Chapter 3 Neoplasia
Prostate Cancer
Pictures coming soon!
Zoë Soon
Prostate Cancer – What is it?
The glandular epithelial cells normally produce prostatic fluid which is required for sperm function. After, skin cancer, prostate cancer is the most common form of cancer in biological males (XY). Prostate cancer most often occurs at the age of 50 and is generally slow growing, meaning that routine screening can result in earlier diagnosis. Despite this, prostate cancer remains the 2nd most common cause of cancer death in males. In 95% of all prostate cancers, the glandular epithelial cells within the prostate (typically on the periphery) become cancerous through DNA mutations, and the cancer is considered an adenocarcinoma. Mutations often involve proto-oncogenes and tumor suppressor genes (TSG) that are responsible for regulating the rates of cell cycling, cell differentiation, and apoptosis. Mutations in p53 TSG are common in prostate cancer and lead to an inappropriate increase in cell proliferation and cells accumulate uncontrollably.

Prostate Cancer – Risk Factors and Prevention Strategies
Age and country of residence are risk factors, with males living in countries with the highest economic indexes being the most at risk. The balance of hormones are thought to play a role as some prostate cancers are androgen dependent and higher testosterone, androgen receptor levels, insulin-like growth factor-1 (IGF-1), and tall adult height are known risk factors. However, given that testosterone levels decrease with age and the fact that prostate cancer is rare before the age of 40, other factors