Chapter 4 Selected Musculoskeletal Disease and Disorders, including Trauma and Rheumatic Disorders
Osteoarthritis, Rheumatoid Arthritis, and Gouty Arthritis
Pictures coming soon!
Zoë Soon
Arthritis:
As the names suggest, all 3 diseases (osteoarthritis, rheumatoid arthritis and gouty arthritis) are depicted by inflammation within articulations (most often within synovial joints).
Osteoarthritis:
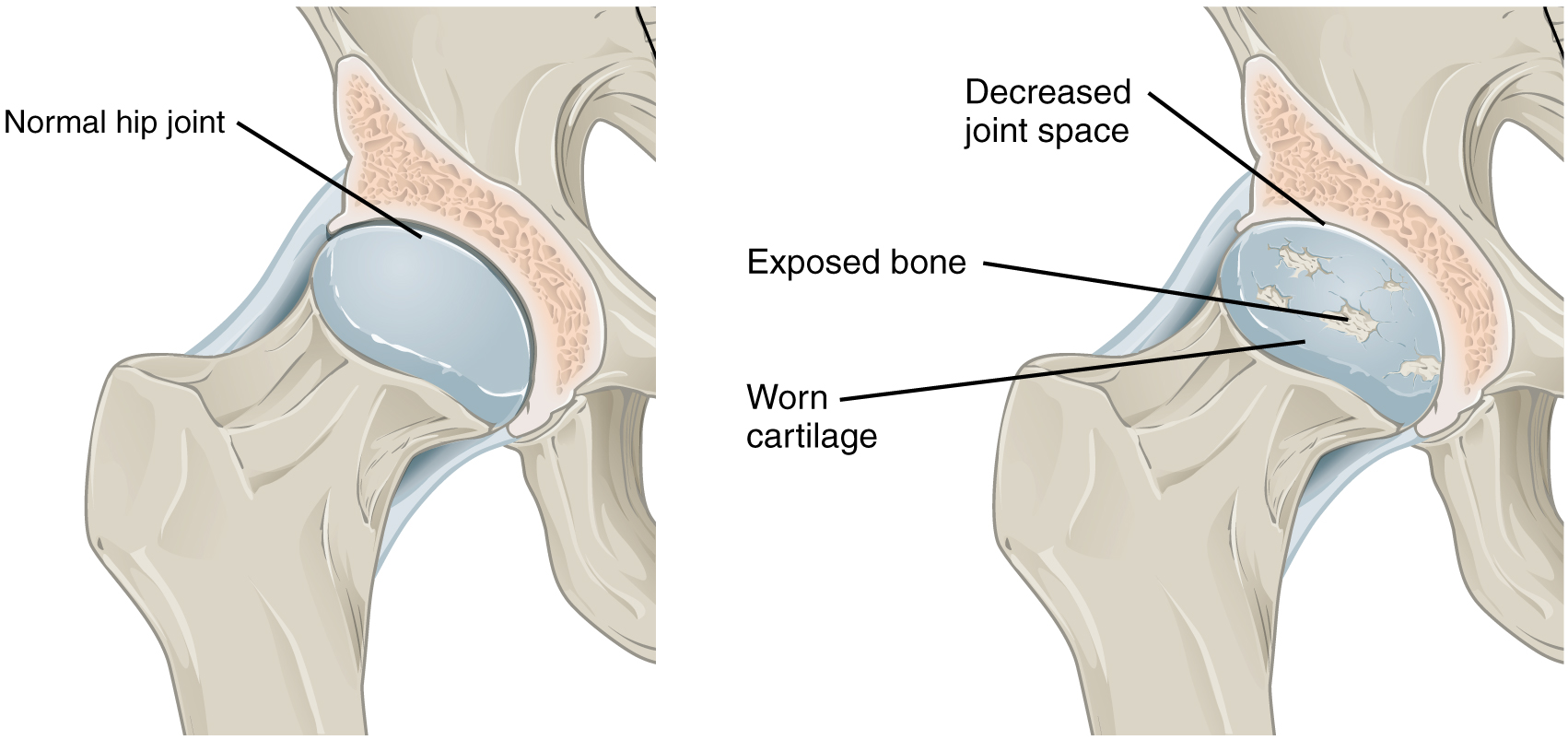
In the case of the most common joint disease, osteoarthritis, the degenerative loss of articular (hyaline) cartilage is associated with aging and wear and tear. Unfortunately, osteoarthritis is a source of chronic disability for millions of people worldwide. Approximately 4 million (>13%) Canadians and more than 30 million Americans have osteoarthritis, with over 50% of older adults affected.
