Chapter 4 Selected Musculoskeletal Disease and Disorders, including Trauma and Rheumatic Disorders
Acute and Chronic Exertional Compartment Syndromes, Rhabdomyolysis, Volkmann’s Contractures, and Crush Syndrome
Pictures coming soon!
Zoë Soon
Chronic Exertional Compartment Syndrome, Acute Compartment Syndrome and Crush Syndrome
In this section, 3 conditions which have many similarities, acute compartment syndrome, chronic exertional compartment syndrome and crush syndrome (crush injury), will be compared.
Both acute and chronic exertional compartment syndromes, can develop anywhere in the body in which a fascial compartment is present. It occurs when severe inflammation within the compartment becomes detrimental to the muscle, nerves, and vasculature within that compartment.
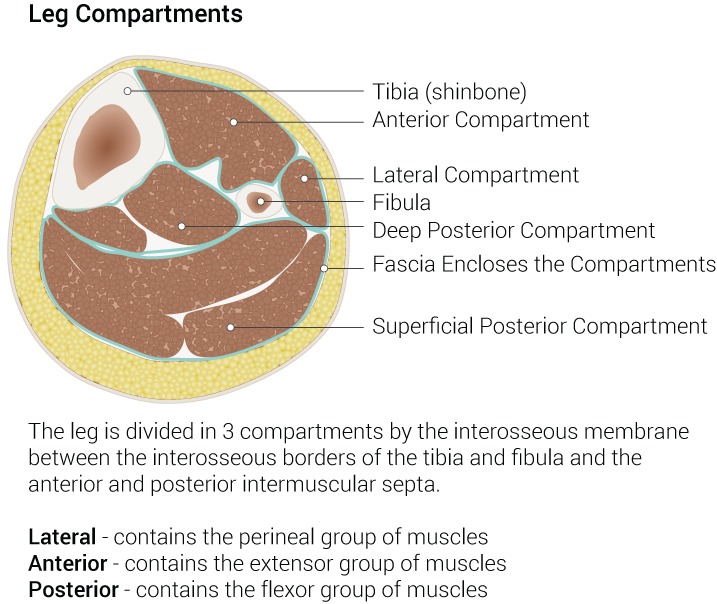
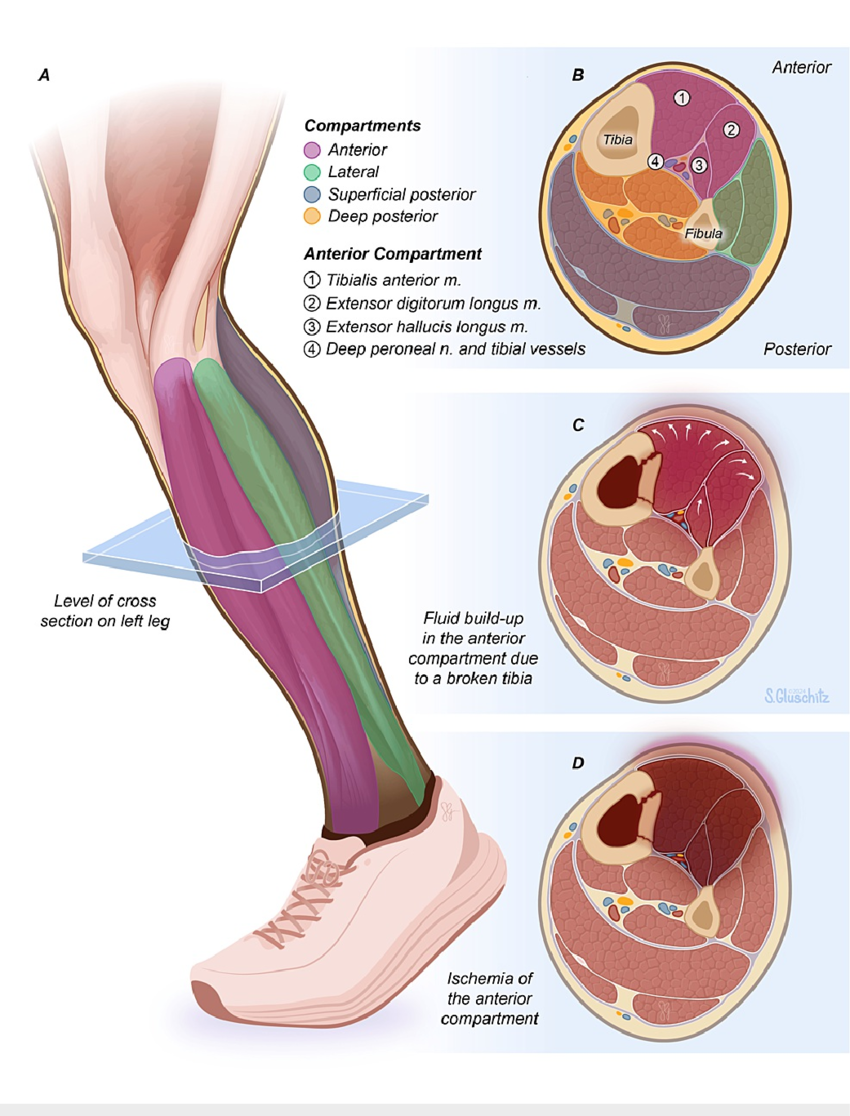
A fascial compartment contains skeletal muscles, nerves, and blood and lymphatic vessels, and is surrounded by a layer of deep fascia, which is non-elastic, dense irregular connective tissue. There are 4 fascial compartments of the lower leg (anterior, lateral, deep posterior, and superficial posterior) and 3 fascial compartments of the thigh (anterior, medial and posterior). There are 2 fascial compartments of the forearm (anterior and posterior) and 2 fascial compartments of the upper arm (anterior and posterior). The hands and wrists contain 10 and 6 fascial compartments respectively. Compartments also exist in the buttocks, abdomen, and feet.
Crush syndrome also can affect fascial compartments, though is specifically depicted by the severe damage of skeletal muscle tissue that occurs, most often as a result of a crushing injury. The ensuing significant death of skeletal myofibers (rhabdomyolysis) puts one at risk for renal failure, cardiac arrest and multi-organ failure.
Acute Compartment Syndrome (ACS)
