Chapter 4. Carbohydrates
Health Consequences and Benefits of High-Carbohydrate Diets
Can we blame the obesity epidemic on the higher consumption of added/ free sugars and refined grains? This is a hotly debated topic by both the scientific community and the general public. In this section, we will give a brief overview of the scientific evidence.
Free and Added Sugars
There is considerable evidence suggesting an association between sugar consumption and many diseases/health outcomes including cardiovascular disease, fatty liver disease, obesity, visceral adiposity, high blood lipid levels, insulin resistance, type 2 diabetes, metabolic syndrome, and cavities (dental caries). [1]
When considering the link between sugar and health, the terms “added sugars” and “free sugars” are often used. Sometimes the definitions for both can vary, however, in this textbook, we will use the following definitions:
- Free sugars include “all monosaccharides and disaccharides added to foods by the manufacturer, cook or consumer, and sugars naturally present in honey, syrups, fruit juices and fruit juice concentrates.” [2]
- Added sugars are defined as refined sugars and syrups that are added to foods during processing or preparation and do not include those naturally occurring sugars or fruit juice.[3]
The main difference between added and free sugars is that added sugars exclude naturally occurring sugars in fruit juices and fruit juice concentrates.
A study in Canada estimated that desserts and sweets, breakfast cereals, baked products, beverages, and snacks are food groups with high added and free sugar content. [4] Processed foods, even microwaveable dinners, also contain added sugars. Added sugars do not include sugars that occur naturally in whole foods (such as an apple), but do include natural sugars such as brown sugar, corn syrup, dextrose, fructose, fruit juice concentrates, maple syrup, sucrose, and raw sugar that are then added to create other foods (such as cookies).
In 2015, it was estimated that Canadians consumed 51.7 g of added sugar and 67.1 grams of free sugars per day, representing 11.1% and 13.3% of their total energy intake, respectively. Desserts, sweets, and beverages contributed to most of the added, free and total sugar intake, with deserts and sweets contributing substantially more than beverages.[5]
The Added Sugar Conudrum in Canada
The World Health Organization recommends that free sugars should make up less than 10% of total energy intake, but ideally less than 5%. [6]
The challenge that Canadians face is that the added or free sugar content of foods and beverages is not contained in the nutritional facts table. In 2022, this changed in the United States, which means that nutritional facts tables now list added sugars, and hopefully this will happen in Canada too. Until this happens, it is best to minimize your intake of added or free sugars in foods (e.g., soft drinks, sports drinks, cakes, cookies, pies).
Obesity, Diabetes, and Heart Disease and Their Hypothesized Link to Excessive Sugar Consumption
As previously highlighted, there is considerable evidence suggesting an association between sugar consumption and cardiovascular disease, obesity, visceral adiposity, high blood lipid levels, insulin resistance, type 2 diabetes and metabolic syndrome.[7] The obesity epidemic has reached both young adults and children, and will markedly increase the prevalence of serious health consequences in adulthood. Health consequences linked to being overweight or having obesity include Type 2 diabetes, cardiovascular disease, arthritis, depression, and some cancers. Consumption of sugary foods likely contributes to the proportion of people who are overweight or have obesity in this country, but so does the consumption of high-calorie foods that contain too much saturated fat, and the sedentary lifestyles of many Canadians.
A major source of added sugars in the Canadian diet is soft drinks.[8] Consistent scientific evidence supports the idea that increased consumption of sugary soft drinks can cause increased weight gain and disease risk. An analysis of over thirty studies in the American Journal of Clinical Nutrition concluded that there is much evidence to indicate that higher consumption of sugar-sweetened beverages is linked with weight gain and obesity.[9] A study at the Harvard School of Public Health linked the consumption of sugary soft drinks to an increased risk for heart disease.[10]
The results of many of these studies have led some public health organizations like the World Health Organization to recommend the consumption of free sugars to less than 10% of total energy intake, but ideally to less than 5%. [11] Similarly, the Canadian Heart and Stroke Foundation recommends that you consume no more than 10% of total calories per day from added sugars, and ideally less than 5%. However, the added sugar conundrum in Canada (see orange box above) makes it hard for consumers to know how much added sugar they are consuming. Despite this, you could consider the following recommendations:
- Know the number of total calories you should consume each day.
