Chapter 4 Selected Musculoskeletal Disease and Disorders, including Trauma and Rheumatic Disorders
Osteopenia and Osteoporosis
Zoë Soon
Osteopenia and Osteoporosis
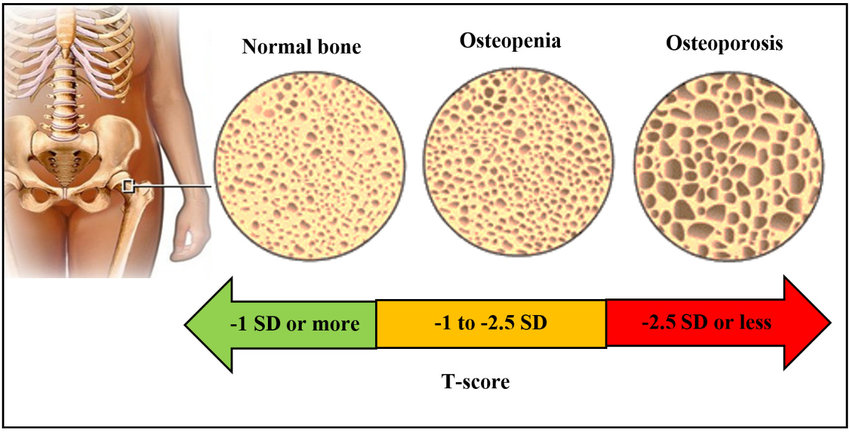
Osteopenia and osteoporosis are characterized by reduced bone volume and bone mass. This makes bones porous, weak, brittle, and more susceptible to breaking. The name osteopenia comes from the Greek words osteo meaning ‘bone’ and penia meaning ‘poverty’. Likewise, the name osteoporosis comes from the Greek words osteo for ‘bone’ and poros referring to the ‘pores’. The suffix -osis is often used in pathology as it is used to specify a ‘condition’ (usually a disease condition).
Osteopenia and osteoporosis affect both trabecular and cortical bone, and reduce all components (organic and inorganic components) that comprise bone. The osteoid organic components are largely comprised of collagen, proteoglycans, and glycoproteins as well as osteocytes and other bone cells (osteoblasts, osteoclasts, and osteoprogenitor cells). The inorganic components of bone are comprised of calcium phosphate salts and a small amount of water. Additionally, bone is penetrated by blood vessels and nerves.
Rickets and osteomalacia are different that osteopenia and osteoporosis, in that both rickets and osteomalacia are characterized by “soft bones”. The affected bones contain the organic components (e.g., osteoid) but have low levels of mineralization (calcium and phosphate content), making the bones softer and more pliant.
Osteopenia typically occurs to bones prior to the development of osteoporosis. The degree of bone loss is less than that of osteoporosis. Osteopenia is characterized by the loss of bone density in a manner that is asymptomatic.
Risk Factors – Osteoporosis
There are many risk factors for the development of osteoporosis and most contribute over the course of many years. Age is the biggest risk factor for osteoporosis, affecting 10% of all Canadians >40 years of age and >21% of all post-menopausal females. Statistics in the USA are similar.
Certainly, lifestyle factors are known to contribute to the development of osteoporosis. For example:
- sedentary behaviour
- smoking
- nutritional deficits
Primary Osteoporosis: There are 2 forms of primary osteoporosis (post-menopausal and age-associated osteoporosis). Post-menopausal osteoporosis is self explanatory in that females are more at risk of developing osteoporosis when estrogen levels decrease after menopause. Age-associated osteoporosis is common after 70 years of age for females and males as bone loss speeds up post-menopause and post-andropause. It is estimated that 50% of biological females and 21% of biological males will experience at least one fracture associated with osteoporosis during their life time. The most common bone fractures occur in the femur neck, vertebrae, and wrists.
Secondary Osteoporosis: Certain diseases, deficiencies, and medications can cause osteoporosis and in this case the term secondary osteoporosis is applied. Juvenile osteoporosis is often secondary to an underlying disease or deficiency and is characterized by an age of onset of 8-14 years. Examples of risk factors, conditions, and/or diseases that can lead to osteoporosis include:
1. Genetics:
- Certain genetic conditions are depicted by mutations in genes that affect specific proteins (e.g., fibrillin and collagen) that play key roles in bone. Examples include: Marfan Syndrome and Osteogenesis Imperfecta
- Family history is a risk factor, suggesting the inheritance of genetic susceptibilities. Along the same line, genetics plays a role in the susceptibility of certain ethnicities (White and Asian) being more at risk for osteoporosis.
- Thin-boned, slender females and males are more at risk for osteoporosis, as there is less bone to lose before structural strength is compromised.