Acute Compartment Syndrome can occur if there has been sudden and severe damage that results in the inflammatory response and an increase in swelling and pressure within any of the fascial compartments. The surrounding deep fascia does not expand readily and inflammation and the accumulation of inflammatory exudate results in intracompartmental pressures that exceed venous pressure, pinching off veins, and impairing venous outflow. The ischemia and hypoxia that then develops within the compartment can lead to progressive loss of function and then death of neurons and skeletal muscle cells (myofibers) if not treated.
The cells within the compartment, particularly those that rely on a constant supply of oxygen and nutrients (e.g., neurons and myofibers) become dysfunctional and die in what is termed ischemic necrosis. Not only do cells become impaired due to lack of oxygen and nutrients, but also suffer from the buildup of waste products, some of which are acidic or toxic (e.g., uric acid). Additionally, cells that revert to anaerobic cellular respiration (i.e., glycolysis) in order to produce ATP, will begin to generate a lot of lactic acid (lactate), leading to acidic conditions that further reduce the ability of cellular enzymes to function, which decreases cellular maintenance abilities. Unfortunately, problems can escalate when cells begin to die, as ruptured cells release electrolytes and other cytoplasmic contents creating a hypertonic environment that draws water to the zone from surrounding blood vessels, leading to more swelling and increases in intracompartmental pressure. It should be noted that fascial compartments that remain closed and intact, yet have sustained interior damage and/or accumulation of exudate are the most susceptible to the development of compartment syndrome. The most common cause of acute compartment syndrome is bone fractures.
