronchi, it might be making breathing more difficult. If it’s pressing on a nerve, it may lead to pain or a tingling sensation or loss of sensation. And then of course, we know that surrounding cells could start dying. We might not be able to replace those dying tissues as quickly as they’re dying, which could lead to ulcers and of course, bleeding. So those might be local effects. Here are some great pictures from one of the textbook showing you how tumors can cause obstruction. So here in the bronchi or here around the digestive tract. Now, if we’re looking at systemic effects of malignant tumors of course, you can imagine that if your body is basically trying to battle this cancer or cancer is consuming quite a bit of your energy, that the rest of your body is a bit starved for energy. So you might feel tired. You might experience weight loss. You might not feel like eating. The tumor cells are very hypermetabolic, right. They’re going through rapid rounds of division. You might experience anemia. So that might be because of blood vessels being disrupted (e.g. inflammation or suppression of either bone marrow or kidney) by tumors or destroyed. And of course, if you’re not delivering blood than tissues are going to be poorly oxygenated, they’re going to experience nutritional deficits as well. If you have nutritional deficits from not eating properly, then again, it could affect the amount of red blood cells and hemoglobin your body is producing, which could lead to anemia. So of course you’re going to be tired if you have anemia. And it might well, again, reflect bone marrow depression. So that term basically means a reduced rate of mitosis of red blood cells, lower red blood cell number, lower white blood cell number. So big problems there. Severe fatigue could be caused by things like inflammation. Your body’s doing a battle course, by not eating properly and by having poor oxygen delivery to your tissues. It might be things in your life too that are contributing you to feeling fatigued. It might be a rigorous treatment schedule. You might not be able to sleep properly. There might be some psychological factors including depression, especially if you’ve just been told you’ve got cancer that can affect your mindset a lot. You could see effusion. So you can imagine, for example, in the lungs, you might see quite a bit of fluid building up in some of those cavities which can then impact things like breathing or movement of the ribcage and heart and things like that. Infection. Sure. You might be more susceptible to infections, especially if you have lower white blood cell numbers. Or if you have a lot of these secretions. Anytime you have a lot of secretions in your body, especially in your lungs, you’ve got this warm wetness – bacteria, love living in that material. So cute, give rise to bacterial pneumonia, which of course could make things worse, if you all of a sudden they’re getting lung damage from, from bacteria at the same time, we mentioned fever is another systemic effect of malignant tumors. That’s part of the inflammatory response. If we go to this next slide, bleeding. Yeah, So we talked about tumor cells potentially eroding blood vessels, fewer red blood cells being produced per second. Of course, if you have fewer platelets and fewer clotting factors within your blood that you’re not going to be able to clot or form those natural band-aids as readily. So if tumors have eroded blood vessels, you have a harder time sealing those vessels so they would bleed longer than normal, which of course makes the problem of anemia even greater. Chronic bleeding is common in the digestive tract. You probably know your gastric mucosa. So the cells that line your GI tract, they have a fairly rapid turnover during normal circumstances, they live about seven days. But of course, if they’re getting injured because of this cancer growing and because of the inflammation around it, they might start really struggling to keep up with replacing those damaged cells. And that could mean that you end up having ulcers and chronic bleeding within that area. Now a paraneoplastic syndrome. This is that weird situation when a tumor starts to releasing a hormone for some reason and all of a sudden you have these really weird endocrine effects. So this is one of the more common types of cancer that does. this. It is a specific cancer in the lung called broncogenic carcinoma. And it produces ACTH. ACTH is a hormone that stimulates the production of glucocorticoids. If you’ve heard of Cushing syndrome, this is not a cancer, but it is a scenario that’s defined as an excessive amount of ACTH being produced. So a problem with the pituitary gland actually is Cushing’s syndrome. So you can see both broncogenic carcinoma and Cushing syndrome. both are conditions where you have too much ACTH. And ACTH produced from a pituitary grand stimulates the adrenal glands to produce glucocorticoids. So if there’s too much of this, then there will be too much glucocorticoids being produced. And we know from lesson two, we talked about the drug glucocorticoid in comparison to ASA and acetaminophen, that glucocorticoid has some problems of itself, especially if it’s an excess. We know it’s catabolic. It breaks down proteins. And that means that not only does this poor person have lung cancer, now they’re having things like fragile skin. They may well develop osteoporosis and of course, delayed healing. Another role of glucocorticoids is gluconeogenesis. You might remember it’s going to take that protein and converted into