65 13.3 Development of Gender
Learning Objectives
- Summarize the differences between gender and sex, and explain theories of gender development.
- Describe sexual orientation.
- Describe gender identity.
Development of gender
Before we discuss gender in detail, it is important to understand what gender actually is. The terms sex and gender are frequently used interchangeably, though they have different meanings. In this context, sex refers to the biological category of male, female or intersex as defined by physical differences in genetic composition and in reproductive anatomy and function. On the other hand, gender refers to the cultural, social, and psychological meanings that are associated with forming masculine, feminine and non-binary identities (Wood & Eagly, 2002). You can think of “male” and “female” as distinct categories of sex — a person is typically born a male or a female — but “masculine” and “feminine” as continuums associated with gender — many people have a certain degree of masculine and feminine traits and qualities.
Beyond sex and gender, there are a number of related terms that are also often misunderstood. Gender roles are the behaviours, attitudes, and personality traits that are designated as either masculine or feminine in a given culture. It is common to think of gender roles in terms of gender stereotypes, or the beliefs and expectations people hold about the typical characteristics, preferences, and behaviours of men and women. A person’s gender identity refers to their psychological sense of being female, man or non-binary. In contrast, a person’s sexual orientation is the direction of their emotional and erotic attraction toward members of the opposite sex, the same sex, or both sexes. These are important distinctions, and though we will not discuss each of these terms in detail, it is important to recognize that sex, gender, gender identity, and sexual orientation do not always correspond with one another. A person can be biologically male but have a female gender identity while being attracted to women or any other combination of identities and orientations.
Gender roles
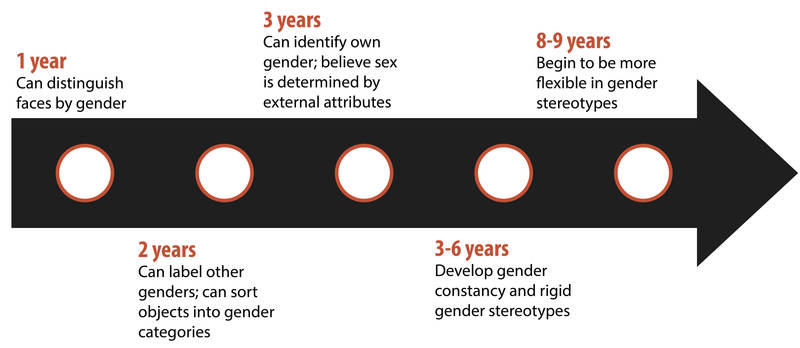
When do children start to learn about gender? The answer is that this begins at a very young age. By their first birthday, children can distinguish faces by gender. By their second birthday, they can label others’ gender and even sort objects into gender-typed categories. By the third birthday, children can consistently identify their own gender (Martin, Ruble, & Szkrybalo, 2002). At this age, children believe sex is determined by external attributes, not biological attributes. Between three and six years of age, children learn that gender is constant and cannot change simply by changing external attributes, having developed gender constancy. During this period, children also develop strong and rigid gender stereotypes. Stereotypes can refer to play (e.g., boys play with trucks, and girls play with dolls), traits (e.g., boys are strong, and girls like to cry), and occupations (e.g., men are doctors, and women are nurses). These stereotypes stay rigid until children reach about age eight or nine. Then, they develop cognitive abilities that allow them to be more flexible in their thinking about others.
How do our gender roles and gender stereotypes develop and become so strong? Many of our gender stereotypes are so strong because we emphasize gender so much in culture (Bigler & Liben, 2007). For example, males and females are treated differently before they are even born. When someone learns of a new pregnancy, the first question asked is “Is it a boy or a girl?” Immediately upon hearing the answer, judgments are made about the child: boys will be rough and like blue, while girls will be delicate and like pink. Developmental intergroup theory postulates that adults’ heavy focus on gender leads children to pay attention to gender as a key source of information about themselves and others, to seek out any possible gender differences, and to form rigid stereotypes based on gender that are subsequently difficult to change.

