Chapter 2 Innate and Adaptive Immunity: From Cell Defense to Tissue Repair
Section 1: Host Resistance and Innate (Non-specific) Defenses
Pictures coming soon!
Zoë Soon
Section 1: Host Resistance and Innate Defenses
The human body must constantly protect itself against microorganisms capable of harming our cells. The capacity to prevent microorganisms from causing diseases is termed host resistance, categorized as either non-specific (protecting against many different foreign agents) or specific (targeting only particular antigens). This chapter focuses on non-specific innate defense, the inflammatory response, fever, and the cellular processes underlying healing.
Pathogenic Microorganisms
Most microorganisms are beneficial – decomposing organic material, forming food-web foundations, and fixing atmospheric gases (e.g., nitrogen N2 and carbon dioxide CO2) into usable forms for plants and other organisms. Microorganisms also synergistically inhabit the intestines of mammals, including humans, producing vitamins (e.g. Vitamin K and B12) which are required for enzymatic functions. Humans also benefit from industrial usage of microorganisms which are utilized in waste and sewage treatment, as well as in the fermentation and preparation of many foods and beverages (e.g. cheese, bread, yogurt, beer, wine, sauerkraut).
While most microorganisms are beneficial, certain species of each type of microorganism are pathogenic:
- Pathogenic bacteria: Unicellular prokaryotes that cause surface infections of eyes or skin, or deeper-tissue infections, often secreting toxins that cause further damage.
- Pathogenic viruses: Acellular agents that cause damage by entering human cells and replicating inside of them.
- Pathogenic fungi: Unicellular (yeast) or multicellular organisms that are capable of damaging skin (e.g. athlete’s foot), mucous membranes (e.g. oral thrush, vaginal yeast infections) or lungs (e.g. aspergillosis). Some produce lethal toxins.