- Consume an overall healthy diet and get the most nutrients for the calories using foods high in added sugars as discretionary calories (those left over after getting all recommended nutrients subtracted from the calories used).
- Lower your sugar intake, especially when the sugars in foods are not tied to positive nutrients such as in sugary drinks, candies, cakes, and cookies.
- Focus on calories in certain food categories such as beverages and confections, and encourage consumption of positive nutrients and foods such as cereals, and low-fat or fat-free dairy products.
Fructose
Before high-fructose corn syrup (HFCS) was marketed as the best food and beverage sweetener, sucrose (table sugar) was the number-one sweetener in North America. Recall that sucrose, or table sugar, is a disaccharide consisting of one glucose unit and one fructose unit. HFCS also contains the simple sugars, fructose and glucose, with fructose at a slightly higher concentration. In the production of HFCS, corn starch is broken down to glucose, and some of the glucose is then converted to fructose. Fructose is sweeter than glucose; hence many food manufacturers choose to sweeten foods with HFCS. HFCS is used as a sweetener for carbonated beverages, condiments, cereals, and a great variety of other processed foods.
Some scientists, public health personnel, and healthcare providers believe that fructose is the cause of the obesity epidemic and its associated health consequences. The majority of their evidence stems from the observation that since the early 1970s, the number of individuals who are overweight or have obesity in North America has dramatically increased and so has the consumption of foods containing HFCS. However, as discussed, so has the consumption of added sugars in general. Animal studies that fuel the fructose opponents show fructose is not used to produce energy in the body; instead, it is mostly converted to fat in the liver—potentially contributing to insulin resistance and the development of Type 2 diabetes. Additionally, fructose does not stimulate the release of certain appetite-suppressing hormones, like insulin, as glucose does. Thus, a diet high in fructose could potentially stimulate fat deposition and weight gain.
In human studies, excessive fructose intake has sometimes been associated with weight gain, but results are inconsistent. In 2012, a scientific review suggested that when fructose is substituted for other carbohydrates in the diet, but the diets contain the same number of calories, fructose does not seem to cause weight gain.[12] Moreover, other studies show that some fructose in the diet actually improves glucose metabolism, especially in people with Type 2 diabetes.[13] However, there is evidence that when taken in liquid forms, such as when consuming soft drinks or fruit juices, the consumption of fructose is associated with higher energy intake, increased body weight, and the onset of metabolic syndrome. [14]
So where does this leave us? Based on the currently available evidence, it’s likely safe to conclude that very high intakes of fructose could have metabolic consequences. But overall, there is no strong evidence that suggests moderate fructose consumption contributes to weight gain, type 2 diabetes and chronic disease, or that moderate intakes are harmful to health.
Do Low-Carbohydrate Diets Cause Weight Loss?
Since the early 1990s, marketers of low-carbohydrate diets have bombarded us with the idea that eating fewer carbohydrates promotes weight loss and that these diets are superior to others in their effects on weight loss and overall health. The most famous of these low-carbohydrate diets is the Atkins diet. Others that are more prominent now include the “Keto” diet and may include the “paleo” diet or the “Earth” diet.