Risk Factors – Acute Compartment Syndrome
Acute Compartment Syndrome risk factors include anything that causes damage that results in a significant inflammatory response and accumulating collection of either inflammatory exudate or leaked blood within a compartment. ACS arises from sudden increases in intracompartmental pressure, such that venous and capillary collapse occurs, leading to compromised arterial blood flow, ischemia and subsequent hypoxia of tissues resulting in cellular dysfunction and ischemic necrosis if not treated.
Risk factors include trauma that induces the inflammatory response within a closed compartment. Trauma can include: bone fractures, gunshot wounds, burns, snake bites, and blunt injuries or vascular defects that cause internal hemorrhaging. Events that cause skeletal muscle damage can lead to both rhabdomyolysis (skeletal muscle cell death) and ACS. These events can include: drug/alcohol abuse, vigorous exercise, seizures, muscle tears, autoimmune vasculitis, virus-induced myositis, androgen abuse coupled with muscle hypertrophy, and deep vein thrombosis. Although rare, there are iatrogenic risk factors for ACS which include tight casts or splints, intramuscular injections, chemotherapy drugs, pressurized IVs, and some reactions to minimally-invasive surgeries. Predisposing factors that increase chances of internal bleeding are also risk factors (e.g., hemophilia, anticoagulative therapy)
Signs and Symptoms – Acute Compartment Syndrome
Signs and Symptoms include the 5Ps (pain, pulselessness, pallor paresthesia and paralysis) which should be monitored when risk factors for acute compartment syndrome are present.
The 6th P of pressure could be added as monitoring the intracompartmental pressure with needle manometer and tonometer is recommended. The individual may feel “fullness” or pressure and the increased swelling may be visible in a leg or arm, especially in comparison to the unaffected leg or arm.
The 5 Ps of acute ischemia in a limb:
Severe Pain that is burning and/or aching often that seems out-of-proportion with the injury, is indicative of ACS. The pain in compartment syndrome often becomes more intense during flexion or passive stretching of the involved muscles. The pain is due to the cell death and lysis that occurs during trauma and ischemic events as released cellular components trigger nociceptors. The pain is not usually responsive to analgesics or elevation of the affected muscle.
Pulselessness: monitoring for a pulse distal to the injury is recommended and the absence of a distal pulse will be of concern and inform treatment. At the same time, capillary refill time can be assessed by pressing the soft pad of the finger or toe that is distal to the affected limb while the finger or toe is positioned at heart level. Once the finger or toe nail has turned pale, the pressure should be released and the time it takes to return to colour should be noted. Normal capillary refill times are less than 2 seconds. More than 2 seconds is cause for concern.
Pallor or paleness should be assessed as it indicates poor perfusion within the affected region as well as distal to the region. Pulse oximetry may be used to monitor perfusion.
Paresthesia can manifest as tingling, numbness, or decreased 2-point discrimination and indicates sensory nerves becoming dysfunctional and/or dying. Paresthesia (abnormal sensation)can develop into hypoesthesia (absence of sensation) if compartment syndrome continues without treatment.
Paralysis can manifest as muscle weakness and/or muscle fatigue, and indicates somatic motor nerves (or skeletal myofibers) are failing or dying. Some paralysis may be temporary and may be partially due to the pain experienced upon movement or exertion as well as muscle cell dysfunction. Paresis (partial paralysis) or muscle weakness caused by somatic motor nerve or myofiber damage can occur. Muscle infarction and myofiber death can result in permanent loss of muscle mass and muscle strength.