- Helminths (parasitic worms): Multicellular eukaryotes that can be ingested with contaminated food or water – infesting the intestines, disrupting nutrient absorption and causing cellular damage. Can also penetrate the skin when wading in contaminated water. Range in size from microscopic to visible to the naked eye.
- Pathogenic protozoa: Unicellular eukaryotes such as Plasmodium falciparum, which is transmitted by mosquito bite and responsible for malaria.
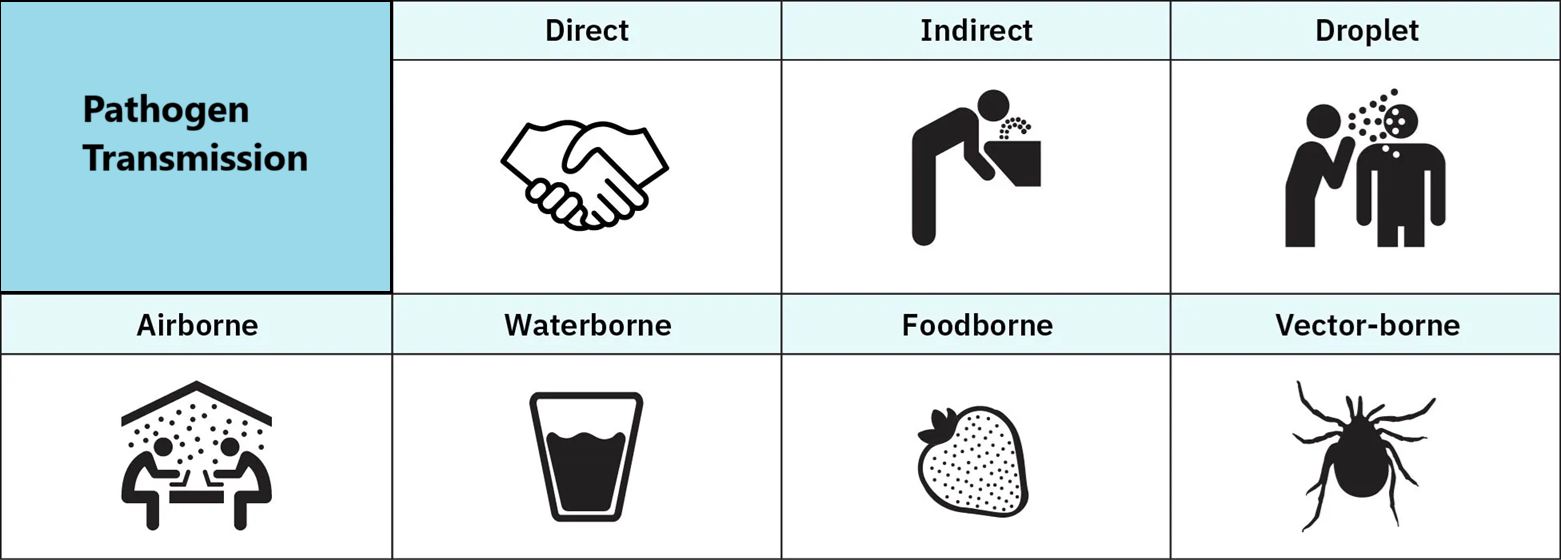
Breaking the Chain of Transmission
Preventing infections involves disrupting pathogen transmission at multiple points:
- Destroy disease reservoirs: e.g. eliminate standing water where mosquitos breed (harbouring malarial protozoa or West Nile virus).
- Proper disposal of garbage and sewage, which can harbour pathogens such as hepatitis viruses and cholera-inducing bacteria.
- Physical barriers include gloves, masks, lab coats, safety goggles, isolation rooms, and sterile equipment in health care.
- Condoms: barrier protection against sexually transmitted infections.
- Hand washing and thoroughly cooking food to prevent ingestion of pathogens.
- Wound care: proper cleaning and suturing to prevent infection.
- Vaccination, optimal nutrition, and adequate sleep reduce susceptibility to disease.
Innate (Non-Specific) Defenses: An Overview
The body’s first line of defense – called innate or non-specific defense – provides immediate, broad protection. Innate reflects that these defenses are present from birth (Latin nati for ‘birth’); non-specific reflects the wide range of pathogens covered. Categories include: physical and mechanical, biochemical, normal flora, phagocytes, complement proteins, interferons, inflammation, and fever.
Physical and Mechanical Innate Defenses
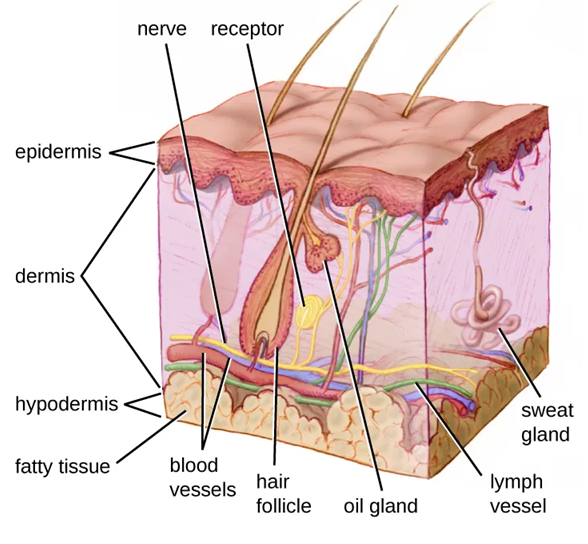
- Skin: Multiple tightly-bound, dehydrated, water-tight, keratin-filled epithelial layers resist microbial penetration. Frequent cell shedding continuously renews this layer.
- Fingernails and hair: Modified epithelial cells providing physical protection and warmth.
