Appendix: Summary of Lab Diagnostics using Immunological Techniques
APPENDIX
|
An array of tools and techniques have played a pivotal role in advancing our understanding of the immune system and have become indispensable applications in diagnostic testing. This appendix is a summary of some of these tools and techniques employed in immunological research and diagnostic testing.
- A1: Agglutination tests.
- A2: Antibody generation
- A3: Complement pathway testing
- A4: Complement fixation test
- A5: Enzyme linked immunosorbent assays (ELISA)
- A6: Enzyme linked Immunosorbent spot assay (ELISpot)
- A7: Immunoblotting (Western blot)
- A8: Immune cell isolation
- A9: Immunofluorescence microscopy
- A10: Immunohistochemistry (IHC)
- A11: Immunoprecipitation
- A12: Precipitin reaction
- Testing for general immune function
A1: Agglutination tests
Agglutination tests detect and/or measure the presence of specific antigen or antibodies in a patient sample. They utilize one of the functions of immunoglobulins, agglutination or the clumping of particles when antibodies detect the corresponding antigens. In agglutination tests, antibodies or antibody-coated particles are mixed with a patient sample containing the corresponding antigen. Agglutination indicates the presence of the molecule being detected in the tested sample. The agglutination reactions can be observed macroscopically as clumping or as the formation of an insoluble precipitate.
A1-1: Hemagglutination and blood phenotyping
The ABO blood phenotyping test is a hemagglutination assay, where agglutination of red blood cells (RBCs) is used to determine an individual’s blood type. Recall that the ABO blood group system is based on the presence of two antigens on RBCs, antigen A and antigen B. Based on the presence of these antigen individuals are classified into four groups, individuals with antigen A (type A), individuals with antigen B (type B), individuals with antigen A and B (type AB) and individuals who do not bear either antigen (type O).
During a blood typing test, patient samples are mixed with antibodies against antigen A and antigen B. If there is an antigen-antibody interaction, RBCs will agglutinate forming visible clumps. A positive reaction indicates the presence of the corresponding antigen on the surface. Thus, the blood type of a patient can be determined by observing the agglutination pattern.
 surface. A person with A-type blood has A-antigen on the RBC surface but not B-antigen. Consequently, this person produces antibodies anti-B that would reject any RBCs with surface B-antigen (B-type or AB-type). A person with O-type blood has no RBC surface antigen and can be transfused into any other person, since neither anti-A nor anti-B would bind these cells.")
Figure A1-1-1 Blood Groups. A and B antigens constitute glycoproteins on the red blood cell (RBC) surface. A person with A-type blood has A-antigen on the RBC surface but not B-antigen. Consequently, this person produces antibodies anti-B that would reject any RBCs with surface B-antigen (B-type or AB-type). A person with O-type blood has no RBC surface antigen and can be transfused into any other person, since neither anti-A nor anti-B would bind these cells.
Image Source: By OpenStax CC BY 4.0, via Wikimedia Commons
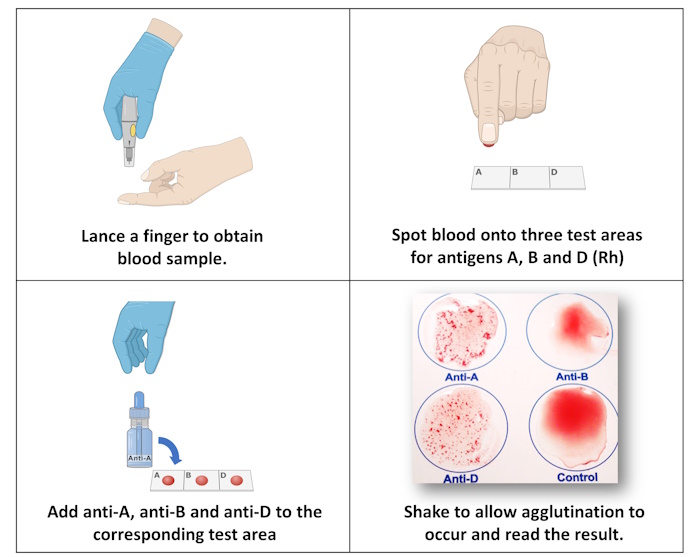

Figure A1-1-2 ABO Blood Typing. (Top) The procedure for blood typing involves spotting blood into three test areas and adding antibodies to A, B and D (Rh) antigens onto each labelled test area. (Bottom) Cell clumping indicates that the red cell has the test antigen on the cell surface.
Image Source: (Top) By Human Bio Media CC BY 4.0, via Blood Typing Lab Test Simulation; (Bottom) By Biology Corner CC BY 4.0, via BiologyCorner.com;
A1-2 Antiglobulin tests and detecting Rh incompatibility
Rh (Rhesus factor) incompatibility occurs in pregnancy, when Rh-negative mothers are exposed to Rh-positive fetal RBCs during delivery. Upon exposure, the mother will produce anti-Rh antibodies. In subsequent pregnancies these anti-Rh antibodies will be transported across the placenta to the fetus, which leads to the destruction fetal RBCs resulting in hemolytic disease of the newborn (HDN). The antiglobulin test, also known as the Coombs test, is an immuno-hematology assay that detects the presence of antibodies that lead to HDN. The tests make use of the Coombs reagent or anti-human-IgG antibodies to detect the presence of IgG antibodies.
In the direct antiglobulin (DAT) test, newborn blood samples are tested to detect antibody bound RBCs. The blood sample is mixed with the Coombs reagent. If the newborn RBCs are coated with antibodies this will result in agglutination. A positive DAT test indicates the mother has produced anti-Rh antibodies, which are responsible for HDN.
The indirect antiglobulin (IAT) test is performed on maternal blood to detect the presence of anti-Rh antibodies. The maternal blood sample is first mixed with Rh-positive RBCs. After incubation, the sample is washed to remove unbound antibodies, and the Coombs reagent is added to detect antibody-bound RBCs. Agglutination indicates a positive IAT test, which shows the presence of anti-Rh antibodies in maternal blood. The IAT test is often performed in the first trimester of pregnancy because RhD-immunoglobulins (RhoGAM) can be given to Rh-negative mothers to reduce the probability of sensitization and subsequent anti-Rh antibody production.
 The IAT test is performed during the first trimester to detect presence of anti-Rh antibodies in maternal blood. In the first step Rh-positive RBCs are mixed with maternal serum containing antibodies. Following a wash step the Coombs reagent is added to the reaction. Agglutination indicates a positive test for anti-Rh-positive antibodies.")