Risk Factors – Osteoarthritis
Besides age, other risk factors include previous joint tissue damage due to trauma or infection. Genetics (e.g., genes that affect collagen levels), family history, obesity, repetitive use during heavy labour, reduced levels of sex hormones, reduced circulation, and diabetes mellitus. Biological females are more susceptible to osteoarthritis especially in knee and hand joints.
Prevention strategies involve daily physical activity and maintenance of healthy weight, following national food guides and adhering to nutritional guidelines, as well as controlling diabetes mellitus and other risk factors.
Signs and Symptoms – Osteoarthritis
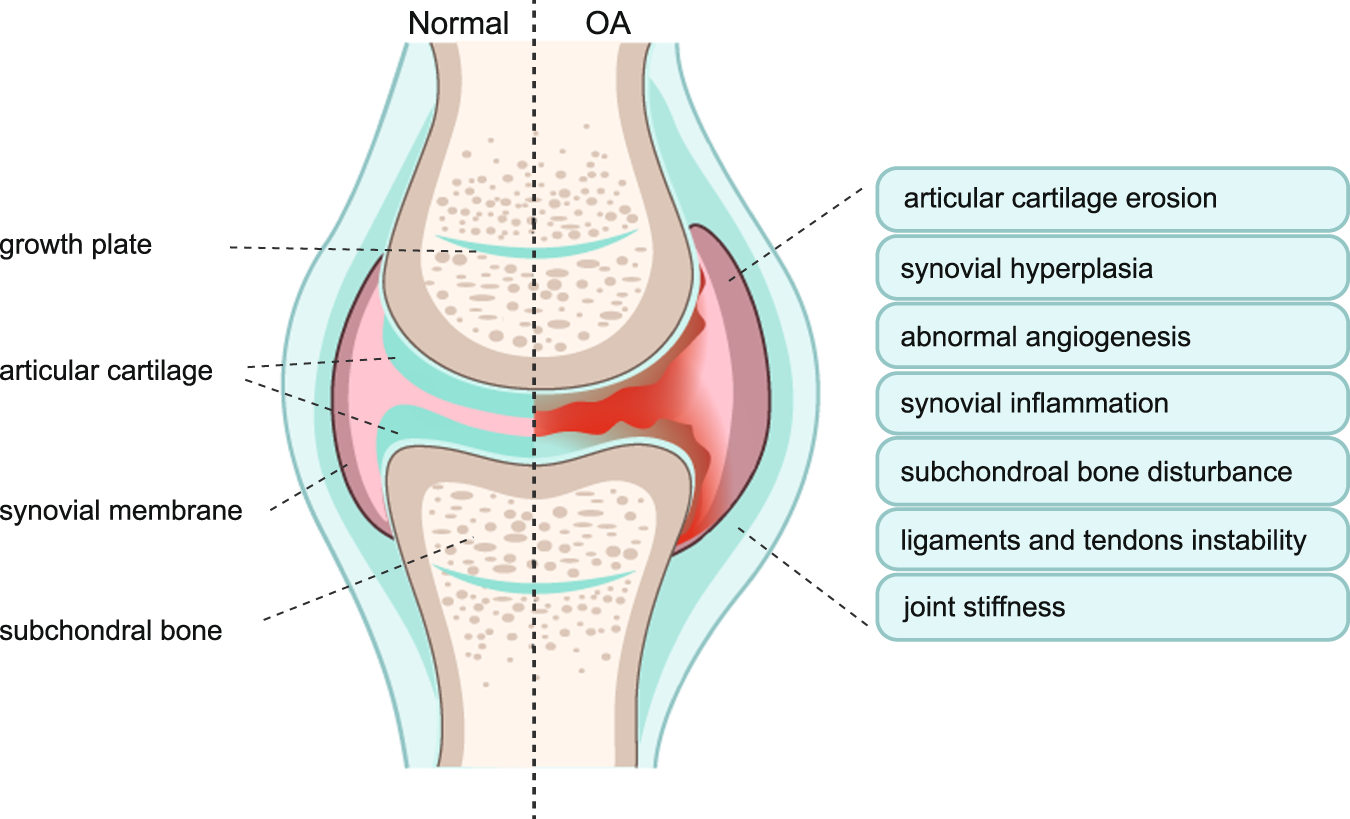
The signs and symptoms include: joint pain, swelling, stiffness, crepitus, and limited range of motion. Although historically, osteoarthritis was considered non-inflammatory, analysis of synovial fluid and the cartilage have revealed pro-inflammatory cytokines and other signs of inflammation.
