1203 Chapter 20. The Cardiovascular System: Blood Vessels and Circulation
20.6 Development of Blood Vessels and Fetal Circulation
Learning Objectives
By the end of this section, you will be able to:
- Describe fetal circulation
- Describe the changes which occur in the fetal circulation following delivery
In a developing embryo,the heart has developed enough by day 21 post-fertilization to begin beating. Circulation patterns are clearly established by the fourth week of embryonic life. It is critical to the survival of the developing human that the circulatory system forms early to supply the growing tissue with nutrients and gases, and to remove waste products. Blood cells and vessel production in structures outside the embryo proper called the yolk sac, chorion, and connecting stalk begin about 15 to 16 days following fertilization. Development of these circulatory elements within the embryo itself begins approximately 2 days later. You will learn more about the formation and function of these early structures when you study the chapter on development. During those first few weeks, blood vessels begin to form from the embryonic mesoderm. The precursor cells are known as hemangioblasts. These in turn differentiate into angioblasts, which give rise to the blood vessels and pluripotent stem cells, which differentiate into the formed elements of blood. (Seek additional content for more detail on fetal development and circulation.) Together, these cells form masses known as blood islands scattered throughout the embryonic disc. Spaces appear on the blood islands that develop into vessel lumens. The endothelial lining of the vessels arise from the angioblasts within these islands. Surrounding mesenchymal cells give rise to the smooth muscle and connective tissue layers of the vessels. While the vessels are developing, the pluripotent stem cells begin to form the blood.
Vascular tubes also develop on the blood islands, and they eventually connect to one another as well as to the developing, tubular heart. Thus, the developmental pattern, rather than beginning from the formation of one central vessel and spreading outward, occurs in many regions simultaneously with vessels later joining together. This angiogenesis—the creation of new blood vessels from existing ones—continues as needed throughout life as we grow and develop.
Blood vessel development often follows the same pattern as nerve development and travels to the same target tissues and organs. This occurs because the many factors directing growth of nerves also stimulate blood vessels to follow a similar pattern. Whether a given vessel develops into an artery or a vein is dependent upon local concentrations of signaling proteins.
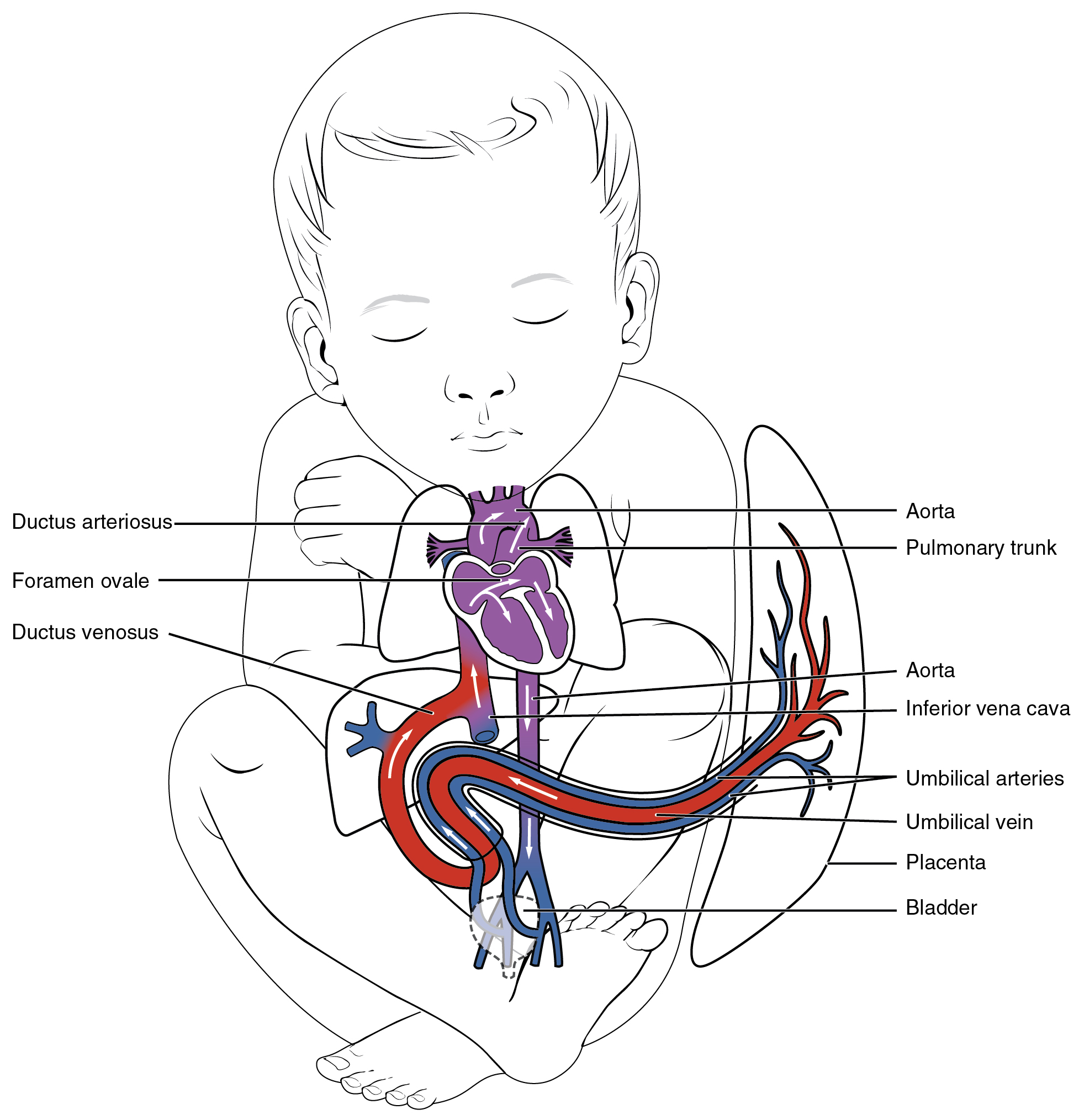