2. Sex Hormone Levels:
- Reduced level or duration of exposure to sex hormones puts one at risk for developing osteoporosis.
- Amenorrhea, late menarche, early menopause, Turner Syndrome (X), Klinefelter Syndrome (XXY)
3. Anabolic Hormone Levels:
- Endocrine Disorders: that lead to hormone deficiencies in anabolic hormones (e.g., sex hormones, thyroid hormone, growth hormone, insulin)
- Diabetes mellitus is a risk factor as lack of insulin or insulin insensitivity leads to poor uptake of cellular building blocks (e.g., glucose and amino acids) that are required by bone cells.
4. Catabolic Hormone Levels:
- Endocrine Disorders that lead to overproduction of hormones that are catabolic (e.g., cortisol, parathyroid hormone).
5. Hyperthyroidism
- While normal levels of thyroid hormone are important for bone growth and maintenance, excess thyroid hormone in adults is reported to induce the activity of both osteoclasts and osteoblasts, with the net effect of bone loss.
6. Pregnancy, though occurring very rarely, is a risk factor for osteoporosis.
- During pregnancy, increased bone resorption can be stimulated to support calcium needs of fetal growth and lactation.
7. Malabsorption Syndromes or Dietary Deficiency States:
- Celiac disease, Cystic Fibrosis, Anorexia Nervosa, Bulimia Nervosa, Gastric Bypass surgery, Alcoholism, and/or Malnutrition can lead to deficiencies in vitamin D, and the vital building blocks for bone (e.g., calcium, magnesium, and amino acids.
8. Chronic Inflammatory Diseases:
- Systemic Lupus Erythematosus, Rheumatoid Arthritis (RA), and Crohn’s disease all are characterized by increased levels of pro-inflammatory cytokines and activated white blood cells. It is thought that pro-inflammatory cytokines increase osteoclast activity and decrease the activity of osteoblasts making one susceptible to osteoporosis. Plus the repetitive damage to the bone ends with RA, makes those regions susceptible to osteoporosis. Likewise, severe osteoarthritis is a risk factor for osteoporosis for the same reasons (plus the immobility/sedentary behaviour that can occur with OA and RA due to pain experienced on movement).
9. Reduced Oxygen Supply to Bones:
- Blood diseases: Sickle Cell anemia, chemotherapy-induced anemia, and blood cancers can lead to reduced delivery of nutrients and oxygen to bone cells, which is a risk factor for osteoporosis.
- Poor oxygenation due to Chronic Obstructive Pulmonary Disorder (COPD, e.g., emphysema) or Chronic Heart Failure (CHF)
10. Reduced Weight-Bearing Activities and Sedentary Behaviour
- Immobility, for example reduces the activity levels of osteocytes and osteoblasts leading to less osteoid production and calcification, resulting in bone atrophy (e.g., lower bone density).
11. Catabolic Medications:
- Medications (e.g., corticosteroids) decrease the activity levels of osteocytes and osteoblasts leading to less osteoid production and calcification, resulting in bone atrophy (e.g., lower bone density).
Signs and Symptoms – Osteoporosis
Osteoporosis develops slowly and asymptomatically often not being diagnosed until fractures or bone pain occur.
Vertebral compression fractures are common, two-thirds of which are painless, though result in stooped posture (kyphosis) and loss of height. If pain does occur, it is either sharp or dull and may become worse with movement. Vertebral fractures can cause muscle spasms. A decrease in height of 2-3 cm occurs with each vertebral fracture
Falls can result in hip fractures, sacral insufficiency fractures, Colles fractures (of the distal radius and possibly ulna).
Hip fractures are common, with the fracture most often occurring in the proximal femur (e.g., femur neck).
Diagnosis – Osteoporosis
Physical examinations to assess for loss of height, kyphosis, signs of fractures, and any loss of muscle strength and balance (to determine risk of frailty and falling)
Typically, blood tests are performed to test for:
- anemia (using complete blood count)
- vitamin D levels
- calcium levels
- sex hormone levels
Bone density measurements using dual-energy x-ray absorptiometry (DXA)
Imaging (e.g., CT scan, SPECT, MRI, Ultrasonography, bone scans) can be used to find bone lesions,
Bone biopsies can be done to exclude any bone pathologies
Some tests are done to rule out other problems (e.g., with thyroid, liver, kidney, etc.) that may contribute to osteoporosis.
Prevention and Treatment – Osteoporosis
Prevention of osteoporosis is important as osteoporosis is not curable and develops over the course of one’s life.
