Chapter 4 Selected Musculoskeletal Disease and Disorders, including Trauma and Rheumatic Disorders
Menisci Tears
Zoë Soon
Meniscus
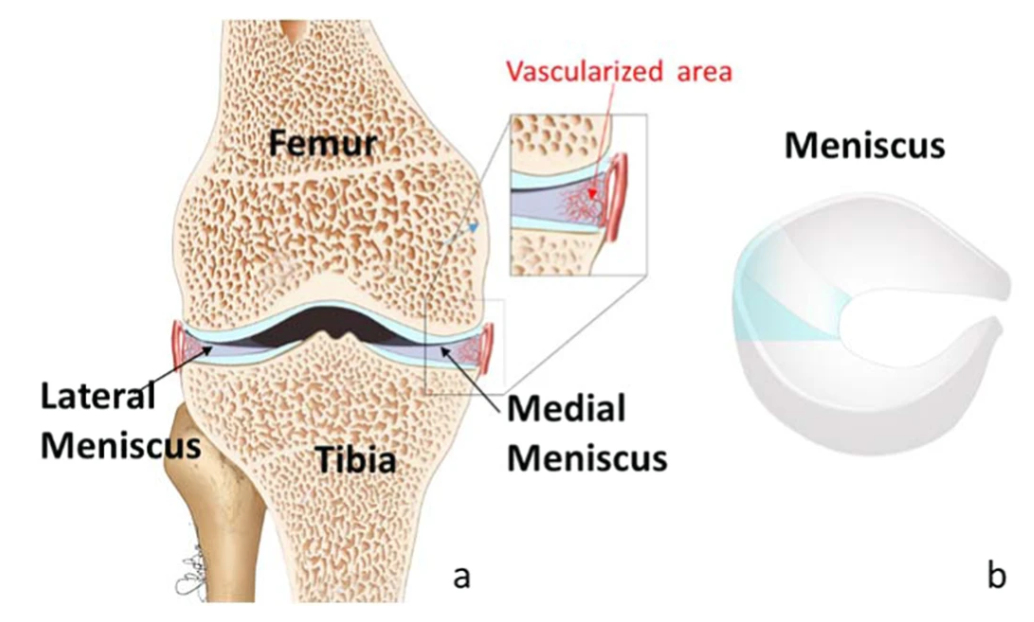
The knee joint contains two menisci (sing.: meniscus), which are crescent-shaped fibrocartilage structures composed largely of collagen, fibroblasts and chondrocytes. The collagen is arranged in longitudinal, circumferential bundles and also interwoven in radial and oblique directions to withstand force. Meniscus is derived from the Ancient Greek word miniskos meaning ‘crescent’. Menisci are also found in the wrist, acromioclavicular, sternoclavicular and temporomandibular joints and play key roles in joint stability. Each knee contains a lateral and a medial meniscus, that unlike articular discs, cover only part of the articulating bones, but similarly provide structural support. Mensci reduce friction, support load, absorb shock, guide range of motion, and provide proprioception. Menisci are wedge shaped and composed of “red” and “white” cartilage, with the red outer portion being more vascularized than the white portion and therefore more adept at healing. It has been found that vascular perfusion diminishes after the age of 40. Nerve endings within the menisci are thought to play a role in providing sensory feedback and proprioception.
Meniscus Tears
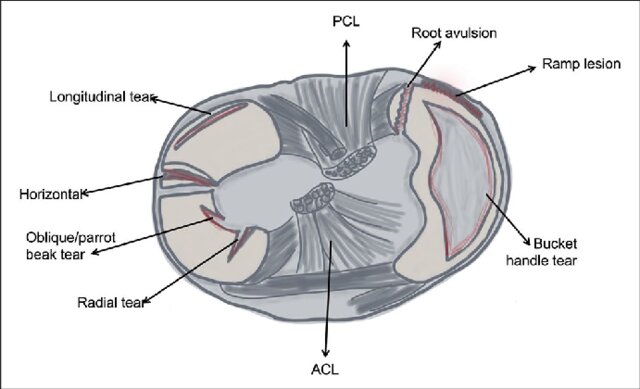
Acute meniscus tears are often due to sport injuries or trauma, whereas chronic or degenerative meniscus tears or damage occur due to prolonged wear-and-tear. Acute tears can occur during sudden twisting or squatting movements. Tears are classified based on their appearance and direction of tear, for example: longitudinal (which may take the shape of a bucket handle), radial, horizontal, oblique flap (or parrot-beak), or root tears.
Risk Factors – Meniscus Tears
Athletes involved in aggressive sports are most at risk and currently meniscal injuries occur most often in young males during sports (e.g., football, skiing, and volleyball). The second most common cause is due to degenerative damage and is observed most frequently in individuals older than 55 years old.
Risk Factors – Meniscus Tears
Athletes involved in aggressive sports are most at risk and meniscal injuries occur most often in young males during sports. The second most common cause is due to degenerative damage and is observed most frequently in individuals older than 55 years old.
