Hepatic Module
Liver Overview
Learning Objectives
By the end of this section, you will be able to:
- Explain the normal physiological roles and functions of liver
- Outline the transport of bile and state three main functions of bile
- Outline the normal transportation, processing and elimination of bilirubin
Liver Histology
The liver has three main components: hepatocytes, bile canaliculi, and hepatic sinusoids. A hepatocyte is the liver’s main cell type, accounting for around 80 percent of the liver’s volume. These cells play a role in a wide variety of secretory, metabolic, and endocrine functions. Plates of hepatocytes called hepatic laminae radiate outward from the portal vein in each hepatic lobule (Figure 1).
Between adjacent hepatocytes, grooves in the cell membranes provide room for each bile canaliculus (plural = canaliculi). These small ducts accumulate the bile produced by hepatocytes. From here, bile flows first into bile ductules and then into bile ducts. The bile ducts unite to form the larger right and left hepatic ducts, which themselves merge and exit the liver as the common hepatic duct. This duct then joins with the cystic duct from the gallbladder, forming the common bile duct through which bile flows into the small intestine.
A hepatic sinusoid is an open, porous blood space formed by fenestrated capillaries from nutrient-rich hepatic portal veins and oxygen-rich hepatic arteries. Hepatocytes are tightly packed around the fenestrated endothelium of these spaces, giving them easy access to the blood. From their central position, hepatocytes process the nutrients, toxins, and waste materials carried by the blood. Materials such as bilirubin are processed and excreted into the bile canaliculi. The hepatic sinusoids also contain star-shaped reticuloendothelial cells (Kupffer cells), phagocytes that remove dead red and white blood cells, bacteria, and other foreign material that enter the sinusoids.

Major Functions of the Liver
Storage of Iron and Vitamins
The liver stores iron as ferritin and has a high propensity for storing vitamins. The vitamin stored in greatest quantity in the liver is vitamin A, but large quantities of vitamin D and vitamin B12 are normally stored as well.
Regulation of Fuel Supply
The liver plays a major role in carbohydrate, protein, amino acid, and lipid metabolism.
The liver performs several roles in carbohydrate metabolism: The liver synthesizes and stores around 100 g of glycogen via glycogenesis, the formation of glycogen from glucose. When needed, the liver releases glucose into the blood by performing glycogenolysis. The liver is also responsible for gluconeogenesis, which is the synthesis of glucose from certain amino acids, lactate, or glycerol. Adipose and liver cells produce glycerol by breakdown of fat, which the liver uses for gluconeogenesis.
The liver is responsible for the mainstay of protein metabolism, synthesis as well as degradation. It is also responsible for a large part of amino acid synthesis. Deamination of amino acids is required before they can be used for energy or converted into carbohydrates or fats. Large amounts of ammonia are formed by the deaminatin process, which are then detoxified by the liver.
The liver plays several roles in lipid metabolism: it performs cholesterol synthesis, lipogenesis, and the production of triglycerides, and a bulk of the body’s lipoproteins are synthesized in the liver.
Detoxification
The liver breaks down bilirubin, a waste product produced when the spleen removes old or damaged red blood cells from the circulation, via glucuronidation, facilitating its excretion into bile. The liver is responsible for the breakdown and excretion of many waste products. It plays a key role in breaking down or modifying toxic substances (e.g., methylation) and most medicinal products in a process called drug metabolism. This sometimes results in toxication, when the metabolite is more toxic than its precursor. Preferably, the toxins are conjugated to avail excretion in bile or urine. The liver converts ammonia into urea as part of the urea cycle, and the urea is excreted in the urine.
Bile Production
The liver plays a key role in digestion, as it produces and excretes bile (a yellowish liquid) required for emulsifying fats and help the absorption of vitamin K from the diet. Bile is composed of bile salts, bicarbonate, bilirubin and other waste products. Bile salts are critical for the digestion and absorption of fats; bicarbonate serves as a buffer to protect small intestine for the acidic chyme; bilirubin gets converted to stercobilin in the small intestines and excreted with other waste products via stool.