Most often osteoarthritis affects the knees, hips and hands, though the weight-bearing lumbrosacral vertebrae and feet joints can also be affected. Typically, osteoarthritis develops bilaterally.
As the cartilage deteriorates, it is replaced by bony spurs, which can lead to pain, and more limited range of motion. With pain and stiffness, a limp and/or predispositions to falls can develop.
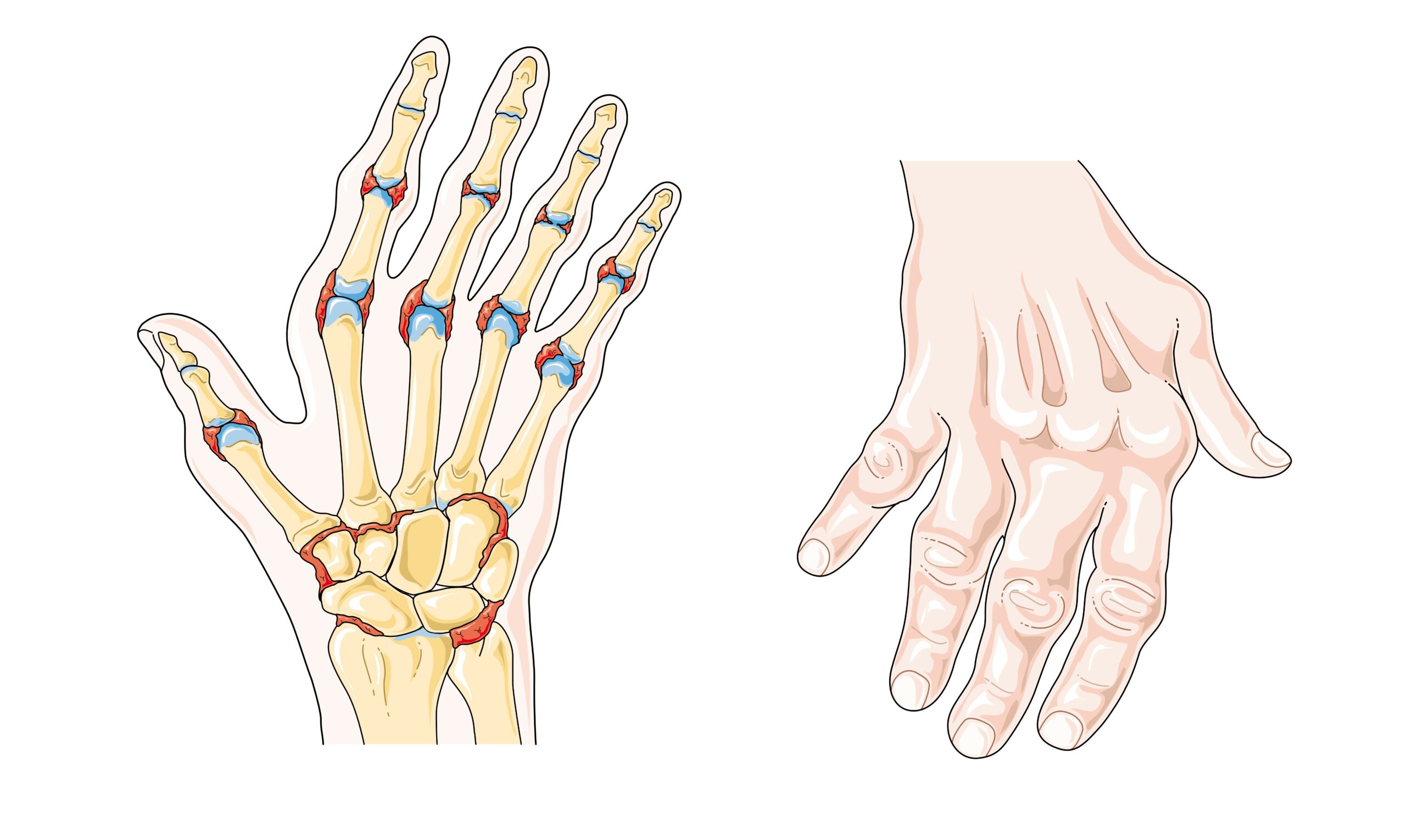
In the case of osteoarthritis of the hand enlarged finger joints (knuckles) can also lead to difficulties in putting on rings or taking them off. Enlarged distal interphalangeal joints are called Heberden nodes, whereas enlarged middle interphalangeal joints are termed Bouchard’s nodes. Heberden nodes develop more frequently in biological females in comparison with biological males.