sugar. And if blood sugar levels go really high for a long period of time, it may cause this person to have diabetes or develop diabetes. A person basically is experiencing high glucose levels in their blood. It can make them insulin resistant, which can give rise to type 2 diabetes. The other thing glucocorticoids do is they stimulate the retention of salt and water in the blood. And if you have a high blood volume because you’ve got a lot of salt and water in the blood. High blood volume leads to high blood pressure. And that high blood pressure can lead to a lot of edema. Lots of blood pressure can make those blood vessels a little bit leaky. And when they leak, of course they give swelling in the areas they leak. So a person can have a puffy face or swelling in the torso can look like they have a beer belly. It can mean that they start losing potassium. So their blood might have low-level of Potassium called hypokalemia. So all of these things are problems because we know the levels of electrolytes are important in your blood for the course, proper regulation of your heart and muscles and neurons. We learn too, when we talked about glucocorticoids in lesson two, that they are an immunosuppressant, they reduce the activity of white blood cells. So that can put this person more at risk for infection. It stimulates the production of red blood cells. And also over a long term, it can make this person emotionally labile, which means that they become very emotional. They may have ups and downs, euphoria and then depression. Some really strange endocrine effects can occur while this person is having lung cancer. Okay, so of course it’s important to find cancer early. We all know diagnostic tests are important. We need better and better ones all the time. And in terms of tests, if I asked you what kind of tests do we do for cancer and Canada, you would probably say, well, we do some routine screening tests, right? Everyone’s heard of the mammogram. And in Canada, they recommend that for women after the age of 40, particularly if they have family members that have had breast cancer. So we would consider those women more at risk. Of course, age is also a risk factor. So you may be well recommended to go get a mammogram done every two years after the age of 50. Now this little bit in italics, I’m never going to ask you what age you should go for diagnostic tests. This is purely for your own information. The only thing that I might ask you about is what kind of routine screening you’re going or people in Canada go for. So breast screening, mammograms, cervical screening, we’ve talked about a lot. So you know that that’s the Pap test. I’m not going to ask you how often. It pretty much again, this is for your benefit. It depends on your previous test results. So most (biological XX) females after the age of 21 will be told by their doctor to go get tested every one to two to three years. Colorectal testing. There’s two types. There’s the stool test where they take feces and I’ll tell you what they look for when we get to that section. And this is recommended after the age of 50, you’ve heard of a colonoscopy as well where they look for polyps or growths in the colon with a camera. This is recommended again, if you’re at high risk you have a family history and it’s recommended when you get older, again, towards the age of 50 and afterwards. If you have a history of irritable bowel disease or if you have signs and symptoms, for example, if you’re seeing blood in your stool, then of course these types of tests would be recommended. We’ve all heard of self-examination. So you of course, can do this with breast, as was the testes looking for lumps and then skin looking for moles that have become disfigured. For example, blood tests, we’ve all heard of that. So person of course, could have their blood drawn if they’re looking at hemoglobin or white blood cells or red blood cells, high or low levels can happen if a person has cancer. And of course, it doesn’t necessarily mean a person has cancer. That can be other things that can cause those levels to change. Another time, of course they’ll do blood tests is during chemotherapy treatment because some chemotherapy can actually reduce white blood cell and red blood cell numbers and they don’t want to reduce those cell levels too much. So they’re not giving chemotherapy treatments too frequently. The person has enough chance to get their blood cell counts back to normal before the next chemotherapy treatment. Other things that you can look for in blood tests are tumor markers. And again, don’t feel you have to memorize these, but just to give you an idea to look for colon cancer, prostate cancer, testicular cancer, ovarian cancer and hepatocellular cancer. You can tell this is cancer of the liver. There are certain proteins that all of a sudden become elevated in the blood. And these proteins typically are markers that are basically proteins that are used to be exhibited when you were an embryo. So all of a sudden your tumor cells are becoming more differentiated and they’re producing proteins that are usually fetal in nature or embryonic. So CEA standing for carcinoembryonic antigen, PSA, of course, you’ve heard of prostate-specific antigen. And if there’s high levels of any of these, can be indicating that this person has that particular cancer. Human chorionic gonadotropin. This is again chorionic referring to placenta CA 125, and alpha fetoprotein. Now of course, to confirm that a person has cancer, you have to do a biopsy. But the next thing