Chapter 1 Introduction to Pathophysiology; Cellular Responses to Stress, Injury, and Aging
Introduction to Pathophysiology
Zoë Soon
Vocabulary
In this section, we will outline several vocabulary terms that are used in pathophysiology, as well as cellular responses to stress, injury, and aging.
P is for Pathology, Pathophysiology, Pathogen, and Pathogenesis – What is the difference between these terms?
First of all, what is this term pathology? If we break that word pathology down, you probably know that ‘-ology’ means ‘the study of’, and pathos is Greek in origin, and refers to disease or pain. So it might make sense that pathology is the study of cell or tissue changes due to disease.
The next term, pathophysiology, if we were to look at the components of that word – you may already know the term physiology, having likely studied anatomy and physiology previously.
Anatomy is the study of a particular structure within the human body and remember, physiology is defined as the study of the function of a particular structure within the human body.
So therefore you might guess that pathophysiology refers to the study of abnormalities in physiology as a result of disease, or study of abnormalities in the function of a particular structure of the human body as a result of disease.
The next term is pathogen, refers to any microorganism that causes disease; it might be a bacterium, a virus, a fungi/yeast, a helminth, or protozoa.
Let’s go through some more terms, the next is pathogenesis. So you know that the Greek word, pathos- is referring to ‘suffering‘ and genesis means the ‘creation of‘ (Latin and Greek). Ok, So we’re basically when we talking about the pathogenesis of something, we’re talking about the creation or the mechanism of that disease, in particular we are referring to all of the steps that occur at the cellular and molecular level, as well as at the organ and organ system level. Therefore, pathogenesis refers to the mechanism of the disease, and all of the steps that unfold as the disease progresses in the body.
The term lesion is defined as the anatomic abnormality of that disease. It might be an open wound, tissue damaged or destroyed by a pathogen, a broken bone, or a cancerous growth.

This torso was created in the image of a man’s torso, dissected so that the internal organs could be seen, and was probably dedicated to heal someone suffering from internal disease or injury. Made c. 200 BCE – 200 CE, most likely in Isola Farnese, Italy. The piece is now part of the collection of the Science Museum in London, UK.

What is disease? What is considered healthy?
It is important to be able to determine what is considered healthy and what is considered disease. Disease most often is accompanied by indicators that signal that something is negatively affecting the normal physiology, either in a temporary or permanent manner. To determine what signs, symptoms, and measurements may indicate disease, it is important to think about the range of physiological measurements that are considered normal, and fall inside the normal and expected functioning range of the human body. This normal range is most conducive to organ and tissue homeostasis and the physical well being of the human body.
As each human is slightly different, it is to be expected that there is a range of physiological measurements that can indicate optimal health. For example, there is a normal range of healthy blood pressure readings, of heart rate measurements, and of body temperatures. It is also true that with these measurements, for example, your own blood pressure, heart rate, and body temperature – they will all change depending on if you are at rest or exercising. In this case, elevations in heart rate, blood pressure and body temperature, if within the expected range for exercise, is considered normal and doesn’t mean that you’re sick. It might just mean that you’re taking a break from sitting and studying and have gone for a run or a bike ride.
So of course it’s very important for health care professionals to know what the normal range of blood pressure and heart rate is, including knowledge that in some cases, these normal ranges are going to be different depending on how old a person is, and at times what biological sex a person is as well as other lifestyle factors. For example, most often, individuals that are biologically female (XX) have higher heart rates during rest and during exercise, in comparison with age-matched, biological males (XY). Additionally, it is known that trained athletes typically have lower resting heart rates than age-matched individuals that are sedentary. Heart rate is age-dependent as well, with infants have higher heart rates than children, and children having higher heart rates than adults. Smokers also typically have higher heart rates than non-smokers. Therefore heart rate typically depends on several factors including: body size, biological sex, age, fitness level, exertion level (during rest or exercise) and lifestyle. Certainly some diseases can affect heart rate, and
This range of normal, healthy functioning of the human body, may bring to mind the word homeostasis. Homeostasis (from two Greek words homoiosis meaning the ‘same’ and stasis meaning ‘standing’ or ‘state’) refers to the relatively stable internal environment that allows for optimal functioning of all of the tissues, organs, and organ systems of your body. You may recall more examples, besides, blood pressure, body temperature, and heart rate which are internally regulated to maintain conditions that are ideal for survival. Try to list as many as you can: water and electrolyte levels, oxygen, carbon dioxide and pH levels. Appropriate levels of nutritional compounds, waste compounds, hormones, growth and other regulatory factors, and the list goes on.
How does Disease affect Homeostasis?
When we think about disease, we know that it may be negatively affecting the functioning of cells, tissues, organs, and possibly even whole organ systems, depending on how widespread its level of impact is. If cells, tissues, and/or organs are not able to maintain homeostasis over time, then more and more cells throughout the body will be affected and start slowing in function, and possibly even begin to die.
Now, as humans, we don’t all have the same abilities. Some of us, for example, might be born blind or perhaps were born hard of hearing. If that’s the case, you don’t have hearing or sight within what is considered the normal range. Does that mean that you were born with a disease? No, we wouldn’t consider blindness or hearing in these particular cases to be considered a disease. It is not negatively impacting the function or health of organs and homeostasis is being maintained in all body systems. So when we speak of disease or disorder or pathophysiology, we’re thinking of things that again, are going to affect cellular homeostasis in a negative way.
So this brings us to back to the question. What is normal? Again, this is really important to understand about yourself, but also your patients/clients if you enter a Health Care Profession. What are these measurements supposed to be in terms of the body’s expected normal range, and ensuring homeostasis of the body? Can we think of measurements that may fluctuate with your circadian rhythm (your wake/sleep cycle?
Diagnostic Test Results Need to Accommodate for Circadian Rhythm and Expected Fluctuations in Body Temperature and Hormone Levels
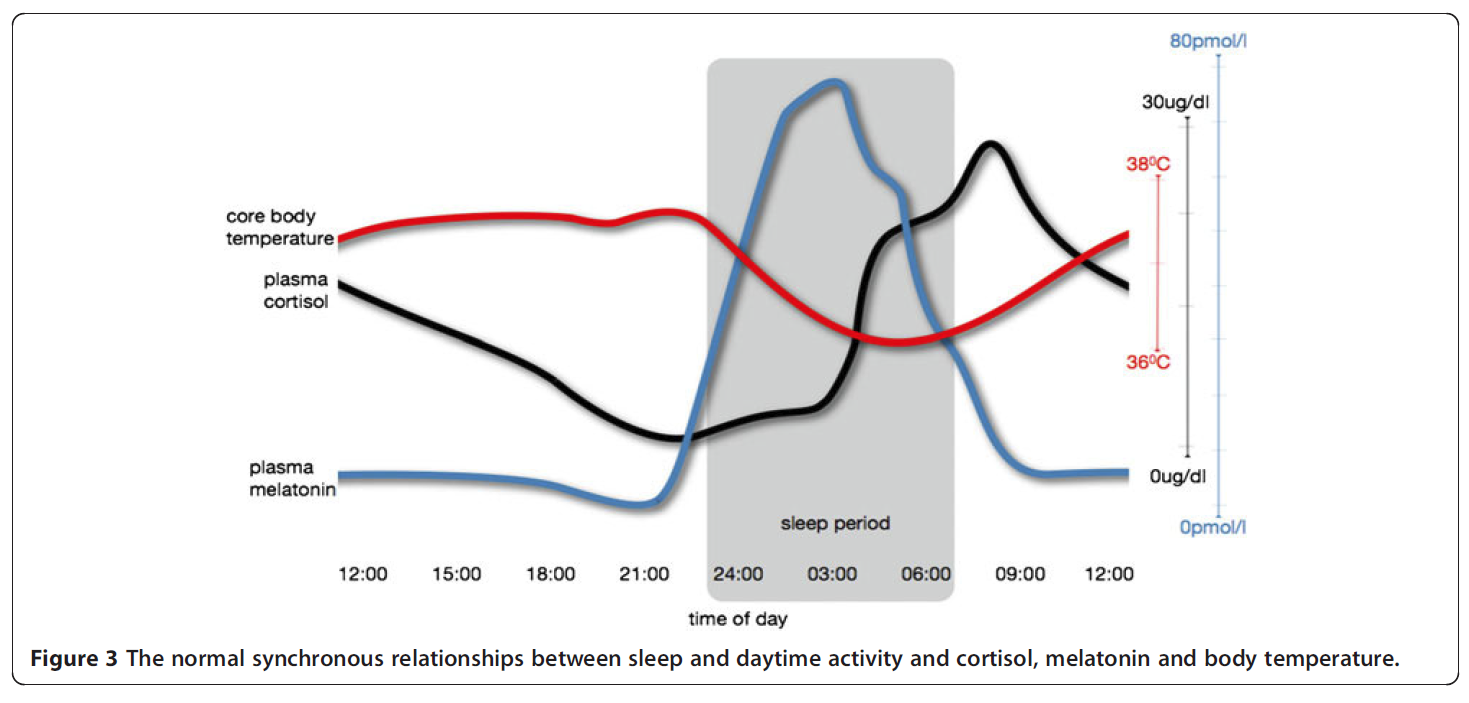
Hickie, I, Naismith, S., Robillard, R, Scott, E, Hermens, D. (2013). BMC medicine. 11. 79. 10.1186/1741-7015-11-79.