Figure A1-2-1 The Coombs test. (Top) The DAT assay is performed to detect the presence of maternal anti-Rh antibody bound RBCs in newborn with suspected HDN. A newborn blood sample is mixed with Coombs reagent containing human anti-IgG antibodies. Agglutination indicates a positive test for antibody-bound newborn RBCs. (Bottom) The IAT test is performed during the first trimester to detect presence of anti-Rh antibodies in maternal blood. In the first step Rh-positive RBCs are mixed with maternal serum containing antibodies. Following a wash step the Coombs reagent is added to the reaction. Agglutination indicates a positive test for anti-Rh-positive antibodies.
Image Source: By Rad~commonswiki CC BY 3.0, via Wikimedia Commons
A1-3 Treponema pallidum hemagglutination (TPHA) test
The TPHA assay is an indirect hemagglutination test used to diagnose syphilis, a sexually transmitted disease caused by the bacterium Treponema pallidum. It is a treponemal test that detects the presence of anti-treponemal antibodies in patient samples. The TPHA test is used as a confirmatory test to diagnose syphilis. It can also be used as a primary screening test for syphilis at all stages beyond the early primary stage of the disease.
TPHA assay uses RBCs sensitized with T. pallidum antigen. If anti-treponemal antibodies are found in the tested patient serum, the RBCs will agglutinate to form a smooth mat of cells at the top of the test plate. If antibodies are not present, the RBCs will settle to the bottom of the plate forming a compact button of non-agglutinated cells. Reactive results in a TPHA assay may indicate an active, past, or successfully treated infection. As such the TPHA test alone is not sufficient for a diagnosis.
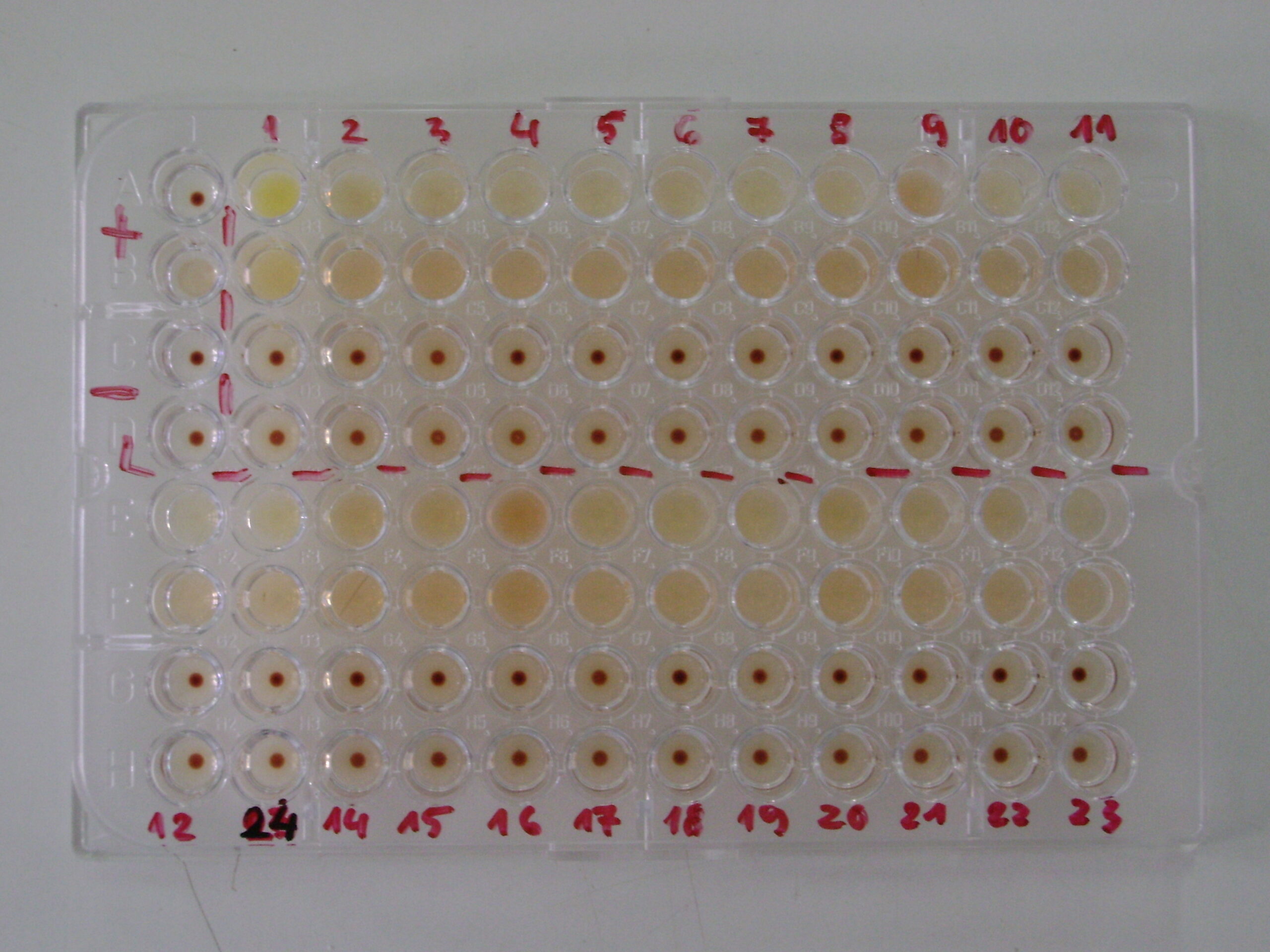
Figure A1-3-1: TPHA assay performed in a microwell plate. The left upper corner contains the positive controls, one with RBC aggregate seen as a dense button and one with agglutination observed as a smooth mat of cells. The negative controls are shown below containing two RBC aggregates. Lanes 1-4 show patient samples with the top two rows containing positive samples and the two bottom rows containing negative samples.
Image Source: By OpenStax CC BY 3.0 via Wikimedia Commons
A1-4 Tube agglutination test
The tube agglutination test is a technique used to detect the presence of antibodies or antigen in a sample. In this test, patient serum is incubated with a specific antigen or an antibody. If the target antigen is recognized by the antibody, a visible reaction occurs in the form of agglutination or clumping. Agglutination is observed macroscopically by gently tipping or swirling the test tubes and observing visible clumps. Alternatively, the degree of agglutination can be quantified using a spectrophotometer or by performing agglutination titers.
The Widal test tube method used for diagnosing typhoid fever is an example of a tube agglutination test. This test involves mixing patient serum with specific antigen derived from Salmonella typhi the microbe causing typhoid fever. Agglutination is indicative of the presence of antibody in patient serum. The Widal test has been replaced with ELISA and nucleic acid detection methods in North America. However, it is still widely used in developing countries due to low cost and availability.