you might do before the biopsy is to do some imaging. Here is of course a mammogram where an X-ray is used. You’ve got a colonoscopy happening here where a camera is used to look for growths or polyps in the colon. So some good imaging tests. Sometimes genetic tests are done as well to see if a person is at risk for developing cancer. So again, it doesn’t tell you if a person has cancer, tells you if they are at more at risk. So BRCA 1, and 2 maybe present if the person has a family history of breast and ovarian cancer – it could mean that they are more at risk for developing those two cancers themselves. You may have heard of Angelina Jolie. We discovered that she, she suspected she did have these two genes as her mother had passed away from breast cancer. And when she discovers she did have those two genes, she elected to have a double mastectomy. And I don’t need you to remember the Philadelphia chromosome. But again, if a person suspects that they have a family history of chronic myeloid leukemia, then they may well have a genetic test done to see if their risk for it. Of course, we know imaging is a great strategy, it gives you a chance to visualize those tissues and see whether you can see any masses forming. In order to confirm, of course, that a cancer is present, you have to gather some of those cells either by scraping cervical cells for a pap smear or going in surgically removing some cells and then testing them to see, or looking at them to see whether they are malignant? And while you’re doing that, you can determine whether if those cancers are estrogen dependent tumors. So for example, some testicular cancers and some breast cancers are hormone dependent. And it’s a good plan to find out whether they are dependent on hormones. Because then of course you can use information in your treatment. You can try and starve them of those hormones to get rid of them. And we’ll talk about that later on. Here’s a great cartoon. It shows you, of course, the cervix, the entrance of the uterus. And how, of course, cancer may will develop in the cervix. So of course it starts out small and it hasn’t spread. So it’s called carcinoma in situ. It’s non-invasive. If it starts invading the cervix, we would say it’s cervix invasive. It may well spread to close by areas. So me well spread into the vagina. And you can tell that once it’s done that we’re breaching the basement membrane. So we’re going from dysplastic benign tumor to an anaplastic tumor that’s become malignant and it can well spread to other areas in the pelvic region, the whole uterus, maybe even into the colon, perhaps even into the bladder. So obviously pap smears are important in and in terms of spread, you can imagine that the first spread is going to be local. And it can be facilitated if the tumor cell is secreting some of these lytic enzymes that we talked about earlier like collegenase. It helps the tumors infiltrate that tissue. So for example, uterine carcinoma, carcinoma in the uterus. You can see that it’s in close proximity to the vagina, so may well spread there next, the next step after spreading locally is to spread to distant sites. And that’s called metastasis. And we talked about how cancer cells can travel through the bloodstream or the lymph fluids or other bodily fluids to regions that are farther away. And it really only takes a few tumor cells to survive that transfer. In order for that secondary tumor to start growing. So what you’ll notice here, I’ve got Grey’s Anatomy picture of a breast tissue. And you can imagine if a person has breast cancer, what the surgeon is going to do is actually going to remove some of these close lymph nodes to investigate whether any of those lymph nodes have breast cancer in them. So that surgeon is going to map how far that breast cancer has spread. So what they’ll do in order to figure out which lymph nodes to take is they’ll inject a tracer dye. And the sentinel lymph nodes will be the ones closest, of course, to the breast (cancer site). Those ones will dye blue. And those are the ones that are going to be removed. And again, taken into the lab, biopsied, are there cancer cells in them? If there are, then it’s indicative that they spread. So the surgeon may well decide to go in again and remove a bit more. Or may well, try to figure out how far it’s spread. Maybe do some imaging of the lungs and the bone, and the liver, and the brain and other sites that breast cancer typically can spread to. To start screening those places as well, to of course, plan for treatment. This process of spreading cancerous cells along membranes. And I’ll show you that in a second. So for example, spreading ovarian cancer through the peritoneal cavity, the peritoneal membranes. That process would be called seeding, Here is a disgusting metastatic tumor of the liver. And here’s the seeding effects shown in this really nice cartoon. So here we start off with this unfortunate primary ovarian tumor. You can see it spreads through the peritoneal membranes and even into the liver. This would be called seeding. Once we’re doing a biopsy, of course, to confirm if this person has cancer, then you’re going to hear the term grading, right? We’re going to grade that cancer. What does grading mean? So when that pathologist is looking at that biopsy under a microscope, they’re going to grade the cancer cells based on how different they look from normal. So grade one, they’re fairly well differentiated, pretty close to normal. And of course, you can imagine there’s four grades, grade 1, 2, 3, 4, which