Chapter 2 The Inflammatory Response, Fever, Healing, Cell Proliferation, Tissue Regeneration and Repair
Innate (Non-Specific) Defenses of the Human Body to Pathogens – Physical, Mechanical, and Biochemical
Pictures coming soon!
Zoë Soon
Inspirational Quote: Healing is an art. It takes time, it takes practice. It takes love. ~ Maza Dohta
Innate (Non-Specific) Defense
This section discusses the importance of understanding the body’s non-specific defenses including inflammation, and fever at a cellular level. Inflammation is the body’s natural response to any ailment, serving as a key aspect in various diseases and disorders. This section will not only explore the benefits of inflammation but also the potential harms of prolonged inflammation, delving into the reasons behind inflammation and fever. In the next section, the cellular processes involving specific immune responses, cell replacement and proliferation, tissue regeneration, and repair strategies that set the stage for healing will be examined. Overall, the focus of this unit is on gaining insights into these cellular mechanisms for a comprehensive understanding of various diseases and disorders.
Host Resistance
The planet is filled with living organisms, both large and small, with each life-form dependent on finding food and shelter in order to survive. The human body is therefore required to protect itself against both macro-organisms (e.g. bears) and micro-organisms that are capable of harming our cells (e.g. some types of bacteria, viruses, protozoa, helminths and fungi). Our ability to prevent micro-organisms from causing disease is often termed host resistance and can be categorized as either non-specific (mechanisms which protect against many different foreign agents) or specific (which protect against only specific foreign agents). This section will focus on microscopic agents that can harm the human body and the non-specific and specific immune responses that provide protection against these pathogens.
Pathogenic Microscopic Agents
As a reminder, micro-organisms have been found in every ecosystem and most are not harmful to humans. Instead, they provide many benefits. Micro-organisms decompose organic material, making organic compound available for living organisms within an ecosystem. Micro-organisms are the building blocks of all food webs. Some micro-organisms are capable of converting atmospheric nitrogen (N2 gas) and/or atmospheric carbon dioxide (CO2 gas) into usable forms for plants. Micro-organisms that synergistically inhabit the intestines of mammals, produce vitamins (e.g. Vitamin K and B12) which are required for enzymatic functions of that animal. Humans also benefit from industrial usage of micro-organisms which are utilized in waste and sewage treatment, as well as in the fermentation and preparation of many foods and beverages (e.g. cheese, bread, yogurt, beer, wine, sauerkraut).
Pathogenic Micro-organisms include:
Pathogenic bacteria, which are unicellular prokaryotic organisms, can cause surface infections of eyes or skin, or deeper infections (and cellular damage) if they are able to penetrate outer tissue layers. Often pathogenic bacteria secrete toxins that cause further damage.
Pathogenic viruses, are acellular and can cause damage if they are able to enter human cells and replicate.
Fungal infections, depending on the species, involve unicellular (yeast) or multicellular organisms that are capable of damaging the skin (e.g. athlete’s foot), tongue (e.g. thrush in infants), vaginal (e.g. yeast infections) or lungs (e.g. aspergillosis). Some pathogenic fungi can be deadly due to the toxins they produce.
Parasitic worms or helminths, which are multicellular eukaryotic organisms, that range in size from microscopic to visible to the naked eye. Often parasitic worms are ingested with contaminated food and infest the intestines benefiting from the nourishment and protection provided, harming the host by disrupting nutrient absorption and causing cellular damage.
Pathogenic protozoa are unicellular eukaryotic organisms cause cellular damage and illness. An example is Plasmodium falciparum which is transmitted through mosquito bite and causes malaria.
Breaking the Chain of Transmission
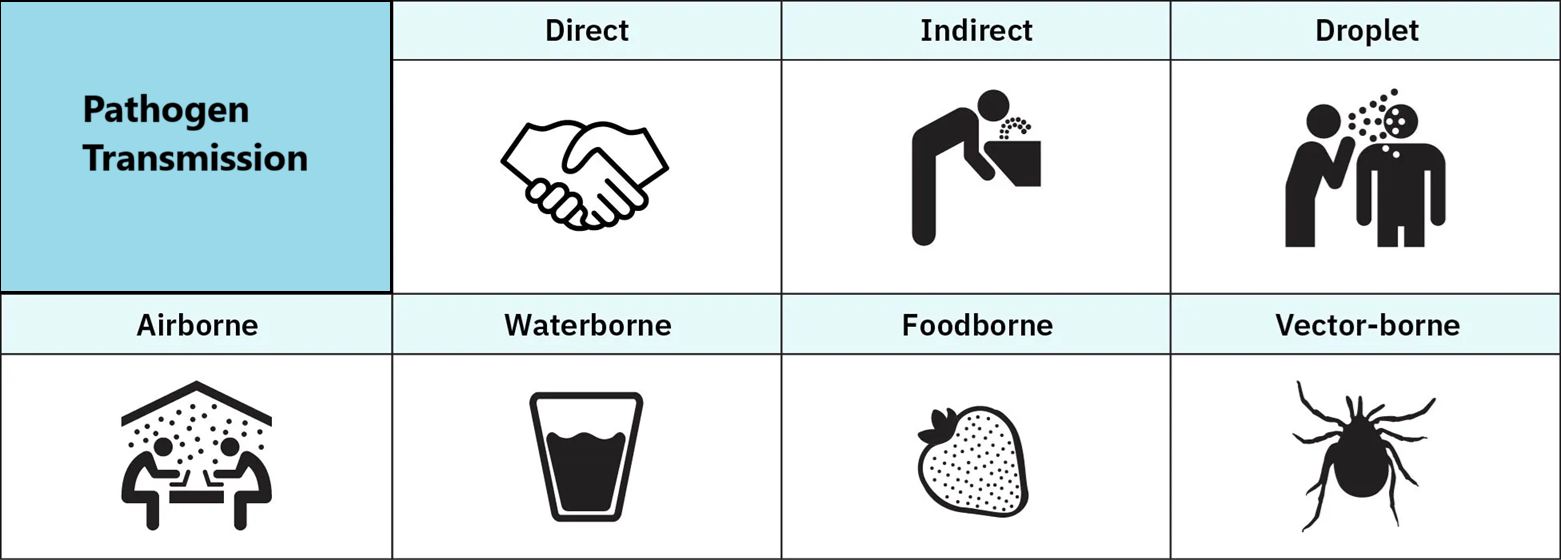
In preventing infections, often many mechanisms are put in place to reduce the chance of exposure and contact with pathogenic micro-organisms. Key measures include destroying disease reservoirs (e.g. eliminating standing water where mosquitos breed, as mosquitoes can harbour infectious agents such as malarial protozoa or West Nile virus). Proper disposal of garbage and sewage is important as it can contain harmful pathogen such hepatitis viruses and cholera-inducing bacteria. For the same reasons, physical barriers (e.g. gloves, masks, lab coats, safety goggles, isolation rooms, sterile equipment) are used in health care and community settings when directly contacting potentially infected individuals. Breaking the chain of transmission often means safeguarding potential portals of entry and exit. Condoms, another type of protective barrier can reduce the risk of sexual transmission of diseases. Respiratory infections are often spread through coughing and sneezing and the spread of airborne pathogens. Properly cleaning and suturing wounds as well as safeguarding against ingestion of pathogens through hand washing and cooking food thoroughly can reduce the chance of infectious agents entering the body. Finally, it has been found that vaccination as well as optimal nutrition and sleep reduce a person’s susceptibility to disease.