This graph is awesome in that there are normal expected daily fluctuations in physiological measurements such as body temperature and hormone levels. When you go to sleep, your body temperature drops by approximately 1οC. This graph also depicts the circadian rhythm of the production and release of two hormones. Cortisol, produced by the adrenal cortex plays many important roles in the body as does melatonin which is secreted by the pineal gland and also induces sleepiness. Both hormones are responsible for the maintenance of the daily circadian rhythm. The graph documents the concentrations levels of both of these hormones as they circulate the blood stream. The plasma cortisol levels rise in the morning which is thought to induce wakefulness and alertness. Whereas, the plasma melatonin levels rise in the evening in response to darkness and are partly responsible for inducing sleep and maintenance of the daily circadian rhythm.
D is for Disease or Disorder – what is the difference? And what is a Syndrome?
At times the following words are used somewhat interchangeably: disease, disorder, syndrome. What’s the difference?
Disease is typically defined as a physiological or biological ailment that has an underlying cause. It may result in anatomical changes that are temporary or become permanent.
A disorder as defined by the National Institutes of Health (NIH), as a “disturbance of normal functioning of the mind or body. Disorders may be caused by genetic factors, disease, or trauma.”
A syndrome refers to a cluster of various signs and symptoms that can vary over time. The NIH defines syndrome as “a set of symptoms or conditions that occur together and suggest the presence of a certain disease or an increased chance of developing the disease”.

What are some Terms to Describe the Duration, Severity, and Stages of Disease?
There are several terms to convey the severity and speed of disease progression.
The phrase acute onset, indicates the onset was sudden and the symptoms were severe. Conversely, the phrase insidious onset. is used when signs and symptoms developed more gradually, being mild at first and then becoming more pronounced. The phrase acute illness, most often refers to a sudden and severe illness that is short-term. With illnesses that have either acute or insidious onsets, the person afflicted may either recover fully, or be left with long-term physical damage, or perhaps even succumb from the illness. The outcomes typically depending on many factors including, the availability of effective treatments as well as the individual’s overall health and ability to overcome the underlying cause.
A chronic illness, is an illness that lasts longer than 3 months, most often starts with milder symptoms in comparison with an acute form of illness. With chronic illnesses, there can be remissions where that person recovers somewhat and feels a little bit better, and then there can be exacerbations or relapses, in which the disease has progressed and that person feels worse for a time.
Current literature suggests that pain, especially chronic pain is not necessarily always indicative of damage. At times, there are cases where a disease or injury has caused damage, yet there has been no pain. Conversely, at times there is chronic pain, when there is no longer any indication of damage. Pain has been found to not always be proportional to the biological or physiological state. The literature suggests that many factors (internal as well as external) can contribute to chronic pain. Therefore treatment of chronic pain can take on many forms that are individual in nature, at times involving physical rehabilitation and exercise strategies, various lifestyle strategies, and therapeutic counselling.
The next term is subacute, and if we were to break that word down, sub- means below, and acute, we know means sudden and severe, right? So we would say a subacute illness is not as severe as in an acute illness and is shorter than a chronic illness. I
The next word subclinical has the prefix, sub- which means below or lower down. So if someone is subclinical, that means that they are not experiencing any symptoms. That means it’s a very early stage in the disease and the person themselves is not even aware that they have any disease. So likely this person would not be seeking medical attention, and even if they did it would be unlikely that a a physician or nurse would be able to notice any disease present. All routine clinical exams would would come up negative, and there would be no signs or symptoms of something wrong. The only way we could to determine that this person has a disease is if some very sensitive, very specific tests (e.g. imaging or lab tests) were done.
Can You Think of Any Good Examples of When a Disease or Disorder is Subclinical? Latent?
You might well think of cancer. Cancerous cells, of course, when they first started growing, are largely undetectable by the patient or a nurse or doctor and by routine clinical exam. So you’d have to do very specific, very sensitive tests to actually know that, that cancer is there. Hence, cancer can present the problem of remaining undetectable in the early, more treatable stages, only causing signs and symptoms in late stages when it becomes more challenging to treat. So of course scientists are always trying to design earlier and more sensitive tests, in order to detect cancer (and other diseases) at earlier and more treatable stages, therefore increasing success and survival rates.
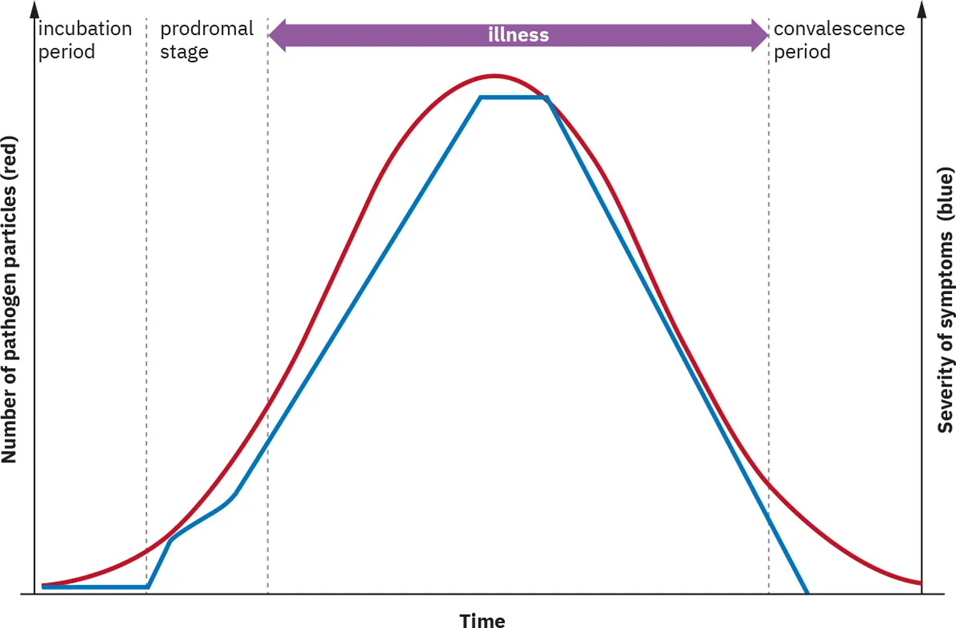
The next phrase is latent stage. There are two different scenarios in which the term latent stage stage is used. There could be an infectious scenario or there could be a non-infectious scenario in which the term latent stage is used. The latent stage in an infection begins when the infection first has taken place, when the pathogen has entered the body. The pathogen, that microbe (e.g. virus, bacteria, protozoa, helminth, prion, or fungi/yeast) will eventually begin to replicate (or amplify) inside the body. At the beginning of an infection prior to any significant pathogen replication, a person is usually not experiencing any signs or symptoms. For example, if it is a cold or flu, they’re not sneezing or coughing yet, and therefore usually they’re not spreading the virus or that bacteria (which in that case is usually through respiratory droplets). We would say in this scenario, the latent stage ends when that person does become infectious (or contagious). Now as mentioned most often, a person becomes infectious once that bacteria or virus (such as a cold or flu virus) has replicated and that person starts having signs and symptoms, perhaps a runny nose and sneezing and coughing. And of course, we know that that microbe is infectious when it is carried in respiratory droplets through the air and on hands and on surfaces of things and is thus transmitted to someone else. However, studies of the COVID19 pathogen, SARS-CoV2 virus, have found that in this case, the infectious stage can occur before signs and symptoms develop, and even in the absence of signs of symptoms this virus can be transmitted to someone else, as in the case of ‘silent spreaders’. So in this case, the latent stage still ends with the beginning of the infectious stage, however, with SARS-CoV2, the infectious stage does not coincide with the onset of signs and symptoms. For non-infectious conditions (e.g., cancer), the latent period ends when the cancer is detectable either by the onset of signs and symptoms or through the results of diagnostic testing.
Now in the absence of signs and symptoms, it can be hard to determine exactly when the infectious stage begins unless perhaps that person is being frequently tested to determine viral load numbers and estimating the probability of that person being now in the infectious stage, rather than the latent stage.
Moving on to the second scenario in which you will hear the phrase latent stage, it is when a non-infectious disease, such as a cancer has begun, but there are no signs or symptoms yet. In this case we would say the latent stage begins with the start of the disease (e.g. the first cancerous cell) and ends when it becomes detectable by testing, perhaps in either routine testing before signs or symptoms are present, or testing that is being done as a result of the emergence of signs and symptoms..
Now, the next terms incubation and incubation stage only occur during infectious diseases. Incubation never refers to a growing cancer. It’s always during infection, and specifically, the incubation stage begins when the infection has taken place (the pathogen has entered the body). The incubation stage ends when signs and symptoms develop. Typically, at the beginning of the incubation stage, a person has been infected with that virus or that bacteria or that fungus, but is not exhibiting any signs or symptoms. Most often, the signs and symptoms are start to occur once that microbe has replicated and signs or symptoms have developed, which marks the end of the incubation stage. Looking back at the definition of latent stage, you will notice that with many infections (e.g. cold, flu) you usually see a pretty big overlap between the latency stage and the incubation stage of of an infection.
So students always find these terms quite similar. You may have to read through them a few times before you get the differences subclinical, latent and incubation, ok.
The next vocabulary word is prodromal. The prodromal period is defined as the first time you become aware that you have signs or symptoms that indicate an illness is present. It might be the first time you feel the scratchiness of the throat when you have been infected with a cold or flu virus.
Where does it hurt? – Is this ailment Local or Systemic?
The next important terms are local and systemic. When we start investigating diseases and disorders, we need to examine the location of the body that’s been affected. If the area is discrete, meaning that only a specific section of the body is affected, we would say that that the injury or infection is localized. If the illness is affecting your whole body, for example, you’ve got a fever and your whole body is hot, we would call that a systemic symptom. Another example would be hypertension (high blood pressure) affects the whole body, so we would consider hypertension to be affect the body systemically.
Complication, Sequelae, or Convalescence?