There are also psychological theories that partially explain how children form their own gender roles after they learn to differentiate based on gender. The first of these theories is gender schema theory. Gender schema theory argues that children are active learners who essentially socialize themselves. In this case, children actively organize others’ behaviour, activities, and attributes into gender categories, which are known as schemas. These schemas then affect what children notice and remember later. People of all ages are more likely to remember schema-consistent behaviours and attributes than schema-inconsistent behaviours and attributes. So, people are more likely to remember men, and forget women, who are firefighters. They also misremember schema-inconsistent information. If research participants are shown pictures of someone standing at the stove, they are more likely to remember the person to be cooking if depicted as a woman, and the person to be repairing the stove if depicted as a man. By only remembering schema-consistent information, gender schemas strengthen more and more over time.
A second theory that attempts to explain the formation of gender roles in children is social learning theory. Social learning theory argues that gender roles are learned through reinforcement, punishment, and modelling. Children are rewarded and reinforced for behaving in concordance with gender roles and punished for breaking gender roles. In addition, social learning theory argues that children learn many of their gender roles by modelling the behaviour of adults and older children and, in doing so, develop ideas about what behaviours are considered appropriate for each gender. Social learning theory has less support than gender schema theory. Research shows that parents do reinforce gender-appropriate play, but for the most part treat their male and female children similarly (Lytton & Romney, 1991).
Gender socialization
Different treatment by gender begins with parents. A meta-analysis of research from Canada and the United States found that parents most frequently treated sons and daughters differently by encouraging gender-stereotypical activities (Lytton & Romney, 1991). Fathers, more than mothers, are particularly likely to encourage gender-stereotypical play, especially in sons. Parents also talk to their children differently based on stereotypes. For example, parents talk about numbers and counting twice as often with sons than daughters (Chang, Sandhofer, & Brown, 2011) and talk to sons in more detail about science than with daughters. Parents are also much more likely to discuss emotions with their daughters than their sons.
Children do a large degree of socializing themselves. By age three, children play in gender-segregated play groups and expect a high degree of conformity. Children who are perceived as gender atypical (i.e., do not conform to gender stereotypes) are more likely to be bullied and rejected than their more gender-conforming peers.
Sexual orientation
A person’s sexual orientation is their emotional and erotic attraction toward another individual (see Figure 13.11). While the majority of people identify as heterosexual, there is a sizable population of people who identify as either homosexual or bisexual. Research suggests that somewhere between 3% and 10% of the U.S. population identifies as homosexual (Kinsey, Pomeroy, & Martin, 1998; LeVay, 1996; Pillard & Bailey, 1995).

Issues of sexual orientation have long fascinated scientists interested in determining what causes one individual to be heterosexual while another is homosexual. For many years, people believed that these differences arose because of different socialization and familial experiences. However, research has consistently demonstrated that family backgrounds and experiences are very similar among heterosexual and homosexual people (Bell, Weinberg, & Hammersmith, 1981; Ross & Arrindell, 1988). Issues related to sexual orientation and gender identity are very much influenced by sociocultural factors. Even the ways in which we define sexual orientation and gender vary from one culture to the next. In some instances, periods of exclusively homosexual behaviour are socially prescribed as a part of normal development and maturation. For example, in parts of New Guinea, young boys are expected to engage in sexual behaviour with other boys for a given period of time because it is believed that doing so is necessary for these boys to become men (Baldwin & Baldwin, 1989).
Genetic and biological mechanisms have also been proposed, and the balance of research evidence suggests that sexual orientation has an underlying biological component. For instance, over the past 25 years, research has demonstrated gene-level contributions to sexual orientation (Bailey & Pillard, 1991; Hamer, Hu, Magnuson, Hu, & Pattatucci, 1993; Rodriguez-Larralde & Paradisi, 2009), with some researchers estimating that genes account for at least half of the variability seen in human sexual orientation (Pillard & Bailey, 1998). Other studies report differences in brain structure and function between heterosexual and homosexual people (Allen & Gorski, 1992; Byne et al., 2001; Hu et al., 2008; LeVay, 1991; Ponseti et al., 2006; Rahman & Wilson, 2003a; Swaab & Hofman, 1990), and even differences in basic body structure and function have been observed (Hall & Kimura, 1994; Lippa, 2003; Loehlin & McFadden, 2003; McFadden & Champlin, 2000; McFadden & Pasanen, 1998; Rahman & Wilson, 2003b). In aggregate, the data suggest that to a significant extent, sexual orientations are something with which we are born.