Innate (or Non-Specific) Defenses:
Even with taking part in preventative and hygienic measures, the human body routinely comes into contact with potentially harmful micro-organisms and the first line of defense, often called innate or non-specific defense, provides immediate protection. The term innate infers that humans are typically born with these abilities. The term non-specific refers to the wide-range of different pathogens that are protected against in this manner. The abilities and features of non-specific, innate defense fall into many categories: mechanical, physical, biochemical, cellular, chemical, and include inflammation and fever.
Physical and Mechanical Innate Defenses:
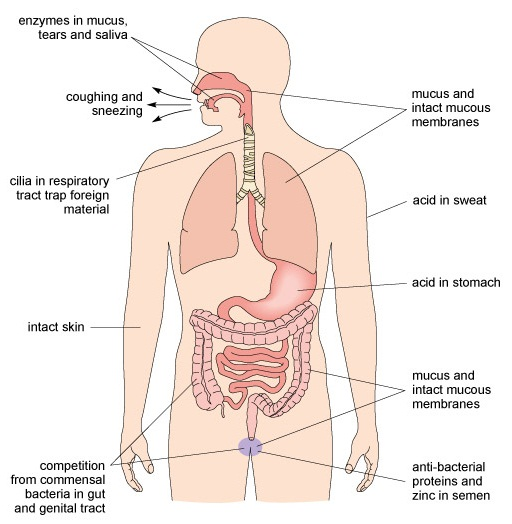
Innate (non-specific) defenses that are physical in nature include the skin which acts like a suit of armor due to its many layers of tightly-bound, dehydrated, water-tight, keratin (protein)-filled epithelial cells. This surface is able to resist microbial penetration and infection. Fingernails and hair which arise from modified epithelial cells that make up the skin, also provide physical protection and warmth. The frequent epithelial cell shedding of the skin and inner linings of the body also ensures that this layer of protection is maintained. Not only is the outer surface of the body exposed to microbes, but also the inner tubes that run through the body (e.g. digestive, respiratory and urogenital tracts). These surfaces are lined with tightly-packed epithelial cells. These cells produce secretions such as sweat, sebum, tears, mucus, cerumen, stomach acid, bile, as well as vaginal, testicular and prostatic fluids provide biochemical protection.
Biochemical Innate Defenses:
Sebum (oil) that is secreted on to the surface of skin by sebaceous glands, contain bactericidal chemical (e.g. antibacterial peptides called defensins), lysozymes, and antibodies that act to limit the growth of harmful microbes on the surface of the skin. Likewise sweat secreted from eccrine sweat glands in the skin contains water, ions, and waste products which protect the surface of the skin, by making it less hospitable as well as by flushing away micro-organisms. Constant tear and meibum production by lacrimal and Meibomian glands is important in protecting the surface of the eye from infection. Tears contain lysozymes and IgA antibodies, while meibum adds oils and other compounds. Cerumen, or ear wax produced from modified sweat glands act similarly to mucus in trapping pathogens and help to prevent outer ear infections. Cerumen is slightly acidic and dry and contains anti-fungal and anti-bacterial chemicals making for a more inhospitable environment for some pathogens.
While the skin’s epithelial cells protect the outside of the body, the epithelial cells lining the digestive, respiratory, urinary and reproductive tracts create a physical barrier preventing microbes from penetrating the body and causing damage. This lining is often called a mucosal membrane, or mucosa, as specialized epithelial cells called goblet cells secrete mucus which is a watery substance containing sticky mucin proteins that trap debris and microbes. The flow of urine through the urinary tract provides a flushing form of physical protection. Despite the acidic nature of urine, it does contain bacteria, though most often in small quantities. The respiratory mucosa contains ciliated cells, with the cilia providing mechanical protection by sweeping mucus with trapped pathogens towards the glottis for swallowing. The acid of the stomach as well as intestinal cryptocidins provides a biochemical form of protection against microbes. The bile produced by the liver, then stored and secreted by the gallbladder into the digestive tract assists with the breakdown (or emulsification) of dietary fats. Bile is alkaline and contain bile salts which are potent anti-microbial agents. Vaginal secretions are slightly acidic and contain anti-microbial polypeptides (e.g. lactoferrin) and enzymes (e.g. lysozyme). Likewise, seminal fluid has been found to contain anti-microbial peptides and enzymes including lactoferrin and lysozyme. Lactoferrin sequesters iron, which deprives bacteria of that required resource. Lysozymes cleaves bacterial cell wall components leading lysis of bacteria.