Pathogenesis – Acute Compartment Syndrome
Damage within a fascial compartment will induce an inflammatory response, which if severe will lead to significant vasodilation, increased vascular permeability and leakage of plasma into the interstitial tissue. The dense irregular connective tissue of the fascial compartment is not very expandable and as a result of inflammation and the build up of exudate and/or blood, the intracompartmental pressure will increase above venous pressure, leading to venous obstruction. The pinching off of veins and capillaries results in arterial obstruction, ischemia and hypoxia. Other factors that contribute to the ensuing hypoxia include the leakage of plasma fluid causing blood sludging and slow flow. The neurons and skeletal muscle cells (myofibers) are particularly sensitive to low levels of oxygen and nutrients and become dysfunctional and can die if not treated. Muscle infarction is a term used to describe ischemic necrosis of muscle tissue. Hypoxia leads to a greater level of anaerobic cellular respiration, which results in an increased production level of lactate (lactic acid). Without proper blood flow, metabolic wastes accumulate and the lowering of pH reduces enzyme function of the affected cells. As cells begin to die, ruptured cells release electrolytes and other cytoplasmic contents creating a hypertonic environment that leads to the accumulation of more fluid and increases in intracompartmental pressure. The ensuing rhabdomyolysis is a risk factor for renal failure, cardiac arrhythmias, and shock. Decompression usually requires a fasciotomy.
Diagnostic Tools – Acute Compartment Syndrome
Monitoring the 5Ps after traumatic injury (e.g., bone fracture) is important in tracking the potential development of compartment syndrome. The 5 Ps are described above in Signs and Symptoms and are as follows: Pain, Pulselessness (distal to injury), Pallor, Paresthesia, and Paralysis.
A tonometer or similar device (e.g., needle manometer), should be used to monitor compartment pressure.
Monitoring for the development of rhabdomyolysis is important as it can lead to renal failure. Blood work testing for rhabdomyolysis will reveal elevated levels of serum creatine kinase and myoglobin. Urine tests will reveal hematuria, proteinuria, myoglobinuria, and tea-coloured urine.
Renal function studies including the monitoring of blood urea nitrogen (BUN) levels is necessary in order to prevent permanent kidney damage. Hemodialysis may be required to lower levels of myoglobinemia.
Imaging: MRI and ultrasound may reveal muscle tears or other damage or abnormalities as well as the extent of fluid accumulation. Angiography may be used to assess vascular occlusions and rule out other vascular problems.
Treatment – Acute Compartment Syndrome
Treatment of the causative agent, plus decompression treatments are typically chosen.
Therefore, most often, treatment involves fasciotomy, coupled with bone fracture reduction (if necessary, for any broken bones), vascular repair and stabilization of the patient. Fasciotomy relieves the pressure in the fascial compartment and is sometimes referred to as decompression therapy.
IV fluid treatments for rhabdomyolysis and myoglobinemia, hypovolemia and acidemia may be required, in addition to hemodialysis.
Post-surgical (fasciotomy) rehabilitation with physiotherapy is recommended to minimize fibrotic shortening through the use of stretching exercises. A muscle strengthening program to regain muscular strength is also important.
Potential Complications – Acute Compartment Syndrome
Sensory problems can occur. For example: hypesthesia (loss of sensations) or dysethesia (abnormally painful responses to normal touches) can develop.
Muscle infarction can occur due to prolonged ischemia and often leads to permanent loss of muscle strength as skeletal myofibers are usually not able to fully regenerate.
Rhabdomyolysis is a risk due extensive muscle infarction and can lead to renal failure.