Not only do bony spurs (osteophytes) develop, but loss of cartilage leads to joint space narrowing as well as subchondral bone degeneration with the development of cysts. Should the osteophytes break loose, they become “joint mice” which can further limit range of motion and cause additional pain, damage, and crepitus. The term osteophytosis refers to the development of bone spurs in joints.
Diagnosis – Osteoarthritis
Typically, diagnosis of osteoarthritis involves imaging (e.g., x-rays, CT scans, MRI, ultrasound, bone scans), often to rule out other causes of the signs and symptoms experienced (e.g., osteomyelitis, bone cancer, or tears in the meniscus, tendons, or ligaments). At times arthrocentesis is used, and the synovial fluid is checked for signs of inflammation and infection.
During diagnosis, osteoarthritis may be staged as involving: a) the surface, b) partial-thickness, or c) full-thickness without and then with subchondral bone damage and/or cysts. This illustrates the pathogenesis of the disease, which can involve:
- The thick smooth articular cartilage erodes releasing proteoglycan and collagen fragments into the synovial fluid
- Fibrillations (deep, long fissures) develop in the articular cartilage
- Osteophytosis
- Subchondral bone remodelling with areas of sclerosis (that have irregular thickening and increased bone density) areas that become cysts
- Fibrosis of the articular capsule surrounding the joint occurs
- Synovitis develops and joint space narrows
- Irritation of joint capsule sensory nerve endings and pain due to increased pressure, pro-inflammatory cytokines,
Treatment – Osteoarthritis
Treatments involve both non-pharmacological and pharmacological interventions as well as surgical interventions.
Non-pharmacological interventions include: physical therapy, prescribed (often low-impact) exercise, and weight loss if and individual has excess weight that is contributing to joint deterioration and/or pain. The use of warm and cold compresses can be helpful as can the use of orthotics in footwear. At times, canes and braces are used to provide support.
Medications that are prescribed can include NSAIDs, acetaminophen, and glucocorticoid injections.
Surgeries are performed using arthroscopy arthroplasty (joint replacements), and joint fusion. Arthroscopy can be used to remove loose articular cartilage, meniscus tears, and other loose bodies. Arthroplasty involves removal of joint surface and inserting metal and plastic prothesis that can be anchored in place with bone cement or bone ingrowth into porous coating of prothesis. Joint fusion involves uniting bones on either side of the joint, which can be helpful removing pain, but limits motion. Surgery carries the (usually small) risk of infection and formation of thrombi (blood clots) and emboli.
Complimentary therapies such as physical therapy, massage therapy, and acupuncture are sometimes utilized.
Rheumatoid Arthritis:
Rheumatoid arthritis (RA) affects approximately 1% of the population and is thought to be caused by an autoimmune disease, that results in progressive damage to joints. In addition to causing chronic inflammation and deterioration of the affected joints, vasculitis, pericarditis, and at times damage to the lungs, heart, eyes, and skin can occur.
Risk Factors – Rheumatoid Arthritis
Genetics are thought to account for 50% of the risk for developing RA, specifically the inheritance of certain alleles (or variations) of the Major Histocompatibility Complex (MHC) genes. Another major risk factor for developing RA is biological sex. It is unclear why RA affects approximately 3 times as many biological females as males, though differing levels of sex hormones are thought to be a contributing factor. This is theory is potentially supported by the fact that pregnancy and even for 1-5 years post-partum can result in a remission (relapse of symptoms). The role of sex hormones on the immune response has been under investigation for some time. Other risk factors include previous infections (e.g., Epstein-Barr Virus, EBV), trauma, as well as smoking. There are dietary risk factors as well including alcohol consumption. Healthy lifestyle, on the other hand, has been associated with the lower risks of developing RA.