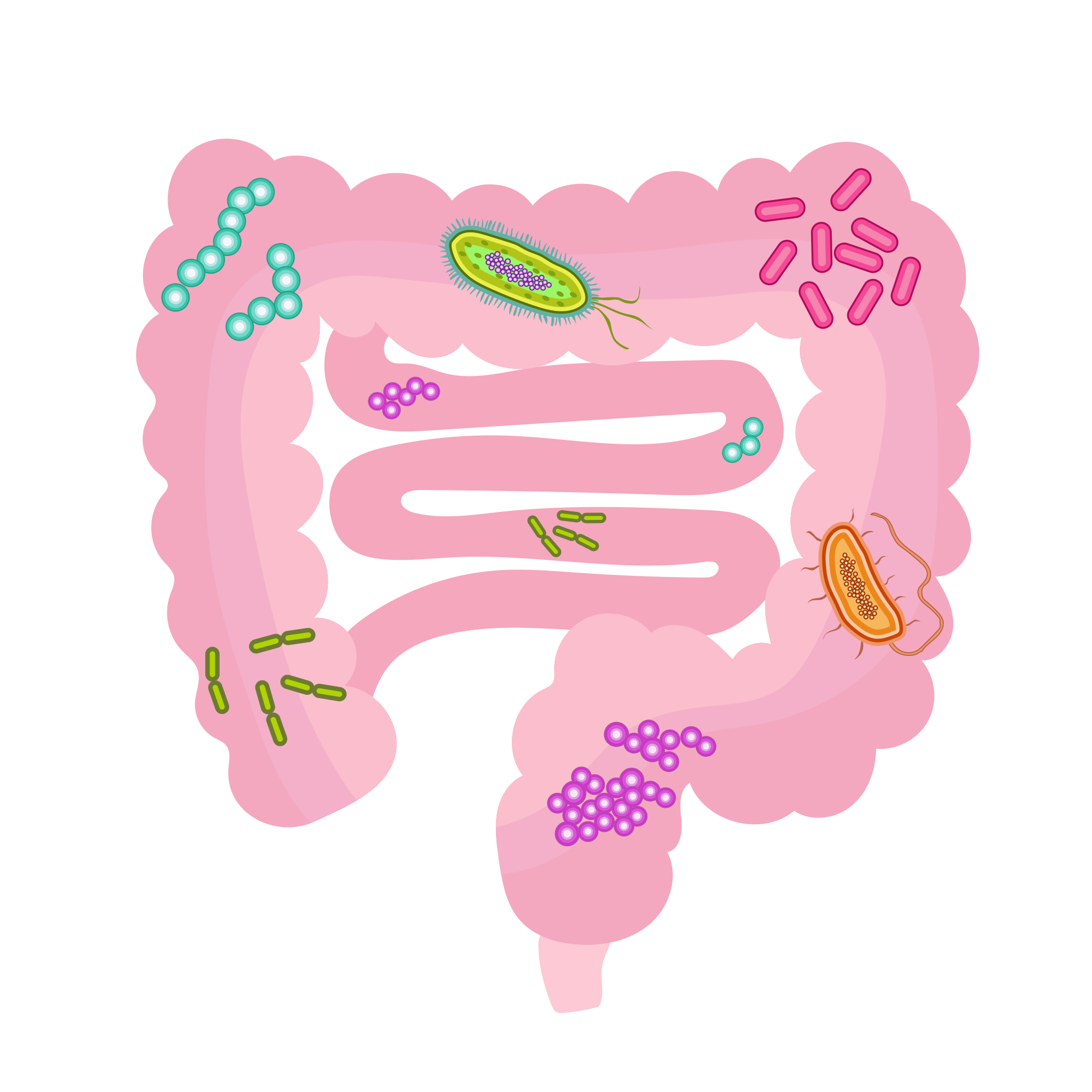
Innate Defenses: Normal Flora
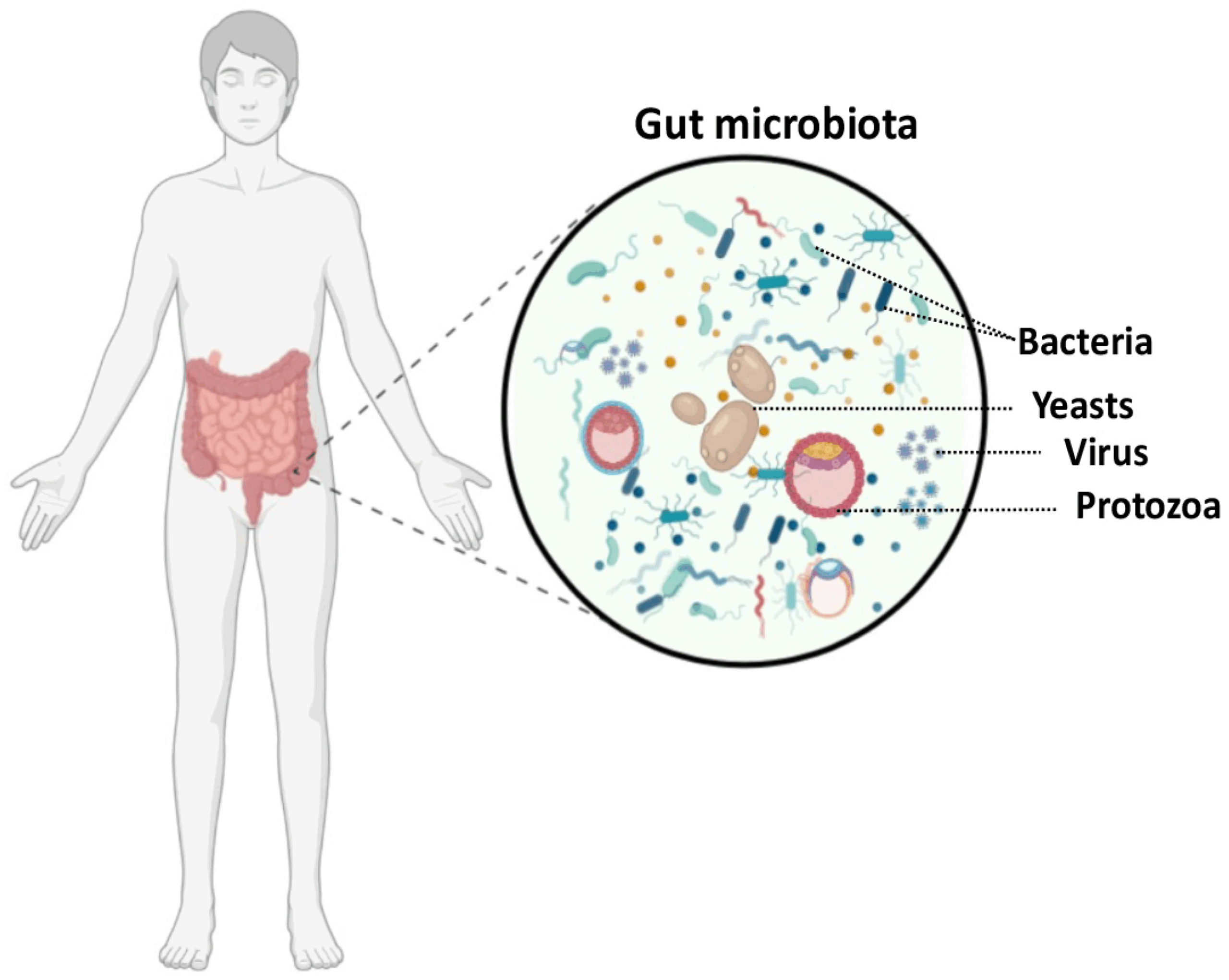
The human microbiome consists of all of the micro-organisms that occupy the surface of the skin, eyes, hair, nails, nose, mouth, respiratory and digestive tracts, urethra, and vagina. The microbes in these regions that do not cause disease are often referred to as the normal flora. These micro-organisms are diverse in nature and are a combination of different types of bacteria, viruses, and fungi. Globally, each person can be inhabited by different populations of microbes, which are affected by climate, diet, and other factors. Even within one person, the local environments affect the populations found in each region. For example, the microbiota populations found on the wrists, differs from those found in the armpits, and those found in the intestines. The normal flora microbes are considered commensals, meaning that they co-exist with their host without causing harm. Typically normal flora micro-organisms benefit from the dead skin and secreted products on the surface of our bodies as well as from some of the nutrients we ingest. The relationship between microbiota and the human host is sometimes mutualistic in that both benefit. These beneficial micro-organisms can help prevent pathogenic microbes from being able to establish themselves and cause infection to the host. They do this by both occupying surface area and at at times secreting biochemicals that deter or harm pathogenic microbes. Intestinal microbes can be helpful in breaking down some food molecules as well as producing vitamins that human hosts benefit from.