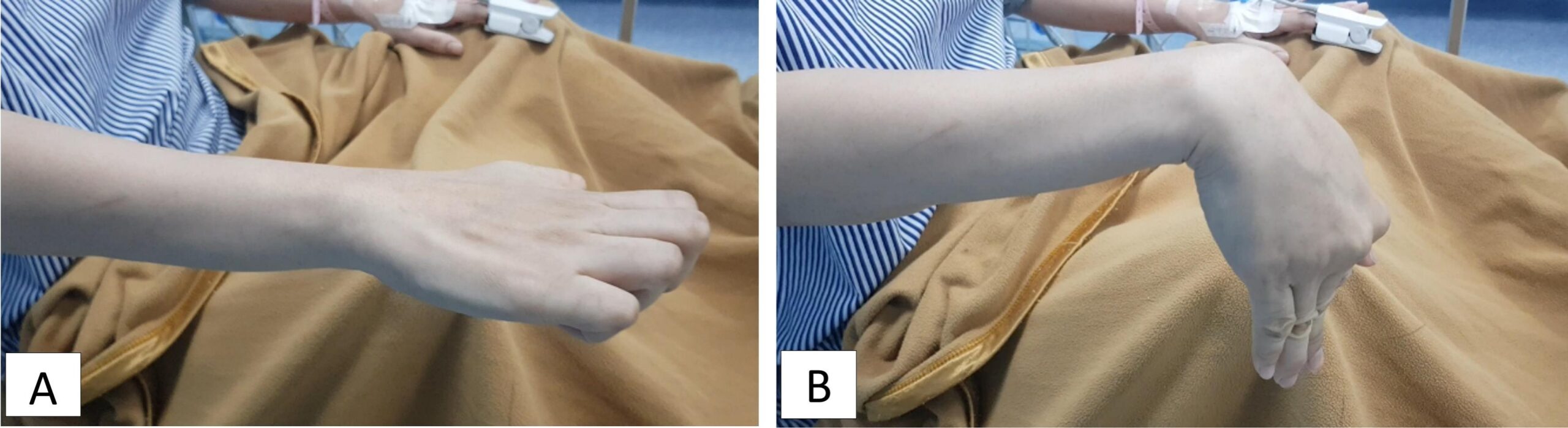
Volkmann Contractures can be caused by the fibrotic shortening of damaged muscles and their tendons as a result of ischemic necrosis. Most often this affects the flexor muscles of the forearm leading to contracture of the wrist and fingers, forming a “claw hand” with limited range of motion.
Shock due to hypotension, hypovolemia, and/or poor venous return leads to poor cardiac output and will contribute to poor perfusion of multiple organs, potentially leading to multi-organ failure.
Cardiac arrhythmias due to hyperkalemia and/or acidosis can occur and lead to either poor cardiac output and/or cardiac arrest (myocardial infarction, MI).
Disseminated Intravascular Coagulation (DIC) can occur when hyper-activation of platelets occurs due to extensive inflammatory response. An abundance of platelet activation results in the formation of clots that circulate becoming lodged in capillaries throughout the body, potentially leading to multi-organ failure. DIC can lead to even more problems as platelets are “used up”, and the individual becomes susceptible to prolonged bleeding due to the loss of clotting abilities.
ACS can lead to multi-organ failure, cardiac arrest, as well as renal failure, all of which can become fatal if treatments are not put in place.
Chronic Exertional Compartment Syndrome
Chronic Exertional Compartment Syndrome (CECS) as the name suggests, is a form of compartment syndrome that typically occurs during vigorous exercise. The exact cause (i.e., etiology) is unknown, but is thought to be due to repetitive stress, micro-damages, muscular hypertrophy and/or hypoperfusion that occurs within a fascial compartment due to exertion (e.g., vigorous exercise). The increase in intracompartmental pressure is temporary but causes transient vascular obstruction, severe pain, paresthesia, muscle tightness, muscle weakness, and/or muscle cramps. These symptoms usually are debilitating and are subdued once exercise is stopped. Although symptoms diminish during rest, it may take over 15 minutes to several hours before the symptoms disappear. The pressure on sensory and somatic motor nerves is thought to be responsible for the symptoms related to sensory (paresthesias) and motor dysfunction (muscle tightness, weakness, cramps).
Risk Factors: The most common risk factor in the development of Chronic Exertional Compartment Syndrome (CECS) is vigorous exercise. For example, running, playing soccer, and military training can be contributing factors which result in CECS that is associated with severe lower extremity pain. Weightlifting can be a risk factor for upper extremity CECS.
Signs and Symptoms: It is thought that CECS is often underdiagnosed, as the symptoms subside with rest and can also resemble other pathologies (e.g., shin splints, tibial stress fractures, nerve entrapment disorders, popliteal artery entrapment syndrome, tendon disorders, and vascular abnormalities, such as claudication). Symptoms are usually bilateral and can include a feeling of “fullness” or “crampy” pain. As mentioned earlier, symptoms during exertion can include severe pain, paresthesia, muscle tightness, muscle weakness, and/or muscle cramps. These symptoms usually cause the athlete to stop and rest, until the symptoms diminish which can take minutes to hours.
