Chapter 1 Introduction to Pathophysiology; Cellular Responses to Stress, Injury, and Aging
Cellular Responses to Stress, Injury, and Aging
Zoë Soon
Testing, Testing, Testing: Diagnostic Tests
The Range and Importance of Diagnostic Tests – Which one to use? And is it sensitive enough? Is it specific enough?
There are so many health care tests that provide clues as to the diagnosis.
There are chemistry tests to assess: components of blood (e.g. lipids, pH and oxygen levels) and components of urine (e.g. urinalysis). There are volume tests for measuring: blood pressure and functional lung volumes. There are palpation tests to assess: heart and pulse rates for example. There are microscopy tests to analyze: cellular features within biopsies as well as the presence of possible pathogens (e.g. throat or vaginal swabs, fecal analysis, sputum tests). There are listening tests (e.g. auscultation of breath, heart and bowel sounds, etc.). There are flow cytometry tests that can be used to count the numbers of WBCs and RBCs per mL in blood,. These tests and more are used in health care research.
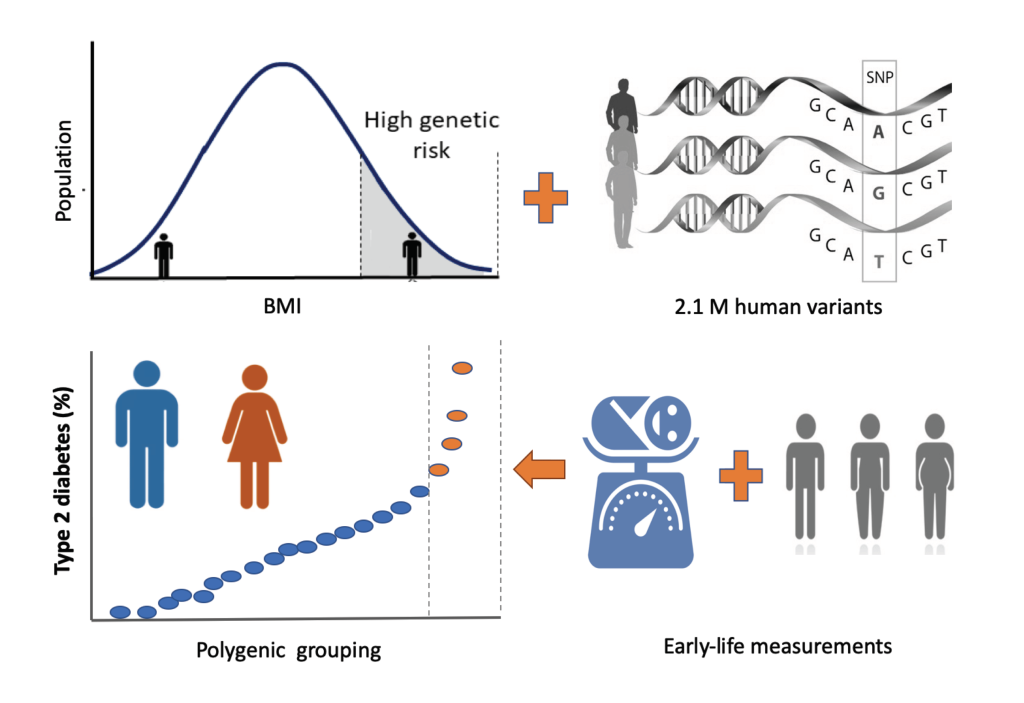
Let’s look at an example in which different tests (in this case weight, BMI, and genetic) may signal there is a risk of, or even the presence of a disease.
Example: Research has found that there are several risk factors for developing Type 2 Diabetes: high birth weight, high BMI (body mass index) at age 10, high BMI as an adult, being biological male (XY) and at times, there may be some genetic components.
In the previous pages, we discussed the importance of determining whether a person’s test results fall into the range of normal (and presumably healthy), or perhaps indicate disease and disruption in homeostasis. Also we should clarify – even though the terms normal and abnormal are used at times in test results, it is likely obvious to you that normal (test results) is not always the same as healthy, and abnormal (test results) does not always mean the presence of a disease or disorder.