Innate Defenses: Phagocytes
In this unit, we will explore the major roles of all types of white blood cells (WBCs, also known as leukocytes). Several types of WBCs are capable of phagocytosis of bacteria and cellular debris. These phagocytes include: neutrophils, monocytes, macrophages, dendritic cells, and eosinophils. The ability to phagocytose and destroy many different types of bacteria provides non-specific defense. Phagocytes are capable of ingesting bacteria or fungal cells and lysing them using either lytic enzymes, Reactive Oxidative Species, or lytic chemicals. The typical mechanism involves the pathogen being phagocytosed in a phagosome which fuses with a lysosome that contains lytic enzymes and chemicals.
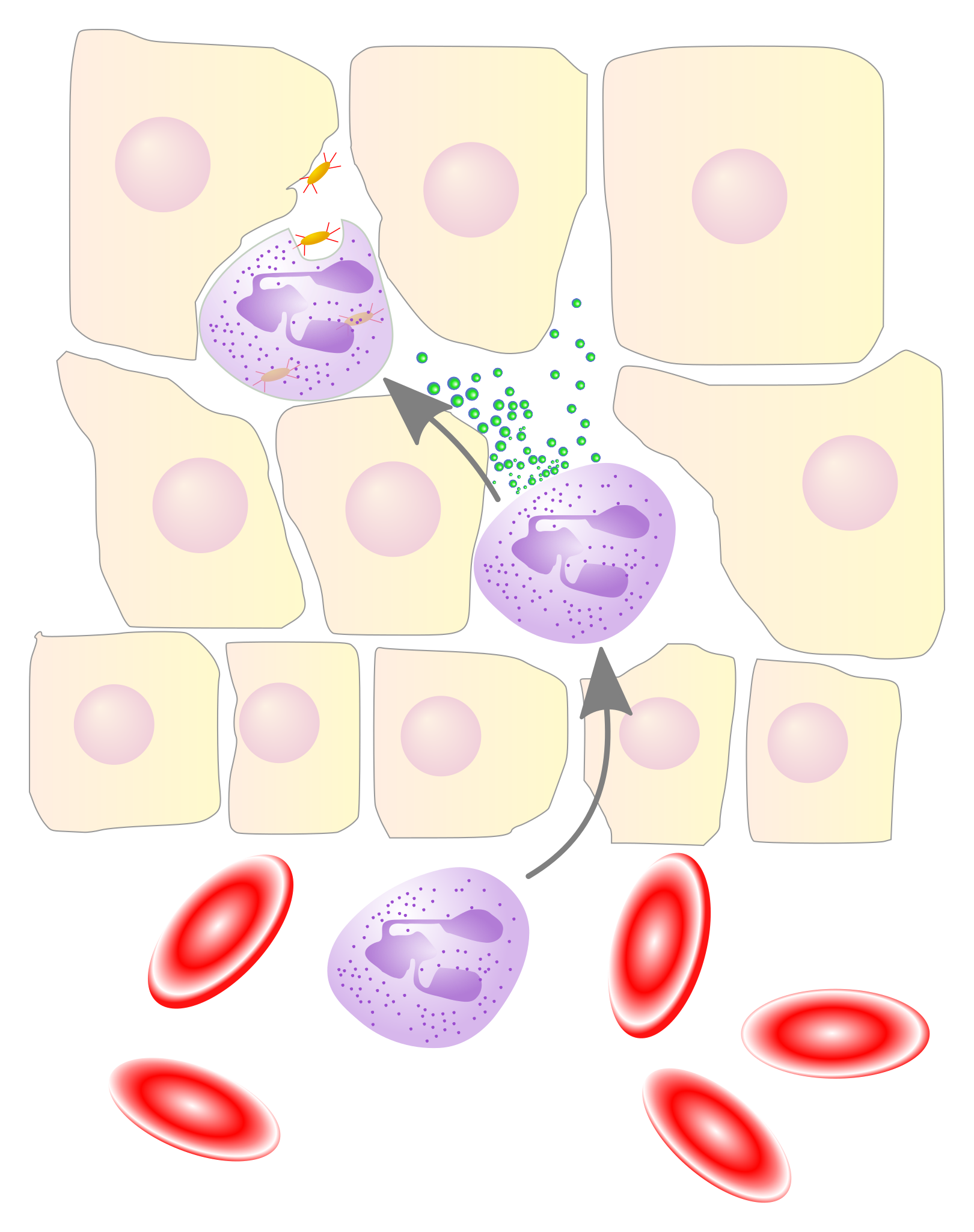
Neutrophils are produced by hemopoietic stem cells in the bone marrow and are the most abundant WBC, making up 70% of the population. Neutrophils circulate the blood stream and often the first to arrive in response to cellular damage. Inactive neutrophils live for 5 hours to 5 days, and activated neutrophils are capable of diapedesis, utilizing chemotaxis and amoeboid movement to consuming 200 bacteria and surviving for 1-2 days. At times neutrophils degranulate releasing toxic chemicals or NETs (Neutrophil Extracellular Traps composed of chromatin fibers and proteases) to destroy microbes in an extracellular fashion. Neutrophils are capable of ingesting 100-200 bacteria and releasing over 50 different toxins.

Monocytes are immature macrophages that once produced by hemopoietic cells within the bone marrow circulate the blood and mature into either fixed macrophages, free macrophages, or dendritic cells within 1-3 days. Despite being immature, monocytes are capable of phagocytosing bacteria as well as secreting cytokines, and functioning as Antigen Presenting Cells (APCs). Macrophages and dendritic cells contain large numbers of cytokines that are capable of inducing inflammation as well as recruiting immune cells (e.g. lymphocytes). Fixed macrophages are phagocytes that have exited the blood stream and utilize amoeboid movement to patrol tissue beds for cellular debris, cancerous cells, and pathogens. Several tissue-specific name have been given to fixed macrophages. For example, fixed macrophages within the brain are termed microglia. Alveolar macrophages in the lungs are sometimes termed dust cells. Macrophages in the liver are also known as stellate macrophages (or Kupffer cells). Macrophages in the vertebrae are referred to as histiocytes and macrophage in the skin are historically called Langerhan cells. Free macrophages circulate the blood stream, exiting through diapedesis (also known as extravasation, emigration, and transmigration) enter tissue beds to assist with the removal of bacteria, cellular debris, aged and dying neutrophils. Dendritic cells travel the blood stream and are located in tissues that are exposed to microbes (e.g. the skin and mucosa) and migrate to lymph nodes once activated in order to function as Antigen Presenting Cells (APCs) in the stimulation of T and B lymphocytes.