Let’s go to some more terms, complication, which refers to the development of further negative conditions. Complications are variable and can take many forms depending on the underlying situation. For example, if a person has had a heart attack, there’s a chance that they will recover without any subsequent complications. However, it may be that a blood clot is produced which lodges in a blood vessel downstream of the heart, causing complications to occur as now there is an organ that is being deprived of adequate blood flow. Other complications of a heart attack may include tears in a weakened or damaged ventricular wall, or the filling of the pericardial sac with too much fluid resulting in the inability of the heart to expand and fill, a condition called cardiac tamponade.
With both the initial illness and with any subsequent complications, there is a chance that permanent damage may be prevented through the body’s own ability to recover and heal, or perhaps the required medical interventions and treatments are 100% successful. If there is a complication, However, if tissues are damaged beyond repair that result in a permanent or long-term impairment, the term sequelae is used. For example, spinal cord damage can lead to quadriplegia. This would be considered and example of a sequelae.
Certainly sequelae may result from either acute or chronic conditions. So let’s see if I can give you some more examples of sequelae.
The first example is diabetes. Diabetes is a chronic condition and if someone is perhaps not taking their medications properly, they may start accumulating biological damage that becomes permanent. Some common complications of long-term diabetes include chronic kidney disease, which can lead to the kidneys deteriorating and eventually failing. So in this case, we would see diabetes developing complications that lead to the sequelae of kidney failure and the requirement of dialysis and placement on the wait list for kidney organ donation and transplantation.
Let’s think of an acute condition that can lead to sequelae. In this example, someone has had a stroke (CVA, cerebrovascular accident). Unfortunately as a result of this particular stroke which has occurred on the left cerebral hemisphere in the frontal lobe, that person now has paralysis on the right side of their body. That paralysis on one side of their body may recover somewhat depending on the extent of the stroke and available treatment. However, some paralysis incurred is usually permanent, and we would call that a sequelae (from the the Latin word sequi, meaning ‘follow’).
A final example of sequelae, that you might not think of, is something that’s that’s not really a deterioration of an organ per se, but is a deterioration of mental health. In this example we will consider how Post-Traumatic Stress Disorder, PTSD is considered a sequelae. Perhaps you can picture the cause of PTSD, which is that this individual has suffered some trauma in their lives. Certainly soldiers coming back from war, or at any individual who’s witnessed or experienced trauma can be at risk for developing PTSD. PTSD can become a long term, maybe even a permanent mental health impairment. Thankfully a variety of new and individualized treatments for PTSD are emerging all of the time and as with some other mental health problems, there can be recovery.
Moving on to the term convalescence, that’s an easier one. Convalescence refers to the period of recovery. Potentially this recovery is facilitated by rehabilitation exercises. In some cases, convalescence involves speech therapy or improved mobility through using a cane, or walker or participation in a stretching or exercise program, et cetera. There are many treatment strategies and lifestyle changes that can improve recovery.
Can you Define: Diagnosis, Prognosis, Morbidity and Mortality?
Diagnosis is defined as the identification of the disease, disorder, and syndrome. An accurate diagnosis is essential in ensuring appropriate means of treatment are provided and also helps in making a prognosis.
Often an up-to-date patient medical history can be helpful in revealing an accurate diagnosis. Can you think of what might be listed in a patient’s medical history that would be informative for making a diagnosis?
The term prognosis refers to the predicted outcome of the illness or injury.
Morbidity, you probably know, refers to the rate of a particular disease within a population. Mortality refers to the typical death rate associated with a disease or disorder.
These terms, brings us to the word etiology, which refers to study of the cause, for example, what is the cause of the disease or disorder or syndrome?
Etiology – Causes of Concern?
Etiology, as we just mentioned is the study of causes of an illness. Let’s see if we can list some categories of causes of diseases, disorders, and syndromes? You can probably think of some already.
We’ve already talked about infectious diseases caused by viruses, bacteria, fungi, and parasites (e.g. protozoan-caused malaria). There’s immune dysfunction. which refers to an illness that arises when your immune system is either deficient or when the immune system is over-active as in the case of allergies and autoimmune diseases. We’ll dive more into the details of immune dysfunction diseases in Lesson Five.
Other causes include: trauma (e.g. bone fractures, wounds, injuries), nutritional deficiencies, cancer, lifestyle, toxins, genetics, congenital defects.
Also, we should take the time to investigate the terms: congenital defects and genetic disorders and hereditary diseases. What is the difference?
Now, genetic disorders, refers to an ailment caused by a DNA mutation. Unfortunately, you can be born with these DNA mutations having inherited them, or DNA mutations can occur later in life. DNA mutations most often occur spontaneously as DNA polymerase makes occasional errors while duplicating DNA each time a cell divides. Most often these errors are repaired by special DNA repair enzymes, although at times, the mistake goes unnoticed, and if it happens to be in a coding section of a gene, it can result in that protein either not being produced, or being produced in a manner that changes its function. In both cases, all the cells that express and require that protein can be negatively affected. Cancer is a result of DNA mutations in genes that are responsible for controlling the rate of cell division or cell cycling (mitosis and apoptosis). This leads cancerous cells to become non-functional and divide uncontrollably. We can therefore say that cancer is a genetic disorder. There are other genetic disorders, which you have likely heard of, that most often a person is born with. Cystic fibrosis for example is a recessive genetic disease caused by a mutation in a gene on chromosome 7. Sickle Cell Anemia is a recessive genetic disease caused by a mutation in the hemoglobin beta chain gene on chromosome 11. Marfan syndrome is an autosomal dominant disorder with a mutation found on chromosome 15. Huntington’s disease is also autosomal dominant, caused by a mutation on chromosome 4.
A hereditary disease is defined as a genetic disease which you have inherited. Hemophilia resulting from a mutation in one of the clotting factor proteins is most often inherited.
If we were to analyze the word congenital, the prefix, con-, in Latin, means ‘with’, and genesis refers to ‘the creation of’. The phrase congenital defects therefore is used to categorize anatomical or function defects that occur during embryonic or fetal development, resulting in defects that a person is born with. Examples of the most common congenital defects are: congenital heart defects, hypospadias (slight misplacement of urethra within penis), clubfoot (inward turn of foot), Down syndrome, cleft lip and cleft palate (incomplete fusion of right and left palatine and/or maxillae bones in the roof of the mouth), limb defects, and mental dysfunction. Nowadays, many of these defects can be corrected through surgery, or physical therapy (clubfoot). There are many causes of congenital (birth) defects, and most are thought to be multifactorial, meaning that likely many factors were responsible. Some congenital defects are caused by genetics. For example Down syndrome is referred to as Trisomy 21, as it results from inheriting three copies of chromosome 21 instead of two. Each case of Down Syndrome is unique with differing degrees of physical and cognitive impairments. At times some of the anatomical defect that may be present (e.g. congenital heart defects) can be repaired. Cleft palate, cleft lip, and limb defects have been linked to many potential factors: genetic susceptibilities, fetal exposure to toxins (mercury, lead), radiation, alcohol, drugs, and/or malnourishment.
At times, fetal exposure to alcohol and drugs can occur when a person doesn’t know that they are pregnant, leading to sequelae such as Fetal Alcohol Syndrome.
So drugs, alcohol and even infections (e.g. rubella virus, measles virus, mumps virus) including some of the sexually transmitted infectious diseases, such as chlamydia, and syphilis, can all cause congenital defects, which in those cases can include blindness, deafness, and cognitive delay and/or impairment.
A growing embryo and the later stage of fetus are especially susceptible to all of these factors as they are going through very critical stages of development including organogenesis (formation of new organs), which is when these toxins can have the most negative effect. Of course, there are other risk factors that are at play, in the development of congenital defects, including overall maternal health, maternal age, and exposure to cigarette smoke. As an example that has been in the news in recent years, you’ve likely heard of the Zika virus which is spread by mosquitos that tend to exist in countries in tropical climates (e.g. Uganda, Central America). Zika virus infections during pregnancy put babies at risk for being born with congenital defects, which can be fatal and include microcephaly, reduced brain development, and subsequent cognitive impediments. All of these agents (microbes, alcohol, drugs, toxins, radiation, x-rays, nutritional deficiencies) that can cause congenital defects (and miscarriages or stillbirths) are frequently grouped together and are called teratogens.
The severity of the congenital defects typically depend on the timing of the exposure to the teratogens, the duration of exposure, the amount and concentration of teratogen, as well as the fetus’s genetic composition. Some people are more genetically susceptible to different toxins than others.
Causes of diseases are sometimes arranged in the following categories. Can you think of examples of each one?
Clinical Manifestations – Signs or Symptoms?
Clinical Manifestations is really just a fancy way of saying signs or symptoms.
Signs are defined as observable indicators of illness. Signs include: fever, rash, lab test results, imaging results.
Symptoms are defined as indicators of illness that are not observable by another person (e.g. a health care practitioner) Symptoms can include: pain, weakness, fatigue, nausea, headache, cramps, and sleeplessness.
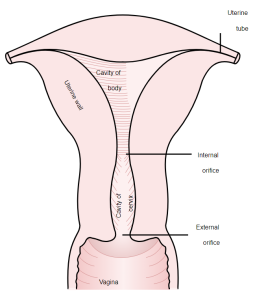
One lab test that you may have heard of involves taking a biopsy. The word biopsy means excision, for the purposes of cutting out and then examining tissue samples, usually under a microscope for signs of disease. At times a biopsy may involve scraping rather than cutting out. For example if you’ve gone for a Pap smear you may know that cervical cells are scrapped and sent to the lab to be examined as means by which to detect early signs of cervical cancer. A Pap smear is a routine test typically performed every 2-3 years (as per personal physician’s recommendations) after an individual has become sexually active. The cervical cells are examined under a microscope to see if there’s been any morphological changes indicative of cancer. Early detection of cervical cancer ensures early treatment and an increased chance of survival.