Protein Synthesis
The liver plays a role in the production of clotting factors, as well as red blood cell production. The liver also produces albumin, the most abundant protein in blood serum. It is essential in the maintenance of oncotic pressure. The liver is a major site of production for thrombopoietin, a glycoprotein hormone that regulates the production of platelets by the bone marrow.
Hormones
The liver synthesizes angiotensinogen, a hormone that is responsible for raising the blood pressure when activated by renin.
Bile Secretion Route
As mentioned previously, bile is produced in the hepatocytes. It is transported into the canaliculi, from which it blows into a series of ducts (that gets bigger). Bile leaves the liver either draining directly into the duodenum via the common bile duct, or is temporarily stored in the gallbladder via the cystic duct. During a meal, the gallbladder contracts, which then secretes bile into the duodenum via the common bile duct.
Transport, Processing, and Elimination of Bilirubin
Red blood cell (RBC) has a typical life span of 120 days. When RBC reach the end of their life due to aging or defects (Figure 2 – 3), they are removed from the circulation by the phagocytic activity of macrophages in the spleen or the liver or hemolyze within the circulation. Within macrophages the hemoglobin molecule is broken up into heme and globin (Figure 2 – 4).
The heme is then further broken down into iron and biliverdin (Figure 2 – 5). Iron is salvaged for later use, it is stored as hemosiderin or ferritin in tissues and transported in plasma by beta globulins as transferrins (Figure 2 – 6). Biliverdin (green pigment) quickly reduces into bilirubin (yellow pigment). The unconjugated bilirubin is then released back into the blood, where it binds with albumin.

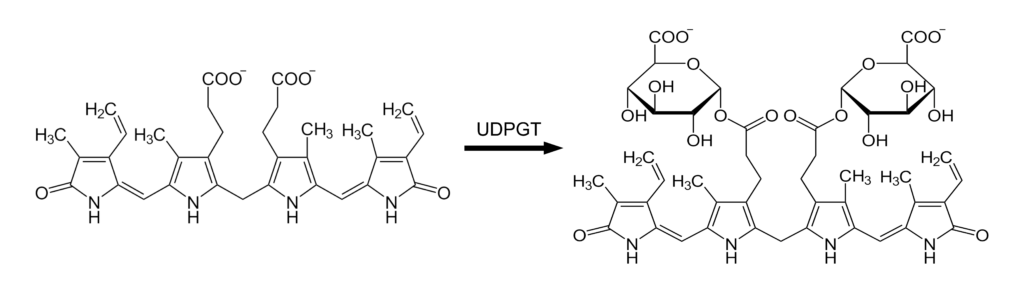
The unconjugated bilirubin-albumin complexes travel to the liver, where further catabolism takes place. Within the hepatocytes, bilirubin is conjugated by UDP-glucuronyl transferase (UDPGT) – addition of two molecules of glucuronic acid – which makes it soluble in water (Figure 3). Most of the conjugated bilirubin is secreted into bile canaliculi and out into the small intestine; some may go back into blood.
Bacteria in the intestines deconjugate and metabolize the bilirubin into colorless urobilinogen, which can be oxidized to form urobilin and stercobilin. Small amounts of urobilinogen will return to the liver via the hepatic portal vein to be recirculated into bile. Urobilin is excreted by the kidneys to give urine its yellow color and stercobilin is excreted in the feces giving stool its characteristic brown color (otherwise, stool would be clay-coloured).
For a video of animated bilirubin catabolism, see Hasudungan, A. Bilirubin Metabolism. YouTube.
Jaundice
Jaundice, is a yellowish or greenish pigmentation of the skin and whites of the eyes due to high bilirubin levels, or hyperbilirubinemia. It can be categorized into pre-hepatic, hepatic, and post-hepatic jandice, depending on where the disorder occurs in causing an accumulation of bilirubin. Causes include:
- Increased bilirubin production
- reduced bilirubin uptake by hepatic cells
- disrupted intracellular conjugation
- disrupted secretion of bilirubin into bile canaliculi
- intra/extra-hepatic bile duct obstruction
Please review common disorders (e.g., hemolytic anemia, Gilbert’s syndrome, Dubin-Johnson syndrome, hepatitis, cirrhosis, and post-hepatic obstruction) and how they relate to jaundice. (See Reading Resources section in the course website).
