Chapter 3 Neoplasia
Neoplasms – Immune Response and Immunotherapy
Pictures coming soon!
Zoë Soon
Innate and Adaptive Immune Responses to Cancerous Cells
Within the innate immune response, there are several leukocytes (i.e., White Blood Cells, WBCs) that play key roles in destroying cancerous cells. For example, powerful phagocytes (neutrophils, macrophages, and dendritic cells) as well as cytotoxic Natural Killer cells (NK cells) are able to recognize and kill many tumor cells. Additionally, the adaptive immune response, with various types of T cells, B cells, and antibodies also can play a role in recognizing tumor cells and targeting them for destruction. In order for a cancer to survive therefore it must evade the innate and adaptive immune systems.
Innate Immune Response to Cancerous Cells
There are many components to the innate immune response, which include physical barriers (e.g., skin, hair, fingernails), chemicals (e.g., gastric acid, bile, normal flora), mechanical barriers (e.g., flushing of urine), phagocytic white blood cells (e.g., macrophages, monocytes, dendritic cells, neutrophils, and eosinophils), non-specific cytotoxic white blood cells (i.e., Natural Killer cells), certain plasma proteins (e.g., fibrinogen, complement proteins, and C-reactive proteins) and chemical messages (e.g., chemotactic chemokines, pro-inflammatory cytokines and pyrogens).
Innate Immune Response to Cancerous Cells – Phagocytes
Phagocytic white blood cells (WBCs or leukocytes) are capable of phagocytosing cell debris, as well as cells that display non-self (foreign) antigens. Most often these antigens belong to infectious agents or pathogens (e.g., bacteria, viruses), but sometimes these antigens are specific to tumor cells. Tumor-specific antigens (TSAs) are often coded by unmutated, abnormally spliced transcripts that are translated into unstable-short lived proteins that are unique to tumor cells. As these TSAs are non-self, non-specific phagocytes (e.g., macrophages, neutrophils, dendritic cells, and monocytes) are at times able to phagocytose tumor cells. Although this can be challenging as TSAs are unstable and present in low densities. It can also be difficult for phagocytes to penetrate and be activated within a tumor.
Innate Immune Response to Cancerous Cells – NK cells
Natural Killer Lymphocytes (NK cells) play an important role in the innate response and are capable of killing both virally-infected and cancerous cells. This is achieved by their ability to check cells for self-antigens (Class I MHC Major Histocompatibility Complex molecules). Virally-infected cells typically display viral antigens on their cell surface Class I MHC molecules that stimulate NK cells. Cancerous cells on the other hand, can stimulate NK cells, because they are “missing-self” surface molecules, due to down-regulating the expression of the cell’s Class I MHC surface molecules. Once active, NK cells release perforin proteins that create portals in the targeted virally-infected or cancerous cell. NK cells also release the enzyme granzyme which travels through the perforin portal into the target cell which induces apoptosis and cytolysis. At the same time, activated NK cells release pro-inflammatory cytokines which serve to recruit and activate other white blood cells (WBCs) such as CD8+ Cytotoxic T cells, mast cells, basophils, macrophages and neutrophils. These cytokines also have potent anti-proliferative, anti-angiogenic, and pro-apoptotic effects on the cancerous cells. However, large solid tumors are often poorly oxygenated and difficult to penetrate – both the hypoxia and cellular density are challenge to NK cell abilities. Additionally, some tumors are able to suppress the anti-tumor effects of NK cells. Research is being done on strengthening the NK cell response to cancerous cells.
Adaptive Immune Response to Cancerous Cells
APC Activation of T cells, B cells, and Production of Anti-Tumor Antibodies
The adaptive immune system plays an important role in protecting against infectious agents (i.e. pathogens) as well as cancerous cells. Both T and B lymphocytes (T and B cells) are responsible for orchestrating a targeted attack of pathogenic and cancerous cells. Once activated Cytotoxic (CD8+) T cells produce daughter Cytotoxic T cells, that embark on a “search and destroy” mission, destroying cells that contain pathogenic or tumor-specific antigens. When B cells are activated, they proliferate to produce daughter cells that generate antibodies that will specifically bind to pathogenic or tumor-specific antigens, targeting them for phagocytosis by immune system phagocytes (e.g., neutrophils).
In order for T and B cells to become activated and launch a defense, non-self antigens (e.g., viral antigens, bacterial antigens or tumor-specific antigens) must be detected. In the case of pathogens, typically, Antigen-Presenting Cells, (i.e., APCs, which include macrophages and dendritic cells) are able to phagocytose pathogens and then display pathogen antigens on their cell surface using MHC Class II molecules in order to stimulate T and B cell activity and antibody production. APCs can also do this with tumor cells and tumor-specific antigens (TSAs), however, there are 2 challenges:
a) Most TSAs are unstable and short-lived, so most don’t survive phagocytosis and then display by APCs.
b) Tumor cells are often not surrounded by enough chemokines and cytokines that are required for attracting and activating APCs.
Malignant tumor cells that evade the adaptive immune system can spread and metastasize.
Direct Activation of Cytotoxic CD8+ T cells by Tumor Cells
It is known that Cytotoxic T cells (CD8+ cells) are capable of becoming active by directly interacting with foreign antigens (e.g., pathogens antigens or tumor-specific antigens, TSAs). However, T cell activation by tumor cells may be low or non-existent for a few reasons:
a) Most tumor cells often arise from epithelial cells, which express low levels of MHC Class I molecules, and therefore TSAs are displayed on the surface of cells at a low level.
b) Most TSAs are unstable and short-lived which limits the ability for Cytotoxic T cells to bind them and be activated.
Research is being done on strengthening the APC, T and B cell responses to cancerous cells.