Misunderstandings about sexual orientation
Regardless of how sexual orientation is determined, research has made clear that sexual orientation is not a choice, but rather it is a relatively stable characteristic of a person that cannot be changed. Claims of successful gay conversion therapy have received wide criticism from the research community due to significant concerns with research design, recruitment of experimental participants, and interpretation of data. As such, there is no credible scientific evidence to suggest that individuals can change their sexual orientation (Jenkins, 2010).
Dr. Robert Spitzer, the author of one of the most widely-cited examples of successful conversion therapy, apologized to both the scientific community and the gay community for his mistakes, and he publicly recanted his own paper in a public letter addressed to the editor of Archives of Sexual Behavior in the spring of 2012 (Carey, 2012). In this letter, Spitzer wrote:
I was considering writing something that would acknowledge that I now judge the major critiques of the study as largely correct. . . . I believe I owe the gay community an apology for my study making unproven claims of the efficacy of reparative therapy. I also apologize to any gay person who wasted time or energy undergoing some form of reparative therapy because they believed that I had proven that reparative therapy works with some “highly motivated” individuals. (Becker, 2012, para. 2, 5)
Citing research that suggests not only that gay conversion therapy is ineffective, but also potentially harmful, legislative efforts to make such therapy illegal have either been enacted (e.g., it is now illegal in California) or are underway across the United States, and many professional organizations have issued statements against this practice (Human Rights Campaign, n.d.)
Gender identity
Many people conflate sexual orientation with gender identity because of stereotypical attitudes that exist about homosexuality. In reality, these are two related, but different, issues. Gender identity refers to one’s sense of being male or female. Generally, our gender identities correspond to our chromosomal and phenotypic sex, but this is not always the case. The umbrella acronym LGBTQ+ is often used by people who refer to their sexual orientation or gender identity in a number of diverse ways: lesbian, gay, bisexual, trans, queer, and all others who use any non-traditional descriptors in their gender or sexual identity. Clearly, the traditional dichotomies of male-female or masculine-feminine do not capture the enormous variability that exists in human gender and sexual identity and expression.
When individuals do not feel comfortable identifying with the gender associated with their biological sex, they experience gender dysphoria. Gender dysphoria is a diagnostic category in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) that describes a conflict between how one identifies with regard to gender and how they present on the outside.
Many people who are classified as gender dysphoric seek to live their lives in ways that are consistent with their own gender identity. This involves dressing in clothing and assuming an identity that conforms with how they identify with regard to gender. These individuals may also undertake transgender hormone therapy to make their bodies look more like the sex with which they identify, and in some cases, they elect to have surgeries to alter the appearance of their external genitalia to resemble that of their preferred identity (see Figure 13.12). While these may sound like drastic changes, gender dysphoric individuals take these steps because their bodies seem to them to be a mistake of nature, and they seek to correct this mistake. Transgender (or trans) is the term most commonly used by people whose gender identity differs from their assigned sex at birth. Other people who might be seen as trans use no term at all to describe their gender identity, preferring instead to refrain from definitions. Indigenous Canadians may describe themselves as two-spirit, reflecting their understanding of gender role and spirituality in Indigenous culture (Provincial Health Services Authority Trans Care BC, 2019). Many cultures have words that describe an understanding of the diversity in gender identity. In Thailand, you can be male, female, or kathoey. A kathoey is an individual who would be described as intersexed or transgendered in Canada and the United States (Tangmunkongvorakul, Banwell, Carmichael, Utomo, & Sleigh, 2010).
Jurisdictions around the world vary in how they treat people who identify as LGBTQ+. In Canada, the Gender Identity Rights Bill C-16 was passed in 2017, protecting transgender and gender-diverse Canadians from discrimination under the Canadian Human Rights Act and from hate speech under the Criminal Code. It also allowed for sentencing decisions in hate crimes to include those committed against transgender and gender-diverse people.
Source: Adapted from Brown, Jewell, and Tam (2020) and Spielman et al. (2019).