are thought to play pivotal roles. Family history, particularly having first-degree relatives that have been diagnosed with prostate cancer is a pre-disposing factor. Genetic susceptibility may be part of the reason Black males (of African or Caribbean ancestry) are more at risk for prostate cancer and more aggressive metastatic forms of prostate cancer, however socioeconomics can also be factors and are considered significant contributors to all diseases. Mutations in several genes (including BRCA1 and BRCA2) are risk factors. Other pre-disposing factors include: abdominal obesity (apple-shape), high BMI, metabolic syndrome, and smoking. Additionally, sedentary behaviour, consumption of red meat and a high-fat, low-vegetable diet also all increase the risk of prostate cancer.
Prevention strategies include healthy diet, regular physical activity, maintaining healthy BMI, and cessation of smoking.
Prostate Cancer – Signs and Symptoms
As with many cancers, frequently there are no signs and symptoms until the cancer has developed.
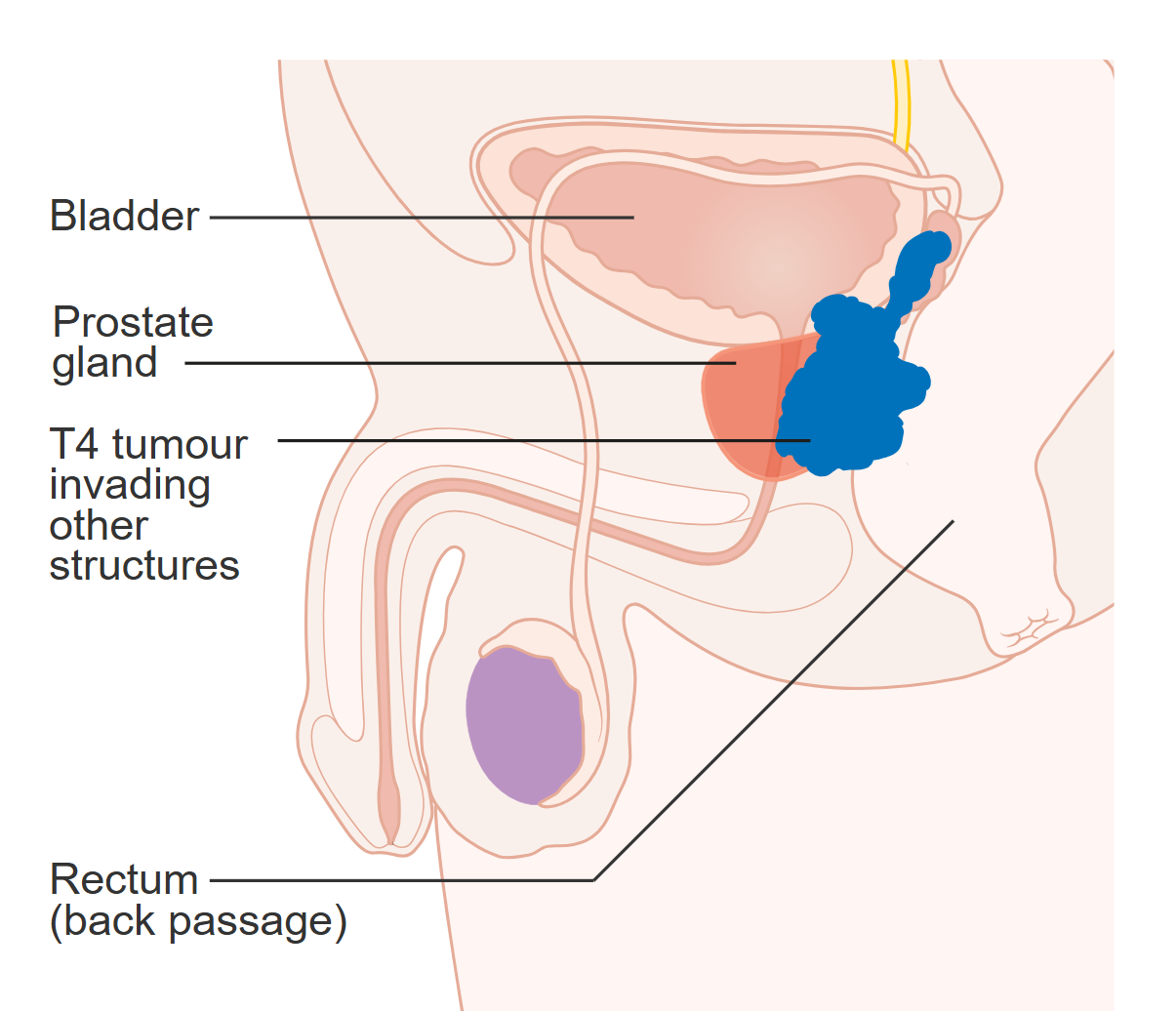
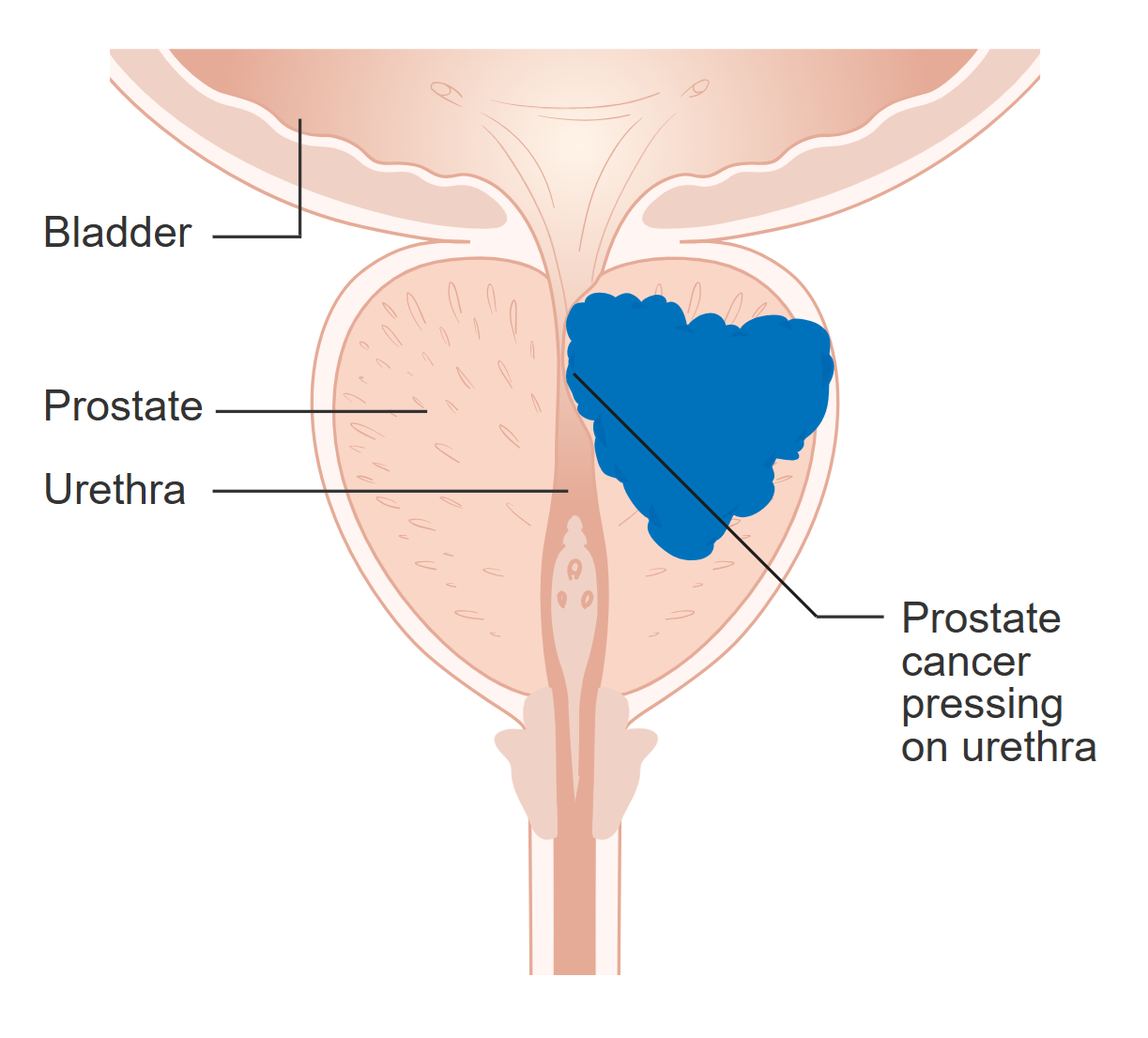
As the growth of the tumor begins to impinge on the urethra, the first signs and symptoms can be similar to benign prostatic hyperplasia (BPH), and include lower urinary tract symptoms (LUTS): urinary frequency, urinary urgency, decreased urine flow rates, dysuria, and hematuria. There can also be erectile dysfunction and back pain, pelvis pain, or pain when sitting or when ejaculating.
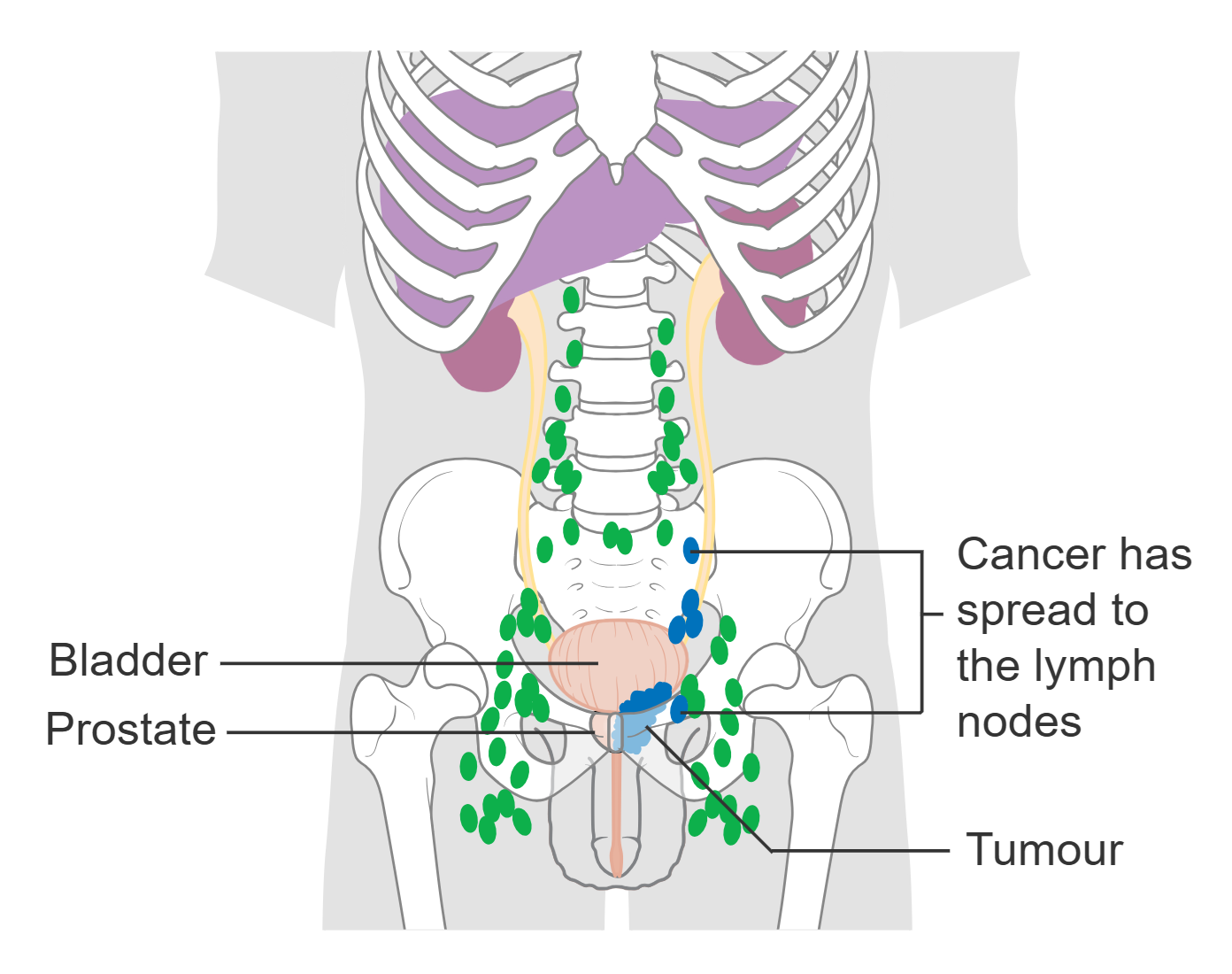
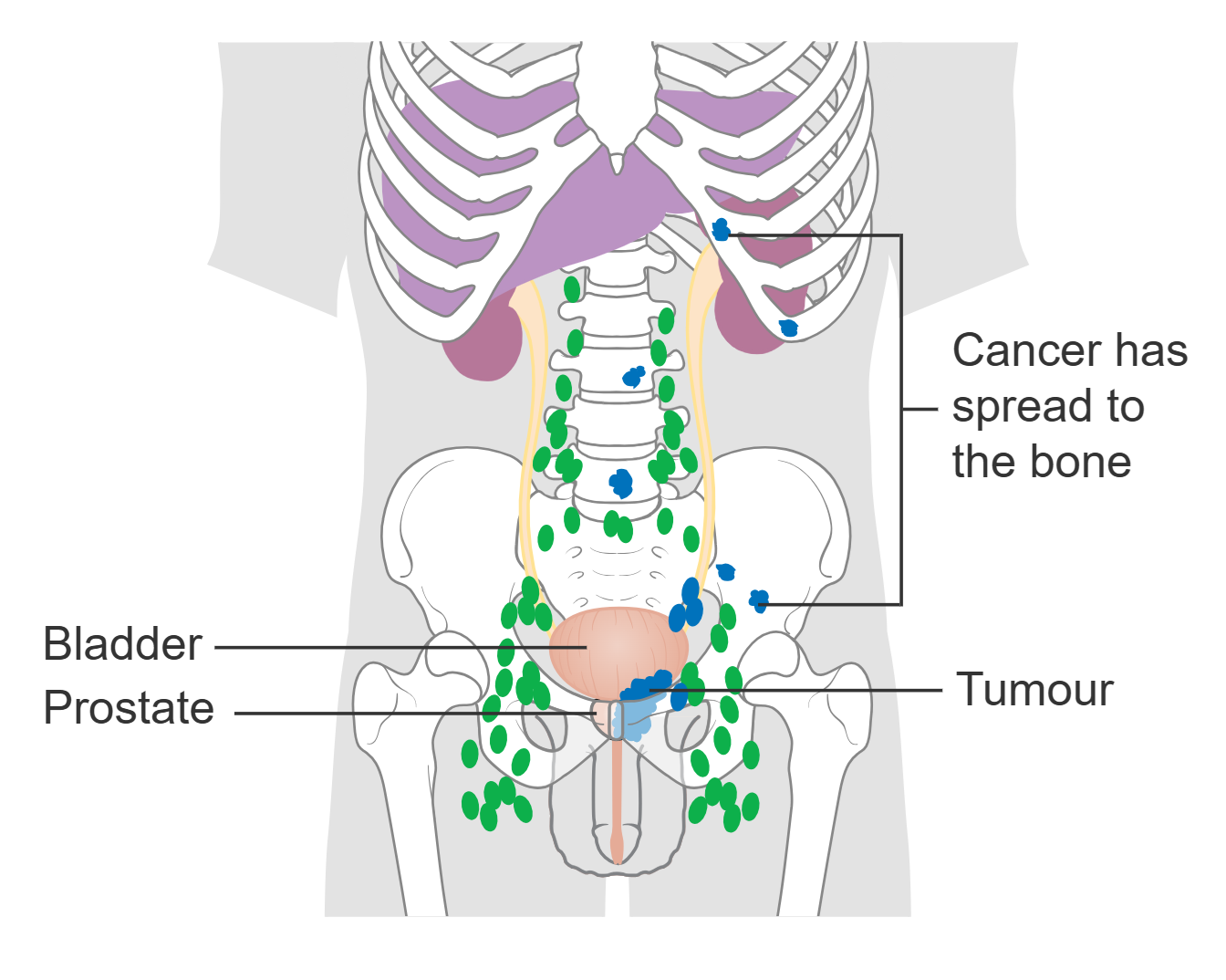