 The patient samples is serially diluted (typically 8 dilutions 1:20, 1:40 etc). (Step 2) Antigens for relevant Salmonella serotypes are added to the wells. (Step 3) Mixture is incubated overnight and (Step 4) agglutination is observed. Agglutination is indicative of the presence of typhoid antibodies. This is a semiquantitative test, where the titre of the patient serum is equivalent to the highest dilution of the serum that gives visible agglutination.") A1-4-1 Tube agglutination test for diagnosing typhoid fever. (Step 1) The patient samples is serially diluted (typically 8 dilutions 1:20, 1:40 etc). (Step 2) Antigens for relevant Salmonella serotypes are added to the wells. (Step 3) Mixture is incubated overnight and (Step 4) agglutination is observed. Agglutination is indicative of the presence of typhoid antibodies. This is a semiquantitative test, where the titre of the patient serum is equivalent to the highest dilution of the serum that gives visible agglutination.
A1-4-1 Tube agglutination test for diagnosing typhoid fever. (Step 1) The patient samples is serially diluted (typically 8 dilutions 1:20, 1:40 etc). (Step 2) Antigens for relevant Salmonella serotypes are added to the wells. (Step 3) Mixture is incubated overnight and (Step 4) agglutination is observed. Agglutination is indicative of the presence of typhoid antibodies. This is a semiquantitative test, where the titre of the patient serum is equivalent to the highest dilution of the serum that gives visible agglutination.
Image Source: By Alhaj-Qasemet al. (2020) Diagnostics, 10(7), 438. CC BY 3.0
A2: Antibody generation
Antibody generation is a fundamental tool in immunology that allows researchers to produce specific antibodies for various applications. Today, antibodies are developed in the lab to recognize and bind a variety of target molecules such as proteins, peptides, and cells. Lab-made antibodies can be used in a wide range of applications including basic research, diagnostic assays, therapeutics, and imaging techniques.
There are two types of lab-made antibodies: monoclonal antibodies (mAbs) and polyclonal antibodies. B cells are key to generating both monoclonal and polyclonal antibodies. In monoclonal antibody production, a single B cell is selected to ensure the generation of an antibody specific to a single epitope. In polyclonal antibody production, a diverse population of B cells are selected to generate a mixture of antibodies that respond to multiple epitopes or regions of the antigen. Monoclonal antibodies offer highly specific and uniform responses while polyclonal antibodies provide broader coverage because they originate from a collective response of multiple B cells.
A2-1 Hybridoma technology
Hybridoma technology was the most commonly used method for generating monoclonal antibodies in the past. In this process, antibody-producing B cells are isolated from immunized mice and are fused with myeloma cells to form hybrid cells, called hybridoma cells. Hybridoma cells are cultured in the lab and once stable lines are established these cells can be used to produce limitless amounts of antibodies. Antibodies generated using hybridoma cells have high sensitivity and specificity.
The general steps of generating monoclonal antibody using hybridomas include:
- Immunization: The process begins by immunizing an animal (typically mice) with the antigen of interest using a series of injections over a period of several weeks. The foreign antigen will stimulate the immune system, leading to the production of antibody secretion B cells specific to the introduced antigen.
- B cell isolation: Antibody producing B cells are isolated from the spleen, a rich source of B cells
- Fusion: Isolated B cells are fused with a myeloma cell line, which is an immortal tumor cell line. The fusion is usually achieved using fusion agent such as polyethylene glycol (PEG)
- Selection: Hybridoma cells are cultured using specific medium that will support only the growth of hybridomas.
- Screening: Once established hybridoma cell lines are screened to identify those producing the most desirable antibody.
- Antibody production: Selected hybridoma cells are grown in large-scale bioreactors or cell culture to make large quantities of antibodies. Antibodies are secreted by the hybridoma cells lines into the culture media, which can be easily harvested, purified, and used.
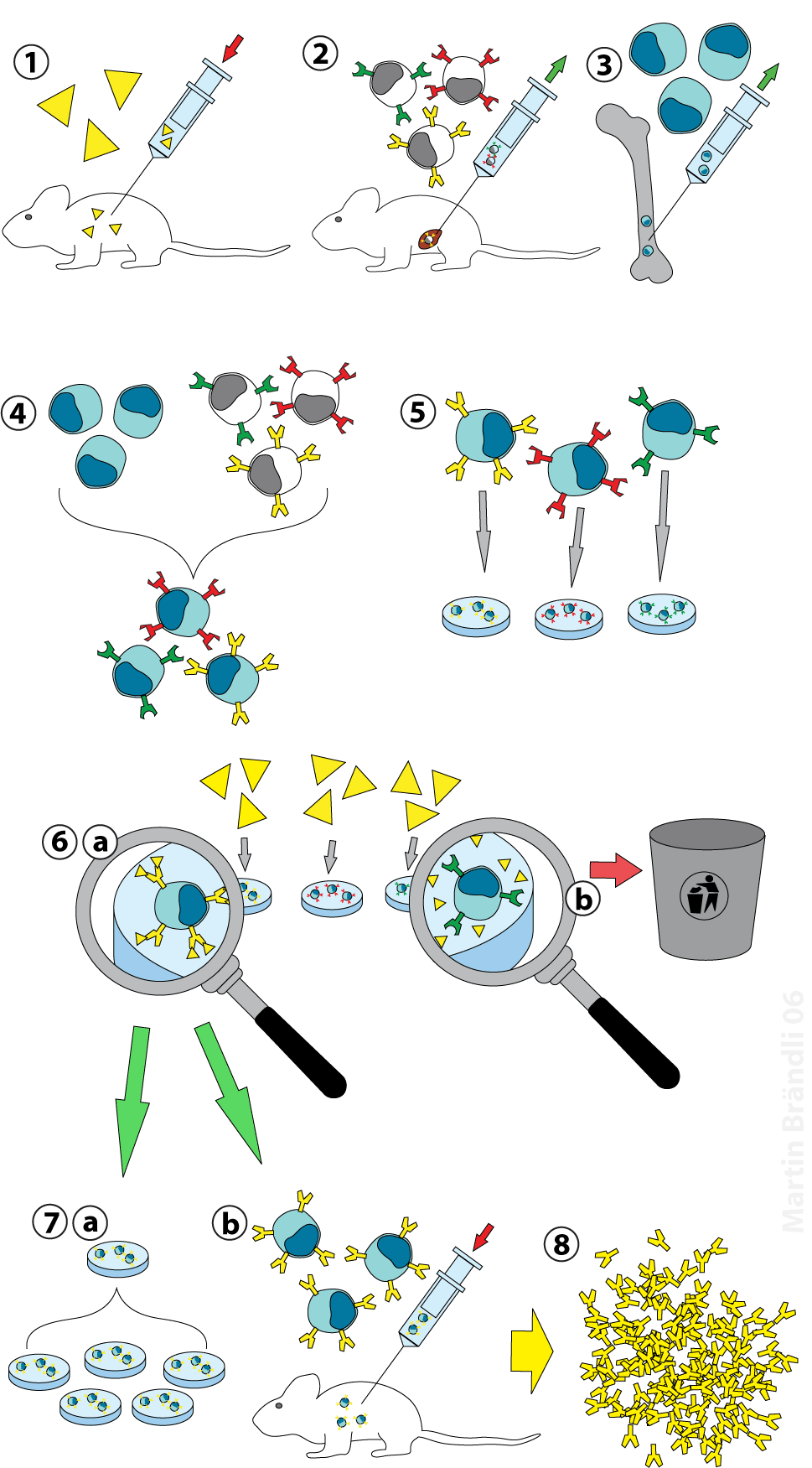
Figure A2-1-1 Hybridoma technology. To produce monoclonal antibodies (1) a mouse is first immunized with a purified antigen and (2) antigen-reactive B-cells are extracted from the mouse. (3) Myeloma cancer cells are also obtained and are (4) chemically fused with the B-cell to produce a hybridoma cell that has the B-cell’s capacity to produce antibody as well as the cancer cell’s ability to grow indefinitely in culture. (5) Individual hybridoma cells are grown and expanded into clonal populations. (6a) Each hybridoma clone is tested for its ability to bind antigen and (6b) non-responders are discarded. Hybridoma cells are then grown in culture (7a) or in animals (7b) to (8)produce large amounts of epitope-specific (monoclonal) antibodies that can be harvested.