Let’s go to the next term, idiopathic disease. That’s a term used when the cause of the disease is unknown. The prefix idios is Greek for “one’s own”. At times, the term essential is used as a synonym for idiopathic, for example essential hypertension, which is high blood pressure that is not a result of a medical condition (most often essential hypertension is linked to obesity, unhealthy diet, sedentary behaviour, and family history).
Here’s another one that sounds similar, iatrogenic disease though is used to refer to a disease that is caused by the health care practitioner, or the treatment. The prefix iatro is Greek for “doctor”.
The next term, predisposing factor, is used as another word for risk factor. Let’s see if we can think of risk factors for different diseases and disorders.
Age is a risk factor. Usually the older you are, the more at risk you are for cancer and other diseases as a lifetime of exposure to different damaging agents has occurred, plus the cells in your body are gradually slowing down are less able to battle infections and heal tissue.
Biological sex, for example being XX or XY can be a risk factors for different illnesses. To name a few, it has been found that biological females (XX) are more at risk for autoimmune diseases as well as have a greater susceptibility to lung cancer. Biological males (XY) are more at risk for cardiovascular disease and X-linked colour blindness and Duchenne muscular dystrophy.
Genetics, as we have mentioned, can make you more susceptible to a disease, for example, sickle cell anemia and cystic fibrosis.
Congenital defects, as you can imagine can sometimes (e.g. congenital heart defects) make the affected organs less robust and more susceptible to the normal wear and tear of aging, injury, and at times disease.
Diet can be a risk factor. There can be two categories of problems, the first affecting the greatest number of people in the world, is malnutrition, which is not very beneficial for your growth as a child, your cognitive function and for your organ function and survival rates in general. Conversely, many Western countries are facing an obesity crisis, in which diets that are high in fat, sugar and/or salt put individuals at risk for heart disease, diabetes, and may even be linked to Alzheimer’s disease.
Occupation can be a risk factor. If you’re exposed to a lot of radiation, asbestos, coal dust, and/or other pollutants, for example, these are risk factors for many different diseases including cancer and lung disease. There is research that is linking pesticide use to the onset of Parkinson’s Disease.
Another predisposing factor or risk factor is where you live – location. So this, of course is not avoidable for most people – you live most often where you are born and are supported unless you have the means to travel. Every part of the world, hosts its own ecology and spectrum of infectious microbes, sociodemographic and cultural factors. For example, Malaria, which affects millions of people each year, is caused by a single-celled microorganism (a protozoan) that is transmitted from person to person by a mosquito bite. The mosquitoes that carry this particular Plasmodium parasite live in certain regions of the world, requiring a tropical climate. So if you live in one of these regions, you’re more at risk for developing malaria. Another example is within Canada, where asbestos was mined until 2011. We know that exposure to asbestos puts you at risk for developing mesothelioma cancer. Cardiovascular disease is the number one killer in the world and again, certain parts of the globe experience higher rates of this disease, most often due to societal lifestyle choices. Take a look through these maps to get a sense as the world’s burden of different disease.
Neglected Tropical Diseases
Now while we are looking at these maps, you will notice that there are different regions of the world that are highlighted as hotspots illustrating:
a) Number of people requiring interventions against neglected tropical diseases
b) The global distribution of the disease burden
c) The disease burden from non-communicable diseases
d) The burden from communicable, neonatal, maternal and nutritional diseases
e) The burden of injury, violence, self-harm and accidents
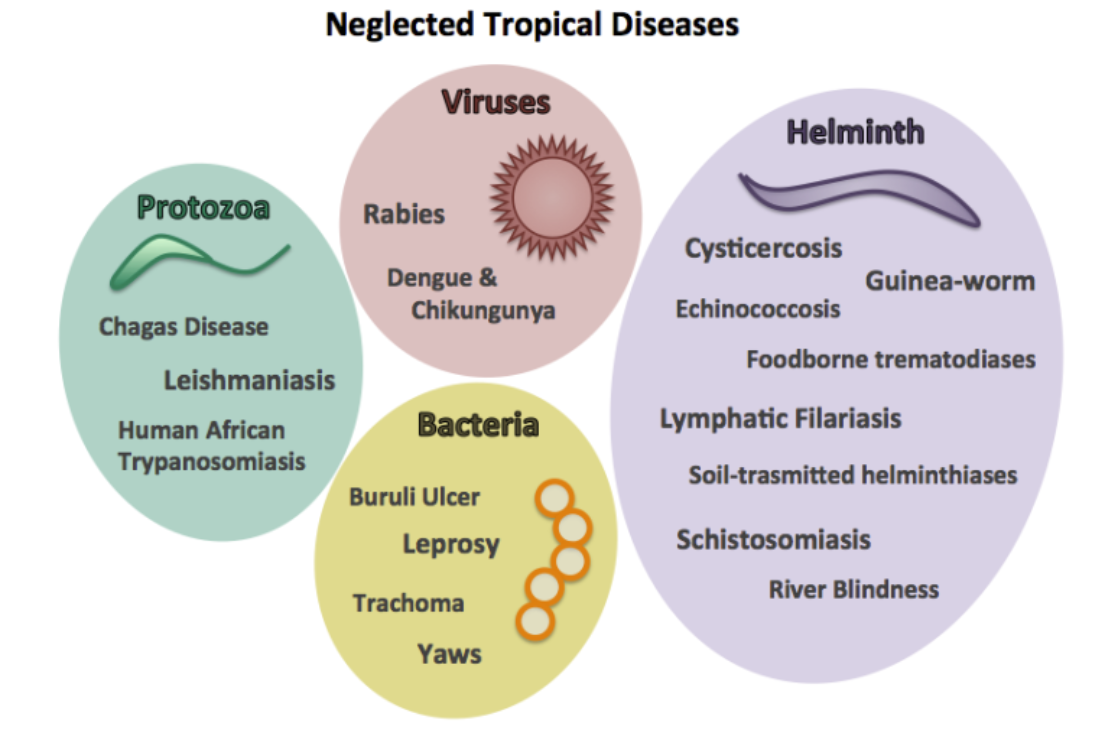
Now what are Neglected Tropical Diseases? As the name suggests, this is a group of diseases that are most prevalent in the tropics and despite affecting millions of people each year, there just isn’t enough of an effective prevention or treatment plan in place yet. In this category, Malaria and Tuberculosis alone kill 2 million people a year. It’s staggering. So of course, the World Health Organization as well as other government agencies (including universities), and private donors are funding research to try and alleviate or eliminate some of these neglected tropical diseases that affect millions and millions of people, causing suffering, disability, and even death. Though more work needs to be done.
These diseases are called neglected because pharmaceutical companies and largely neglect putting research money into the development of preventions (e.g. vaccines) and treatments for those diseases. Part of the problem is that the Western nations are largely unscathed by these diseases, (e.g. malaria, tuberculosis) and therefore companies anticipate that treatments addressing these tropical diseases would be less profitable and instead focus on developing drugs to combat cardiovascular disease and other diseases more prevalent in Western nations. Another part of the problem is that some of these neglected diseases require large amounts of money to be spent on improving local infrastructure (e.g. sanitized water, access to clean and healthy food and food preparation and health care, mosquito netting, public safety measures for workplace etc.) and at times health education.
Let’s briefly describe a few more of these Neglected Tropical Diseases (NTDs), just to give you an idea as to what is on the list:
Chagas disease , like Malaria is caused by a protozoa carried by an insect vector. Rabies and Dengue fever, both are caused by viruses and Leprosy is caused by a bacteria. There are many diseases caused by different helminths, which are tiny little parasitic worms (e.g. Guinea-worms). They generally enter the body through contaminated water that is consumed or even waded in. Some helminths can penetrate the skin of ankles and feet and rest of the body while standing or swimming in water and some types of helminths enter the body through contaminated food or water.
The case numbers of NTDs are staggering. with 1.4 billion people currently affected. And just to give you some numbers, there was a study found that more than 1500 drugs came to market between 1975 and 2004 and only 10 were targeted at these neglected tropical diseases out of 1500. Now, a large number of those drugs, 1500 were targeted against diseases and disorders that the Western nations experience. So things that are involved with heart disease, high cholesterol, and a lot of those diseases that can be offset by healthy lifestyle.
What is Epidemiology?
So this brings us to the word epidemiology – what is epidemiology? Epidemiology is the science of tracking the pattern and the occurrence of disease. This is very important, because we want to be prepared each year and be able to ensure that we are developing and putting in place effective prevention strategies and treatment strategies. We want to be really efficient with tax-payers’ money in health care money. As well as be proactive with training and hiring health care professionals. We want to have a very targeted approach. So typically these prevention strategies involve ensuring education, healthy food security, travel advisories, vaccinations, equipping health facilities with medical equipment, staff, testing labs, and medicines. Education can involve teaching the public about healthy food, exercise, safe driving and hygiene strategies to minimize risk of exposure to contagious diseases, such as during COVID19 with the hygiene strategies of masking and gloving being put in place. Most often education strategies involve providing public information on how to avoid preventable diseases. For example, the prevention of sexually transmitted diseases through the use of barrier protection. So, if you are an epidemiologist in Canada, you’re going to be involved in tracking the diseases that affect Canadians each year and then ensure that money is spent on the most effective prevention and treatment strategies for those particular diseases.
That brings us to our next term. What is a communicable disease? Communicable is used interchangeably with infectious.