These diets typically imply that long-term weight loss is achieved through a reduction in dietary carbohydrates and glycemic load. However, a number of diet intervention studies have found that low-glycemic-load diets do not cause significantly greater long-term weight loss compared with higher-glycemic-load diets.[15] Furthermore, a recent meta-analysis of 121 randomized controlled trials found no difference in weight loss at 6 months comparing low-fat, low-carbohydrate, or moderate-carbohydrate with usual diet controls.[16]
With these randomized controlled trials being the gold standard, how can we know if people were able to stick to the diet and if the deviation from the diet resulted in no differences? To overcome this, a series of inpatient feeding studies were conducted, where patients did not have access to off-site food. In these studies, if the exposure to high-glycemic load occurs, then proponents of the Atkins or Keto diets (which are based on the carbohydrate-insulin model of obesity) would suggest that this high glycemic load leads to excess insulin secretion, accumulation of body fat and increases in appetite, which would lead to higher energy intake when compared to low-glycemic load diets. However, a 2-week inpatient feeding study actually found the opposite; when patients were exposed to high-glycemic load diets, they consumed ∼700 kcal/d less and experienced body fat loss compared to the 2 weeks spent by the same participants on a very-low-glycemic-load diet.[17] These changes occurred despite the low glycemic-load diet resulting in lower insulin secretion.
Some may suggest that 2 weeks isn’t long enough and a serious pitfall in the research, however, another study found that 10 to 15 weeks of a high-carbohydrate diet significantly increased satiety when compared to a low-carbohydrate diet.[18] This change in satiety occurred even with significantly higher post-food insulin levels, which contradicts the carbohydrate-insulin model of obesity.
The challenge with some research studies assessing the impacts of low carbohydrate diets on weight loss is that dietary protein, which plays a large role in satiation, is not controlled. If these studies do not control for protein intake, then how can we know if protein is playing a role and how do we know if low or high-carbohydrates play a role in weight loss? Feeding studies, that ensure the number of total calories and protein are the same, have found that high-carbohydrate diets are associated either with a small or non-significant change in body fat.[19]
Despite the claims these diets make, there is little scientific evidence to support that low-carbohydrate diets are significantly better than other diets in promoting long-term weight loss.