Eosinophils are another type of WBC capable of phagocytosis. Additionally they play roles in allergies adn asthma as well as in the destruction of helminths (parasitic worms). Eosinophils contain toxin-filled granules that can be released to kill pathogens. Toxins include Reactive Oxidative Species (ROS) as well as cationic (major basic) proteins, elastase (proteolytic) enzymes. Eosinophils circulate the blood stream and contain RNases to destroy viruses. Eosinophils can also release cytokines that regulate the immune system (eg. induce inflammation and activate immune cells). To assist in the healing process, eosinophils release growth factors (e.g. VEGF, vascular endothelial growth factor).
Steps of Phagocytosis:
- Activation – A phagocyte (e.g. neutrophil, monocyte, macrophage, dendritic cell, eosinophil) is activated by pro-inflammatory cytokines. Activated phagocytes can recognize and adhere to cellular debris and foreign material, such as microbes and produce toxins such as anti-microbial oxidants (Reactive Oxidative Species, ROS).
- Chemotaxis – Activated phagocytes follow chemokine trails and increasing concentration levels to the site of infection or injury.
- Recognition and Adherence – A phagocyte may not be able to bind to a bacterium, if it has a slime capsule or surface proteins. Opsonins (e.g. antibodies, lectin, complement proteins) that have bound to the bacterium facilitate phagocyte adherence to the bacterium.
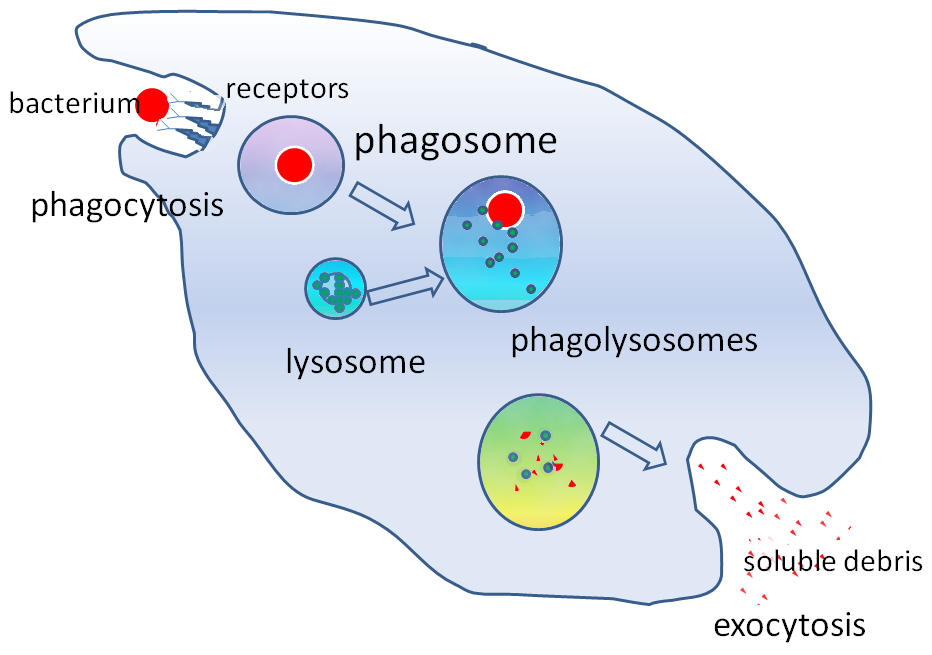
- Ingestion: Once attached, the phagocyte extends plasma membrane extensions (pseudopods) to surround the bacterium. When these pseudopods encircle the bacterium and meet, they form a vesicle called a phagosome around the bacterium which enables phagocytosis (a form of endocytosis).
- Killing and Recycling – Within the phagocyte, the phagosome fuses with a lysosome to create a phagolysosome. The lysosome’s lytic enzymes kill the bacterium and the bacterial components are digested into smaller components in order to be recycled, displayed, or expelled.
- Antigen Display – Within the phagocyte’s endoplasmic reticulum, bacterial antigens are coupled to major histocompatibility complexes (MHC) and sent to the plasma membrane to be displayed on the surface of the phagocyte in order to stimulate recruitment and activation of the immune system cells (T cells and B cells).
- Expulsion – The remaining undigested parts of the bacterium are in the phagolysosome, which fuses with the cell membrane to expel these undigestible parts as waste.
Innate Defenses: Natural Killer Cells
Natural Killer (NK) cells are another type of WBC, specifically a lymphocyte which provides non-specific defense using different mechanisms than phagocytosis. All three types of lymphocytes (NK cells, T cells and B cells) arise from hemopoietic cells in the bone marrow. NK cells make up 5-20% of lymphocytes and circulate the bloodstream. NK cells are termed cytotoxic as they are able to kill other cells. Specifically, NK cells are able to recognize and destroy most damaged cells, abnormal cells, cancerous cells, virally- or bacterially-infected cells and extracellular pathogenic cells (bacteria, fungi, and protozoa). NK cells contain small granules of perforin and granzymes (protease proteins) that can be degranulated (exocytosed) when in close proximity to abnormal/damaged/cancerous/infected cells or pathogens. NK cells are able to release perforin proteins that form portals in the targeted cells, allowing granzymes to enter and either induce apoptosis or allow the targeted cell to swell with water and lyse. NK cells are strategic, inducing apoptosis of virally-infected cells rather than lysing these cells in order to prevent any newly formed virions from being released, which could result in the infection of surrounding host cells. NK cells can release alpha-defensins as well which target bacterial cell walls for destruction. In the presence of infected or cancerous cells, NK cells release pro-inflammatory cytokines that aid in the activation of other WBCs (e.g. macrophages and neutrophils). In addition to providing innate defense, both NK cells and macrophages are responsible for recycling senescent cells (cells that have stopped replicating and are at risk of DNA damage often due to age).
*Note: Defensins are a large family of anti-microbial peptides that disrupt bacterial or fungal structure or metabolism.
**Note: Cancerous cells or pathogens that evade the NK cells can spread through tissue, blood or lymph to potentially create damage in multiple locations in the body.
Innate Defenses: Complement System
The complement system is comprised of over 30 complement proteins produced by the liver, that circulate the blood. The complement proteins become active during infections and play a crucial role in the immune response. There are three complement pathways: Classical, Lectin, and Alternative.
The Classical Pathway is triggered by the presence of antibodies that have formed complexes with antigens on the surface of a pathogen (e.g. bacterial cell walls). This stimulates a cascade of complement protein activation, including C1, C2, C3, etc. Initially, C1 must bind to two antibodies to start the cascade. In each case of complement protein activation (Classical, Lectin and Alternative), there are 3 common outcomes. Firstly, C3b attaches to the bacterial cell wall and acts as an opsonin, enhancing phagocytosis. Secondly, the C3b proteins stimulate the formation of C5-9 into Membrane Attack Complexes (MAC), which create portals or pores in the bacterial cell leading to the entrance of water, cellular swelling and eventual rupture. Thirdly, the activation complement proteins attract white blood cells for further defense and induce mast cells and basophils to release pro-inflammatory cytokines (e.g. histamine).