Image Source: By Martin Brändli CC BY 2.5, via Wikimedia Commons
A2-2 Recombinant antibody technology
While hybridoma technology was instrumental in generating monoclonal antibodies for years, recombinant antibody technology has gained significant popularity in recent years for antibody production. Recombinant antibodies are synthetic antibodies generated using recombinant DNA technology. Initial steps involved in making recombinant antibodies are similar to hybridoma technology. Animals are immunized with the desired antigen and B cells are extracted from these animals. However, once B cells are isolated, instead of generating hybridomas, B cells are sequenced to map their VDJ regions. The mapped genes are then introduced into a host system such as bacteria or yeast using genetic engineering.
Recombinant antibodies are more desirable than the traditional hybridoma based antibodies because they can be fully humanized, making them more compatible when using as a human therapeutic. What is more, recombinant antibodies can be further customized based on the need of each individual application. Production of recombinant antibodies can be easily scaled up for large-scale production, providing cost-effective and efficient manufacturing. In contrast, maintaining individual hybridoma cells lines can be resource-intensive and time-consuming. The ability to screen large antibody libraries and rapidly generate recombinant antibodies accelerated the discovery of novel antibodies against various targets. Finally, the use of standardized systems for antibody production ensures greater batch-to-batch consistency and reproducibility, which is crucial for maintaining the safety and efficacy of therapeutic antibodies.
A3: Complement pathway testing
The complement system consists of more than 30 proteins that participates in the innate immune response. Complement testing is used to diagnose and monitor certain immune-related conditions. These tests evaluate the activity and levels of various components within the complement system.
A3-1 Total hemolytic complement (CH50) assay
The CH50 assay aka the total hemolytic complement assay is assesses the overall activity and function of the complement system, particularly the classical complement pathway. As discussed in Unit 2, the classical complement pathway is initiated primarily by antigen-immunoglobulin complexes.
The CH50 assay measures the lysis of sheep red blood cells (SRBCs) coated with anti-sheep antibodies in the presence of antibodies. If classical complement pathways components such as C1, C2, C3 and C4 are all available in a patient sample, the membrane attack complex (MAC) will be assembled leading to SRBC lysis. However, if there are deficiencies or dysregulation within the complement system (C1-C9) or if there is consumption of complement due to immune (or autoimmune) complexes the CH50 assay results will be abnormal. The complement deficiencies can be hereditary or acquired.
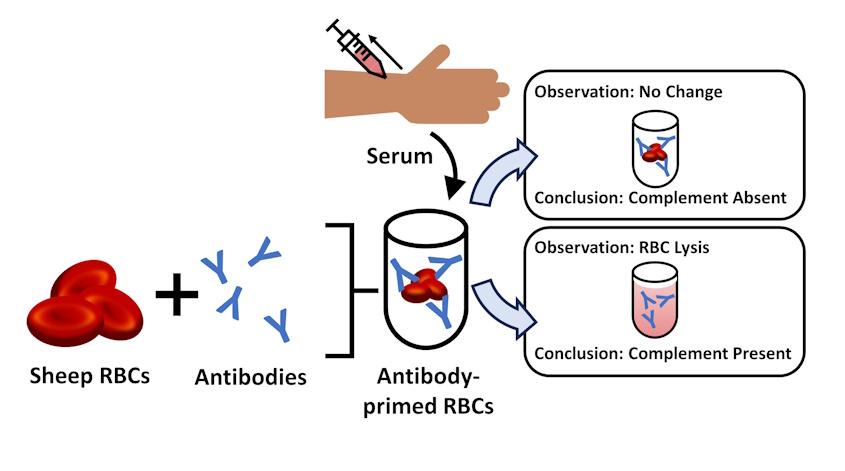
Figure A3-1-1 CH50 assay. Sheep red blood cells are sensitized with antibodies to serve as targets for complement mediated lysis. Patient samples are collected using standard venipuncture and centrifuged to separate plasma. Sensitized SRBCs and patient plasma is incubated under specified conditions to induce hemolysis. Samples are centrifuged, and the extent of RBC lysis is assessed via measuring the release of hemoglobin into the supernatant. The CH50 value is calculated based on the dilution of patient’s plasma at which 50% of sensitized RBCs are lysed.
A3-2 Alternative complement hemolytic (AH50 ) assay
The AH50 assay is used to evaluate the function and activity of the alternative complement pathway. As discussed in Unit 2, the alternative pathway is spontaneously activated.
The AH50 assay measures the lysis of rabbit red blood cells in the presence of complement proteins in a patient serum sample. Rabbit RBCs contain low levels of sialic acid, which makes them highly susceptible to alternative pathway mediated lysis. When alternative complement pathways components are available in a patient sample, MAC will be assembled resulting in RBC lysis. Abnormal AH50 results indicate a potential alternative pathway component defect.
Interpretation of results
The alternative pathway shares C3 and C5-C9 components with the classical complement pathway. However, it also has unique complement components including Factors D, B and properidin. As such CH50 and AH50 assays are often run in conjunction to identify specific complement pathway abnormalities.
- Absent alternative pathway activity (AH50=0) in the presence of a normal CH50 (CH50=100) suggests an alternative pathway component deficiency.