Psychology in Everyday Life
The case of David Reimer
In August of 1965, Janet and Ronald Reimer of Winnipeg, Canada, welcomed the birth of their twin sons, Bruce and Brian. Within a few months, the twins were experiencing urinary problems; doctors recommended the problems could be alleviated by having the boys circumcised. A malfunction of the medical equipment used to perform the circumcision resulted in Bruce’s penis being irreparably damaged. Distraught, Janet and Ronald looked to expert advice on what to do with their baby boy. By happenstance, the couple became aware of Dr. John Money at Johns Hopkins University and his theory of psychosexual neutrality (Colapinto, 2000).
Dr. Money had spent a considerable amount of time researching transgendered individuals and individuals born with ambiguous genitalia. As a result of this work, he developed a theory of psychosexual neutrality. His theory asserted that we are essentially neutral at birth with regard to our gender identity and that we don’t assume a concrete gender identity until we begin to master language. Furthermore, Dr. Money believed that the way in which we are socialized in early life is ultimately much more important than our biology in determining our gender identity (Money, 1962).
Dr. Money encouraged Janet and Ronald to bring the twins to Johns Hopkins University, and he convinced them that they should raise Bruce as a girl. Left with few other options at the time, Janet and Ronald agreed to have Bruce’s testicles removed and to raise him as a girl. When they returned home to Canada, they brought with them Brian and his “sister,” Brenda, along with specific instructions to never reveal to Brenda that she had been born a boy (Colapinto, 2000).
Early on, Dr. Money shared with the scientific community the great success of this natural experiment that seemed to fully support his theory of psychosexual neutrality (Money, 1975). Indeed, in early interviews with the children, it appeared that Brenda was a typical little girl who liked to play with “girly” toys and do “girly” things.
However, Dr. Money was less than forthcoming with information that seemed to argue against the success of the case. In reality, Brenda’s parents were constantly concerned that their little girl wasn’t really behaving as most girls did, and by the time Brenda was nearing adolescence, it was painfully obvious to the family that she was really having a hard time identifying as a female. In addition, Brenda was becoming increasingly reluctant to continue her visits with Dr. Money to the point that she threatened suicide if her parents made her go back to see him again.
At that point, Janet and Ronald disclosed the true nature of Brenda’s early childhood to their daughter. While initially shocked, Brenda reported that things made sense to her now, and ultimately, by the time she was an adolescent, Brenda had decided to identify as a male. Thus, she became David Reimer.
David was quite comfortable in his masculine role. He made new friends and began to think about his future. Although his surgery had left him infertile, he still wanted to be a father. In 1990, David married a single mother and loved his new role as a husband and father. In 1997, David was made aware that Dr. Money was continuing to publicize his case as a success supporting his theory of psychosexual neutrality. This prompted David and his brother to go public with their experiences in an attempt to discredit the doctor’s publications. While this revelation created a firestorm in the scientific community for Dr. Money, it also triggered a series of unfortunate events that ultimately led to David committing suicide in 2004 (O’Connell, 2004).
This sad story speaks to the complexities involved in gender identity. While the Reimer case had earlier been paraded as a hallmark of how socialization trumped biology in terms of gender identity, the truth of the story made the scientific and medical communities more cautious in dealing with cases that involve intersex children and how to deal with their unique circumstances. In fact, stories like this one have prompted measures to prevent unnecessary harm and suffering to children who might have issues with gender identity. For example, in 2013, a law took effect in Germany allowing parents of intersex children to classify their children as indeterminate so that children can self-assign the appropriate gender once they have fully developed their own gender identities (Paramaguru, 2013).
Key Takeaways
- Gender and sex are different concepts.
- Gender development begins in early childhood. Parents and others reinforce gender stereotypes.
- Sexual orientation is distinct from gender identity.
Exercises and Critical Thinking
- What can parents do to allow their children to develop gender roles that are not constrained by stereotypes?
- How would you react if your child came out as trans?
- What hurdles do non-gender-conforming children face?
Image Attributions
Figure 13.8. Uniquely Bhutanese by Michael Foley is used under a CC BY-NC-ND 2.0 license.
Figure 13.9. Used under a CC BY-NC-SA 4.0 license.