The Lectin Pathway utilizes Mannose-Binding Lectin (MBL), which is a protein produced by the liver that circulates the bloodstream. The Lectin Pathway is initiated by MBL binding to pathogen surfaces that contain mannose. Mannose is a sticky sugar (carbohydrate) used by some bacteria as part of their slimy capsule for adhesion. Mannose is also present on the surface of other pathogens: yeast, viruses, and protozoa. Once MBL is bound to the pathogen’s surface, a similar cascade of complement protein activation occurs, leading to C3b attachment to the pathogen cell wall or membrane. This results in functions similar to the Classical Pathway: opsonization, enhancing phagocytosis, inducing MAC pore formation, and promotion inflammation and recruitment of WBCs.
*Some examples of pathogens that have been shown to be bound by MBL are: bacteria (e.g. Salmonella and Streptococci), yeast (e.g. Candida albicans which causes oral thrush and vaginal yeast infections), viruses (e.g. HIV, SARS CoV-2, and influenza A), and protozoa (Leishmania, spread by sand flies).
The Alternative Pathway is independent of antibodies and lectin. The complement proteins upon recognizing the presence of a pathogen (e.g. bacteria, protozoa, fungi, or virally-infected cells) initiate the cascade themselves. Various proteins such as Properdin, Factor B, and Factor D contribute to complement activation and binding to the pathogen. In a similar manner to the Classical and Lectin Pathways, C3b attachment results in opsonization, enhancing phagocytosis, inducing MAC pore formation, and promotion inflammation and recruitment of WBCs.
Innate Defenses: Interferons
Interferons (IFNs) are a type of cytokines (signalling glycoproteins). Interferons are released by almost all cell types during any type of infection (viral, bacterial, fungal, protozoa). The name interferon is derived from their main function of interfering with viral replication. There are over 20 different IFN genes. Some IFNs act as anti-viral proteins (AVPs) blocking viral replication. Some IFNs act as endogenous pyrogens (inducing fever). The presence of interferons can also cause muscle pain, body aches, and flu-like symptoms. Type I interferons are produced by virally-infected cells and stimulate the expression of anti-viral proteins (AVPs) in neighbouring cells that will inhibit the viral replication of its RNA/DNA. During an infection, alpha IFNs activate NK cells and macrophages, Gamma-interferons are released by NK cells, cytotoxic T cells (CD8 T lymphocytes) and helper T cells (CD4 T lymphocytes) and stimulate macrophage activity. Beta-interferons are produced by fibroblasts and are considered anti-inflammatory and are released in preparation for healing.
Cytokines: are a family of signalling glycoproteins that are produced by macrophages, B cells, T cells, mast cells, fibroblasts, endothelial cells, and stromal (connective tissue) cells. Some cytokines have a role in innate (non-specific defense) and some cytokines have a role in specifc defense and immune responses. There are four categories of cytokines that this unit will discuss.
- Interferons: as mentioned in the previous section, these cytokines have many subtypes and fulfill various roles. Interferons can be secreted by host cells, infected cells, NK cells, T cells, and fibroblasts. Interferons are released by cells in response to pathogens (viruses, bacteria, protozoa, fungi) and tumors. There are Type I, Type II, Type II interferons, and within the Type 1 category, there are alpha, beta and gamma interferons. The main roles of interferons are to interfere with viral replication, activate NK cell and macrophages during infection, act as endogenous pyrogens and slow down inflammation after infection in preparation for healing.
- Chemokines: are responsible for inducing chemotaxis and recruitment of WBCs.
- Lymphokines: are produced by T lymphocytes (T cells) to: a) attract macrophages and b) stimulate B lymphocytes (B cells)
- Interleukins: as the name suggested are cytokines produced by leukocytes for signaling and activating each other. Specifically interleukins are produced by Helper T cells to: a) activate macrophages and stimulate fever (act as endogenous pyrogens); b) stimulate T & B cell differentiation; c) stimulate hemopoietic cells to proliferate producing more WBCs.
Innate Defenses: Inflammation
Inflammation is a protective response that is stimulated by any type of irritant or damage to cells. Possible causes of cellular damage or irritation include: cuts, blunt trauma, burns, infections, sprains, chemicals, ischemia, excess heat or cold, and foreign objects (e.g. thorns). Inflammation is an important innate response as it facilitates the removal of harmful irritants and pathogens and sets the stage for healing.
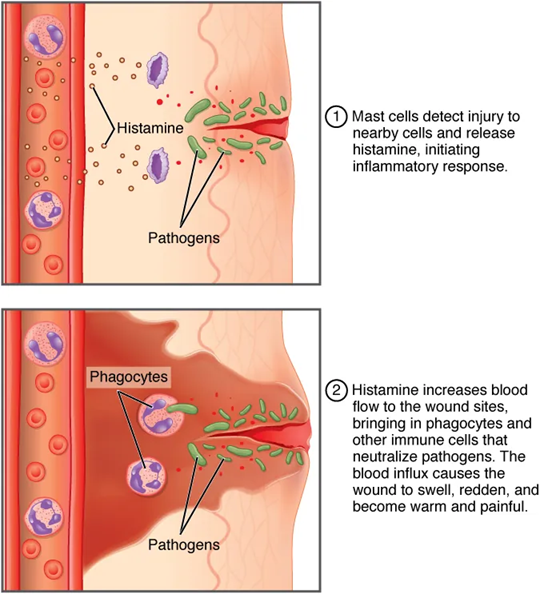
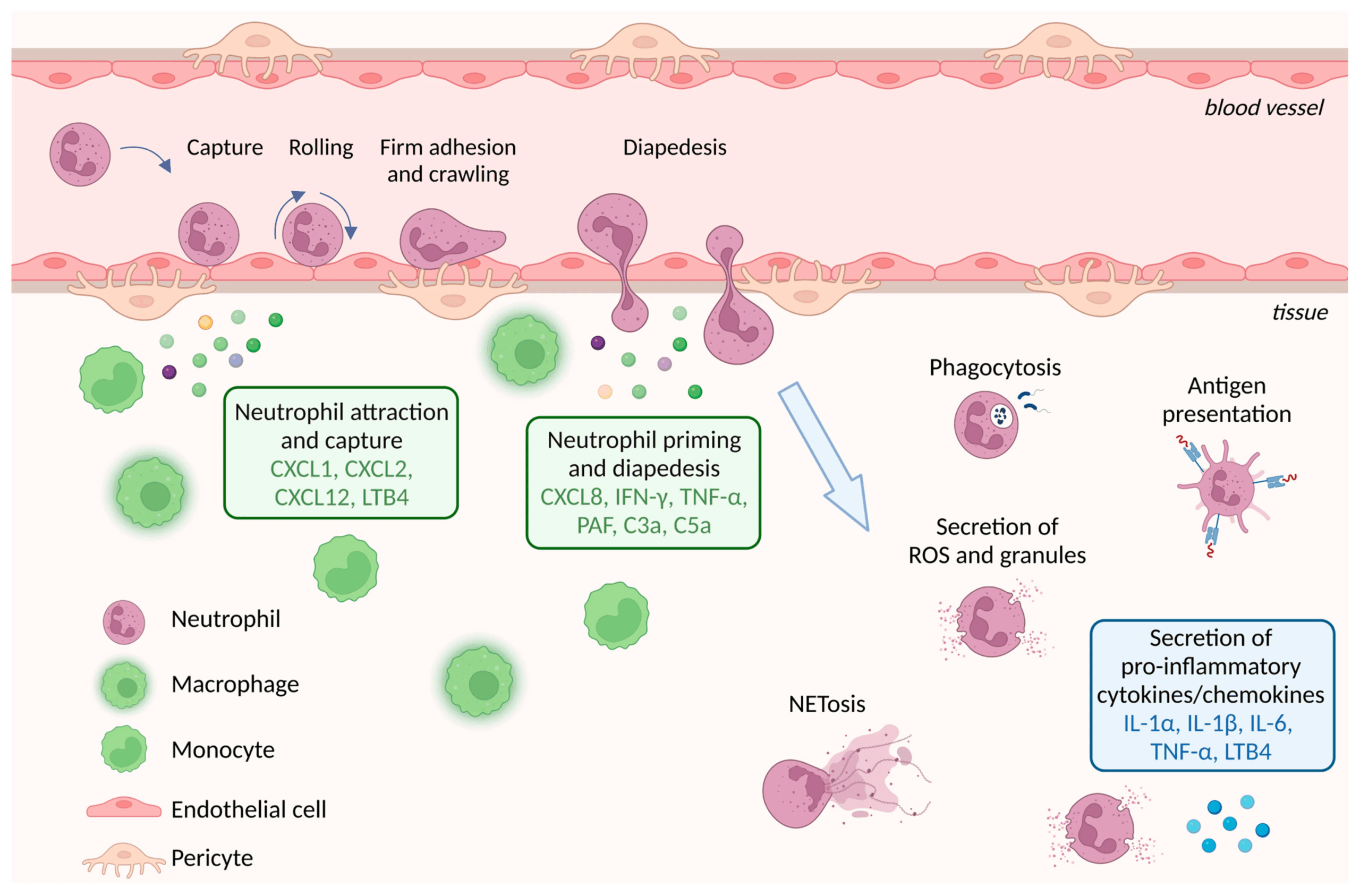