is not shown here. Grade 4 being the worse, the least differentiated, the most anaplastic. And these grade 4 cells are of course, likely going through more rapid rounds of mitosis and more likely to have lost cell to cell contact inhibition, most likely to spread. Now you’ll also hear the word staging. Now, what does that mean? And that basically describes the extent to which the cancer has spread through the body. Okay, so here’s a nice cartoon is showing you this unfortunate stomach cancer. And staging is typically done on what’s called the TMN system. And it’s easy to remember T stands for tumor. And the T number is graded one through four, as you can see here. And T is basically measuring the size of the tumor. So you can imagine again, one is small and four is going to be larger, right? So the bigger it is, of course the worse off you are potentially. The N number stands for lymph nodes. So if you were to look at surrounding lymph nodes, how many lymph nodes are involved. And again, this would be on a scale from one to 4. 4 being the worst. And then M stands for metastasis. And that’s for the spread. So documenting how far it has spread. And again, it’s on a scale of one to four. And this TMN system is going to be different depending on which cancer you’re looking at. So for example, in the stomach, a T4 or maybe this is five centimeters. But if we’re looking at a breast cancer may be a T4 is considered seven centimeters, right? So it really depends on the cancer. Each cancer, of course, it’s going to have its unique features and grow differently. So it will have its own classification system. Okay, So here is, of course, hopefully what you’re thinking Stage Zero was not on the diagram. Stage 0 carcinoma is in situ. Stage 1 and 2 cancer is limited to that organ or that initial location might be in a neighbouring structure, but fairly localized. Stage three, we’re spreading into surrounding structures and into the regional lymph nodes. And stage 4, we’re going to distant sites, ok. Now these terms all pretty much mean the same thing. Carcinogenesis. So the formation or creation of cancer, oncogenesis again, basically what is the process by which normal cells have transformed into cancerous cells? Okay, what happens to these cells? How did they become cancerous? And we would say that it takes many factors to convert a cell into a cancer cell. Typically it’s not just one mutation that does it. Typically there’s quite a few things that may be involved that cause several mutations. So there may be some environmental effects. So maybe some asbestos. Perhaps you have a genetic susceptibility to having some mutations that you have fewer DNA checker enzymes that check the DNA after it’s duplicated. From exposures to different viruses, such as HPV or hepatitis C virus for example. Smoking of course. I’ve just listed some more viruses already. And so basically any of these three categories can be involved in mutating or changing the expression level of different genes so that they become cancerous. Now those regulatory genes that we are concerned about, we can give them specific names. So if we’re talking about a proto-oncogene, what a proto-oncogene is, is it’s a gene that stimulate cell division. And we also have proto-oncogene that inhibits differentiation and death. Okay, so we’ve got these genes that are basically simulating cell cycling. Now, if these proto-oncogenes were mutated, they typically develop a dominant mutation. When they’re mutated, then they’re called oncogenes. And just like the name implies, those mutated oncogenes give rise to cell division that’s too fast, right and decrease the rate of cell differentiation and death, too much, right. So here’s this scheme. We’ve got proto-oncogenes in our body and there’s been over 40 that have been identified. So regulating the proper rate of cell cycling, they stimulate cell cycling and they inhibit differentiation and death. When you mutate them, they become oncogenes and they promote more cell division and less death and less cell differentiation. So it’s like you’re putting your foot on the gas too much, too much putting your foot on the gas. Tumor suppressor genes, you can tell again by their name what they’re normally supposed to do is they normally are supposed to suppress tumor, tumors from starting. So their job is to slow down cell division and to promote apoptosis. But when these genes mutate, of course they don’t do that. They don’t slow down cell division, right? They don’t put their foot on the brake anymore. And as a result, those cells become immortal. Basically they become cancerous. They go through rapid rounds of division without dying. Now, so here is my stop and go pedals. You can think about proto-oncogenes as we’re stepping on the gas too much. And tumor suppressor genes, then all of a sudden we’re not stepping on the brake enough. Is what happens when those guys mutate. Then the third type of gene that if they are mutated, can also give rise to cancer. And these genes are involved in DNA repair, right then DNA checker enzymes. And of course, there’s genes that control the rate of mutation, they’re DNA checker mutate genes. These genes don’t have a direct impact on the rate of mitosis or apoptosis, but they definitely control the rate that mutations are allowed. Hopefully they don’t allow any mutation. But of course, if the stability genes have been mutated themselves than this isn’t happening properly. And just to give you a sense as to how important those DNA checker genes are. p53, which is involved