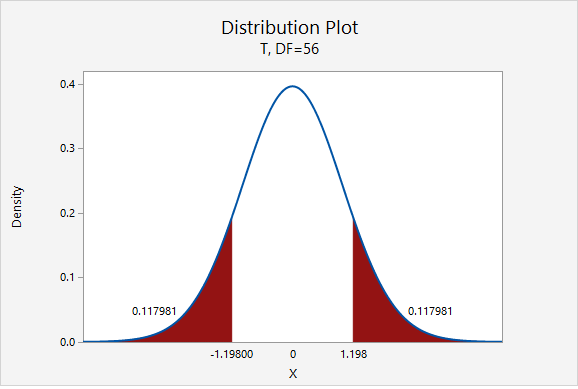
In the above figure, a typical bell curve indicates the range of test results that can be expected in a set population. In this case, resting heart rate data has been graphed for 57 college males. Even though the low and high ends of the graph have been coloured red, all of the resting heart rates in this particular population ( which are from ~60-80bpm) are in the expected normal range. Typically, if a resting heart rate is below 60bpm or above 100bpm, it would be considered abnormal, and indicative of a disruption in homeostasis. If a disease is suspected, and results fall outside of what is considered normal, usually follow-up and complementary tests are performed in order to gain enough information to make an accurate diagnosis.
It should be noted that test results that are high or low, don’t necessarily indicate disease. If there isn’t a disease despite abnormal test results we would use the term False Positive. Additionally individuals with disease can have test results that are normal. In this situation we would use the term False Negative.
Let’s examine this further including the terms: True Positives, True Negatives.,
Quick Reminder: In the last section we defined different terms such as: atrophy, hypertrophy, dysplasia, anaplasia, neoplasia. We noted that dysplasia is considered pre-cancerous, and dysplastic cells are no longer completely differentiated. They are slightly undifferentiated and they might be having a little bit more mitosis than normal. If that continues, might well develop a neoplasia or an actual growth or tumour. If the tumour stays within the basement membrane, we know it’s a benign neoplasia and if it starts spreading, it breaches the basement membrane, we know that it’s become malignant (or cancerous).
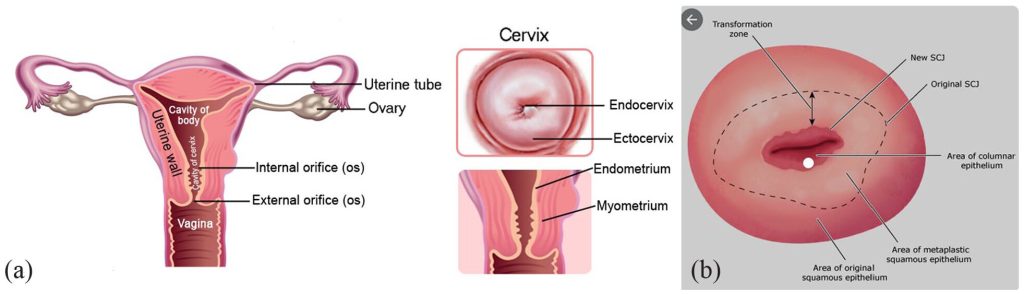
In this table, let’s examine the possible results of a Pap smear in which cervical cells are scraped and are examined to see whether the cells have reverted to an undifferentiated state. Luckily, cervical cancer is a very slow cancer, so routine screening once every 2-3yrs (as per recommended by a physician, depending on patient’s risk level) means you’re more likely to catch it in a dysplastic state well before a malignant state. This is important in ensuring that it can be treated with a good degree of success.
Normal Test Results |
Abnormal Test Results |
|
Healthy – this person does not have disease (e.g. cervical cancer) |
True Negative – a healthy person’s test results are normal |
False Positive – a healthy person’s test results are abnormal |
| Example – Pap Test to detect signs of cervical cell dysplasia or anaplasia. Healthy person does not have cervical pre-cancer or cancer. | Cervical cells examined under microscope have normal cell morphology = True Negative | Cervical cells examined under microscope have abnormal cell morphology – which may indicate pre-cancer or cancer. Perhaps cells are affected by minor infection or other temporary non-cancerous issues = False Positive |
Sick – this person does have the disease (e.g. cervical cancer) |
False Negative – a sick person’s test results are normal |
True Positive – a sick person’s test results are abnormal |
| Example – Pap Test to detect signs of cervical cell dysplasia or anaplasia. This person does have cervical pre-cancer or cancer. | Cervical cells examined under microscope have normal cell morphology. Missed scrapping cells that are affected by pre-cancer or cancer = False Negative | Cervical cells examined under microscope have abnormal cell morphology – which in this case accurately reflect pre-cancer or cancer = True Positive |
Now as we can see in the above test, it is virtually impossible to design a diagnostic test that is 100% accurate all of the time. Most often complementary and follow-up tests are done in order to become more confident in diagnoses.