Pathogenesis – Rheumatoid Arthritis
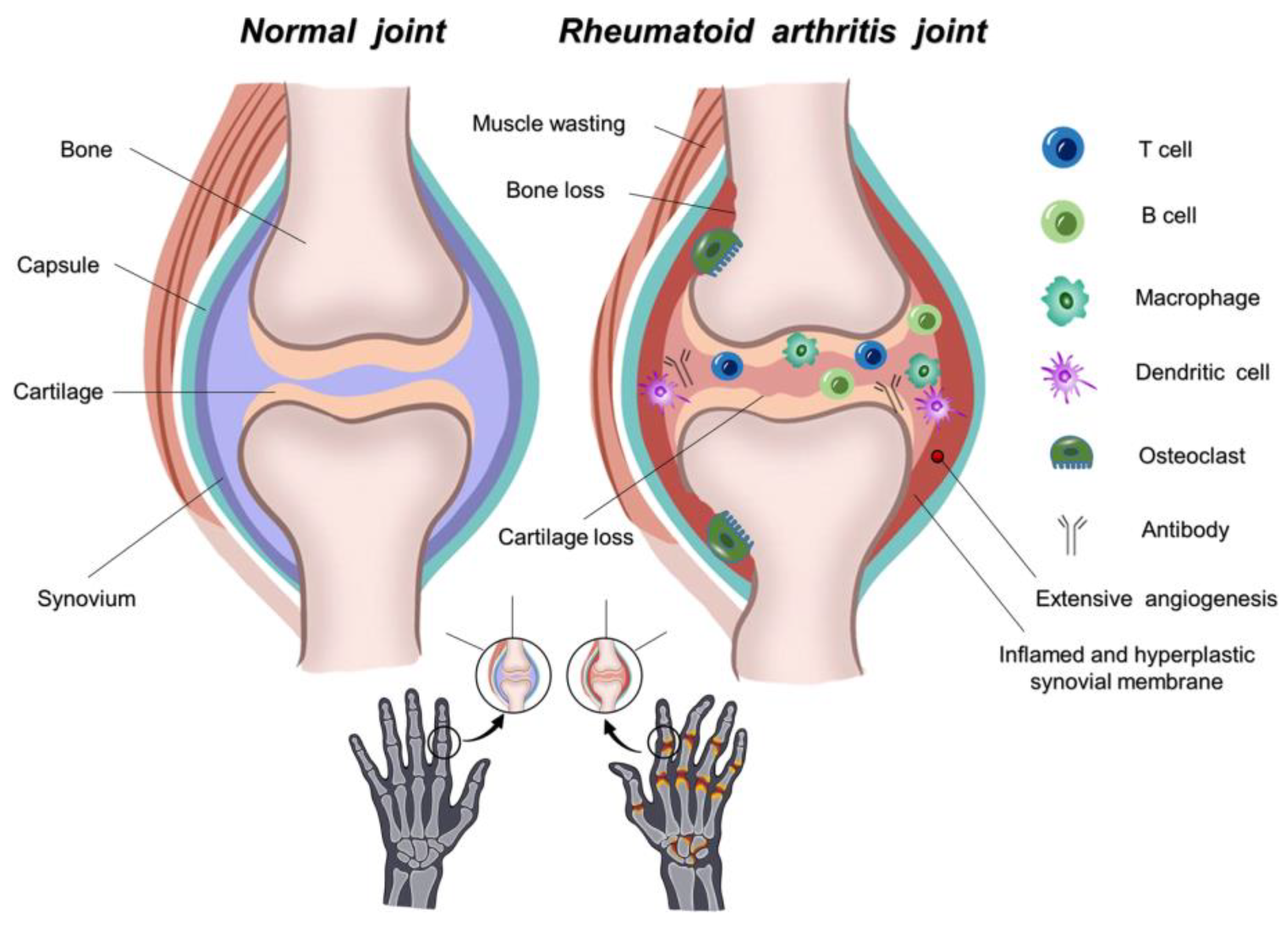
RA begins when the body’s immune system starts to recognize and launch an attack against self-antigens within its own synovial joints. Both activated T and B lymphocytes are involved and B cells produce autoantibodies (termed Rheumatoid Factors, RFs) that target the joint for destruction. 40% of patients also develop antinuclear antibodies (ANA). Macrophage production of pro-inflammatory cytokines increases the inflammation and chronic destruction within the joint. Synovitis occurs with cell proliferation creating an inflamed thickened synovial membrane. The formation of pannus (fibrovascular tissue or granulation tissue) containing new connective tissue and tiny blood vessels occurs over portions of the joint surface. Articular cartilage erodes. Progressive damage of cartilage, bone, tendons and ligaments occurs. Fibrous (scar) tissue may form and calcify within the joint space. If this calcified fibrous tissue crossed the joint space and bridges the two bones, joint fixation, loss of range of motion as well as joint deformity may develop if not treated. The term ankylosis is used in this type of instance to describe the fusion of bones resulting in joint immobility. Vasculitis can develop anywhere in the body, but may be seen in the skin in the form of purpura (small red-ish spots due to small blood vessel leaks). Vascular damage makes an individual more prone to atherosclerosis, myocardial infarction and stroke (i.e., cerebrovascular accident, CVA). Lung inflammation and fibrosis may also occur.
