Chapter 4 Selected Musculoskeletal Disease and Disorders, including Trauma and Rheumatic Disorders
Plantar Fasciitis
Zoë Soon
Plantar Fascia
Plantar Fasciitis
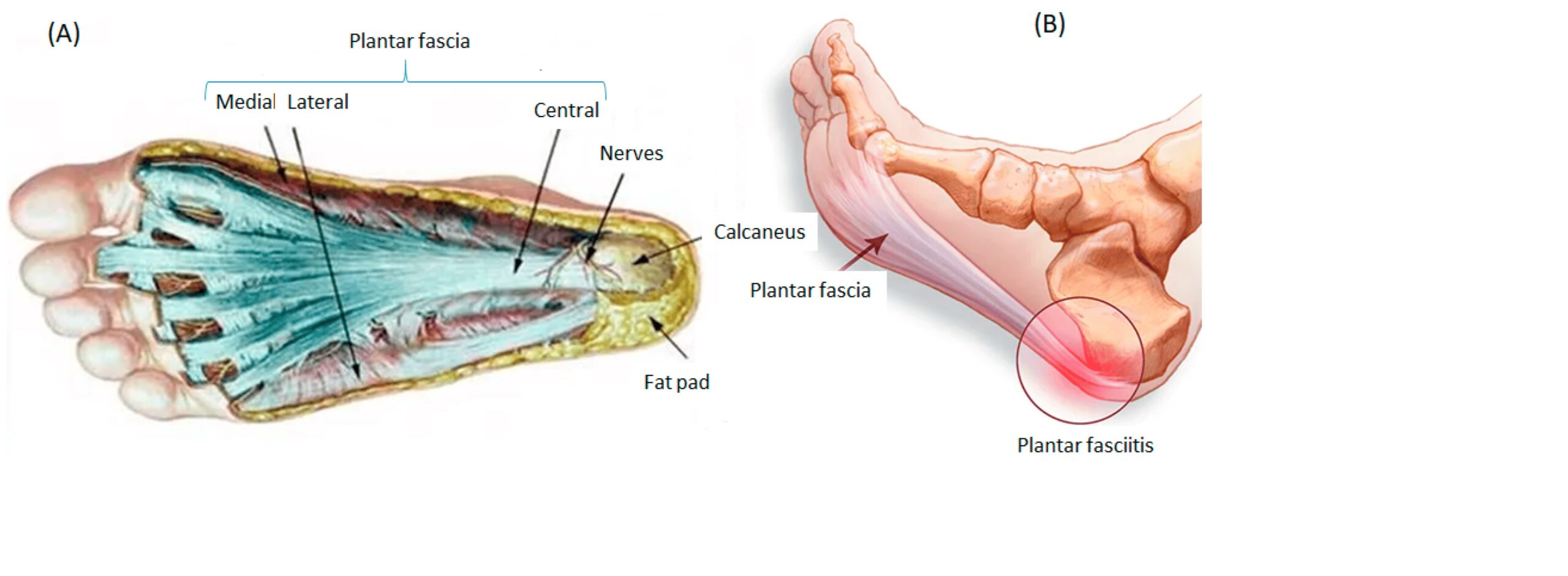
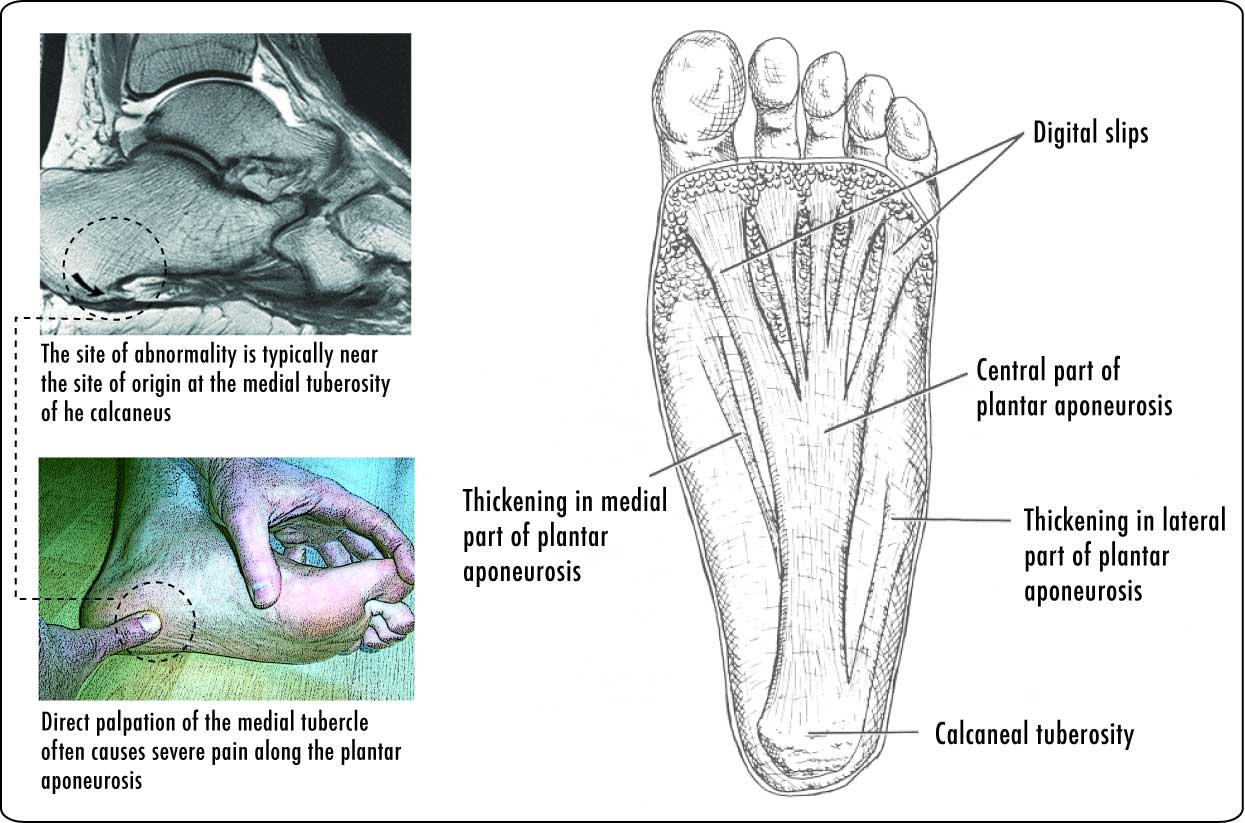
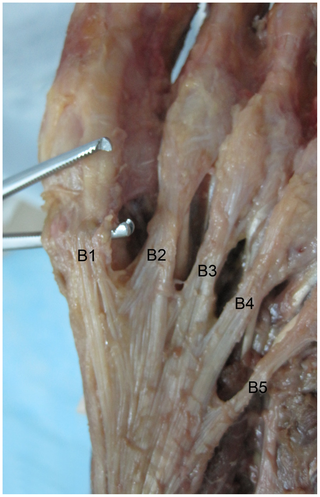
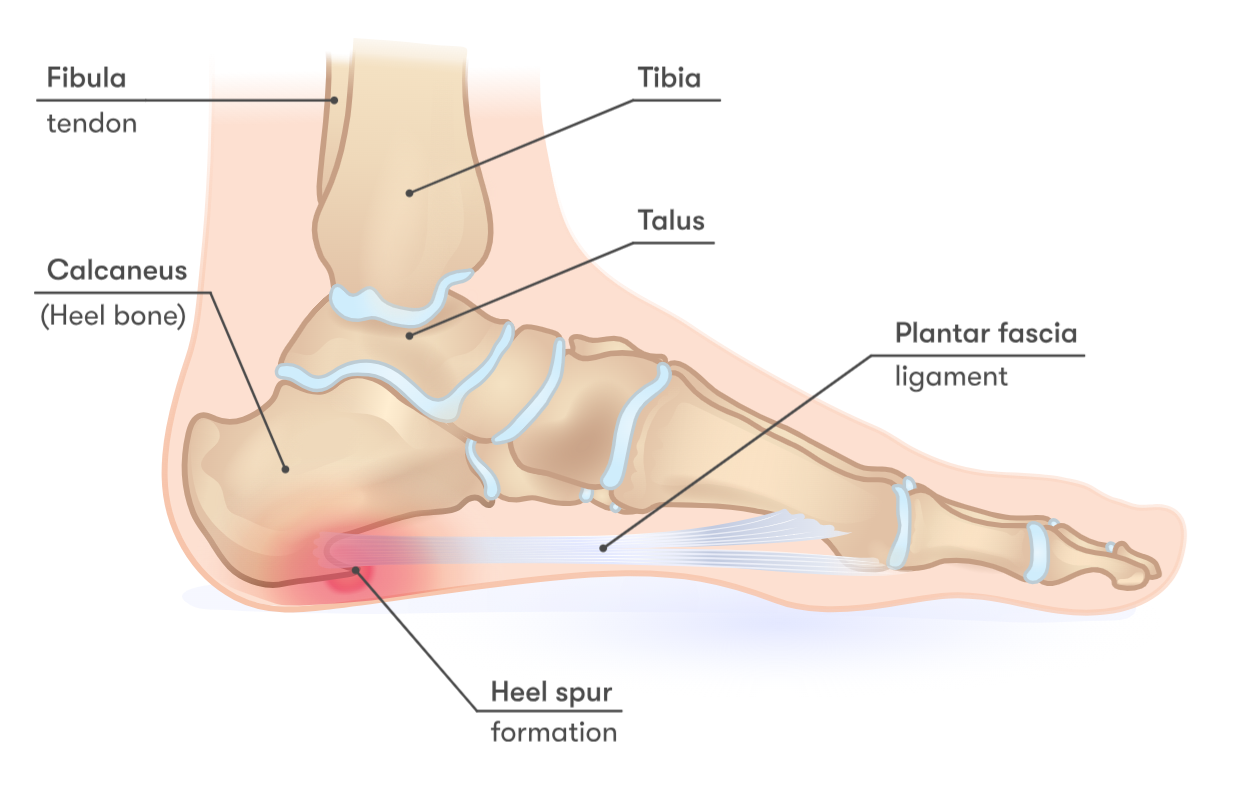
Irritation and inflammation of the plantar fascia, which is a thick, broad aponeurosis (or flat tendon) that extends along the bottom (or sole) of the foot supporting the arch. Aponeurosis and tendons are connective tissues that are composed largely of long fibrous collagen proteins. The plantar fascia originates at the medial tubercle of the calcaneus and then divides into 5 bands at the metatarsophalangeal joints (joints between metatarsals and proximal phalanges of toes) and extends forming fibrous flexor sheaths around tendons of flexor muscles of the toes (and located on the bottoms of the toes). The plantar fascia plays a role in walking acting like a spring and is estimated to carry a significant portion (~15%) of the body’s load (weight) acting as a tension bridge.