The next term is notifiable disease. Now you might expect that epidemiologists are tracking notifiable diseases – what is a notifiable disease in Canada? Notifiable diseases, typically are defined as diseases that are tracked in number as they are regular, frequent, and timely information is necessary in planning the prevention and control of the disease in order to maintain public safety. Enough medications and resources need to be purchased and made available. Appropriate and timely public education needs to be delivered. So if I were to ask you to list some diseases that you think are notifiable in Canada which diseases would you list?
You may start thinking of serious ones, such as AIDS, which is definitely a notifiable disease. Take a look through this list and point out the diseases you recognize. How many of these diseases are infectious? More than half or less than half?
Notifiable Diseases in Canada and the Years Notifiable:
Over the next year or so if you continue your studies in this field you will begin to notice that most of these diseases are microbial and they are infectious.
Do you think this may explain why epidemiology, health care planning and public announcements are important?
What is the difference between prevalence and incidence?
Incidence is defined as the number of new cases, while prevalence is defined as the number of new cases plus the number of older but current cases. So you can tell by the math, that prevalence is always going to be higher than incidence because it’s new plus old cases. So this is the type of thing that epidemiologists track. Let’s take a look at this graph:
Endemic, Epidemic or Pandemic – which is which?
As we have done previously, looking at the etymology (study of word origins) of each of these terms can be helpful in remembering the difference between them.
Endemic is made up of two Greek words: ‘demos’ translating to people, and ‘endo-‘ referring to within. So if a disease or disorder is endemic, we would say that disease is maintained in a population at expected levels, and occurs without an outside source. For example, we know that there’s going to be a certain number of cold virus infections in Canada every winter, which is most often caused by rhinoviruses or adenoviruses. These infections do not need to be brought into Canada from another country. Although these cold viruses have a seasonal peak of infections, these viruses are maintained at a low level year round, evolving, and then causing yearly increase in infections typically rising in the fall and peaking over the winter. A certain approximate number of infections is expected in Canada each year, and we would say the the cold viruses are endemic to Canada.
The next term, epidemic. again consists of two Greek words: ‘demos’ (people) and ‘epi-‘, meaning above. So epidemic is used to refer to an outbreak of a specific disease that is occurring at a higher rate, affecting more people than expected within a set population. So if we think of the flu virus, again, similarly to the cold viruses, we expect a certain number of flu cases to occur in Canada every year. So we would say that the flu virus is endemic to Canada. Occasionally there are years, when all of a sudden there’s a higher flu rate than expected. During that time, we would say there’s, there’s a flu epidemic in Canada.
If we examine the word pandemic, with ‘demos’ meaning people and ‘pan-‘ meaning all or global, you may guess as to this term’s usage. A pandemic is used at a time when an infectious disease, such as the flu or the coronavirus (e.g. SARS-CoV2 also known as COVID19) has spread across borders. During a pandemic a pathogen has spread across regions, and may even spread worldwide. You may know of the more recent examples of pandemics which have included: the Spanish flu of 1918, the H1N1 flu in the early 2000s, and then SARS (CoV1) in 2003 and the novel corona virus (SAR-CoV2) COVID-19 in 2019.
How hard is to cure cancer (or find cures for other diseases)?
Let’s take a brief pause and consider how new medications and treatments (e.g. new surgeries and other procedures) are developed and then tested before being approved for use.
I think if we quickly go through the steps, we’ll have a new appreciation for how much money, work labour, and time it requires, not to mention innovative ideas as well as ethical safety measures.
Due to the expense, pharmaceutical companies fund approximately 80% of health research, with the rest funded by philanthropists (e.g. Bill and Melinda Gates), governments (which include universities).
Why is it so expensive and why does it take so long?
Let’s look at the 4 big stages of drug development:
Stage Zero: At this stage either,
a) Combinatorial chemistry is used to create and purify a synthetic compound. Often these compounds are developed using previously-researched data that projects what type of chemical properties (size, shape, charge, enzymatic qualities, etc.) are desired in combating this disease. Frequently the process of synthetic compound design is informed by detailed knowledge of disease-specific cellular targets that this new medical compound is being designed to interact with, and what type of interaction would be beneficial.
Also at Stage Zero, instead of synthetic approaches it may be that,
b) a natural compound is purified. For example if a plant is suspected to have medicinal properties, it would be important to purify the exact compound(s) which is thought to be helpful and prepare it for testing. We have to keep in mind that all plants consist of thousands of different compounds, some of which may be inadvertently harmful. So it is important to isolate and identify compounds that are of value and that any negative side-effects or interferences of other components are avoided.
Stage One, most often involves testing these purified (synthetic or natural) compounds in Petri plates full of human cells. There are many human cell lineages that can be used to test the safety and effectiveness of these new compounds. Some cell lineages are epithelial cells, others are muscle cells, some are neural cells. There are even cell lineages that have been designed to mimic certain disease conditions. At this stage you can perform dose-dependent studies, in which different plates of cells are exposed to increasing amounts of the new compound. Each of these plates can be investigated to determine whether the cells were harmed in any way, as well as whether the new compound was effective in off-setting any of the disease qualities of the cells that are mimicking the disease. At the end of this stage, decisions are made as to whether this new compound should go forward to Stage Two. If the compound has been found to be harmful, the study will end, and the researchers will go back to Stage Zero to find another chemical that might be a good candidate.
Stage Two, is most often conducted in an animal model, typically in mice or rats that has been bred in a lab specifically for this purpose. At this point, it has been determined that the compound is safe and may be effective in alleviating the disease. The mice or rats are used as they are mammals and genetically and physiologically quite similar to humans. The benefit of this type of lab animal model, is that the genome sequence of mice is known. Mice and rats produce large litter sizes frequently (every 21 days), meaning that there can be sufficient numbers of test subjects that can be used, meaning that the statistical analysis that is required to properly verify the results of the study can be done. At this point, the compound is still too experimental to be ethically tested in humans. Further testing is required, to make sure that the compound is indeed safe. It is important to determine whether exposure to this compound is safe for all organ systems and that no negative side-effects are present. It is equally importantly to determine if the compound is indeed effective in diminishing the negative effects of the disease. Again, dose-dependent studies are performed and often mice that are bred to exhibit disease-like qualities are used in the study. In this way, it can be determined whether the new compound is helpful in curing or lessening the effects of the disease. At the end of Stage Two, if the compound has been deemed to be effective with zero to minimal side effects, it will move on to Stage Three.
Stage Three involves performing a double-blind study in a small group of humans that are effected by the disease and have signed up for this experimental drug trial. Frequently this group is not responding well to current therapies and are interested in trying out a drug which may work better. Should studies find this experimental drug to be successful, it will be ramped up to include larger groups of humans and the study will be repeated. At this time it is important to document any differences in how different age groups respond, as well as groups of humans that differ in biological sex or other key factors that may be of impact. It may be that different dosages or modes of administration (oral, injection) are examined at this time.
What is a double-blind study?
A double-blind study is a study in which there are two conditions:
a) The person receiving the drug or treatment is not told whether this is the new drug (or treatment) or whether it is a placebo or sham treatment.
b) Additionally the health practitioner giving out the new drug/treatment is also not aware of whether they are giving out the experimental drug/treatment or a placebo/sham treatment.
The reason this is done, is because there is what is called the placebo effect. The placebo effect typically means that ~30% of people that have received the placebo/sham treatment will feel better. It is believed that a positive mindset and anticipating improvement, actually can make a person feel better.
In a study in which the goal is determining whether the new drug/treatment is effective, it is deemed only effective if it’s improvements in alleviating signs and symptoms is better than what is observed in those that have received a placebo/sham treatment.
Studies have shown that even being in the presence of a health care practitioner can stimulate a placebo effect. Possible explanations include the comfort of being cared for.
What is a placebo drug?
Now for a placebo drug, sometimes a sugar pill is used, but most often, the drug that is currently on the market is used, as the idea is that researchers would like to prove whether the experimental drug is indeed better than what is currently available. Additionally, it is more ethical to have patients continue the best treatment possible during the study. The current drug is of course better for the patient than a sugar pill.
What is a sham treatment?
A sham or mock treatment mimics the actual treatment in a way that the patient is not aware that the treatment didn’t occur. There are examples of sham acupuncture, in which needles that look and feel like acupuncture needles are used, however the sham needles do not actually enter the skin.
If a placebo drug makes 30% of people feel better why is it unethical to just use sugar pills to treat diseases?
You probably know the answer to this one: the reason is because the positive effects of placebo drugs (or sham treatments) do not last. Typically after a certain amount time (weeks to months) the patient again begins to feel the effects of the disease. This is not surprising as the disease has not been cured, but is continuing to cause negative effects within the body.
Movie Time: Click here to watch the 4 minute TEDEx animation: The Power of the Placebo Effect and then answer the following question:
Unfortunately most new drugs, get thrown out after Stage One or Stage Two for one of 3 reasons:
a) They don’t work
b) They cause harm
c) They aren’t better than drugs that are currently on the market and are more expensive to make.
However, very rarely, there is a success story, and a new drug skips the large-scale human study and is immediately approved for use. When does this occur?
a) When the drug works so well, it is deemed most ethical to make it available to the public at once. This did occur with the drug AZT, azidothymidine, which is an anti-viral drug used in cases of HIV.
What is an Off-Label Drug?
Another term you may hear is off-label drug. An off-label drug has been through all of the stages of testing and has been found to effective at alleviating a different condition than what it was initially designed for.
I can give you two examples of off-label drug use.
- Thalidomide was made in the 1950s in Germany. It was initially thought to be really helpful for alleviating morning sickness in pregnant women. Unfortunately, even though it did help with morning sickness, they found that it actually caused a lot of congenital defects in addition to miscarriages. In terms of congenital defects, there were a lot of babies born that were blind or deaf or had a cleft palate, or who had missing or disfigured limbs. It took them about six years to figure this out and get the drug off the market. In the meantime, thousands of babies were affected across Canada, Germany, the United Kingdom, the US, throughout Europe. Since this time, thalidomide, although not safe to use during pregnancy, has been found to be good for some cancer treatments.