Figure 13.10. The Girls by Billy V is used under a CC BY-NC-SA 2.0 license.
Figure 13.11. Gay Couple From Back Hand Holding on CSD 2006 Berlin – Make Love Not War by Till Krech is used under a CC BY 2.0 license.
Figure 13.12. Used under a CC BY 4.0 license.
References
Allen, L. S., & Gorski, R. A. (1992). Sexual orientation and the size of the anterior commissure in the human brain. Proceedings of the National Academy of Sciences, USA, 89, 7199–7202.
Bailey, M. J., & Pillard, R. C. (1991). A genetic study of male sexual orientation. Archives of General Psychiatry, 48, 1089–1096.
Baldwin, J. D., & Baldwin, J. I. (1989). The socialization of homosexuality and heterosexuality in a non-western society. Archives of Sexual Behavior, 18, 13–29.
Becker, J. M. (2012, April 25). Dr. Robert Spitzer apologizes to gay community for infamous “ex-gay” study. Truth Wins Out. Retrieved from http://www.truthwinsout.org/news/2012/04/24542
Bell, A. P., Weinberg, M. S., & Hammersmith, S. K. (1981). Sexual preferences: Its development in men and women. Bloomington: Indiana University Press.
Bigler, R. S., & Liben, L. S. (2007). Developmental intergroup theory: Explaining and reducing children’s social stereotyping and prejudice. Current Directions in Psychological Science, 16(3), 162–166.
Brown, C. S., Jewell, J. A., & Tam, M J. (2020). Gender. In R. Biswas-Diener & E. Diener (Eds.), Noba textbook series: Psychology. Champaign, IL: DEF. Retrieved from http://noba.to/ge5fdhba
Byne, W., Tobet, S., Mattiace, L. A., Lasco, M. S., Kemether, E., Edgar, M. A., . . . Jones, L. B. (2001). The interstitial nuclei of the human anterior hypothalamus: An investigation of variation with sex, sexual orientation, and HIV status. Hormones and Behavior, 40, 86–92.
Carey, B. (2012, May 18). Psychiatry giant sorry for backing gay ‘cure.’ The New York Times. Retrieved from http://www.nytimes.com/2012/05/19/health/dr-robert-l-spitzer-noted-psychiatrist-apologizes-for-study-on-gay-cure.html?_r=0
Chang, A., Sandhofer, C. M., & Brown, C. S. (2011). Gender biases in early number exposure to preschool-aged children. Journal of Language and Social Psychology, 30(4), 440–450.
Colapinto, J. (2000). As nature made him: The boy who was raised as a girl. New York, NY: Harper Collins.
Hall, J. A., & Kimura, D. (1994). Dermatoglyphic asymmetry and sexual orientation in men. Behavioral Neuroscience, 108(6), 1203–1206.
Hamer, D. H., Hu, S., Magnuson, V. L., Hu, N., & Pattatucci, A. M. (1993). A linkage between DNA markers on the X chromosome and male sexual orientation. Science, 261, 321–327.
Hu, S. H., Wei, N., Wang, Q. D., Yan, L. Q., Wei, E. Q., Zhang, M. M., . . . Xu, Y. (2008). Patterns of brain activation during visually evoked sexual arousal differ between homosexual and heterosexual men. American Journal of Neuroradiology, 29, 1890–1896.
Human Rights Campaign. (n.d.). The lies and dangers of efforts to change sexual orientation or gender identity. Retrieved from http://www.hrc.org/resources/entry/the-lies-and-dangers-of-reparative-therapy
Jenkins, W. J. (2010). Can anyone tell me why I’m gay? What research suggests regarding the origins of sexual orientation. North American Journal of Psychology, 12, 279–296.
Kinsey, A. C., Pomeroy, W. B., & Martin, C. E. (1998). Sexual behavior in the human male. Bloomington: Indiana University Press. (Original work published 1948)
LeVay, S. (1991). A difference in the hypothalamic structure between heterosexual and homosexual men. Science, 253, 1034–1037.
LeVay, S. (1996). Queer science: The use and abuse of research into homosexuality. Cambridge, MA: MIT Press.