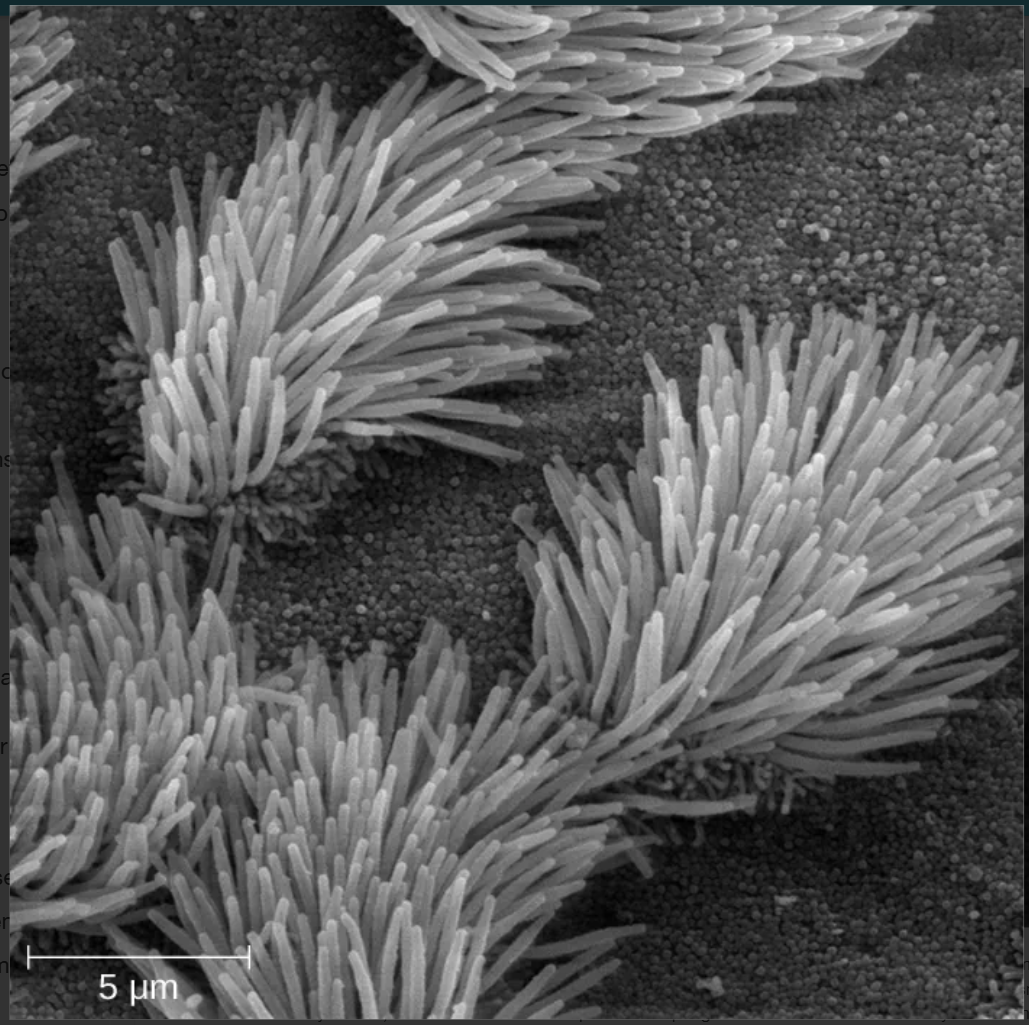
- Cilia: In the respiratory mucosa, cilia sweep mucus containing trapped pathogens toward the glottis for swallowing – a mechanism called the mucociliary escalator.
- Mucus: Produced by goblet cells lining the digestive, respiratory, urinary, and reproductive tracts. Contains sticky mucin proteins that trap debris and microbes.
- Urine flow: Flushing action through the urinary tract provides physical protection.
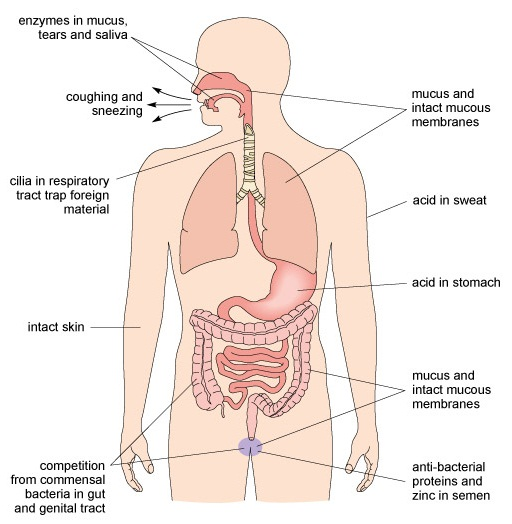

Biochemical Innate Defenses
Secretions from glands and organs create a chemically hostile environment for pathogens:
| Sebum | Bactericidal oil secrete by sebaceous glands onto the skin.