Risk Factors – Plantar Fasciitis
There is a high incidence in runners, as well as athletes of many sports that involve running or jumping (e.g., tennis, soccer, aerobics, volleyball) and professions that involve walking. Incident rate is estimated to be 2-4 cases per 1000 people per year. Long periods of standing, as well as carrying excess weight are risk factors, as is exercising on hard floors, especially with bare feet. Bony heel spurs can be associated with plantar fasciitis, though many individuals have asymptomatic heel spurs.
Pathogenesis – Plantar Fasciitis
Plantar fasciitis is multifactorial and the definite cause is unclear, though it is associated with microtrauma due to excessive stretching or repetitive stressing of the plantar fascia. Repetitive microtraumas can lead to degeneration, in which the collagen and vasculature of the plantar fascia becomes disorganized and inflamed.
Signs and Symptoms – Plantar Fasciitis
Pain is often felt first thing in the morning and is predominantly located on the plantar surface of the foot near to the calcaneus. Typically the pain then decreases with walking, but then increases throughout the day as activity or prolonged sitting occurs. There may be some stiffness and swelling. The individual may walk with a limp or on their toes to avoid pain.
Diagnostic Tests – Plantar Fasciitis
Pain may be reported when plantar-anterior calcaneal tubercle is palpated, or during ankle or toe dorsiflexion (pointing toes). Other physical tests (such as the Windlass test) are often done to rule out Achilles tendonitis, bursitis, stress fractures, and other problems. Sometimes imaging (e.g., x-ray, ultrasound) is used to rule tumors or fractures, as well as locate or reveal any heel spurs which may have formed in response to abnormal stresses.