Lippa, R. A. (2003). Handedness, sexual orientation, and gender-related personality traits in men and women. Archives of Sexual Behavior, 32, 103–114.
Loehlin, J. C., & McFadden, D. (2003). Otoacoustic emissions, auditory evoked potentials, and traits related to sex and sexual orientation. Archives of Sexual Behavior, 32, 115–127.
Lytton, H., & Romney, D. M. (1991). Parents’ differential socialization of boys and girls: A meta-analysis. Psychological Bulletin, 109(2), 267–296.
Martin, C. L., Ruble, D. N., & Szkrybalo, J. (2002). Cognitive theories of early gender development. Psychological Bulletin, 128(6), 903–933.
McFadden, D., & Champlin, C. A. (2000). Comparisons of auditory evoked potentials in heterosexual, homosexual, and bisexual males and females. Journal of the Association for Research in Otolaryngology, 1, 89–99.
McFadden, D., & Pasanen, E. G. (1998). Comparisons of the auditory systems of heterosexuals and homosexuals: Clicked-evoked otoacoustic emissions. Proceedings of the National Academy of Sciences, USA, 95, 2709–2713.
Money, J. (1962). Cytogenic and psychosexual incongruities with a note on space-form blindness. Paper presented at the 118th meeting of the American Psychiatric Association, Toronto, Canada.
Money, J. (1975). Ablatio penis: Normal male infant sex-reassigned as a girl. Archives of Sexual Behavior, 4, 65–71.
O’Connell, S. (Writer/Producer). (2004). Dr. Money and the boy with no penis [Television documentary series episode]. In Horizon. London, England: BBC.
Paramaguru, K. (2013, November 12). Boy, girl or intersex? Germany adjusts to a third option at birth. Time. Retrieved from http://world.time.com/2013/11/12/boy-girl-or-intersex
Pillard, R. C., & Bailey, M. J. (1995). A biologic perspective on sexual orientation. The Psychiatric Clinics of North America, 18(1), 71–84.
Pillard, R. C., & Bailey, M. J. (1998). Sexual orientation has a heritable component. Human Biology, 70(2), 347–365.
Ponseti, J., Bosinski, H. A., Wolff, S., Peller, M., Jansen, O., Mehdorn, H. M., . . . Siebner, H. R. (2006). A functional endophenotype for sexual orientation in humans. Neuroimage, 33(3), 825–833.
Provincial Health Services Authority, Trans Care BC. (2019). Two-spirit. Retrieved from http://www.phsa.ca/transcarebc/trans-basics/two-spirit
Rahman, Q., & Wilson, G. D. (2003a). Large sexual-orientation-related differences in performance on mental rotation and judgment of line orientation tasks. Neuropsychology, 17, 25–31.
Rahman, Q., & Wilson, G. D. (2003b). Sexual orientation and the 2nd to 4th finger length ratio: Evidence for organising effects of sex hormones or developmental instability? Psychoneuroendocrinology, 28, 288–303.
Rodriguez-Larralde, A., & Paradisi, I. (2009). Influence of genetic factors on human sexual orientation. Investigacion Clinica, 50, 377–391.
Ross, M. W., & Arrindell, W. A. (1988). Perceived parental rearing patterns of homosexual and heterosexual men. The Journal of Sex Research, 24, 275–281.
Spielman, R., Dumper, K., Jenkins, W., Lacombe, A., Lovett, M., & Perlmutter, M. (2019). Emotions and motivation. In OpenStax, Psychology. OpenStax CNX. Retrieved from https://cnx.org/contents/Sr8Ev5Og@10.16:UQgvP5NH@9
Swaab, D. F., & Hofman, M. A. (1990). An enlarged suprachiasmatic nucleus in homosexual men. Brain Research, 537, 141–148.
Tangmunkongvorakul, A., Banwell, C., Carmichael, G., Utomo, I. D., & Sleigh, A. (2010). Sexual identities and lifestyles among non-heterosexual urban Chiang Mai youth: Implications for health. Culture, Health, and Sexuality, 12, 827–841.
Wood, W., & Eagly, A. H. (2002). A cross-cultural analysis of the behavior of women and men: Implications for the origins of sex differences. Psychological Bulletin, 128(5), 699–727.

{kind=link}