Contains lysozymes, IgA antibodies, and defensins (antimicrobial peptides that disrupt bacterial or fungal structure or metabolism) |
| Sweat | Contain water, ions, and waste products that flush microorganisms from skin surfaces and make the environment less hospitable to pathogens. |
| Tears & meibum | Tears contain lysozymes and IgA antibodies. Meibum adds oils and other protective compound. Together they protect the eye surface. |
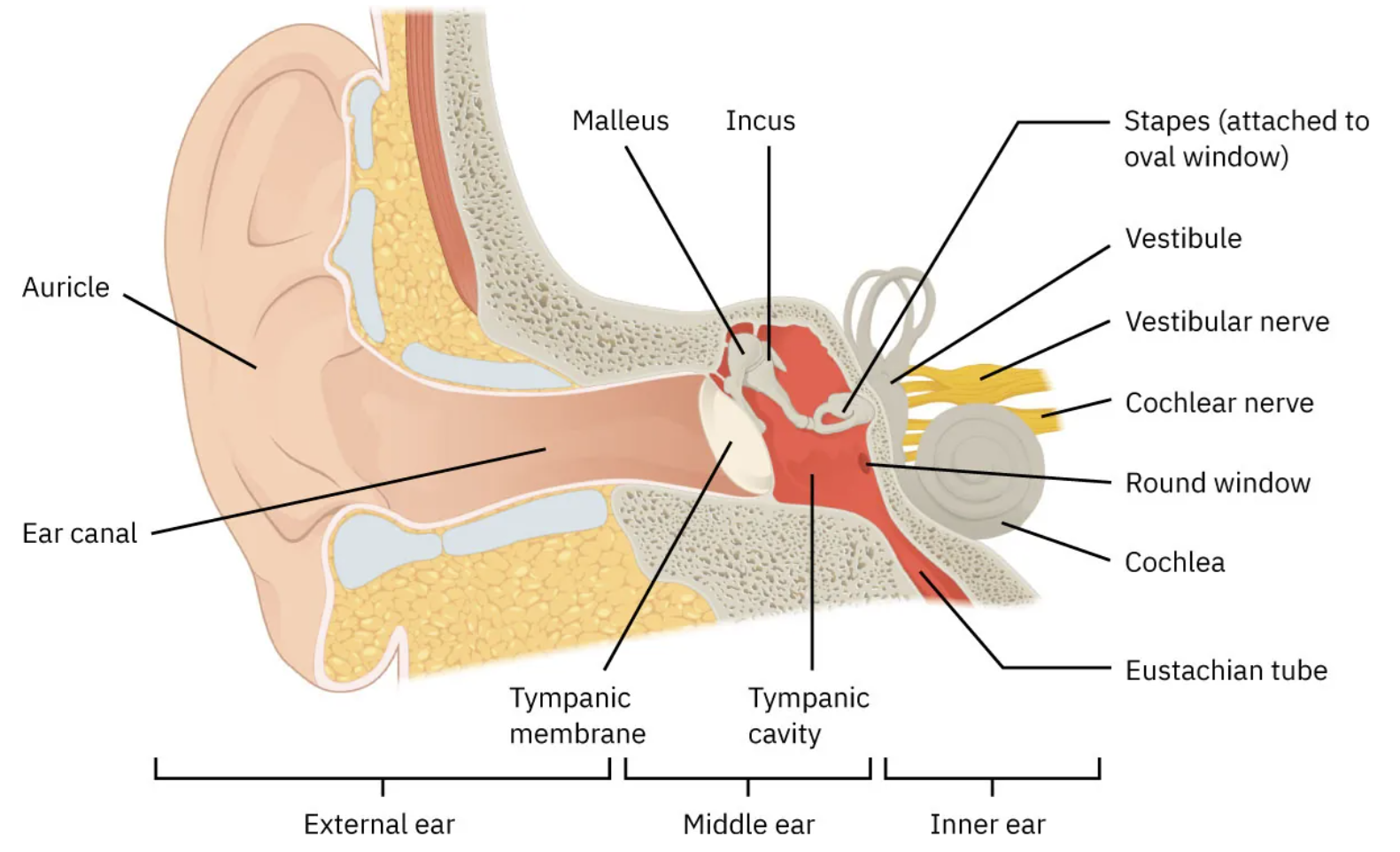
| Cerumen (ear wax) | Produced by modified sweat glands. Slightly acidic and dry with antifungal and antibacterial properties. Traps pathogens and resists outer ear infection. |
| Stomach acid | Destroys most ingested microbes; strong biochemical protection within the digestive tract. |
| Bile | Produced by the liver, stored, and secreted by the gallbladder. Alkaline; contains bile salts that are potent antimicrobial agents. |
| Vaginal secretions | Slightly acidic; contain lactoferrin (sequesters iron, depriving bacteria of a required resource) and lysozyme (cleaves bacterial cell wall components) |