Some studies provide evidence that in comparison to other diets, low-carbohydrate diets improve insulin levels and other risk factors for Type 2 diabetes and cardiovascular disease. The overall scientific consensus is that consuming fewer calories in a balanced diet will promote health and stimulate weight loss, with significantly better results achieved when combined with regular exercise.
Health Benefits of Whole Grains in the Diet
While excessive consumption of simple carbohydrates is potentially bad for your health, consuming more complex carbohydrates is extremely beneficial to health. There is a wealth of scientific evidence supporting that replacing refined grains with whole grains decreases the risk of obesity, Type 2 diabetes, and cardiovascular disease. Whole grains are great dietary sources of fibre, vitamins, minerals, healthy fats, and a vast amount of beneficial plant chemicals, all of which contribute to the effects of whole grains on health. Eating a high-fibre meal compared to a low-fibre meal (see Figure 4.14 “Fiber’s role in carbohydrate digestion and absorption”) can significantly slow down the absorption process and can therefore affect blood glucose levels.
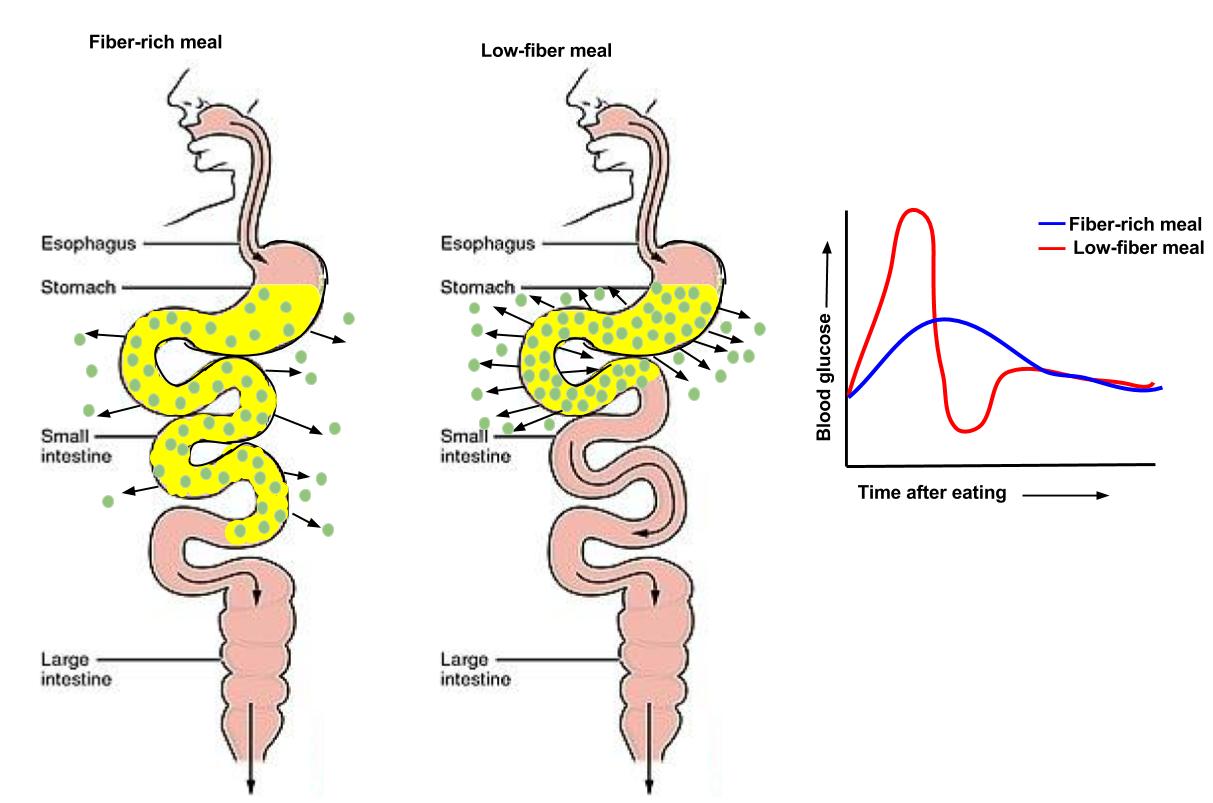
Figure 4.14 compares the effects of high-fibre and low-fibre diets on carbohydrate digestion and absorption. High-fibre diets promote efficient digestion, regulate blood sugar levels, and enhance nutrient absorption, while low-fibre diets may lead to slower digestion and potential blood sugar imbalances.
Fibre can also play a role in reducing the risk of heart disease, through improvement in blood lipids. When someone consumes a high-fibre diet, the fibre binds to bile (which contains cholesterol), and they are excreted, so less cholesterol is reabsorbed and blood levels are reduced. In contrast, when someone consumes a low-fibre diet, less fibre can be bound to bile, so less cholesterol is excreted, resulting in more being reabsorbed and elevated blood levels of cholesterol.
Diets high in whole grains have repeatedly been shown to decrease weight. A large group of studies all support that consuming more than two servings of whole grains per day reduces one’s chances of getting Type 2 diabetes by 21 percent.[20] A study found that women who consumed two to three servings of whole grain products daily were 30 percent less likely to have a heart attack.[21]
Regarding whole grains:
- “Dietary fibre from whole grains, as part of an overall healthy diet, helps reduce blood cholesterol levels and may lower risk of heart disease.”
- “Fiber-containing foods, such as whole grains, help provide a feeling of fullness with fewer calories and may help with weight management.”