Typically inflammation will occur when damaged cells release cytokines which trigger mast cell activation. Once activated, mast cells degranulate releasing pro-inflammatory cytokines such as histamine, bradykinin, and prostaglandin, all three of which cause vasodilation of local blood vessels resulting in increased blood flow to the area. These specific types of prostaglandins, bradykinin, and histamine also increase the permeability of local capillaries, resulting in plasma fluid leaking into the damaged tissue bed. This leaked plasma fluid (called exudate) contains plasma proteins such as fibrinogen as well as platelets. Platelets, fibrin, and clotting will form any necesary platelet plugs to seal any broken blood vessels. Additionally platelets and fibrin serve to contain the infected or damaged area. Platelets are even capable of coating or encircling bacteria, facilitating phagocytosis by neutrophils. At the same time, blood vessel wall endothelial cells express factors that facilitate the stages of diapedesis (emigration) of WBCs into the tissue bed. Endothelial cells express receptors that stimulate WBC rolling and adhesion and then will express enzymes to loosen junctions between neighbouring endothelial cells to facilitate transmigration (WBC exiting blood vessel to enter tissue bed). Additionally, chemokines are secreted by many cell types including endothelial cells and mast cells. It has been found that there are many contributors (cells, cytokines, and chemokines) to the inflammatory response, which serves to increase the movement and recruitment of neutrophils, monocytes, macrophages, dendritic cells, eosinophils and basophils. Not only do WBCs contribute to removal of pathogens and cellular debris, they also secrete growth factors to stimulate healing.
It is often state that there are two phases of inflammation: vascular and cellular. In the vascular phase, vasodilation and increased capillary permeability are occuring within local blood vessels. In the cellular phase, emigration of the WBCs is occurring.
Local Effects of Inflammation:
There are 5 possible signs of inflammation, some of which are viewable from the surface when the injury affects the skin or underlying connective tissue. These 5 signs are: redness, warmth, swelling, pain, and sometimes loss of function. The increased blood flow (hyperemia) causes both redness and warmth as blood temperature (37C) is often slightly warmer than surface tissues of the body. The increased capillary permeability allows for leaked plasma fluid (exudate) leaking into interstitial spaces causes the swelling, which can be called edema when the amount of leaked fluid is substantial. Several chemicals can trigger nociceptors (pain sensory neuron receptors). For example, chemicals released by damaged cells, chemicals released from mast cells (e.g. prostaglandins and bradykinins,). Leaked blood and extracellular ATP can trigger nociceptors as can pressure building up from exudate. Interestingly, it has been found that histamine stimulates a particular type of nociceptor which gives rise to an itching sensation.
There are four types of exudate: serous, fibrinous, purulent and hemorrhagic. Serous exudate is watery, containing some proteins and WBCs. Small burn blisters that haven’t be punctured, typically contain serous exudate. Fibrinous exudate found in severe injuries and infections is thick, sticky, contains fibrin and is associated with an increase of scar tissue formation. Purulent exudate is often thick, yellow-green, containing WBCs and micro-organisms occurring in bacterially-infected abscesses and acne. Hemorrhagic exudate contains blood from damaged blood vessels.
Systemic Effects of Inflammation:
There are several systemic effects that arise during the inflammatory response: mild fever, malaise, fatigue, headache, and loss of appetite. At times decreased mental function can occur particularly in the elderly.
*Note: Problems can arise when too little inflammation occurs. In some immunosuppressive diseases, too little inflammation can result in prolonged irritation, damage, infection of tissues and greater amounts of tissue damage which could be permanent depending on the location.
**Note: Unfortunately, too much inflammation can also be a problem. Chronic health issues such as atherosclerosis, osteoarthritis, autoimmune diseases, allergies, and asthma stimulate prolonged inflammatory responses resulting in too much WBC activity which leads to cyclical deteriorative bouts of tissue healing and destruction. It has been found that the cytokine leukotriene plays a role in prolonged inflammation. Leukotriene, as the name suggests is produced by many types of leukocytes including mast cells, basophils, neutrophils, monocytes, and eosinophils. Leukotriene is a vasodilator, it increases capillary permeability, and within cases of asthma has been found to be a potent bronchoconstrictor.