Signs and Symptoms – Rheumatoid Arthritis
Signs and symptoms have an insidious onset and include: symmetrical, swollen, painful, stiff joints most often in the hands, knees, hips and feet as well as fatigue, malaise and sometimes fever. There can be periods of relapse and exacerbation. As joints are damaged, deformities in the hands begin to appear (e.g., boutonnière and swan neck deformities). RA can lead to osteopenia or osteoporosis which put one at risk for vertebral compression fractures and hip fractures. Other signs and symptoms include the development of subcutaneous nodules that might be seen in the skin on hands, elbows, etc. Unfortunately, as this disease progresses, individuals can begin to have difficulty performing daily activities and approximately 40% of individuals become disabled. Early treatment is recommended to offset and slow down the progression of the disease.

Diagnosis – Rheumatoid Arthritis
Rheumatoid arthritis is diagnosed based on patient history, physical examination of involved joints, imaging (e.g., x-rays, ultrasound), and blood tests. Imaging can reveal destruction of cartilage, bone, tendons and ligaments. Blood tests often reveal inflammation through elevated levels of Erythrocyte Sedimentation Rate (ESR) and C-reactive protein (CRP). Blood tests and analysis of synovial fluid reveal high levels of RF.
Treatment – Rheumatoid Arthritis
Treatments include: hot and cold compresses, therapeutic exercises, the use of orthotics, glucocorticoids, NSAIDS, Disease-Modifying antirheumatic drugs (DMARDs) and various surgeries as required. Surgery options such as synovectomy, tendon realignment, and arthroplasty (joint replacement) are performed as necessary. Often individuals are treated with immunosuppressive drugs (e.g., DMARDs) which puts them at greater risk for infections.
Non-pharmacological treatments include: physical therapy, prescribed (often low-impact) exercise, and weight loss if and individual has excess weight that is contributing to joint deterioration and/or pain. At times, canes, braces and other assistive devices are used to provide support.
Gouty Arthritis:
Gouty arthritis is caused by the build up of uric acid crystals within joints causing irritation and inflammation.
Pathogenesis – Gouty Arthritis
Purines such as adenine and guanine are nitrogenous bases that have several roles in human cells. For example, adenine and guanine form two of the four nucleobases used to make deoxyribose nucleic acid (DNA). Adenine and guanine are also used to make high energy fuel molecules, adenosine triphosphate (ATP) and guanine triphosphate (GTP). Purine turnover occurs naturally in all nucleated cells. The breakdown of purines (purine metabolism) produces the waste product, uric acid, which enters the bloodstream and then is removed from the blood stream by the renal nephrons (of the kidneys). If uric acid isn’t eliminated quickly enough (in the form of urine), either due to inefficient elimination (in 90% of cases) or due to overconsumption of purines (<10% of cases), then uric acid can build up in the blood stream which is termed hyperuricemia.
Consuming large amounts of purine-rich foods (e.g., anchovies, sardines, organ meats) or purine-rich beverages (beer, hard liquor) puts a person at risk for hyperuricemia.
Hyperuricemia pre-disposes to the accumulation of uric acid crystals in synovial fluid, as well as in skin, cartilage, tendon, ligament, and kidney. Within joints, accumulations or urate crystals form microtophi and then larger tophi. Often this occurs over a long stretch of time 10-20 years, before tophi and signs and symptoms of gout develop (most commonly at 30-60 years of age).
A tophus is a subcutaneous hard nodule filled with uric acid crystals that is surrounded by a zone of inflammation and is visible in the affected joints. The uric acid crystals are irritating to cells in the region including macrophages which trigger an immune response. Activated neutrophils migrate to the area releasing inflammatory compounds that cause pain and deterioration of the joint if not treated.
Strangely, there is a seasonality to gout flares with spring and summer being peaks times of year which correlates with cortisol levels dropping and levels of neutrophils increasing. This may not be a coincidence due to the inflammatory role of gout flares. Interestingly not everyone with hyperuricemia develops gout, there appears to be genetic susceptibilities involved as well as differences in gut microflora (and the metabolism of urate by gut flora).