More advance stages of metastatic prostate cancer include signs and symptoms that are common with other metastatic cancers: unexplained weight loss and anorexia (loss of appetite), fatigue, cachexia, anemia, and bone pain, pain and edema, and signs of kidney failure (e.g., uremic symptoms = high blood urea nitrogen, BUN and serum creatinine levels, pruritis, nausea, vomiting, brain fog, fatigue). Metastasis to local lymph nodes and bones of the pelvic girdle, vertebrae, ribs may occur without treatment.
Prostate Cancer – Diagnosis
Screening that involves assessing for increases in blood levels of prostate-specific antigen (PSA) as well as digital rectal exams (DRE) has allowed for asymptomatic cases to be diagnosed and treated earlier. DRE can reveal hard nodules on the prostate gland as well as changes in size or contour that can occur with prostate cancer. Prostate cancer found early have a 100% survival rate, whereas metastatic prostate cancer is rarely curable.
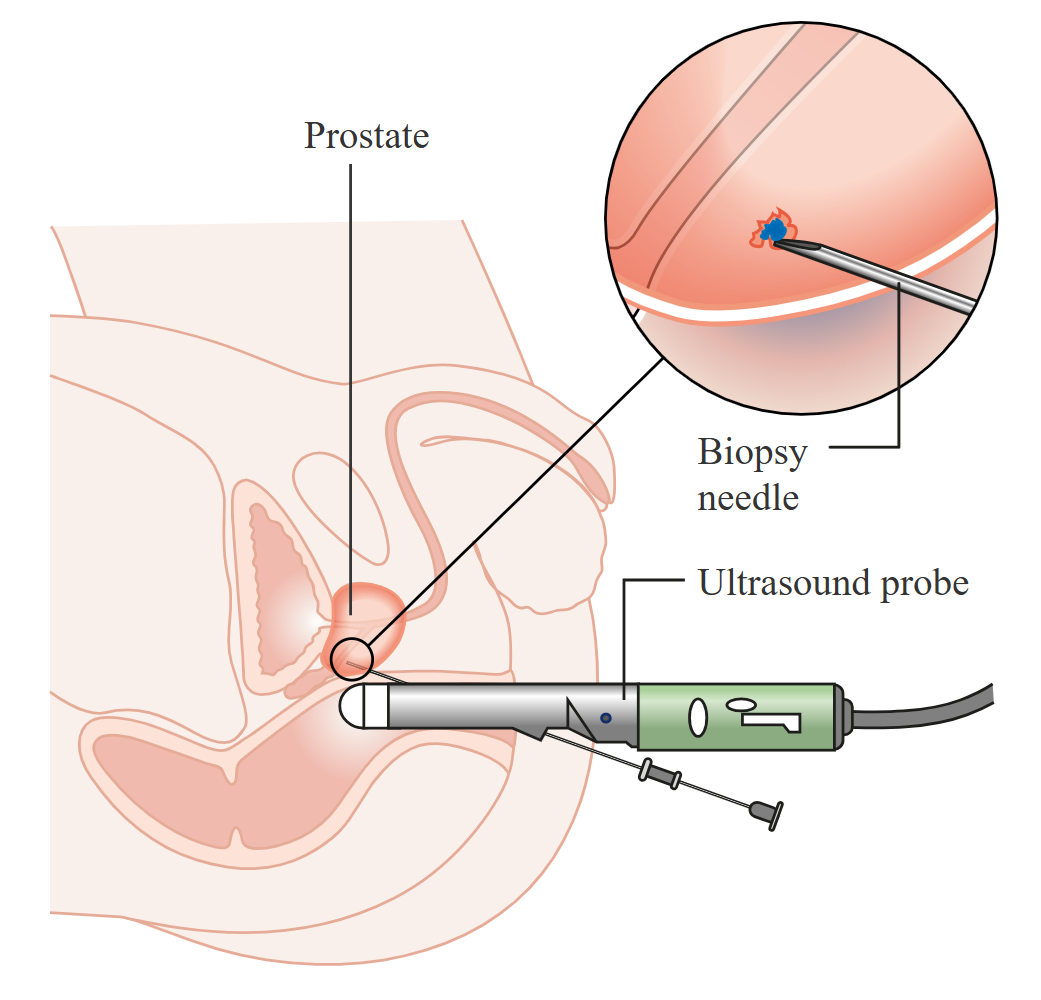
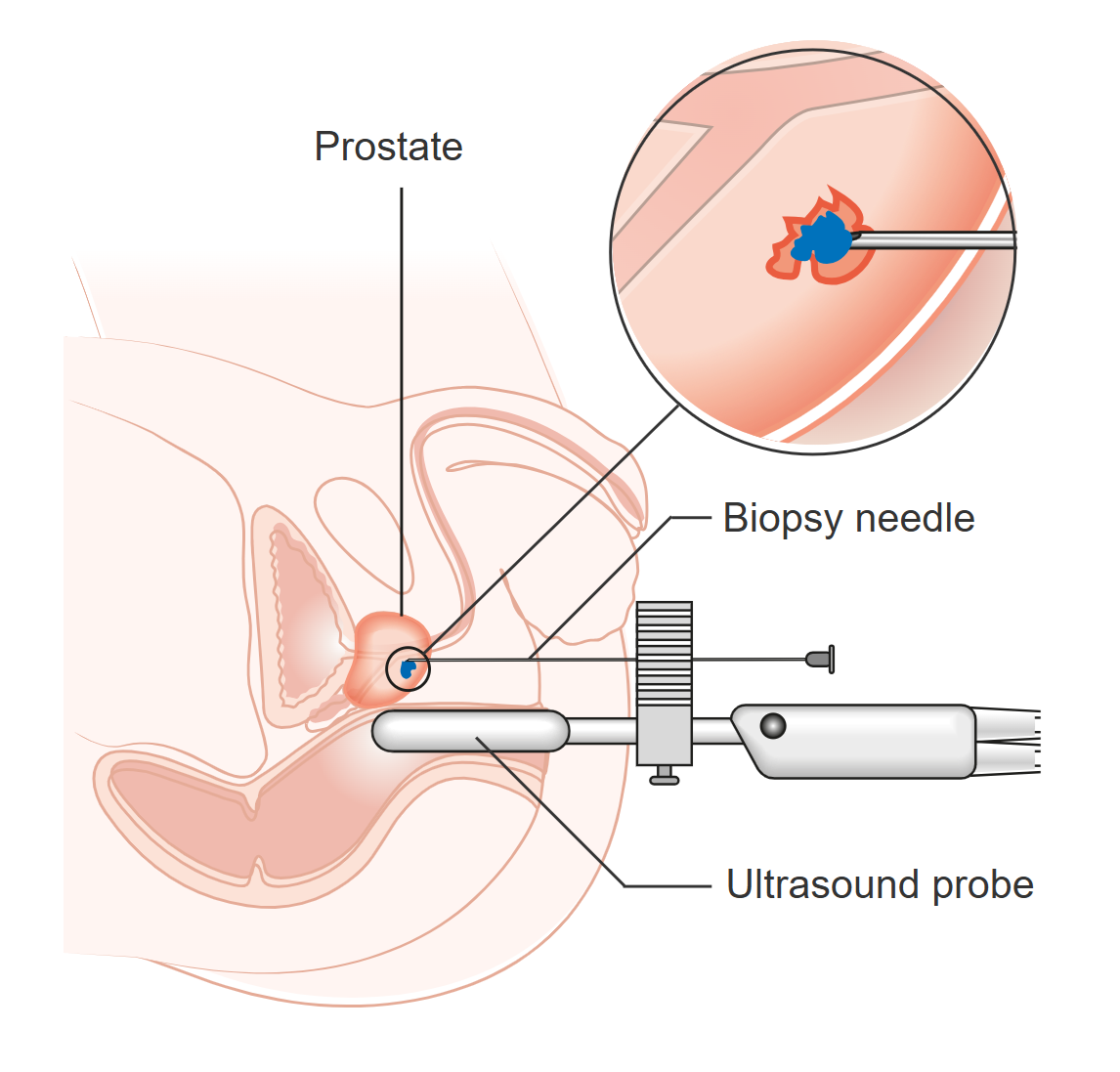
PSA is a glycoprotein protease normally produced by the epithelial cells of the prostate gland and is an important component of seminal fluid. Interestingly, PSA is not as specific as it sounds, in that other tissues also produce this protein and it is found at low levels in biological females as well. In all people, small amounts of PSA enter the blood stream and the amount of PSA in the blood is indicative of the size of the prostate gland. PSA tests are generally more sensitive than DRE and are highly recommended due to their value in early detection. That being said, increases in PSA do not necessarily indicate prostate cancer, confirmational testing is required. Histological (microscopic) examination of a biopsy can confirm whether prostatic masses are cysts, benign, or malignant based on cell morphology (i.e., cellular appearance may indicate metaplasia, dysplasia, or anaplasia) and stage of undifferentiation. Typically, biopsies are guided by imaging (e.g., MRI or transrectal ultrasonography)
Biopsies of the prostate gland and nearby lymph nodes, if positive for prostatic cancer, are frequently followed up with imaging (e.g., CT scans, MRI, bone scans, transrectal ultrasonography) to determine the location and extent of any spread (metastasis). Two strategies for biopsy collection are TRUS and Transperineal as shown in the figures below.