| Seminal fluid | Contains antimicrobial peptides and enzymes including lactoferrin and lysozyme. Composed of secretions from epididymis, seminal vesicles, and bulbourethral and prostate glands. |
Innate Defenses: Normal Microbiota
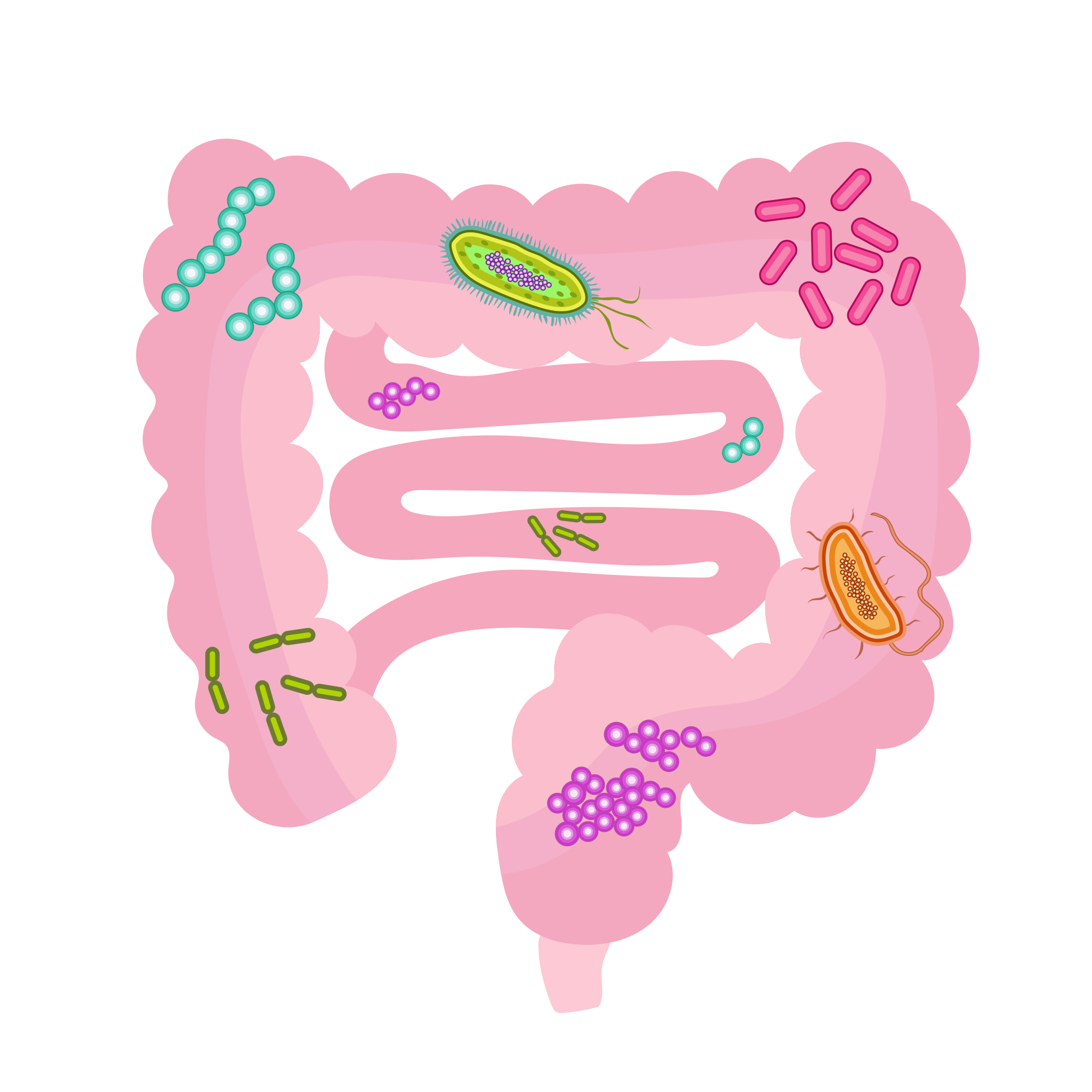
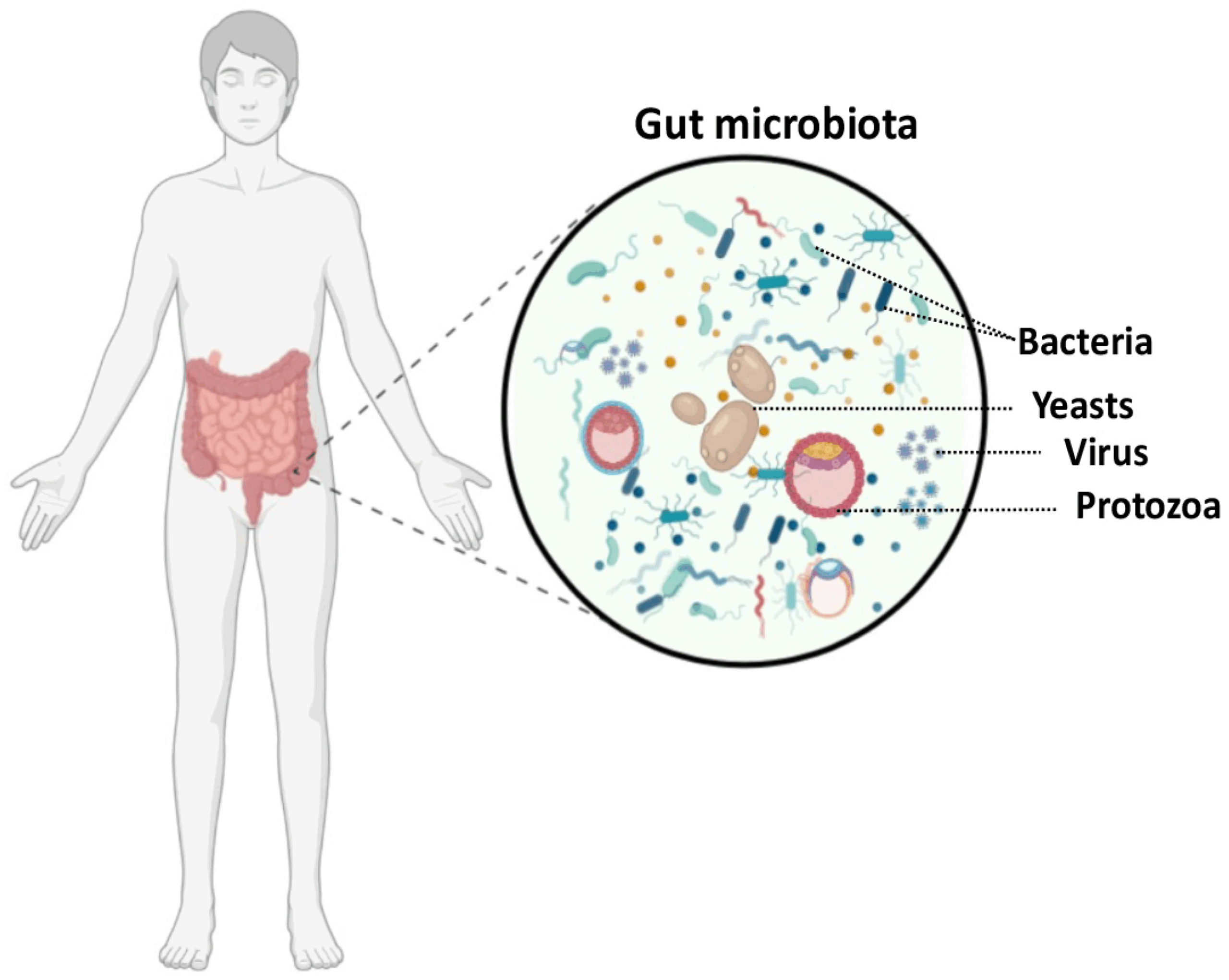
The human microbiome encompasses all microorganisms on the skin, eyes, hair, nails, nose, mouth, respiratory and digestive tracts, urethra, and vagina. Microbes in these regions that do not cause disease are called normal flora or normal microbiota. They vary by individual, body location, climate, and diet.
Normal microbiota are commensals – co-existing without causing harm, benefiting from dead skin cells and secretions. The relationship is often mutualistic: both host and microbe benefit. Normal microbiota protect against pathogens by both occupying surface area and secreting deterrent biochemicals. Intestinal microbes additionally help break down indigestible compounds (dietary fiber) and produce beneficial vitamins.
Think About Questions:
Why is inflammation considered a non-specific defense? What are other non-specific defenses of the human body?