Risk Factors- Gouty Arthritis
Risk factors for gout include: genetics (and therefore family history), alcoholism, diet, obesity, biological sex, and age. It has been found that estrogen provides biological females with a uricosuric effect (i.e., estrogen promotes the secretion and elimination of uric acid by nephrons). Therefore, biological males are more at risk for gout than pre-menopausal females, as are individuals that have a diet high in purine-rich foods (e.g., meat and seafood) or drink (e.g., beer and hard liquor). Chemotherapy treatment is also a risk factor as there is an increased breakdown of cellular DNA. Other risk factors include diabetes, hypertension, kidney disease, use of diuretics, and age (post-menopausal for females).
Signs and Symptoms- Gouty Arthritis
While the development of tophi within joints can take a long time (10-20 years), the pain and inflammation that suddenly occurs is acute, displaying all of the signs of inflammation warmth, redness, swelling, and pain that is usually extreme. Frequently the big toe joints are affected, though other joints can also be affected as well (e.g., ankle, wrist, finger, and knee are among the more common ones). Inflammation of the proximal big toe joint was termed podagra by the Ancient Greeks which translates as “foot-grabber” which now may a good way to remember the unpleasant pain associated with gout. The swelling can limit range of motion and be accompanied by fever. As hyperuricemia also puts one at risk for kidney stones, signs and symptoms of renal calculi (kidney stones) may occur at the same time (or before or after).
Diagnosis- Gouty Arthritis
Diagnosis typically involves physical examination and aspiration of synovial fluid to analyze for monosodium urate crystals and rule out other causes of inflammation and pain (e.g., infection). Blood and urine tests can be performed as well to determine the levels of urea and uric acid in the blood and urine. X-rays can be used to assess any erosions of bone or cartilage in addition to any changes in joint space. Ultrasound can be used to detect signs of crystal formations and bone erosion.
Treatment- Gouty Arthritis
Treatment often involves treating the joint that is affected as well as taking steps to avoid future episodes. Pharmacological treatment may include: NSAIDs, glucocorticoids, and other medications.
Typically, surgical removal of tophi only occurs, when infection, joint deformity is present as other interventions (medications) lead to better outcomes and faster healing.
Lifestyle changes are often recommended which include reducing consumption of high-purine foods, alcohol, high-fat foods, sugary foods, sugary drinks, and increasing levels of water intake to approximately 8 glasses of water per day. Establishing a healthy weight and diet coupled with daily physical activity is recommended.
Arthritis Summary
Key Take Aways – Specific Learning Objectives Study Guide
Osteoarthritis:
an inflammatory joint disease due to “wear and tear”, most often affecting hips and knees
- obesity
- biological males; 40+yrs; biological females 55+yrs
- history of auto-immune disease (e.g. Rheumatoid Arthritis, Lupus, Ankylosing Spondylitis)
- physical/psychological trauma, or chronic pain
-
Joint pain that is relieved when joint is rested
- Heberden nodes in distal finger joints = thickening of subchondral bones (sclerosis = ↑ bone density)
- Bouchard nodes in middle joints of fingers = ditto (thickening of subchondral bones (sclerosis = ↑ bone density)
-
articular cartilage degenerates, and fibrillation (deep long fissures in articular cartilage occur),
-
joint capsule thickens, becomes fibrotic and sticks to deformed underlying bone narrowing joint space, limiting ROM, causing:
-
pain & stiffness, swelling, paresthesia (e.g. numbness), stiffness, creaking, limp, predisposition to falls, joint deformation.
- irritation of many sensory nerve endings in joint capsule
- Bone spurs (osteophytes) form & can break off (“joint mice”) into synovial cavity & irritate synovial membrane causing synovitis; subchondral cysts form; exudate buildup
Treatment: rest, orthotics, ROM exercises, physio & massage therapy, optimizing BMI may involve loss of excess body fat through healthy diet and exercise, pain & anti-inflammatory meds, possible surgery if deformation, excess pain and/or loss of mobility (hip & knee replacements are common), acupuncture, canes, hand braces.
Rheumatoid Arthritis:
A chronic, systemic, inflammatory auto-immune disease causing joint swelling, tenderness, destruction of synovial joints leading to disability & premature death.
Risk Factors:
- age (young adult onset is most common)
- genetics (specific HLA antigens)
- biological female
- smoking
- possible T cell defect in telomere repair
- prior viral infection resulting in cross-affinity to self antigens
- imbalance of chemokines involved in triggering an immune response
- long-term exposure to antibodies.