- Normal AH50 (AH50=100) with absent CH50 (CH50=0) suggest deficiencies in early classic pathway involving C1, C2 or C4.
- Absent AH50 and CH50 (CH50=0 and AH50=0) suggest a late component deficiency involving C3, C5, C6, C7, C8 and C9.
- Normal CH50 and AH50 CH50=100 and AH50=100) in the presence of recurrent infections and continue suspicion of complement deficiency may require testing of the MBL pathway function.
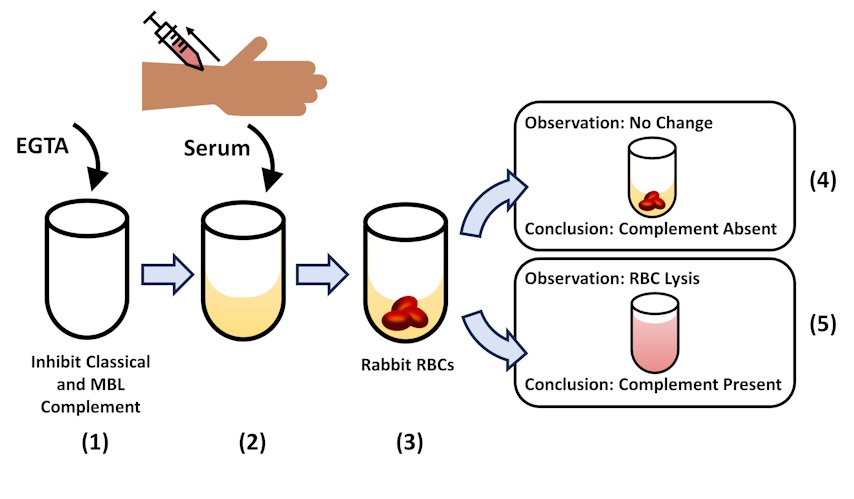
Figure A3-2-1 AH50 assay. (1) Collection tubes are prepared with EGTA, which removes calcium required for the activation of the classical and MBL pathways. (2) Patient samples are collected using standard venipuncture and centrifuged to separate plasma. (3) Rabbit red blood cells are used in this assay due to their low sialic acid content and susceptibility to lysis. Rabbit RBCs and patient plasma is incubated together to induce hemolysis. (4-5) Samples are centrifuged, and the extent of RBC lysis is assessed. The AH50 value is calculated based on the dilution of patient’s plasma at which 50% of sensitized RBCs are lysed.
A4: Complement fixation (CF) test
The complement fixation test uses components of the complement system as reagents to detect the presence of specific antibodies in patient samples. While this test was widely used in the past to diagnose infections, today, ELISA assays and DNA-based methods have replaced complement fixation tests.
CF tests uses sheep RBCs, anti-sheep RBC antibody, and guinea pig serum as a source of complement proteins. When these three reagents are mixed under normal circumstances, complement proteins bind to antibody coated RBCs resulting in MAC formation and hemolysis.
When performing a CF test, patient samples are first treated with heat to inactivate human complement proteins, as their presence will interfere with the results. Next, the known antigen is added to the serum sample. If the patient sample contains antibodies specific to the antigen antigen-antibody complexes will be made. Following this incubation, guinea pig complement proteins are added to the mixture, which will bind the antigen-antibody complexes. These complement proteins are now fixed on the antigen-antibody complexes. When sensitized sheep RBCs are added to this mixture (containing antigen-antibody-complement proteins) they will not be lysed since the complement proteins are already bound. In this assay, a lack hemolysis indicated a positive CF test. The patient sample contains the specific antibodies examined in the CF test.
| (1)
(2)
(3)
(4)
(5) |
 |
Figure A4-1 The complement fixation assay. (1) Patient samples are collected using standard venipuncture and heat treated to remove complement proteins. (2) The samples are then incubated with the test antigen. If the patient sample contains the antibody (left) they will form antigen-antibody complexes. (3) Next, complement proteins from guinea pig serum are added to these samples. If antigen-antibody complexes are present the complement proteins will be bound to these complexes becoming fixed (unavailable for further interactions). (4) Final step of the assay involves adding sensitized or antibody bound sheep red blood cells (SRBC) to the reaction. (5) If complement proteins are already fixed, SRBCs will not be lysed. This results in a positive CF test (left). If complement proteins are available, it will lead to MAC formation on SRBCs, leading to lysis. In this case, the patient sample did not contain the antibody being examined.
Image Source: Ranjan, et al. (2016). J. adv. parasitol.. 2. 80-99. 10.14737/journal.jap/2015/2.4.80.99. [Shared under creative commons licence]
A5: Enzyme linked immunosorbent assays (ELISA)
ELISAs use catalytic properties of enzymes to detect and quantify immune reactions. They can be used to detect and measure levels of antibodies in blood, to estimate the level of tumor markers, to track disease outbreaks, to screen donor blood and plasma and to detect past exposures to infectious agents.
ELISA assays are performed in 96 or 384 well plates and depend on two basic elements: (1) capture or coating of antigen of interest and (2) detection of antibodies or antigen in patient samples. Antigen capture on the microwell plate can be either direct or indirect. In direct capture, the antigen is adsorbed directly on the microwell plate. Indirect capture involves a capture antibody, which is first immobilized on the well plate. The target antigen is captured through its interaction with the capture antibody. Similarly, analyte detection can also be performed directly or indirectly. In direct detection, the analyte is detected with a labelled primary antibody. Indirect detection makes use of two antibodies, where the primary antibody binds to the analyte and a labelled secondary antibody interacts with the primary antibody.
Three main types of ELISAs are relevant to diagnostic testing: direct ELISAs, indirect ELISAs and sandwich ELISAs.
Direct ELISA assays use direct capture and direct detection. Patient samples contains the target antigen, which is detected using an enzyme-labelled primary antibody. Next detection in carried out by adding a substrate that generates colour, fluorescence or chemiluminescence upon cleavage by the enzyme.
Indirect ELISA assays use direct capture and indirect detection. Initial steps are identical to a direct ELISA assay with the exception of requiring two antibodies. Antigen of interest are adsorbed to the well plate. A patient sample containing the primary antibody is incubated with the antigen. Following the incubation and washing, an enzyme-labelled secondary antibody that recognizes the primary antibody is added to the sample. Due to the signal amplification that happens at the final step, where one primary antibody can be bound by several labelled secondary antibodies indirect ELISAs offer higher sensitivity than direct ELISAs.