- Another example is Viagra which is a vasodilator that was developed for use in heart disease in which it would be beneficial to dilate the coronary (heart) arteries. However, the researchers found the vasodilation of penile arteries occurred resulting in enhanced male erections. So of course, it had gone through all of these tests and was found to be safe and effective. As Viagra, is used for purposed other than heart disease, use for erectile dysfunction would be considered an off-label use.
What is an example of a natural compound that is medicinal?
a) Antibiotics are antibacterial agents that are most often produced by other micro-organisms (including yeast/fungi). Humans have found it to be useful to mass-produce some of these antibiotics (e.g. penicillin) to combat bacterial infections, which can be fatal.
What can a biopsy tell you?
Microscopic analysis of cells and tissues is used to detect signs of disease and can be helpful in determining the cause and extent of disease progression. The study of the appearance of tissues, specifically the structure, shape, and arrangement of cells, is termed cell morphology. Now, it is important to know that diseases as well as just normal adaptations to the environment can cause changes in cell morphology, though usually in different ways.
In this section let’s take a look at the terms that are used to describe changes in cellular shape and growth patterns.
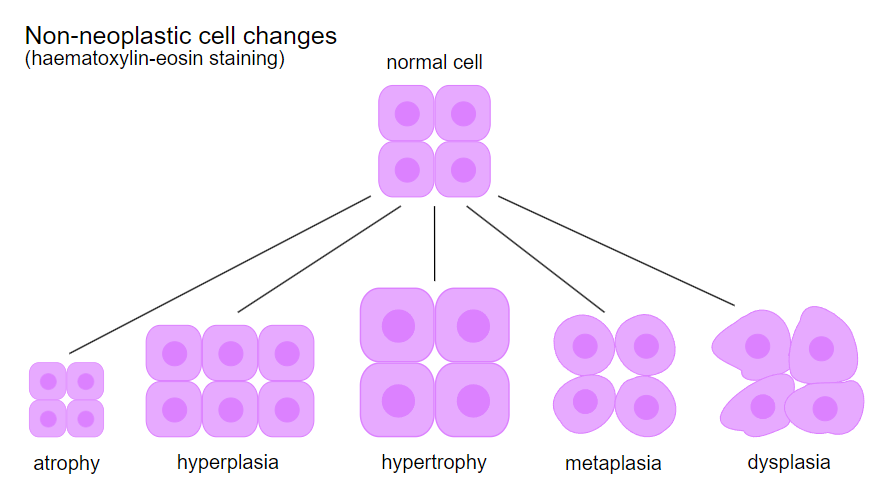
In the figure, the artist has illustrated some of the non-cancerous (non-neoplastic) cell morphology and growth pattern changes that can occur. So let’s go through them one at a time.
First of all, you will notice that the normal cells have been drawn to resemble stratified (many layer) cuboidal epithelial cells. Each of these cells contains one purple nucleus. Okay, notice this is our starting point. Each human cell type has a typical diameter, shape, and set of organelles which would be considered to fall in the normal, healthy range.
If a biopsy was taken and the cells examined were much smaller than expected, we would conclude that these cells had shrunk, and would say that there has been some atrophy.
Now, if I asked you, what do you think causes atrophy?
You may be able to think of many examples. One might be the skeletal muscle atrophy that occurs, while a person is not able to use those muscles, either due to bedrest, or due to the restraint of wearing a cast when a bone is broken. Even astronauts that have been in space experience muscle atrophy as their muscles are not required to generate as much force in a low-gravity environment have The body is quite efficient and it is often a use-it-or-lose-it natural phenomenon that takes place, as the body remodels itself. Cells will reduce the expense of making muscle proteins (e.g. myosin, actin, troponin, tropomyosin) if they are not required, and skeletal muscle cells will shrink or atrophy as a result. At times it is quite visible. For instance when a cast is removed from an arm, comparisons to the non-casted arm, can show a noticeable difference in diameter. The recently casted arm may be smaller in diameter than that of the non-casted arm. Luckily in these 3 scenarios, skeletal muscle cells can build up their proteins and strength when the person begins to use that muscle again.
There’s actually at least 7 causes of skeletal muscle atrophy. In addition to the first 3 examples (bed rest, low gravity, casted), the 4th example would be caused by reduced neural input to your muscle. This occurs when there’s been neural damage, perhaps even as much as a spinal cord injury. If someone’s been in a car accident and they’ve had a spinal cord injury, perhaps it has resulted in becoming paraplegic or quadriplegic. In both of these instances, the nerves in their spine were severed and there is no longer neural input to their leg muscles. Without neural input, they can’t move their legs. As a result, their leg muscle cells start atrophying (again the body remodels to be efficient, and it is a use-it-or-lose-it phenomenon involved in maintaining skeletal muscle size). The net effect of this might become visible over time, and a person’s legs may become thinner in diameter.
The 5th example, which is unfortunately common in the world, is starvation or poor nutrition. In this instance, if a person is not getting enough dietary amino acids and other nutrients, the skeletal muscle cells (and in fact all of the cells of the body) will not have the building blocks needed for growth and maintenance and they might start atrophying. iskhein ‘keep back’ + haima ‘blood’
A 6th example would be: ischemia, a term that refers to poor blood flow. Ischemia originates from the Greek words ischein ‘hold back’ and haima ‘blood’. So let’s examine the instance when there’s not much blood flow to this muscle. It may be that the blood vessels are damaged or partially blocked with atherosclerotic plaque resulting in less blood flow. Reduced blood flow, means there is reduced nutrient and oxygen delivery, which means this cell can’t produce proteins and it can’t maintain itself at its proper size.
The 7th cause of atrophy, just a reduction in hormones. For example when people get older, their bodies produce less estrogen, less testosterone, less growth hormone, amongst other growth factors and hormones. As a result there is less cellular stimulation to produce and maintain proteins leading to noticeable atrophy of muscle, bone, and other tissues.
Now the reverse of atrophy, of course, is hypertrophy. I should point out that in biology the prefix, a- means ‘without’, and trophy means ‘growth’. The prefix hyper- means ‘more’, so hypertrophy refers to more growth, or bigger. In the above illustration, you can see that these 4 cells have grown in size.
Let’s now define the difference between physiologic hypertrophy and pathologic hypertrophy.
An example of physiologic hypertrophy occurs when a person starts an exercise program, perhaps going for a run every day, resulting in their leg muscles getting bigger and bigger. In this case, the skeletal muscles that are being used more frequently produce more muscle proteins (e.g. myosin and actin), and as a result the skeletal muscle cells’ diameters increase in diameter. Additionally these cells become stronger due to the increased number of myosin and actin cross-bridges that can form and build tension to lift load (or generate force). You may be aware there can be two very distinct types of exercise training: resistance and cardiovascular.
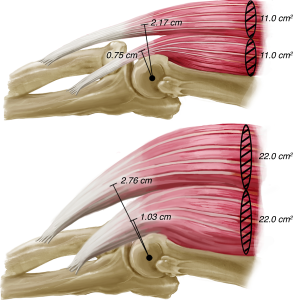
Some athletes that perform a lot of resistance training (e.g. weight lifting) at the gym and other athletes predominantly perform cardiovascular training (e.g. long distance running), and of course there are other individuals that do a mix of both types of activities (resistance and cardiovascular). In all instances, athletes that train frequently, will experience remodeling in their body that contribute to improved performance (e.g. faster times, greater weight lifts) over time. As mentioned, skeletal muscular hypertrophy of the specific muscles being used in these activities will occur. Additionally the heart muscle may also hypertrophy, with the walls of both left and right ventricles increasing in width and even increasing the diameter of the ventricular cavities. This heart remodeling is beneficial in athletes in that it helps to deliver more blood to the working tissues of the body per minute during exercise. Therefore these muscles will receive sufficient oxygen to support ATP production which is required for muscle activity.

In the above figure, if you look carefully the remodeling that occurs during resistance training is different than with cardiovascular (aerobic) training. With resistance training the ventricles don’t increase in their fill volume, but do increase ventricular wall thickness. The rationale is that the myocardium will be able to generate more pressure which will help send blood through that bodybuilder’s blood vessels. You can imagine that a body builder has bigger skeletal muscles that have increased in vasculature as well – to support the activity of these larger skeletal muscles. So the heart will have remodeled at the same time in order to push blood into a lot of blood vessels that are potentially compressed while lifting weights. So we would say, this is a nice, healthy heart for a bodybuilder. With the endurance runner, their myocardium thicken this, and the fill volume also increases. The rationale is that if the heart can send a larger volume through your blood vessels, it doesn’t have to beat quite as quickly which helps with reducing fatigue, which of course is important during 3 hour marathons. Notice in both hearts, that progenitor cells are activated, which means hyperplasia (increased cell number due to mitosis or cell division) is occurring and is contributing to the increased thickness of the ventricular walls. You’ll also notice that both conditions are reversible, meaning that if a person stops training and becomes sedentary, the cellular changes will reverse.