The effect of dorsiflexing the toes on arch height (A). The windlass mechanism (B).
![Figure 2. (A) The plantar fascia and the longitudinal arch of the foot form a truss. (B) Dorsiflexion of the toes during the late stance phase of gait tensions the plantar fascia around the metatarsal heads leading to an increase in the height and stability of the longitudinal arch of the foot “Windlass” mechanism. Source: Reprinted from Latt L.D.; Jaffe, D.E.; Tang, Y. Evaluation and Treatment of Chronic Plantar Fasciitis. Foot Ankle Orthop. 2020 [9] (SAGE Open access licensed under CC BY-NC-SA 4.0, no permission required).](https://pressbooks.bccampus.ca/pathophysiology/wp-content/uploads/sites/1961/2024/03/WindlassMechanism.png)
Treatment – Plantar Fasciitis
Treatment often involves approximately PRICE (Protection, Rest, Icing, Compression and Elevation), possibly anti-inflammatories (e.g., NSAIDs) and usually involves a full recovery. Protection can involve taping, orthotics, and improved shoes. In some cases where degeneration of the fascia has occurred, techniques such as platelet rich plasma injections, extracorporeal shock-wave therapy (ESWT), surgery, and physical therapy (stretching and strengthening exercises) are recommended. Some individuals recover quickly whereas other individuals can take 6 weeks or longer.
Prevention – Plantar Fasciitis
Running can create forces of 2-3 times an individual’s body weight creating strain on the foot. It is therefore recommended that individuals wear shoes with adequate arch support and heel cushioning. Discarding old shoes and rotating shoes daily that are in good condition is advised. Stretching the plantar fascia and leg muscles as well as warm-ups before and after exercise is recommended.
Summary
- Plantar fascia
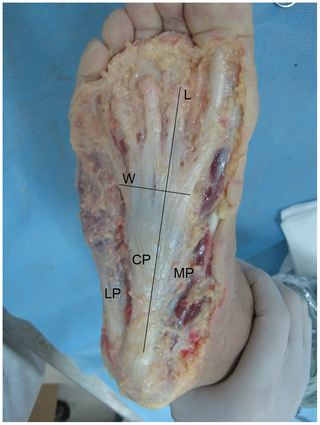
LP, lateral part; CP, central part; MP, medial part; L, length; W, width.
- Bone spurs are sometimes associated with plantar fasciitis, though bone spurs can also be asymptomatic
- Plantar fasciitis:
- Caused by sudden increase in walking, like during travel.
- Results in tiny tears, leading to pain.
- Rehabilitation exercises post PRICE (Protection, Rest, Ice, Compression, Elevation).
- Focus on maintaining range of motion, preventing scarring.
- Stretching exercises crucial.
Media Attributions
- Plantar Fascia © Noriega, D.C.; Cristo, Á.; León, A.; García-Medrano, B.; Caballero-García, A.; Córdova-Martinez, A. is licensed under a CC BY (Attribution) license
- Plantar Aponeurosis © Kosi Gramatikoff is licensed under a Public Domain license
- Plantar_Bewegung © Kosigrim is licensed under a Public Domain license
- WindlassMechanism © Latt L.D.; Jaffe, D.E.; Tang, Y. is licensed under a CC BY-NC-SA (Attribution NonCommercial ShareAlike) license
- Plantar_aponeurosis_-_axial_view © Da-wei Chen, Bing Li, Ashwin Aubeeluck, Yun-feng Yang, Yi-gang Huang, Jia-qian Zhou, Guang-rong Yu is licensed under a CC BY (Attribution) license
- Plantar_aponeurosis_-_central © Da-wei Chen, Bing Li, Ashwin Aubeeluck, Yun-feng Yang, Yi-gang Huang, Jia-qian Zhou, Guang-rong Yu is licensed under a CC BY (Attribution) license
- Bony Heel Spur © InjuryMap - InjuryMap is licensed under a CC BY-SA (Attribution ShareAlike) license