Sandwich ELISAs (generally known as antigen capture assays) are the most widely used ELISA format. They involve indirect capture and indirect detection. The assay is known as a “sandwich” ELISA because the analyte is bound between two primary antibodies, each detecting a different epitope of the antigen. Steps involved in a sandwich ELISA is identical to that of an indirect ELISA with the exception of indirect antigen capture with a capture antibody. Sandwich ELISAs offer high sensitivity and specificity as it uses three specific antibodies for analyte detection.
 In direct ELISA antigens of interest are detected using a labelled primary antibody. (2) Indirect ELISA involves two antibodies. The primary antibody that binds the antigen of interest, and the secondary antibody that binds the primary antibody. Since multiple secondary antibodies can bind a single primary antibody, the detection signal is amplified at this stage making indirect ELISAs more sensitive. (3) Sandwich ELISAS use indirect capture and indirect detection, making use of three antibodies. The capture antibody binds the antigen of interest. The primary antibody is found in patient samples. If they are present, the labelled-secondary antibody will bind to the antigen-antibody complexes resulting in a positive test. (4) Competitive ELISA requires the test antigen to displace a competing antibody-bound antigen. This method provides higher consistency in quantification.")
A5-1 Common ELISA assays. (1) In direct ELISA antigens of interest are detected using a labelled primary antibody. (2) Indirect ELISA involves two antibodies. The primary antibody that binds the antigen of interest, and the secondary antibody that binds the primary antibody. Since multiple secondary antibodies can bind a single primary antibody, the detection signal is amplified at this stage making indirect ELISAs more sensitive. (3) Sandwich ELISAS use indirect capture and indirect detection, making use of three antibodies. The capture antibody binds the antigen of interest. The primary antibody is found in patient samples. If they are present, the labelled-secondary antibody will bind to the antigen-antibody complexes resulting in a positive test. (4) Competitive ELISA requires the test antigen to displace a competing antibody-bound antigen. This method provides higher consistency in quantification.
Image Source: By Allan.richard5093, CC BY 4.0, via Wikimedia Commons
A6: Enzyme linked Immunosorbent spot assay (ELISpot)
The ELISpot assay is a widely used immunological technique that allows the detection and quantification of individual cytokine-secreting T cells or antibody secreting B cells. ELISpot is based on the same principles as ELISA assays but combines it with the analysis of individual cells. ELISpot measures the secretion of cytokines, such as interferon-gamma, interleukins (ILs) and, and other immune-related molecules, by capturing and visualizing the proteins produced by individual cells.
The interferon-gamma release assay (IGRA) is an example of an ELISpot assay used to test for latent tuberculosis infections. Interferon-gamma (IFN-G) is the primary cytokine release in response to infections by the microbe Mycobacterium tuberculosis. Since people with latent tuberculosis do not display symptoms of the disease, the only way to identify past exposure is through a tuberculin skin test or a blood test. IGRA is more specific for identifying tuberculosis infections particularly in people who were vaccinated as children as it uses antigens that are not found in the tuberculosis strains used in the vaccine.
In the ELISpot assay, T cells from the patient sample are first stimulated with the tuberculosis antigen. The cells are then allowed to settle on a well plate coated with antibodies that recognize IFN-G. If the activated T cells release IFN-G, the cytokine will be captured by the capture antibody. Antibody bound IFN-G is detected using a labelled-secondary antibody, which reveals a circle (spot) surrounding the position of each activated T cell. These circles give ELISpot assay its name.
In addition, ELISpot assays are also useful for assessing functionality of T and B cells, evaluating vaccine efficacy, and monitoring immune reactivity in diseases such as cancer and autoimmune disorders.
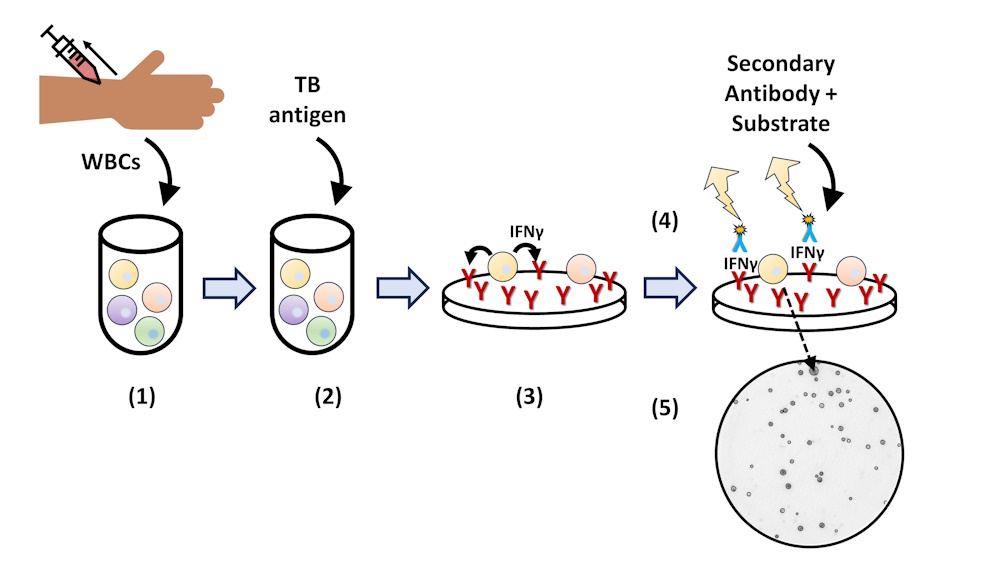
Figure A6-1 The T.SPOT TB assay. (1) White blood cells are isolated from a whole blood sample. (2) Cells are stimulated with TB antigen and transferred to cells pre-coated with capture antibodies for IFN-G. (3) IFN-G is bound to capture antibodies. (4) IFN-G is detected using a labelled-secondary antibody and detection reagent that reacts with enzyme labelled secondary antibody is added. (5) Reaction generates spots in the areas where IFN-G was released. Spots are enumerated for a T cell count.
A7: Immunoblotting (Western blotting)
Immunoblotting or Western blotting is a technique employed to detect and analyze specific proteins within a biological sample using antibodies. Western blots can also be used to evaluate the size of a protein and to quantify the amount of protein.
The first step of Western blotting involves mixing the sample with a detergent called sodium dodecyl sulfate (SDS) to denature (unfold) the proteins. Proteins are then separated by size using gel electrophoresis. Following separation, proteins are transferred to a blotting membrane ensuring the proteins maintain their relative position from the gel onto the membrane. The membrane is the ‘blocked’ to prevent non-specific binding and subsequently incubated with a primary antibody that specifically recognizes the protein/antigen of interest. Unbound antibodies are washed off and the membrane is incubated with a labelled secondary antibody, which allows the detection and/or visualization of the protein. Addition of the detection substrate generates a signal that may be quantified.
Western blots are still used in Lyme disease testing, HIV confirmation tests and hepatitis C confirmation tests by diagnostics labs.