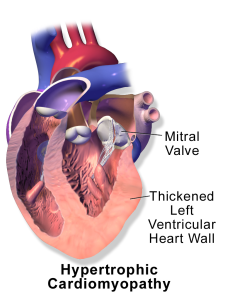
Now with pathologic hypertrophy, you might guess correctly that hypertrophy has occurred as a result of a disease. In this instance, the underlying disease is causing an organ to become larger. There could be several reasons for this phenomenon. There may be infiltration by a large number of immune system cells, or there may be inflammation (swelling or edema), or perhaps abnormal accumulations of inclusion bodies or vacuoles within the organ’s cells. In the case of heart disease and hypertension (high blood pressure), the heart’s ventricular muscles need to work harder, and to generate the increased force required to deliver blood flow. Perhaps there’s a lot of blood vessel damage through out the body and the heart has to push blood through these damaged vessels, which is much harder. Thus, the workload (for the heart) has gone up and the heart has hypertrophied in response. So it can be a sign of damaged blood vessels, or blood vessels full of atherosclerotic plaque, or even abnormally narrowed vessels, that can no longer dilate. In these instances, hypertrophy is not a sign of a healthy heart. In fact, the heart shape is no longer that beautiful cylinder shape that you would see with an athlete or normal, healthy person. The cylinder shape is very effective at pushing blood out of it. When a heart hypertrophies during heart disease, instead of a beautiful cylinder, it becomes more of a sphere. So even though the wall is thicker, the muscle itself becomes less effective and less efficient. It is not pushing blood nearly as effectively. It is a sign of deterioration and it’s a sign that the heart is not working as well and is under duress. In these instances, we would use the term pathologic hypertrophy, and instead of making a person more athletic (with larger cardiac output as in the case of physiologic hypertrophy), it is often a sign that this organ is starting to deteriorate.
Let’s go to the next term, hyperplasia. Can you tell what’s happened in the illustration? The cells are the same size as the cells depicted as normal, but there’s more cells, instead of four cells, now there’s eight. You can see that’s growth in cell number, there has been mitosis (or cell division). The suffix -plasis, comes from the Greek word meaning ‘formation’. As with hypertrophy, there can be both physiologic and pathologic hypertrophy.
So when would you see physiologic hyperplasia?
One example of physiologic hyperplasia, is in the growing that occurs during childhood (starting prenatally from fetus to embryo to baby to child to teenager to adult). The second example of physiologic hyperplasia occurs during pregnancy (in the growing of the uterus, abdomen, breasts, and other tissues which are designed to support the pregnancy and newborn).
When would you see pathologic hyperplasia?
Most example of pathologic hyperplasia, occur due to a disease that is causing an imbalance of growth hormones (which may be temporary). This can be rectified by treating the underlying disease or through use of medication that re-establishes hormones at normal levels. At times, pathologic hyperplasia occurs for other reasons. Sometimes pathologic hyperplasia results in the formation of a benign tumour. If this tumour is pressing on tissues and causing negative clinical manifestations, it may be surgically removed.
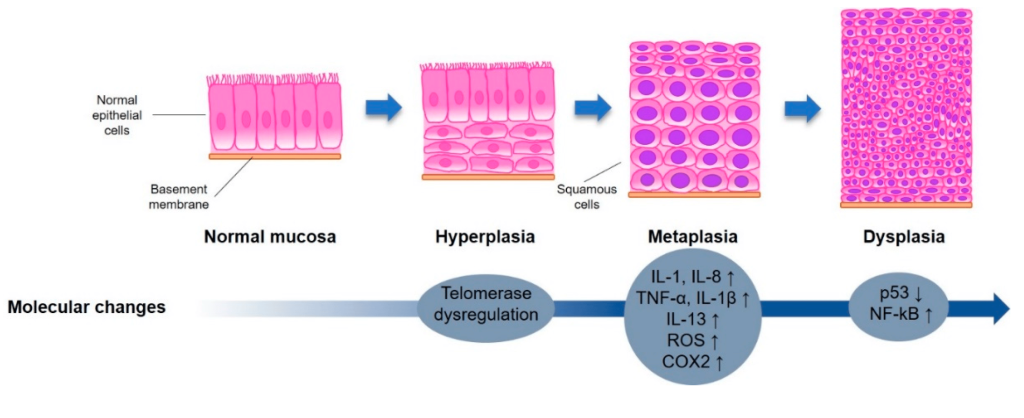
Let’s go to the next term, metaplasia, originating from the Greek words for ‘change form’. In the above figure, the cells have become more round, to illustrate a type of change in structure/form. Within the human body, we see metaplasia occur in the trachea (windpipe) of smokers. Prior to metaplasia, the trachea consists of a healthy single layer of tall ciliated cells. This tissue is therefore composed of simple, pseudostratified, columnar ciliated epithelial cells. This tissue contains Goblet cells that secretes mucus in order to trap pathogens and debris, to prevent that material from entering (and potentially damaging) the lungs. The cilia are going to sweep the mucus containing any debris upwards to eventually be swallowed sending that material to the stomach for destruction and removal. Now if you’re a smoker and these cells in the trachea are being perpetually damaged, the tissue remodels itself to become more robust and resilient. The simple columnar ciliated cells replace themselves with multiple layers of squamous cells now, in a tissue we would call stratified squamous epithelium with no cilia and fewer Goblet cells. As a result the tracheal wall becomes more resilient to smoke, but is also less functional. This tissue is less functional because the cells are not producing the mucus as they should and they don’t have the cilia. So if you’ve got a long-term smoker, you might find they get a smoker’s cough because you now need to use coughing to try and clear the debris and mucus out of the trachea. Metaplasia is thought to be reversible if the source of irritant is removed.
The next term, dysplasia, with the prefix dys– in Greek meaning bad, so altogether the word dysplasia referring to ‘bad growth’. In the above figure, you can see these cell shapes are changing are the cells themselves are becoming less functional, becoming de-differentiated (more immature). This type of change potentially makes a cell pre-cancerous. As a cell becomes less and less differentiated (mature), it becomes more and more likely to resume cell cycling (mitosis). Cells that continually go through mitosis are not mature, and not functional, and of course, continue to produce more and more cells.
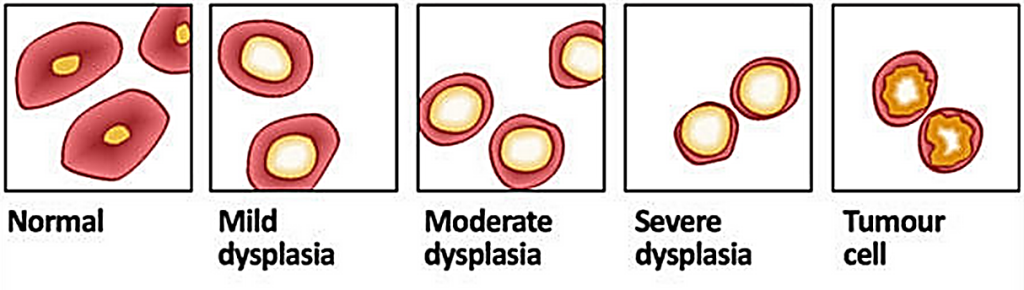
If dysplastic cells do enter this stage of continually cycling, we would refer to them as anaplastic, and the growth and accumulation of a mass of new cells would be called a neoplasm ‘new growth” or tumour, which may be benign (non-cancerous) or may be malignant, cancerous (metastatic, capable of spreading and infiltrating other tissues and organs). Anaplastic cells are often immortal, and have entered a state of uncontrollable cell division. Malignant cells are capable of breaking through basement membranes (shown in blue in the figure below) and spreading to neighbouring tissues.

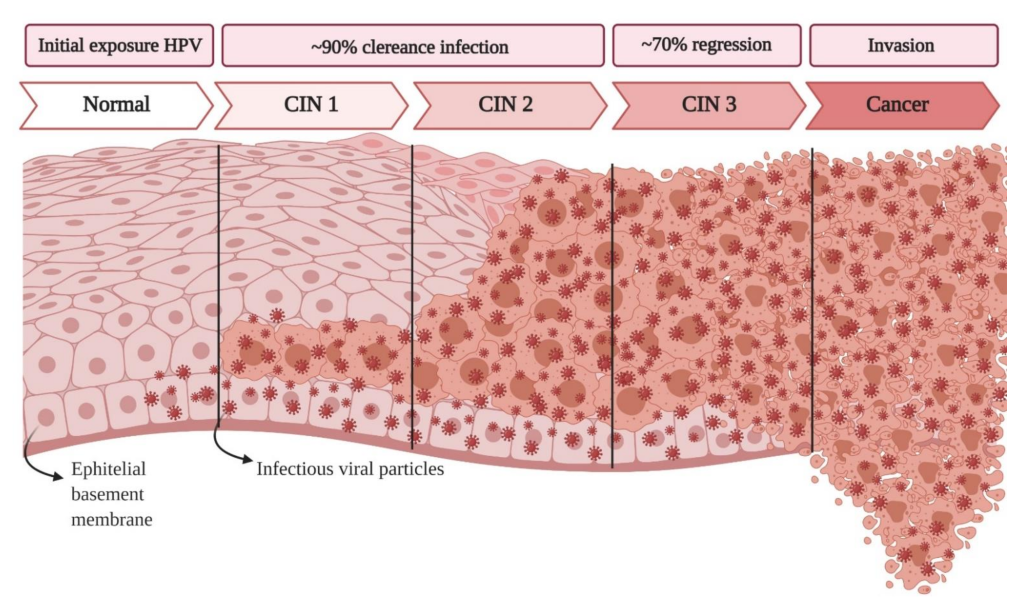
Tumour Types: Benign (non-cancerous) and Malignant (cancerous)Cells typically become dysplastic due to a particular type of irritant (e.g. cigarette smoke, pollutants, some viruses, UV and radiation exposure) that has led to either DNA mutations, or changes in gene expression. If the irritant is removed, and normal gene expression resumes, the cells may revert from dysplastic back to normal. However, if further more permanent changes in gene expression occur due to more irritation causing further DNA mutations which can no longer be compensated for, the dysplastic cells may become anaplastic (completely de-differentiated, non-functional, and continually cell cycling). As mentioned earlier, these anaplastic cells may give rise to either a benign neoplasm or a metastatic (or malignant) neoplasm. The progression of morphological changes that occur as a cell cancer is illustrated below. Carcinoma in situ is depicted as pre-malignant as the basement membrane is still intact. Most carcinomas in situ eventually progress to become malignant carcinomas.