*”Shin splints” is also known as Medial Tibial Stress Syndrome (MTSS).
*Nerve entrapment is thought to occur due to repetitive strain causing constant pressure and ischemia resulting in microdamage, vascular changes, and possibly scar tissue all of which can disrupt the myelin sheath and impair nerve function. The most common example of nerve entrapment is Carpal Tunnel Syndrome.
*Popliteal artery entrapment syndrome (PAES) is a rare condition that usually occurs when an abnormal or accessory insertion of the medial head of the gastrocnemius muscle is present. PAES causes similar symptoms as CECS and other vascular obstructions, with running athletes experiencing posterior leg pain and foot paresthesia.
Diagnosis often involves physical examination, examining the muscles’ range of motion, tenderness to palpation, pain on passive stretch, as well as exercises to test provocation and gait analysis. Imaging (e.g., ultrasound, MRI, x-ray) can be used to detect any defects in the deep fascia, which can be a risk factor. Imaging is also used to rule out other causes of pain or inflammation (e.g., shin splints, tumors, deep venous thrombosis, tendon pathologies). Nerve conduction velocity tests can be used to detect and rule out nerve entrapment. Needle manometers or tonometers can be used to assess intracompartmental pressure. Measuring intracompartmental pressure before and after exercise is considered a gold standard diagnostic test.
Microdialysis is a technique that carefully extracts water-soluble compounds from a tissue’s extracellular space. In CECS, microdialysis has revealed high levels of lactate, glutamate and glycerol in the tissue’s extracellular space.
Conservative treatments can last for 3-6 months and includes ice, NSAIDs, physiotherapy exercises (e.g., stretching, gait training, and warm up routines), foot orthoses (for leg CECS), and massage.
Minimally invasive treatments have involved:
- fascial fenestration (use of small needle to poke holes in fascia),
- Extracorporeal Shockwave Therapy, ESWT (uses high-intensity acoustic waves to reduce inflammation and stimulate tissue regeneration) and
- botulinum toxin A injection (to reduce muscle contraction, which reduces intracompartmental pressure and pain).
Surgical treatment is used only when conservative treatments are not effective and include fasciotomies (open, endoscopic, or ultrasound-guided) which can involve single or multiple incisions, with minimal incisions correlating with better outcomes. Endoluminal release which has been successfully used in carpal tunnel surgery has been used. Endoluminal release uses a light-emitting plastic device with an inner small scalpel blade.
Most surgeries are successful, though complications of surgeries can occur and include nerve injury, scar formation, nerve entrapment, hematomas, and infection.
Possible Complications from CECS include muscular atrophy, permanent nerve damage and fascial fibrosis, which makes recurrent CECS more likely.
Preventative techniques involve ramping up training gradually over weeks and months, as an abrupt escalation in intensity and volume of exercise training puts one at risk for CECS. Use of supportive shoes is also recommended.
Crush Syndrome
Crush syndrome (also known as crush injury or traumatic rhabdomyolysis), as the name implies, occurs when there is a crush or compression of arms, legs or any part of the body that causes skeletal muscle damage, triggering the inflammatory response and muscle swelling.
The term rhabdomyolysis originates from the Greek words rhabdos meaning rod, myo meaning muscle and lusis meaning loosening, dissolving or dissolution. Rhabdomyolysis refers to the rapid death and lysis of skeletal (striated) muscle, releasing myoglobin proteins into the blood, which can lead to acute kidney failure. Traumatic rhabdomyolysis indicates that muscle death has been due to trauma rather than other causes. As noted above, acute compartment syndrome can also result in rhabdomyolysis.