Both prevention and treatment involve lifestyle adaptations which include:
- weight-bearing and muscle strengthening exercises
- healthy diet with recommended levels of calcium and vitamin D included
- limiting alcohol and caffeine consumption
- smoking cessation
Treatment of osteoporosis can involve anti-osteoporosis medications (e.g., bisphosphonates), vertebroplasty, orthotics, healing of fractures, hormone (e.g., estrogen) replacement therapy
Physical and occupational therapy can be helpful in addition to home adaptations to reduce risk of falls (e.g., hand rails, replacing slippery flooring)
At times treatment for depression and pain is required particularly with the development of kyphosis.
An additional goal of treatment involves keeping a person mobile as long as possible as immobility brings additional risk factors (e.g., deep vein thrombosis and pressure ulcers).
Osteopenia and Osteoporosis Summary:
- Osteoporosis:
- Chronic disease of older adults.
- Old cortical and trabecular bone resorbed faster than new bone formed.
- Decrease in osteoblast activity, increase in osteoclast activity.
- Common sites: femoral neck, vertebrae, wrists.
- Hormonal influence: estrogen and testosterone levels affect osteoblast activity.
- Risk factors: aging, hormonal changes, sedentary lifestyle, smoking, glucocorticoids use, early menopause, low calcium/vitamin D diet, genetics, excessive alcohol/caffeine.
- Diagnosis: bone density scan, serum/urine calcium/phosphate levels.
- Prevention: diet, exercise, weight-bearing exercises, bisphosphonates.
- Treatment: physiotherapy, pain management, prevention of further bone loss.
Key Take Aways – Specific Learning Objectives Study Guide
Osteopenia and Osteoporosis:
Both are bone weakening diseases characterized by reduced bone volume due to loss of both:
- Organic bone matrix (osteoid) = collagen, glycoproteins and proteoglycans
- Inorganic bone matrix (calcium salts/minerals) = CaPO4
- Osteoporosis is more severe than osteopenia and is depicted by greater loss of bone volume and bone density putting an individual at risk for low-impact bone fractures.
- Osteopenia can be treated by ensuring sufficient dietary nutrients required for bone maintenance as well as taking part in regular recommended exercises (e.g., prescribed weight-training).
- Osteoporosis is characterized by irreplaceable loss of bone microstructure and density.
Osteoporosis:
Osteoporosis is considered a chronic disease that affects many older adults, in which old cortical (compact) and trabecular (spongy/cancellous) bone is being resorbed faster than new bone matrix is being made. The most severe loss of bone density typically occurs in the femoral neck, vertebrae, and wrist. Bone maintenance and synthesis is impacted by various hormone levels: Thyroid Hormone (TH), Cortisol, Growth Hormone (GH), estrogen and testosterone are important for maintaining osteoblast activity. Lower levels of estrogen and testosterone in old age, result in lower levels of osteoblast activity.
Risk factors:
- age
- post-menopausal biological (XX) females due to lower estrogen levels
- early menopause
- sedentary lifestyle
- use of corticosteroids (e.g., glucocorticoids)
- low intake of dietary Ca++ and/or vitamin D
- excessive alcohol or caffeine
- smoking
- rheumatic arthritis
- diabetes mellitus
- genetics
Categories of Osteoporosis:
- 1st Degree Osteoporosis = due to age related decreases in hormones (e.g., sex hormones)
- 2nd Degree Osteoporosis = due to underlying disease
- Celiac disease, due to malabsorption of Ca++ and/or vitamin D
- Hyperthyroidism, due to increased metabolic activity
- Hyperparathyroidism due to increased osteoclast activity
Signs & Symptoms: low-impact fractures (1.5 million/yr in USA), hip fractures, height reduction, kyphosis, vertebral compression fractures
Routine Check-Ups: regular bone mass density scan tests after the age of 50
Diagnostic Evaluation:
- monitoring bone density using dual energy X-ray absorptiometry (DEXA) or other imaging (CT scans, MRI)
- monitoring serum/urine for low serum levels of Ca++, PO4, low levels of parathyroid hormone (PTH),
- assessing for bone deformities
Prevention: through avoidance of modifiable risk factors
Treatment:
- pain management
- bisphosphonates (work by decreasing osteoclast activity)
- weight-bearing exercises
- calcium carbonate and vitamin D supplementation
- Vitamin D Recommended Dietary Allowance for adults 19 years and older is 600 IU (15 mcg) daily for men and women, and for adults >70 years it is 800 IU (20 mcg) daily.
- Caution should be used not to exceed this dosage as vitamin D can build up to excessive and harmful levels in the body.
Physiotherapy: to alleviate pain & maintain function of muscles, tendons, and nerves, recommendations include use of proper warm-up, appropriate equipment, training.
Media Attributions
- Comparative-view-of-normal-bone-osteopenia-and-osteoporosis-26-Reproduced-under-the © Rani, Seema & Bandyopadhyay-Ghosh, Sanchita & Ghosh, Subrata & Liu, Guozhen. is licensed under a CC BY (Attribution) license