A8: Immune cell isolation
This section highlights techniques that selectively separate specific subsets of immune cells by using antibodies. They play a critical role in research, diagnostics, and therapeutics.
A8-1 Flow cytometry and FACS analysis
Flow cytometry allows individuals cells to be counted and analyzed based on various physical properties such as size, complexity, and specific labelling. The basic principle of flow cytometry involves the passage of cells through a flow cell, where cells suspended in fluid are passed through a laser beam. As each cell pass through the laser, they scatter the light. The scattered light is collected by a series of detectors, which converts these signals into electrical impulses to provide information about the characteristics of a cell.
Two physical properties, the size and internal complexity (granularity and topology), determines the extent of light scattering. Two measures of scattered light are assessed, forward-scattered light (FSC) and side-scattered light (SSC). FSC is proportional to cell size. FSC is a measure of diffracted light (light bent as the cell passes through the laser) and therefore is used to differentiate cells based on size. SSC is proportional to internal complexity or granularity. SSC measurements are collected by a lens placed 90 degrees to the laser beam, which measures refracted and reflected light.
A common method used to display light scatter data is a dot plot. FSC values are plotted on the x-axis and SSC is plotted on the y-axis, where each dot represents a cell. Based on FSC and SSC values different immune cell populations can be identified. For example, granulocytes (eg: neutrophils and basophils) will have larger FSC and SSC values than lymphocytes (T cells and B cells), which are smaller and less complex.
Fluorescence-activated cell sorting or FACS is a specialized application that combines flow cytometry with the ability to physically separate or sort cells based on fluorescent properties. In FACS, the flow cytometer is equipped with a cell sorter. The cell sorter can identify cells based on fluorescence and sort them into different collection tubes or plates.
Cells to be sorted by FACS are fluorescently labelled, using either fluorescent antibodies or fluorescent dyes. Fluorescence induces the device to put a charge on the fluid droplet containing the fluorescent cell. Since the charge is matched to a specific wavelength of fluorescent light, differentially labelled cells can be given different charges. Sorting is accomplished using an electrostatic deflector that moves the charged droplet containing the cell into the assigned collection vessel.
A8-2 Immunomagnetic cell separation
Immunomagnetic cell separation is a technique for isolating cells using magnetic beads. The beads are coated with antibodies or ligands that recognize and bind specific surface markers on target cells allowing selective capture and separation of cells. Immunomagnetic cell separation is particularly useful for isolating specific immune cells for therapeutic applications.
To select for cells of interest (aka positive selection), the heterogeneous cell suspension is first incubated with coated magnetic beads, allowing the beads to bind the desired antigen expressing target cells. Next, a magnetic field is applied causing the magnetically labelled cells to be immobilized near the magnetic source. Non-target cells are then be removed by washing, while target cells remain bound to the beads. Final step involves the elution or release of the cells from the beads so they can used in downstream applications.
Alternatively, immunomagnetic cell separation is also useful for removing an unwanted cell type from a population (negative selection). Here the magnetic beads are coated with an antibody that will bind and contain the cells to be removed. Following incubation, these cells will remain bound to the magnetic source, resulting in their removal from the population.
Magnetic cell isolation is a faster and a much simple process compared to FACS. It also does not require specialized equipment. However, FACS offers many more capabilities as it is possible to sort multiple cell types simultaneously, isolate cells based on internal markers, isolate cells based on protein levels and sort complex cell types with multiple markers to obtain samples with higher purity with FACS.
A9: Immunofluorescence
Antibodies are specific to their corresponding antigen. This specificity makes them an invaluable resource for probing and identifying specific molecules in cells, tissues, and biological fluids. In addition, antibodies can be conjugated or attached to other molecules such as fluorescent dyes. Antibodies labelled with fluorescent molecules are used in immunofluorescence assays (IFA) to detect and visualize specific antigens such as viral proteins.
Two main IFAs are used in diagnostic testing, direct immunofluorescence, and indirect immunofluorescence. In direct immunofluorescence assays, a fluorescently labelled primary antibody is used to identify analytes in patient samples. Indirect immunofluorescence assays involve two steps for detecting analytes. The unlabeled primary antibody binds specifically to the target molecule and the secondary antibody with the fluorescent molecule binds to the primary antibody.
Diagnostic tests that use both IFA techniques are available for syphilis testing caused by the spirochete Treponema pallidum. The direct fluorescent antibody (DFA) assay is used as a screening test for syphilis. The test is performed on smears of exudate (fluid) from lesions and chancres. Slides are incubated with a fluorescently labelled primary antibody specific to pathogenic treponemes. A positive result constitutes a visible fluorescence signal when slides are examined using a microscope.
The fluorescent treponemal antibody absorption (FTA-ABS) test is an indirect fluorescent assay used to confirm a syphilis diagnosis. In this test, the patient serum is absorbed (ABS component of the test) by mixing with a sorbent that will remove non-specific antibodies. The absorbed serum is then tested on a microscope slide containing antigens from the Treponema strain specific to syphilis. If the patient serum contains syphilis specific antibodies, they will bind to the antigen. Washed slides are then incubated with fluorescently labelled anti-human antibodies. As with the DFA test, a positive result constitutes a visible fluorescence signal when slides are examined using a microscope.
The ANA (anti-nuclear antibody) test and the CLIFT (Crithidia luciliae immunofluorescent) test used to detect autoantibodies associated with autoimmune diseases such as rheumatoid arthritis and systemic lupus erythematosus are two additional examples of diagnostic tests employing indirect immunofluorescence.
A10: Immunohistochemistry (IHC)
Immunohistochemistry is a technique that exploits the specific binding between an antigen and an antibody. It combines anatomical, immunological, and biological techniques to visualize the distribution and location of specific proteins within the context of cells and tissue in their histological context (in situ). IHC is used to identify and classify cancer cells, for characterizing tumours that guide treatment decisions, to detect infectious agents in tissue, and for diagnosing autoimmune diseases.
Antibodies used in IHC are chemically coupled to enzymes that convert a colourless substance to a coloured reaction product in situ. Tissue samples are incubated with the antibody followed by the addition of the substrate. In the presence of an antigen-antibody complex, the coloured product is deposited at the sites of interaction and can be observed using a microscope.
A11: Immunoprecipitation
Immunoprecipitation (IP) is a technique used to isolate and purify proteins of interests from a mixture based on their interactions with antibodies. Antigen-specific antibodies employed in IPs to bind and precipitate the target protein of interest.