Diagnosis of rhabdomyolysis includes physical exams, identifying the etiology of muscular damage, as well as imaging, blood tests and urine tests. Blood tests positive for high levels of serum creatine kinase are indicative of rhabdomyolysis. Urine test strips in cases of rhabdomyolysis would reveal the presence of heme in urine as well as protein. Urinalysis may also reveal urine that is dark tea coloured due to the accumulation of myoglobin, indicating myoglobinuria. Myoglobin is a heme pigment-containing protein that is similar to hemoglobin in structure, function, and colour. Within urine, heme and proteins are normally at very low levels, and increases are a sign of damage and inflammation to the renal glomeruli and/or nephrons. In cases of rhabdomyolysis, under the microscope, urine will not contain any red blood cells (RBCs), despite heme being detected by urine test strips. This indicates that the positive hematuria result is due to the presence of myoglobin rather than hemoglobin (which is located within RBCs).
Risk factors of crush syndrome include the crushing injuries that can occur when people are injured in building collapses, earthquakes, and some vehicle and workplace accidents. Crush syndrome involves trauma resulting in structural damage and ischemia to skeletal muscles and likely other soft tissues as well, depending on the accident. Ischemia can quickly lead to acidosis as cells utilize anaerobic cellular respiration to generate ATP in order to survive. Anaerobic cellular respiration (i.e., glycolysis) produces lactate (lactic acid), which when
elevated, requires the kidney to secrete the excess H+ in order to prevent a drop in blood pH below 7.35. If kidney function is impaired or unable to keep up, a condition termed acidosis (acidemia) occurs which causes cellular dysfunction throughout the body that can be fatal, particularly due to its effects particularly within the heart and brain.
Pathogenesis – Crush Syndrome
The death of skeletal muscle cells due to ischemia as well as shearing forces, results in the cellular contents of these myofibers (including cellular proteins such as myoglobin, actin, myosin, troponin, tropomyosin) spilling into the bloodstream, leading to high levels of myoglobin in the blood (i.e., myoglobinemia) as well as increased levels of serum creatine, creatine kinase, potassium and phosphate.
As with acute compartment syndrome, electrolytes (e.g., sodium, calcium) in addition to proteins from ruptured cells creates a hypertonic region. This increased osmotic pressure results in water molecules accumulating in the region, further increasing the swelling and intracompartmental pressure. If untreated, the loss of water from blood vessels (intravascular spaces) due inflammation and/or osmotic pressure (exhibited in crush injuries and acute compartment syndrome) leads to hypovolemia and hypotension. Third-spacing is a term that can be used in this instance (as well as in compartment syndromes).
*The term third-spacing taken from the notion that there are 3 main spaces in the body that hold fluid: inside cells (intracellular), inside blood vessels (intravascular) and in between cells (interstitial spaces). The term “third-spacing” is used when too much fluid moves from the plasma of blood vessels (intravascular space) into the interstitial space. This creates many serious problems: edema, hypovolemia, hypotension and reduced cardiac output (volume of blood that the heart pumps per minute).
Signs of crush syndrome involve the obvious physical trauma that has occurred. Imaging studies (e.g., x-ray, ultrasound, MRI, CT scan) can be used to document the extent of the damage and inform treatment of broken bones and soft tissue repair. In the field it may be necessary to perform amputations in order to free a person that is trapped by unmovable wreckage. Time is often of essence to ensure person’s survival, and wreckage that can not be moved in time may also lead to amputation(s).
Signs and symptoms of rhabdomyolysis include muscle pain, muscle weakness and muscle swelling, as well as blood and urine test results that indicate high serum levels of creatine kinase, myoglobin, phosphate, potassium, and dark tea-coloured urine.
Crush syndrome can be a direct result of untreated acute compartment syndrome, in which case the 5P symptoms associated with limb ischemia may be present (pain, pallor, paresthesia, paralysis, and pulselessness).
Signs of shock include confusion, nausea, anxiety, diaphoresis, vomiting, hypotension, reflex tachycardia, loss of consciousness, and coma.
Crush syndrome death can be due to hypovolemic shock and/or cardiac arrest due to hyperkalemia (increased serum potassium).