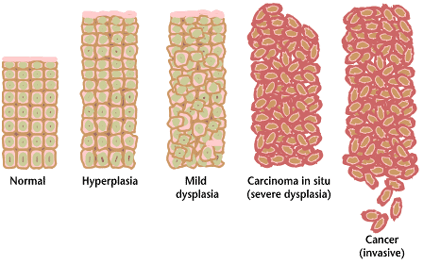
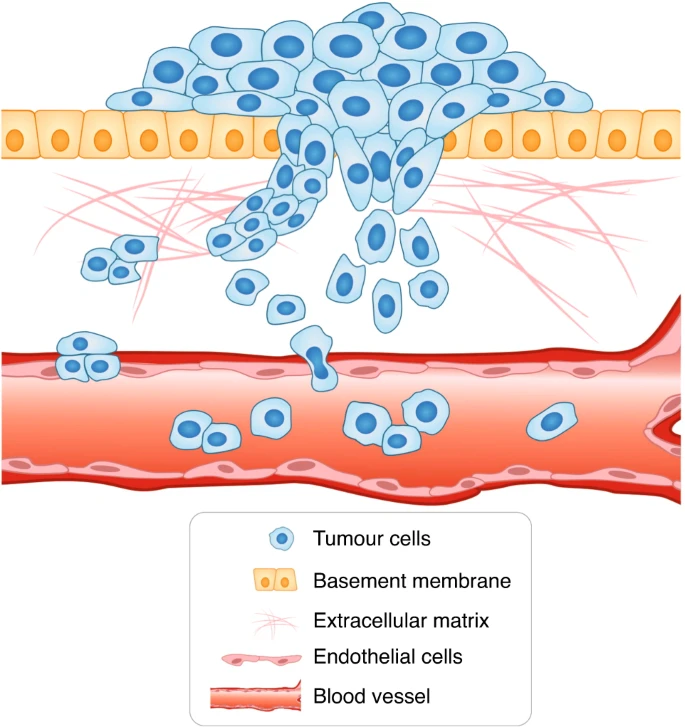
Once malignant cancerous cells have broken through the basement membrane they can enter the blood or lymph vessels and spread to distant sites in the body infiltrating tissues and developing into secondary cancers. If untreated this can lead to the failure of multiple organs.
Let’s look at three examples using these terms (hyperplasia, metaplasia, dysplasia):
1. It is known that smoking causes irritation to cells within the respiratory tract and that it is the leading cause of lung cancer, in addition to being a risk factor for other cancers.
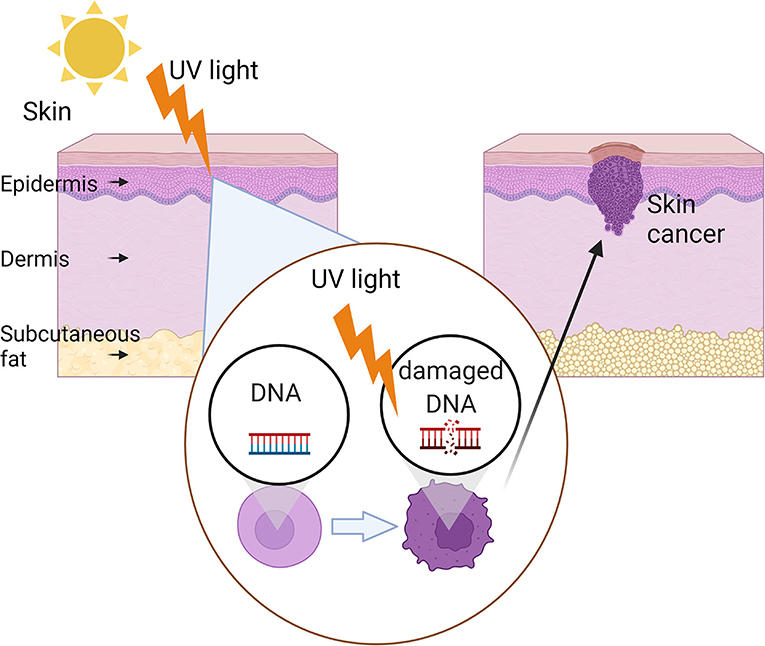
2. It is known that Ultraviolet light (UV) causes DNA mutations within skin cells, and is the leading risk factor for the most common forms of skin cancers (e.g. basal cell carcinoma, squamous cell carcinoma, and melanoma).
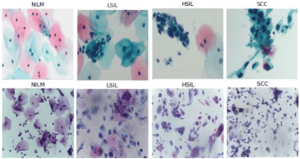
3. There are many strains of Human Papilloma Virus, HPV, some of which are known to be risk factors for the development of cervical cancer, some of which cause warts on the skin (including genital warts). Some strains (types) of HPV are therefore termed oncoviruses (a virus that can cause cancer). As a preventative measure for cervical cancer, in Canada, the HPV vaccine is available for youth. HPV is transmitted by skin-to-skin contact as well as sexually, ideally the vaccine is given to all youth prior to sexual activity, which increases risk of viral exposure. HPV is also linked to penile cancers and cancers of the mouth, throat, anus and vagina. With all cancers, we know that early detection makes for a better prognosis and better chance of recovery. To ensure early detection, in Canada, it is recommended that abnormalities in the mouth, throat, anus, vagina and penis are reported to the physician early. The cervix (entrance to the uterus) is more difficult to self examine. In this case, it is recommended that once individuals become sexually active that they have regular Pap smears (tests) done in which cervical cells are swabbed or scraped, sent to a lab to be looked at under the microscope. The lab technicians that perform this test are looking at the cellular morphology of the these cervical epithelial cells to see if any dysplasia or anaplasia has occurred. A physician’s recommendations on the frequency of Pap smear tests, should be followed, which is usually every 2-3 yrs. The Pap test is named after the physician that discovered this test in 1923, Georgios Papanikolaou. Pap tests may be full automated in the future and/or replaced with HPV testing as tests evolve and improve.
Let’s take a look at cervical cells from various Pap tests to illustrate the change in morphology that occur.
TEDEx How to Hack HeadLines – Fake medical news or real?
What is healthium? Does it reduce cholesterol?
Does chocolate reduce stress?
How do you make sure news about medical research is believable? Ask yourselves these questions:
Has the research been submitted for peer-evaluation? Has the research been found to be reproducible? Was a large enough sample size (# of people) used to ensure robust statistical analysis is possible?
What is that actual difference? Is the difference/cure/alleviation of symptoms statistically significant? Were there negative side effects?
Has this been proven to be a short-term effect or long-term effect? How long?
Was the study double blind? Has it been reproduced by another research team? Was this study done in humans or mice or fish etc.?
Media Attributions
- A634998 is licensed under a CC BY-NC-SA (Attribution NonCommercial ShareAlike) license
- fresco-with-wounded-aeneas-3854
- The normal synchronous relationships between sleep and daytime activity and cortisol
- three-doctors-attend-a-man-with-the-plague-12034 is licensed under a CC BY-NC-SA (Attribution NonCommercial ShareAlike) license
- 4 Stages of Infection © Christy Bowen, Lindsay Draper, Heather Moore is licensed under a CC BY (Attribution) license
- Private: Different cell types & differentiation © OpenStax is licensed under a CC BY (Attribution) license
- Neglected Tropical Diseases © Rachel Cotton is licensed under a CC BY-NC-SA (Attribution NonCommercial ShareAlike) license
- Non-neoplastic_changes.svg © Dennis Hansen is licensed under a CC BY (Attribution) license
- fig-3-full © Vigotsky AD, Contreras B, Beardsley C. is licensed under a CC BY (Attribution) license
- Exercise-induced_cardiac_growth_-_Cardiac_remodeling_from_Aerobic_and_Resistance_exercise © Kyle Fulghum, Bradford G. Hill is licensed under a CC BY-NC-SA (Attribution NonCommercial ShareAlike) license
- Blausen_0166_Cardiomyopathy_Hypertrophic © Blausen Medical Communications is licensed under a CC BY (Attribution) license
- 5971147bf2f20018315cd3b0_figure-2[1]crop
- Tumor_Types_MTK © WolfpackBME is licensed under a CC BY-NC-SA (Attribution NonCommercial ShareAlike) license
- Cancer_progression_from_NIH is licensed under a Public Domain license
- Metastasis © Novikov, N.M., Zolotaryova, S.Y., Gautreau, A.M. et al is licensed under a CC BY (Attribution) license
- Metaplasia, Dysplasia Lung © Ashraf-Uz-Zaman, M.; Bhalerao, A.; Mikelis, C.M.; Cucullo, L.; German, N.A. is licensed under a CC BY-SA (Attribution ShareAlike) license
- UV skin cancer © Breen I and Richmond J is licensed under a CC BY (Attribution) license
- HPVcervicalcancer © Causin, R.L.; Freitas, A.J.A.d.; Trovo Hidalgo Filho, C.M.; Reis, R.d.; Reis, R.M.; Marques, M.M.C. is licensed under a CC BY (Attribution) license
- Cervix © Henry Vandyke Carter - Henry Gray (1918) is licensed under a Public Domain license
- Pap Test © Karasu Benyes, Y.; Welch, E.C.; Singhal, A.; Ou, J.; Tripathi, A. A is licensed under a CC BY (Attribution) license