Pathogenesis – Meniscus Tears
An acute tear will become inflamed and joint effusion will develop within a few hours. Locking of the joint may occur if pieces of the meniscus impede joint movement. Tears to the red (vascularized) zone are better at healing that tears to the white (non-vascularized) zones. The extent of healing depends on the location of the tear, as well as the overall health of the individual and availability of supportive treatments.
Signs and Symptoms – Meniscus Tears
Acute meniscus tears are typically accompanied by joint pain, in addition to loss of joint stability and possibly locking (loss of range motion), and/or clicking sounds. An individual may limp and exhibit signs of joint tenderness, difficulty squatting and/or extending knee.
Diagnostic Tests – Meniscus Tears
A physical examination may be followed up by analysis of effusion using arthrocentesis. Fluid is analyzed for blood, bacteria, glucose, protein and cells. Arthrocentesis can also be used to drain excess effusion. Imaging (e.g., x-ray, arthrography, MRI) are used to assess the tear and any other damage as well as rule out fractures and arthritis. Imaging plays an important role in determining treatment options. Arthroscopy can be used during assessment and treatment.

Treatment – Meniscus Tears
The use of PRICE (Protection, Rest, Ice, Compression, and Elevation) can help alleviate swelling and pain. Anti Inflammatory medications (e.g., NSAIDs), analgesics (e.g., Tylenol) and corticosteroid injections may be recommended.
While some meniscal tears heal without intervention, most tears require surgical treatment. Surgery is performed to either prevent the tear from becoming larger, or to remove pieces that may cause locking or increase the risk of developing arthritis. Treatment depends on the location, type of tear, extent of damage, age and activity levels of the individual, and may involve meniscectomy or repair of meniscus. Treatment goals are to restore pain-free movement, enable physical activity, and prevent muscular atrophy. Physical therapy and the use of stretching and strength building exercises play an important role in rehabilitation enhancing the quality of life and return to sport.
In addition to prescribed rehabilitative and progressive exercises, therapies such as transcutaneous electrical nerve stimulation (TENS) may be used as well as massage.
Prevention – Meniscus Tears
Prevention strategies include strengthening supporting muscles, as well as wearing supportive shoes designed for the sport or activity that one is participating in. Additionally, a healthy diet and lifestyle, as well as loss of excess weight are recommended. Other preventative strategies include ramping up activity or training levels over time rather than engaging in sudden intense exercise. This can help to offset the risk of tearing a meniscus as well as other inducing microtrauma or stress damage to other tissues.