Treatment – Crush Syndrome
Treatment for crush injuries is prioritized to ensure vital organs are salvaged and protected. Structural damage to blood vessels, bones and other tissues are repaired while monitoring for signs of crush syndrome and crushing pressures.
Care most be taken. If the crushing pressure is released too suddenly, reperfusion injury can occur, which will increase the amount of damage caused. Reperfusion injry, as the name suggests is caused by a sudden influx of blood flow that leads to damaged, leaky cells taking in too much fluid and rupturing which in addition to increasing the extent of necrosis, can exacerbate the third-spacing problem. Ideally, perfusion with oxygenated blood occurs more slowly, giving cells a chance to re-establish ATP and enzyme levels allowing for recovery and repair of cells that are still intact.
With crush syndrome, myoglobinemia and kidney function need to be monitored and treated, as kidney failure can quickly develop if not treated due to the nephrotoxic effects of myoglobin accumulating within nephron tubules. Blood tests are used to assess the levels of serum creatine kinase, myoglobinemia, as well as BUN (blood urea nitrogen levels. Urine tests are used to assess for myoglobinuria. Acute tubular necrosis leads to kidney failure which can be fatal.
Crush syndrome is complicated by injuries that may involve hemorrhaging and sepsis which can also be fatal. Antibiotic treatments and blood transfusions may be utilized.
Treatment of crush syndrome often involves treatment for hypotension, hyperkalemia, abnormal heart rhythms, kidney failure, as well as for infection and other potential complications such as disseminated intravascular coagulation (DIC). Often hemodialysis and careful administration of intravenous hydration including sodium bicarbonate buffer is utilized.
Summary
- Compartment Syndrome:
- Three types: acute, chronic, crush.
- Occurs due to high pressure in muscle compartment.
- Caused by inflammation and swelling in muscle compartment.
- Leads to inadequate blood delivery to muscles.
- Can cause muscle and nerve necrosis.
- Survival: Skeletal muscle longer than nerves (4-8 hours).
- Signs/symptoms: “Five Ps” – severe Pain, Paralysis, Paresthesia, Pallor, Pulselessness.
- Diagnostic test: nail bed pinch test (refill time >2s indicates problem).
- Treatment: fasciotomy to relieve pressure.
- Neurovascular Injuries:
- Can occur during fracture or treatment.
- Pressure measurement: use of a tonometer.
- Pathophysiology:
- Diagram shows muscle compartments and fascia.
- Damage leads to local pressure, tamponade, tissue death, inflammation, edema, necrosis, nerve injury, muscle infarction.
- Complications:
- Rhabdomyolysis and myoglobinemia, kidney damage, extracellular fluid shift, low blood volume, hypotension, dysrhythmias, acidosis.
- Volkmann’s Contracture:
- Ischemic damage to flexor muscles and nerves, leading to fibrosis and contracture.
- Shock:
- Defined as inadequate blood flow to tissues.
- Signs include paleness, excessive sweating, hypotension, tachycardia, nausea/vomiting.
- Management:
- Fasciotomy, slow pressure release, bicarbonate for acidosis, dialysis for myoglobin removal.
- Diagnostic Tools:
- Passive leg stretch test for pain induction.
- Complications:
- Untreated conditions can lead to amputation.
- Treatment Example:
- Image of fasciotomy procedure.
Media Attributions
- Leg Muscle Compartments © Beckie Palmer is licensed under a CC BY (Attribution) license
- Acute-Compartment-Syndrome-of-the-Lower-Limb-Figure-1a-Healthy-lower-limb-cross-section © Hobbs, Mikayla & Rahman, Hira & Raj, Rhea & Mandalaneni, Kesava & Pemminati, Sudhakar & Gorantla, Vasavi.
- Volkman Contracture © Meirizal , Hilmi Muhammad , Muh Rifki Zidny , Muhammad Ichwan Noorrafiqi , Bernadeta Fuad Paramita Rahayu , Rahadyan Magetsari is licensed under a CC BY-NC-ND (Attribution NonCommercial NoDerivatives) license

{kind=link}