In immunoprecipitation, samples such as serum, cell extract, or tissue extract are incubated with specific antibodies. The antibody-antigen complex is then precipitated from the rest of the complex with the aid of agarose beads bound to protein A or protein G. Protein A and G are bacterial proteins that bind to antibodies with high affinity. After the precipitation, the samples are washed to remove any non-specifically bound proteins. The protein of interest is then eluted or released from the immunocomplex so it can be further analyzed using techniques such as Western blotting.
A12: Precipitin Assays
The precipitin test was the first assay developed for quantifying antigen and antibody titres. It relies on the interaction between antigens and antibodies and the resulting antigen-antibody complex formation. The immunocomplexes form a lattice structure that becomes visible as either a ring or a line. “Precipitin” in this assay refers to the precipitate that forms when the antibody reacts with the corresponding antigen.
The outcome of the precipitin reaction depends on the amount of antigen added:
- Prozone effect
The prozone effect occurs when there is an excess of antibodies relative to antigen. Each antigen molecule is bound by antibodies. However, the presence of excess antibodies prevents crosslinking of antigen molecules, the resulting complexes are generally small in size and do not form precipitates. - Zone of equivalence
This zone represents the optimal conditions for forming precipitin complexes. In the zone of equivalence, the maximum number of antigen-antibody complex are formed resulting in a robust, detectable assay signal. - Postzone effect
Postzone refers to the region in which the concentration of antigen exceeds the optimal range for immunocomplex formation. In this zone, the excess antigen can interfere with the formation of visible precipitates.
When performing precipitin assays, the prozone effect can be overcome by diluting samples to reduce the concentration of antibodies. This enables the formation of properly sized complexes for accurate detection. Various antigen concentrations may be tested to overcome the limitation of postzone effects.
A12-1 Precipitin ring test
The precipitin ring test is a liquid based assay used to detect the presence of antigen-antibody complexes. To perform the test, a fixed amount of patient serum is placed in the bottom of a clear test tube. Next varying amount of soluble antigen is gently layered above the antibody solution. If the patient sample contains the antibody, immunocomplexes will form, and a white ring will become visible at the interface of the two liquid layers. Absence of a visible ring is indicative of the absence of antigen-antibody complexes.
The precipitin ring test is quick and easy to perform, cost-effective and can be adapted to detect both antibodies and antigen in biological samples. However, due to limited sensitivity and the semi-quantitative nature of the assay, other immunological assays such as ELISAs have replaced the precipitin ring test for the most part.
A12-2 Radial immunodiffusion assay
The radial immunodiffusion assay (RID) is a semi-solid based method for quantifying antigen-antibody interactions. In this assay, a predetermined dilution of patient serum is mixed with agar or agarose to generate semi-solid media on a plate. The solidified gel is cut to create small wells, which are then filled with various concentrations of antigen. As the antigen diffuses into the gel, it interacts with the antibody present in the agar to form a distinct precipitin ring around the well. The diameter of the ring is directly proportional to the concentration of antigen in the solution.
To estimate the concentration of an unknown sample, the diameter of the ring produced by the sample is measured and plotted on a standard curve generated using known concentrations of antigen. While RIA is a well-established method for quantifying immune products, more sensitive and automated immunoassays such as ELISAs have largely replaced RIA.
A13: Tests for General Immune Status
A13-1 Complete Blood Count with Differential (CBC diff)
The complete blood count (CBC) test is a common blood test that provides information about the overall health status of a patient. It measures various components in a blood sample including red blood cells (RBC), white blood cells (WBC) and platelets. The CBC test with differential provides additional information regarding WBC as it counts the total numbers of five different WBC types: neutrophils, basophils, eosinophils, monocytes. and lymphocytes. In this test, a blood sample from the patient is analyzed using an automated hematology analyzer, which can identify and bin cells according to size, shape, and specific markers.
The CBC with differential provides additional insight into immune function of a patient as abnormal WBC differential counts may be indicative of infections, autoimmune diseases, allergic reactions, or leukemia. For example, an increase in the neutrophil count may be due to an active infection, inflammation, or acute stress, while an increase in the lymphocyte count may be indicative of a chronic infection or lymphocytic leukemia.
A13-2 C-reactive Protein Test (CRP)
Various conditions such as infection, tissue injury, autoimmune diseases and certain cancers can increase inflammation in the body. The C-reactive protein (CRP) is an acute phase protein released by the liver in response to inflammation. Acute phase proteins (APPs) are a group of approximately 30 unrelated proteins that are regulated in response to inflammation or injury. They are produced and released by the liver in response to tissue damage or insult, and are mediators of the inflammatory response. Prothrombin, plasminogen, fibrinogen, alpha-1 antitrypsin, haptoglobin and complement proteins are some other examples of APPs.
CRP is one of the most well-known and commonly measured APPs. Its levels rise rapidly in response to inflammation and can be used as a marker of inflammation and infection. Elevated CRP levels are also linked to an increased risk of heart disease. Therefore, monitoring CRP levels can help identify individuals who are at higher risk of heart disease.
Immunoturbidimetry is the most common method used to measure CRP. This test relies on CRP specific antibodies and the change in turbidity (cloudiness) associated with antigen-antibody complex formation. Serum samples are mixed anti-CRP antibodies. CRP will bind the antibody leading to the formation of a cloudy product. The turbidity of the sample will be higher if greater than normal ranges of CRP is being present in the sample. ELISA assays for measuring CRP are also available.
CRP is a non-specific marker of inflammation. While elevated CRP levels are indicative of the presence of inflammation, the cause or location of the inflammation cannot be identified with this test.
A13-3 Erythrocyte Sedimentation Rate (ESR)
The ESR test also known as sedimentation rate (sed rate) test measures the rate at which RBCs settle in a vertical tube over a specific period of time. The ESR test is based on the principle that when blood is drawn into a narrow tube and allowed to stand undisturbed, the RBCs will gradually settle at the bottom due to gravity. The rate at which they sediment is influenced by various factors, including the presence of APPs. APPs neutralize the negative charge present on the surface of RBCs, increasing their “stickiness.” When APP levels are elevated, the presence of sticky RBCs result in a corresponding increase in ESR.
To perform an ESR test, whole blood samples are placed in a tall, thin tube (Westergren tube) and allowed to stand upright for a specific duration, typically one hour. During this time the RBCs will sediment due to gravity. After the designated time, the height of the serum present at the top of the tube is measured. Higher ESR rates suggest more significant inflammation in the body.
Similar to the CRP test, the ESR test is a non-specific indicator of inflammation in the body. It is not specific to any disease or condition and can only provide an indication of the presence and severity of inflammation. Due to its low cost and reproducibility, the ESR is often used as a “sickness indicator” in conjunction with other diagnostic tests for detecting infections, autoimmune disorders, inflammatory diseases and certain cancers.

{kind=link}
{kind=link}
{kind=link}
{kind=link}