Prostate Cancer – Treatment
Treatments options for prostate cancer depend on the extent of spread and include:
- surgery (e.g., TURP, radical prostatectomy, orchiectomy),
- chemotherapy,
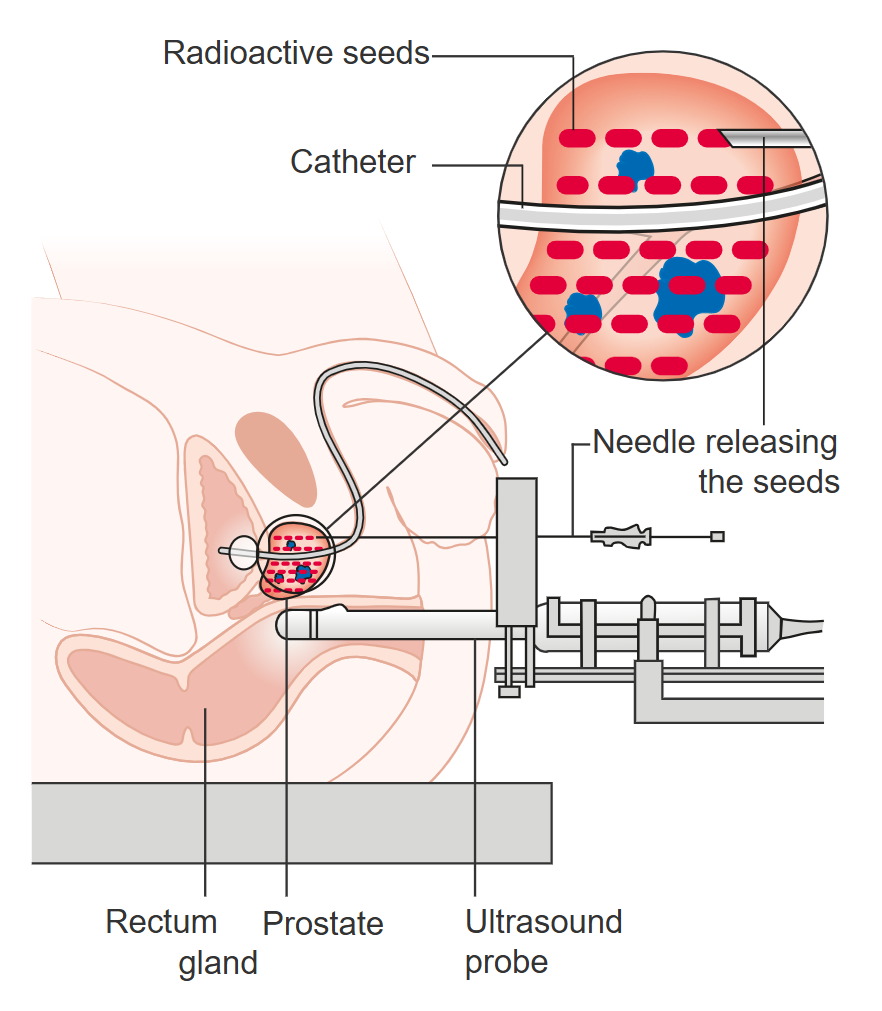
- radiation therapy (often using brachytherapy, temporary implant of radioactive seed in prostate),
- hormonal therapy (e.g., anti-androgens, androgen suppressants and orchiectomy) and
- targeted therapy (e.g., inhibitors that block PARP enzymes required by BRCA1/2 mutated cancerous cells)
- supportive treatments (e.g., support, counselling, nutrition plans, support for urinary incontinence and bowel problems).
Side Note: In addition to BRCA1, BRCA2, other genes that carry a risk of developing prostate cancer include: Hereditary Prostate Cancer 1 and 2 (HPC1 and HPC2), HOXB13, HPCX, CAPB, ATM, and FANCA.
Media Attributions
- Diagram_showing_T1-3_stages_of_prostate_cancer_CRUK_278 © Cancer Research UK is licensed under a CC BY-SA (Attribution ShareAlike) license
- Diagram showing stage T4 prostate cancer © Cancer Research UK is licensed under a CC BY-SA (Attribution ShareAlike) license
- Prostate Cancer that has spread to the Lymph Nodes © Cancer Research UK is licensed under a CC BY-SA (Attribution ShareAlike) license
- Prostate Cancer that has spread to the Bone © Cancer Research UK is licensed under a CC BY-SA (Attribution ShareAlike) license
- Diagram showing prostate cancer pressing on the urethra © Cancer Research UK is licensed under a CC BY-SA (Attribution ShareAlike) license
- Transrectal ultrasound scan (TRUS) and biopsy for prostate cancer © Cancer Research UK is licensed under a CC BY-SA (Attribution ShareAlike) license
- Transperineal biopsy for prostate cancer © Cancer Research UK is licensed under a CC BY-SA (Attribution ShareAlike) license
- Prostate Radiation © Cancer Research UK is licensed under a CC BY-SA (Attribution ShareAlike) license

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}