***Note: The cytokines involved in inflammation, histamine (a nitrogenous compound), and the lipids Prostaglandin, and Bradykinin and Leukotrienes are referred to as vasoactive compounds as they all induce a change in blood vessel diameter. They also play a strong role in causing bronchoconstriction, bronchiole/intestinal mucus production and chemotaxis of WBCs.. In addition to mast cells, activated platelets also secrete pro-inflammatory histamine, bradykinin and histamine.
****Note: During healing of a wound, in addition to the surrounding tissue cells (mesenchymal cells, endothelial cells, fibroblasts, epithelial cells), the following activated WBCs (macrophages, T-lymphocytes) have been found to secrete growth factors (EGF, TGF-alpha, PDGF, FGF-1, FGF-2, PDGF, TGF-alpha, TGF-beta) to stimulate healing.
Innate Defenses: Fever
The rise in body temperature above 37.2°C is termed a fever and can occur when pyrogens are released in response to cellular damage or irritation. As with inflammation, fever can be caused by any type of cellular damage or irritation (e.g. cuts, blunt trauma, burns, infections, sprains, chemicals, ischemia, excess heat or cold, and even heart attacks, strokes and some degenerative disease). Low-grade fever (38-39°C) is an important innate response as it accelerates WBC activity, inhibits pathogen metabolism and replication rates, and speeds up healing.
Chemicals that stimulate the thermoregulation center in the hypothalamus to increase body temperature are termed pyrogens. Endogenous pyrogens (e.g. interferons and interleukins) are those produced by the body whereas exogenous pyrogens are foreign components (e.g. LPS, Lipopolysaccharides of bacterial cell walls),
*Note: High, spiking fever (40°C or above) can be dangerous as it can induce febrile seizures, which put the brain at risk for neural damage. High temperature is also exhibited in those suffering from heat stroke, and the inability to thermoregulate to cool oneself.
**Blunted or absent febrile response to an infection can occur in the elderly or immunosuppressed and this may delay diagnosis and treatment.
***Fever of Unknown Origin, FUO are thought to be caused by inflammatory responses to undetectable cellular damage (possibly due to infections, trauma, cancer, heart attacks, blood clots, inflammatory diseases, or drug reactions, etc.)
****Systemic Inflammatory Response Syndrome can be fatal and is associated with an enormous release of inflammatory cytokines causing systemic vasodilation, capillary permeability which results in hypotension and cirulatory shock. Most freuqent causes include sepsis.
Summary: Normal Innate Defenses of the Body:
- Innate (non-specific) Defenses:
- Mechanical/Physical – skin, hair, mucus, sebum, urination, cilia, cell shedding
- Biochemical – sweat, tears & saliva (lysozymes), bile, stomach pH, cerumen, mucus, vaginal secretions, prostatic and testicular secretions,
- Normal Flora
-
Phagocytes: (WBCs such as monocytes, fixed and free macrophages, microglia, neutrophils, eosinophils, dendritic cells) capable of diapedesis/emigration/transmigration.
- Complement System (Classical Pathway with antibody, Lectin Pathway, and Alternative Pathway) – involving 30+ complement plasma protein cascade of activation – resulting in opsonization, MAC (Membrane Attack Complexes), stimulation of mast cells & basophils
- Cytokine family: Glycoproteins produced by WBCs, fibroblasts, endothelial cells, stromal (connect tissue) cells
-
Interferons: (chemical messages that stimulate defense)
- Alpha Interferons – produced by virally infected host cells to attract & stimulate NK cells and stimulate AVP production in neighbouring cells.
- Beta Interferons – produced by fibroblasts to slow inflammation, and promote healing
- Gamma Interferons – produced by T & NK cells to stimulate macrophage activity
-
Chemokines: induce chemotaxis
-
Lymphokines: produced by T lymphocytes to: 1) attract macrophages & 2) stimulate B lymphocytes to produce antibodies
-
Interleukins: produced by helper T cells to:1. activate macrophages and stimulate fever (act as endogenous pyrogens)2. stimulate T & B cell differentiation3. Stimulate hemopoietic cells to proliferate → producing more WBCs
-
Natural Killer cells (NK Lymphocytes) – type of WBC (White Blood Cell/Leukocyte)
-
- Inflammatory Response
- Fever – speeds up WBC activity and repairs, inhibits pathogen activity
Think About Questions:
Why is inflammation considered a non-specific defense? What are other non-specific defenses of the human body?
Why does inflammation occur any time that there is an injury or disease?
Did you know that biologists sometimes call the digestive system an external tube that penetrates the body? Name one feature of the digestive system that prevents ingested microbes from causing an infection.
Why does taking an antacid put you more at risk for stomach infections?
Imagine you have a papercut – list the innate factors of your body that will help eliminate the bacteria that enter that cut.
On a neutrophil, define the following: pseudopod, phagosome, lysosome, granule
How does a NK cells kill bacteria?
What is properdin?
What is an interferon?
What is a respiratory burst?
Did you know that some diseases are caused by auto-antibodies? And some are caused by auto-complement proteins? https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(23)01524-6/fulltext
Media Attributions
- Innate Defense – Open University © Basiro Davey, Carol Midgley, Claire Rostron and Daniel Berwick is licensed under a CC BY-SA (Attribution ShareAlike) license
- Inflammatory Response © J. Gordon Betts, Kelly A. Young, James A. Wise, Eddie Johnson, Brandon Poe, Dean H. Kruse, Oksana Korol, Jody E. Johnson, Mark Womble, Peter DeSaix is licensed under a CC BY (Attribution) license
- Gut Microbiota © Jawhara, Samir is licensed under a CC BY (Attribution) license
- Pathogen Transmission © Christy Bowen, Lindsay Draper, Heather Moore adapted by Zoë Soon is licensed under a CC BY (Attribution) license
- Private: Gut_microbiota © Wakana Sasaki is licensed under a CC BY (Attribution) license
- Private: phagocytosis © By GrahamColm at English Wikipedia, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=6811745 is licensed under a CC BY-SA (Attribution ShareAlike) license
- Private: Neutrophil Granulocyte © Laboratoires Servier is licensed under a CC BY-SA (Attribution ShareAlike) license
- Private: NeutrophilerAktion.svg © Mario Schubert is licensed under a Public Domain license
- neutrophils-12-01981-g003 © Tsioumpekou, M., Krijgsman, D., Leusen, J. H. W., & Olofsen, P. A. (2023). The Role of Cytokines in Neutrophil Development, Tissue Homing, Function and Plasticity in Health and Disease. Cells, 12(15), 1981. is licensed under a CC BY (Attribution) license

{kind=link}
{kind=link}
{kind=link}