in regulating DNA repair. It’s nicknamed the guardian of the genome. We see p53 mutated in about 30 to 50 percent of all cancers that arise. So again, a nice summary table of different risk factors that of course can give rise to cancer. So let’s go through these things. So genetic factors, you may have a genetic susceptibility like Angelina Jolie, you may have BRCA1 and 2. And that might mean that you are more at risk for breast and ovarian cancer, for example. Viruses we looked at HPV as well as hepatitis viruses that can give rise to liver cancer. UV rays, of course, that put you at risk for skin cancer. X-rays, gamma rays are of course, linked to DNA mutation. We’ve talked about some chemicals such as asbestos, if you breathe that in, it puts you at risk for lung cancer. Different solvents of course, are out there as well. Don’t feel you have to memorize these solvents. If you were to think about any type of irritant that’s chronic. Just like with Terry Fox. If you have chronic healing going on or a lot of healing, there’s more mitosis, more chance of cancer developing. So for us with some people who have irritable bowel type diseases, such as chronic irritation in the colon that can…., such as ulcerative colitis that can give you a risk factor for colon cancer. The older you are, of course, the more rounds of mitosis you’ve been through. So you are more at risk for developing a mutation in one of those mitotic events and then diet as well. They found that a high fat diet or a diet full of smoked foods can give you greater risk factor for colon cancer as well as gastric cancer and then some hormones. So if you have a lot of estrogen in your body, and we’ll talk about this when we get to ovarian cancer. So in this slide we’re going to take a look at how a cell becomes cancerous. You’re going to see it takes quite a few assaults of that cell in order to create those mutations that then lead to cancer. So to start the ball rolling, what happens is pro-carcinogens cause the first irreversible change in cellular DNA. It’s not cancer yet. Typically we need further changes to the DNA. And those might well be caused by promoters, which would be considered hormones or environmental chemicals. Basically any other carcinogen that creates further changes in DNA. And of course, the changes that give rise to cancer would be changes that involve that cell, again losing those regulatory genes, the cells. If they’ve lost those genes, become less differentiated, their rate of mitosis increases. And perhaps we get a decrease in the rate of apoptosis. And as differentiation becomes less, those cells may start becoming dysplastic or even anaplastic. So typically we need continued exposure of carcinogens are promoters that give rise to more and more DNA mutations. So that those crucial genes are the ones that end up being affected that create that cancerous cell that has the ability to become malignant. And of course, in becoming malignant, it’s able to grow unregulated, and it’s able to detach and spread. So there’s a beautiful figure that shows the many assaults on DNA that typically have to take place in order for a cell to go from a normal cell to cancerous cell. So we can see that on the side we’ve got some carcinogens. So maybe there is some, there’s UV exposure, maybe there’s asbestos those maybe there’s HPV virus, perhaps smoking, and these assaults on the cell, they may cause our cell to become less functional, less normal, perhaps even proliferate. We may go past the point of reversible change. And that cell you can see with its membrane changing, it has to start evading the natural killer cells. So it has to become undetectable to natural killer cells. So cells that don’t display abnormal antigens. A lot of cancer cells do display abnormal antigens, in which case they would be destroyed by your natural killer cell. These guys that end up becoming metastatic, of course, are evading your natural killer cells. So they don’t have any signs on their cell membrane that they’re not normal. Here’s some other factors, of course, that can promote DNA mutation different food additives, such as we affect gastric cancer. Looking at smoked foods for example, industrial pollutants, radiation, all of these can assault your DNA. Okay, so risk factors, of course, we’ve gone through these a few times now, but DNA mutations. So perhaps you’re unfortunate as Angelina Jolie and you’ve have BRCA one or two. And you might know that or suspect that because you have a family history of say, breast cancer, ovarian cancer. If you’re exposed to viruses such as hepatitis C or HPV. If you’re exposed to UV, X-rays, gamma rays, of course. And we know that risk is increased with higher cumulative dosages of those types of things. We’ve mentioned asbestos. Don’t feel you have to memorize all of these things. Of course, chemotherapy drugs. The way they work is by altering DNA, causing DNA mutations, biological factors we’ve talked about age being important and diet being important and different hormone level exposures. So when we get to ovarian cancer, you you’ll see that if you’ve been exposed to estrogen for a long period of time or a lot of estrogen that can be a risk factor. Chronic irritation. We talked about Terry Fox for example. Okay, so I’m hoping you get a sense of it. It’s probably a good place to take a bit of a brain break. So why don’t we take a bit of a break and we’ll pick up the second part in the next video. I hope you have an awesome day and you enjoy these cartoons, and I’ll see you in the next one.