Summary:
- Meniscus tears are amongst the most common knee injury
- Meniscus is cartilage

- Cartoon illustrates red zone (well vascularized) and white zone (less blood vessels)
- Tear in white zone slower to heal due to less blood, oxygen, and nutrients
- Tear in red zone heals more quickly
- Knee cartilages function as shock absorbers and guide range of motion
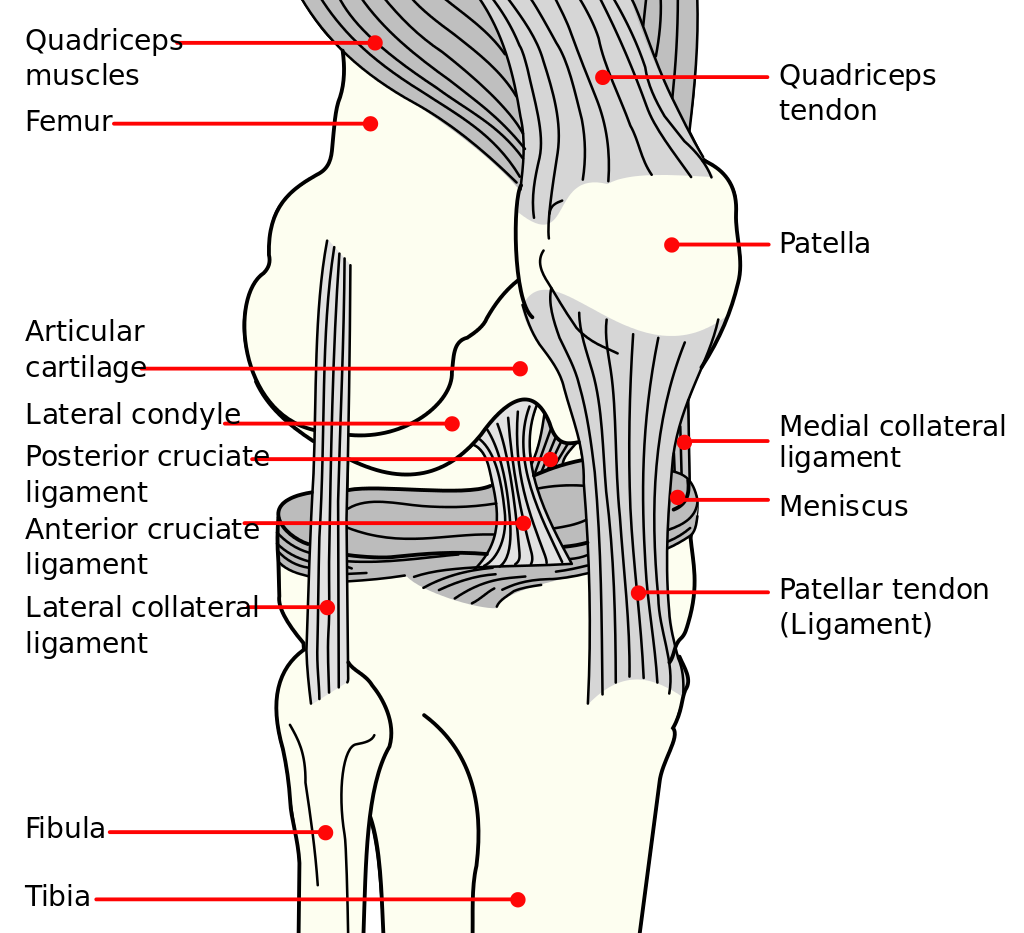
- Terrible triad: tear in MCL, ACL, and medial meniscus (common in soccer)
- Overuse injuries lead to inflammation in tendons or ligaments
- Inflammation affects nerves in affected regions
- Prevent overuse injuries: ramp up activity, proper warm-up, appropriate shoes/equipment, proper training and technique
- Pain due to micro-tears in meniscus, bleeding, inflammation
- Signs and symptoms: pain on movement
- Treatment: RICE, anti-inflammatories, physical therapy, massage, rest
- Treatment: RICE, fluid aspiration, antibiotics for infection
- PRICE (Protection, Rest, Ice, Compression, Elevation) can help manage symptoms and prevent excessive scar tissue formation.
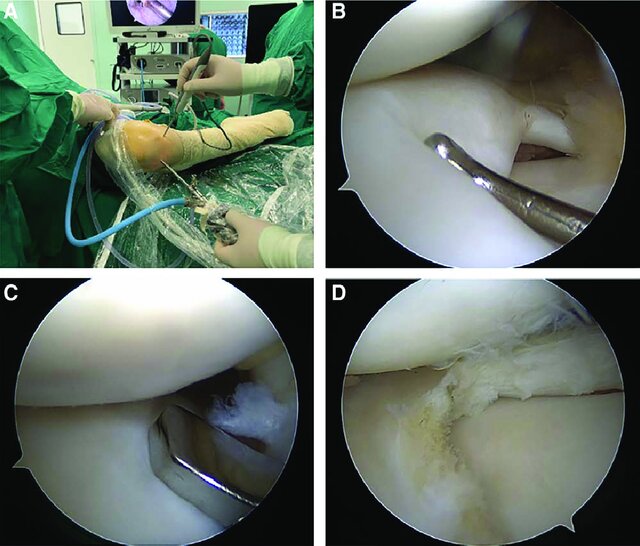
- Arthroscopy allows surgeons to view and repair joint injuries, such as ligament tears or meniscus tears.
- Viewing scope and surgical instruments for repairing damaged tissue
- Arthography: X-ray or CT scan to view joint damage
- Radio-dense dye (iodine) for X-ray, MRI contrast medium for MRI
- Prevention: proper warm-up, technique, equipment, gradual activity increase
Media Attributions
- Menisci © V. Vetri, K. Dragnevski, M. Tkaczyk, M. Zingales, G. Marchiori, N. F. Lopomo, S. Zaffagnini, A. Bondi, J. A. Kennedy, D. W. Murray & O. Barrera is licensed under a CC BY-SA (Attribution ShareAlike) license
- Representation-of-all-meniscal-tear-patterns_W640 © Ajay Asokan , Anouska Ayub, and Manoj Ramachandran is licensed under a CC BY-NC (Attribution NonCommercial) license
- Knee-MR-imaging-of-types-of-meniscal-tears-A-longitudinal-tear-The-sagittal-FS_W640 © Francisco EspinosaKarla V. Rodriguez-AlanisKarla V. Rodriguez-Alanis is licensed under a CC BY-NC-ND (Attribution NonCommercial NoDerivatives) license
- Surgical-procedures-of-arthroscopic-meniscoplasty-A-The-patients-were-placed-in-a_W640 © Zhang, Zaihang & She, Chang & Li, Liubing & Mao, Yongtao & Jin, Zhigao & Fan, Zhiying & Dong, Qirong & Zhou, Haibin & Xu, Wei. is licensed under a CC BY-NC (Attribution NonCommercial) license
- Knee © Mysid is licensed under a Public Domain license
- Meniscus_tear_types.svg © Mikael Häggström is licensed under a Public Domain license

{kind=link}