Why does inflammation occur any time that there is an injury or disease?
Did you know that biologists sometimes call the digestive system an external tube that penetrates the body? Name one feature of the digestive system that prevents ingested microbes from causing an infection.
Why does taking an antacid put you more at risk for stomach infections?
Imagine you have a papercut – list the innate factors of your body that will help eliminate the bacteria that enter that cut.
On a neutrophil, define the following: pseudopod, phagosome, lysosome, granule
How does a NK cells kill bacteria?
What is properdin?
What is an interferon?
What is a respiratory burst?
Did you know that some diseases are caused by auto-antibodies? And some are caused by auto-complement proteins? https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(23)01524-6/fulltext
Inspirational Quote: Healing is an art. It takes time, it takes practice. It takes love. ~ Maza Dohta
Media Attributions
- Pathogen Transmission © Christy Bowen, Lindsay Draper, Heather Moore adapted by Zoë Soon is licensed under a CC BY (Attribution) license
- Innate Defense – Open University © Basiro Davey, Carol Midgley, Claire Rostron and Daniel Berwick is licensed under a CC BY-SA (Attribution ShareAlike) license
- cilia2 © Nina Parker, Mark Schneegurt, Anh-Hue Thi Tu, Philip Lister, Brian M. Forster is licensed under a CC BY-NC-SA (Attribution NonCommercial ShareAlike) license
- Goblet Cell Producing Mucus © Nina Parker, Mark Schneegurt, Anh-Hue Thi Tu, Philip Lister, Brian M. Forster ( Image credit micrograph: Micrograph provided by the Regents of University of Michigan Medical School © 2012) is licensed under a CC BY-NC-SA (Attribution NonCommercial ShareAlike) license
- skin © Nina Parker, Mark Schneegurt, Anh-Hue Thi Tu, Philip Lister, Brian M. Forster (Image credit: modification of work by National Institutes of Health) is licensed under a CC BY-NC-SA (Attribution NonCommercial ShareAlike) license
- ear © Christy Bowen is licensed under a CC BY-NC-SA (Attribution NonCommercial ShareAlike) license
- Private: Gut_microbiota © Wakana Sasaki is licensed under a CC BY (Attribution) license
- Gut Microbiota © Jawhara, Samir is licensed under a CC BY (Attribution) license