- Liu S, Munasinghe LL, Ohinmaa A, Veugelers PJ. Added, free and total sugar content and consumption of foods and beverages in Canada. Heal reports. 2020 Oct 21;31(10):14–24. ↵
- World Health Organization. Sugars intake for adults and children. Geneva; 2015 ↵
- Louie JCY, Moshtaghian H, Boylan S, et al. A systematic methodology to estimate added sugar content of foods. European Journal of Clinical Nutrition 2015; 69(2): 154-61. ↵
- Liu S, Munasinghe LL, Ohinmaa A, Veugelers PJ. Added, free and total sugar content and consumption of foods and beverages in Canada. Heal reports. 2020 Oct 21;31(10):14–24. ↵
- Liu S, Munasinghe LL, Ohinmaa A, Veugelers PJ. Added, free and total sugar content and consumption of foods and beverages in Canada. Heal reports. 2020 Oct 21;31(10):14–24. ↵
- World Health Organization. Sugars intake for adults and children. Geneva; 2015 ↵
- Liu S, Munasinghe LL, Ohinmaa A, Veugelers PJ. Added, free and total sugar content and consumption of foods and beverages in Canada. Heal reports. 2020 Oct 21;31(10):14–24. ↵
- Liu S, Munasinghe LL, Ohinmaa A, Veugelers PJ. Added, free and total sugar content and consumption of foods and beverages in Canada. Heal reports. 2020 Oct 21;31(10):14–24. ↵
- Malik VS, Schulze MB, Hu FB. Intake of Sugar-Sweetened Beverages and Weight Gain: A Systematic Review. Am J Clin Nutr. 2006; 84(2), 274–88. http://www.ajcn.org/content/84/2/274.long. Accessed September 22, 2017. ↵
- Public Health Takes Aim at Sugar and Salt. Harvard School of Public Health. https://www.hsph.harvard.edu/news/magazine/sugar-and-salt/. Published 2009. Accessed September 30, 2017. ↵
- World Health Organization. Sugars intake for adults and children. Geneva; 2015 ↵
- Sievenpiper JL, de Souza RJ, Mirrahimi A, Yu ME, Carleton AJ, Beyene J, et al. Effect of Fructose on Body Weight in Controlled Feeding Trials. Ann Intern Med. 2012 Feb 21;156(4):291. ↵
- Elliott SS, Keim NL, et al. Fructose, Weight Gain, and the Insulin Resistance Syndrome. Am J Clin Nutr. 2002; 76(5),911–22. http://www.ajcn.org/content/76/5/911.full. Accessed September 27, 2017. ↵
- Tappy L, Lê K-A. Metabolic Effects of Fructose and the Worldwide Increase in Obesity. Physiol Rev. 2010 Jan;90(1):23–46. ↵
- Hall KD, Farooqi IS, Friedman JM, Klein S, Loos RJ, Mangelsdorf DJ, et al. The energy balance model of obesity: beyond calories in, calories out. Am J Clin Nutr. 2022 May;115(5):1243–54. ↵
- Ge L, Sadeghirad B, Ball GDC, da Costa BR, Hitchcock CL, Svendrovski A, et al. Comparison of dietary macronutrient patterns of 14 popular named dietary programmes for weight and cardiovascular risk factor reduction in adults: systematic review and network meta-analysis of randomised trials. BMJ. 2020 Apr 1;m696. ↵
- Hall KD, Guo J, Courville AB, Boring J, Brychta R, Chen KY, et al. Effect of a plant-based, low-fat diet versus an animal-based, ketogenic diet on ad libitum energy intake. Nat Med. 2021 Feb 21;27(2):344–53. ↵
- Shimy KJ, Feldman HA, Klein GL, Bielak L, Ebbeling CB, Ludwig DS. Effects of Dietary Carbohydrate Content on Circulating Metabolic Fuel Availability in the Postprandial State. J Endocr Soc. 2020 Jul 1;4(7). ↵
- Hall KD, Farooqi IS, Friedman JM, Klein S, Loos RJ, Mangelsdorf DJ, et al. The energy balance model of obesity: beyond calories in, calories out. Am J Clin Nutr. 2022 May;115(5):1243–54. ↵
- de Munter JS, Hu FB, et al. Whole Grain, Bran, and Germ Intake and Risk of Type 2 Diabetes: A Prospective Cohort Study and Systematic Review. PLoS Medicine. 2007; 4(8), e261. https://www.ncbi.nlm.nih.gov/pubmed/17760498. Accessed September 27, 2017. ↵
- Liu S, Stampfer MJ, et al. Whole-Grain Consumption and Risk of Coronary Heart Disease: Results from the Nurses’ Health Study. Am J Clin Nutr. 1999; 70(3), 412–19. http://www.ajcn.org/content/70/3/412.long. Accessed September 27, 2017. ↵