Malignant Neoplasms – Immunotherapy
There are many strategies in place for harnessing the immune system and strengthening its response and ability to eliminate cancerous cells. Some of these strategies include using Biological Response Modifiers (BRMs). BRMs are able to enhance or suppress the immune response. There are many types of BRMs that are useful in treating many different diseases (e.g., cancer, autoimmune diseases, chronic inflammatory diseases, and some cases of cardiovascular diseases).
Biological Response Modifiers (BRMs) that are used to treat some cancers include:
- Antibodies (produced in the lab) that bind to specifically to receptors that are present on some types of cancerous cells. Antibodies once bound to receptors on the surface of cancer cells act as opsonins and enable phagocytes (e.g., neutrophils and macrophages) to engulf and destroy the cancerous cell. Examples include:
-
- Antibodies against Human Epidermal Growth Factor Receptor 2 (HER-2) on some types of breast cancers.
- Antibodies against CD20, a cell membrane protein found on some types of B cell cancers (lymphomas).
-
- Radioactive Antibodies: similar to the above example, monoclonal antibodies are produced in the lab and then attached to radioactive isotopes. The antibodies bind to the specific tumor cell antigens, and the radioactive isotope degrades releasing damaging particles and energy that kills the cancerous cell. Both above examples can be radiolabelled, e.g.,
- Radioactive Antibodies against Human Epidermal Growth Factor Receptor 2 (HER-2) on some types of breast cancers.
- Antibodies against CD20, a cell membrane protein found on some types of B cell cancers (lymphomas).
- Chemotherapy Drug conjugated Antibodies: monoclonal antibodies can also be attached to chemotherapy drugs. The antibodies bind to the specific tumor cell antigens, and the chemotherapy drug blocks cell cycling and/or kills the cancerous cell.
- Interferons: specific types of alpha interferons stimulate a greater immune response
- Interleukin: specific types of interleukins are helpful in stimulating specific types of B cells (i.e., plasma cells) to produce more antibodies.
- Granulocyte Macrophage Colony Stimulating Factors (GM-CSF) are growth factors that stimulate the production of granulocytes (e.g., neutrophils and basophils) and macrophages which boost the immune response
- Vaccines to Prevent Cancer
- Human Papillomavirus (HPV) vaccine protects against HPV infections, as HPV oncoviruses are a risk factor for cancers of the cervix, penis, vagina, and oropharynx
- Hepatitis B Virus (HBV) vaccine protects against the oncovirus HBV which is a risk factor for liver cancer
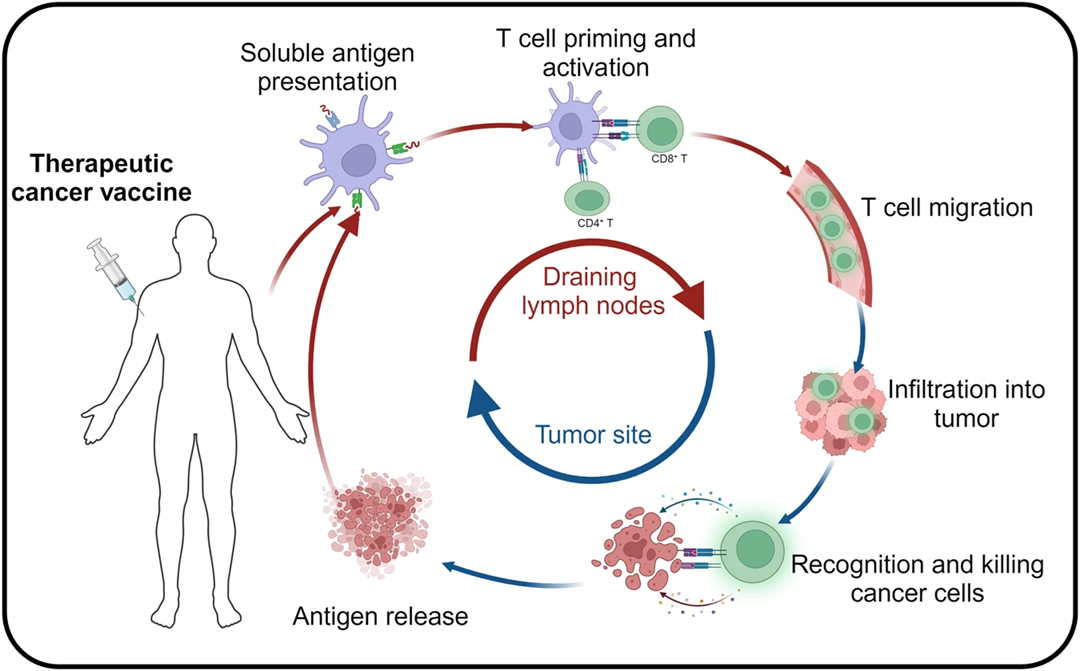
- Vaccines to Treat Cancer
- Bacillus Calmette- Guerin (BCG) vaccine was originally developed to prevent Tuberculosis. It is used to treat early-stage bladder cancer as it stimulates bladder inflammation and an immune response
- Vaccines being Researched for Treating Cancer
- Tumor whole cell vaccines – vaccines made from specific tumor cells
- Tumor Antigen vaccines – vaccines made from tumor antigens
- Dendritic Cell (DC) vaccines – made by harvesting DC cells and growing with cancer cells, priming DC cells to recognize tumor-specific antigens
- Other Immunotherapies being Researched
- Enhancing T cell immune response
- Enhancing Macrophage immune response
Media Attributions
- Possible Personalized Cancer Vaccine Therapies © Ting Fan, Mingna Zhang, Jingxian Yang, Zhounan Zhu, Wanlu Cao & Chunyan Dong is licensed under a CC BY (Attribution) license