As the embryo grows within the mother’s uterus, its requirements for nutrients and gas exchange also grow. The placenta—a circulatory organ unique to pregnancy—develops jointly from the embryo and uterine wall structures to fill this need. Emerging from the placenta is the umbilical vein, which carries oxygen-rich blood from the mother to the fetal inferior vena cava via the ductus venosus to the heart that pumps it into fetal circulation. Two umbilical arteries carry oxygen-depleted fetal blood, including wastes and carbon dioxide, to the placenta. After birth, the umbilical vein and arteries regress to become the ligamentum teres and the medial umbilical ligament, respectively.
There are three major shunts—alternate paths for blood flow—found in the circulatory system of the fetus. Two of these shunts divert blood from the pulmonary to the systemic circuit, whereas the third connects the umbilical vein to the inferior vena cava. The first two shunts are critical during fetal life, when the lungs are compressed, filled with amniotic fluid, and nonfunctional, and gas exchange is provided by the placenta. These shunts close shortly after birth, however, when the newborn begins to breathe. The third shunt persists a bit longer but becomes nonfunctional once the umbilical cord is severed. The three shunts are as follows (Figure 1):
- The foramen ovale is an opening in the interatrial septum that allows blood to flow from the right atrium to the left atrium. A valve associated with this opening prevents backflow of blood during the fetal period. As the newborn begins to breathe and blood pressure in the atria increases, this shunt closes. The fossa ovalis remains in the interatrial septum after birth, marking the location of the former foramen ovale.
- The ductus arteriosus is a short, muscular vessel that connects the pulmonary trunk to the aorta. Most of the blood pumped from the right ventricle into the pulmonary trunk is thereby diverted into the aorta. Only enough blood reaches the fetal lungs to maintain the developing lung tissue. When the newborn takes the first breath, pressure within the lungs drops dramatically, and both the lungs and the pulmonary vessels expand. As the amount of oxygen increases, the smooth muscles in the wall of the ductus arteriosus constrict, sealing off the passage. Eventually, the muscular and endothelial components of the ductus arteriosus degenerate, leaving only the connective tissue component of the ligamentum arteriosum.
- The ductus venosus is a temporary blood vessel that branches from the umbilical vein, allowing much of the freshly oxygenated blood from the placenta—the organ of gas exchange between the mother and fetus—to bypass the fetal liver and go directly to the fetal heart. The ductus venosus closes slowly during the first weeks of infancy and degenerates to become the ligamentum venosum.