Signs & Symptoms: joint pain and inflammation, stiffness, joint deformation
Pathophysiology: Inflammation spreads to articular cartilage, fibrous joint capsule, surrounding ligaments & tendons
Most common in fingers, feet, wrists, elbows, ankles, knees; also shoulders, hips, cervical spine (lungs, heart, kidneys, & skin).
-
Synovitis – marked inflammation, cell proliferation
-
Pannus – made of granulation tissue = new connective tissue with tiny blood vessel that typically forms in a wound during the healing process; but in this case healing doesn’t occur and it spreads
-
Cartilage erosion – creates unstable joint
-
Fibrosis (scar tissue) – calcifies and obliterates joint space
Possible Complications:
-
Ankylosis – joint fixation and deformity develop if untreated
-
Atrophy of muscles
-
Bone alignment shifts (Ulnar drift, deformation and swanning of fingers); Boutonniere deformity
-
Muscle spasms due to inflammation/pain
-
Contractures and deformity develop.
-
Flare-ups associated with anemia (e.g. iron-deficiency)
-
More prone to lung fibrosis, atherosclerosis, MI, and stroke
- Chronic anti-inflammatory use can cause bleeds
Diagnostic Tests: Appearance of auto-antibodies (Rheumatoid Factors, RF) in blood tests, imaging, ↑ESR (faster Erythrocyte Sedimentation Rate), ↑CRP (increased C Reactive Protein levels in blood), presence of Anti-Nuclear Antibodies (ANA) in blood
Treatment: anti-inflammatory drugs, disease-modifying antirheumatic drugs, supportive care, cessation of smoking, healthy diet
Gouty Arthritis:
A chronic inflammatory arthritis, characterized by hyperuricemia and the formation of urate crystals in joints causing joint swelling, tenderness, destruction of synovial joints which can lead to disability as well a chronic nephropathy.
- biological males >40yrs
- sedentary lifestyle
- low fluid intake and/or use of diuretics
- low intake of fruits containing vitamin C
- high meat (purine-rich) diet (sometimes called the “rich man’s disease”, as high meat consumption is a risk factor, particularly shrimp, lobster, liver, kidney and red meats such as pork and beef)
- alcohol (beer, wine, spirits)
- obesity
- family history, genetic susceptibilities
- chemotherapy
- consumption of sweetened beverages and foods containing high-fructose corn syrup
Signs and Symptoms:
-
Acute gout flares due to tophaceous deposits (tophi) of urate crystals in joints.
-
Gout is associated with co-morbidities such as hypertension, diabetes mellitus, ischemic heart disease, congestive heart failure, metabolic syndrome, chronic kidney disease, and obesity.
- Most people with asymptomatic hyperuricemia do not develop gout.
Pathophysiology:
-
Results from deposits of uric acid and crystals in the joint, causing inflammation, leukocytosis and sometimes fever.
-
Uric acid & crystal formation resulting from any combination of the above risk factors, which may also include inadequate renal excretion of uric acid.
- Formation of tophus – large, hard nodule of urate crystals
-
Tophi cause local painful inflammation and occur after the first attack of gout.
-
Tophi can be found in cartilage, bone, joints, tendons and even skin, though predominantly within articular and subcutaneous regions.
-
Tophi can cause erosion of bone and joint tissues, and synovial fluid becomes yellow and cloudy.
- Joint damage can cause joint deformities and osteoarthritis; additionally urate nephropathy and conjunctivitis can occur.
Media Attributions
- Osteoarthritis © openstax is licensed under a CC BY (Attribution) license
- Osteoarthritis © Qing Yao, Xiaohao Wu, Chu Tao, Weiyuan Gong, Mingjue Chen, Minghao Qu, Yiming Zhong, Tailin He & Guozhi Xiao is licensed under a CC BY (Attribution) license
- Private: Rheumatoid_arthritis © Servier Medical Art adapted by Netha Hussain is licensed under a CC BY-SA (Attribution ShareAlike) license
- 800px-Rheumatoid-Arthritis © National Library Of Medicine US is licensed under a Public Domain license
- Rheumatoid Arthritis © Ali, Muhammad, Viviana Benfante, Domenico Di Raimondo, Riccardo Laudicella, Antonino Tuttolomondo, and Albert Comelli is licensed under a CC BY (Attribution) license
- Swan neck deformity in a 65 year old patient with Rheumatoid Arthritis © wikimedia commons is licensed under a CC BY-SA (Attribution ShareAlike) license

.jpg){kind=link}
{kind=link}
{kind=link}