So, the goal of tests is to be either specific or sensitive (or both). What does that mean?
Sensitivity – Can a test accurately detect True Positives? – which is important! Sensitivity, is a test’s ability to be positive in the presence of the disease. If a test can correctly identify 99 out of 100 sick people that do have the disease, the test is 99% sensitive, which is an extremely impressive ability for a test.
Specificity – Can a test accurately detect True Negatives? – which is important! Specificity, is a test’s ability to be negative in the absence of the disease. If a test can correctly identify 99 out of 100 healthy people that do not have the disease, the test is 99% specific, which is an extremely impressive ability for a test.

In the above figure, a new added step to the protocol for cervical testing is being developed and implemented in some countries. The newly added step is the first one, in which a Primary HPV (Human Papilloma Virus) test, a highly sensitive test is used that screens for the DNA presence of the HPV strains that are considered high risk for cancer development. The cytology test involves the Pap smear with microscopic analysis of cervical cellular morphology. Traditionally, the cytology (Pap smear) test is used as the initial test, and is also considered highly sensitive with an even greater degree of specificity than the HPV test. The third test in the above figure, the colposcopy test is considered a highly specific test.
What is a colpscopy? Colpscopy is a specificity test performed when abnormal cells are detected in a Pap smear. It involves using a colpscope, a thin flexible tube with lighted, magnifying camera that can examine the cervix, vagina, and vulva for lesions and signs of cancer.

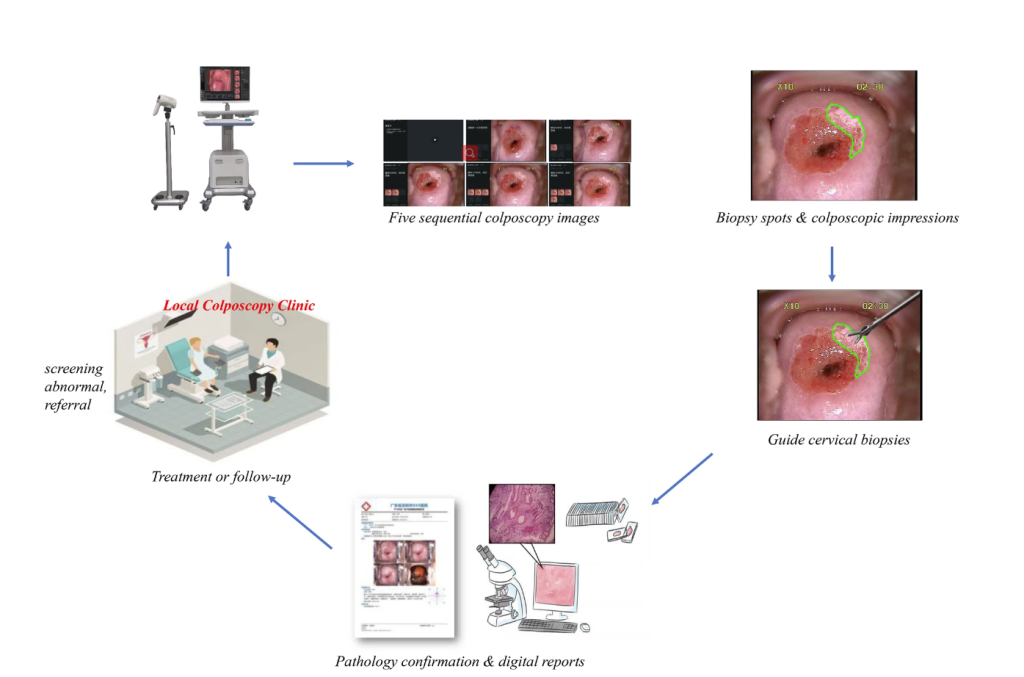
The above figures show the strategy most often used in diagnostic testing, in which the first test used is a highly Sensitive test, which is very good at identifying illness, and makes sure that you can alert as many people as possible that may have the illness. The Specificity test typically follows the Sensitivity test, and is used to identify false positives (e.g. make sure those that are healthy are correctly identified, and then alerted that they don’t have the disease, and are not treated for a disease that they don’t have). a more specific test next.
Ethics of Diagnostic Tests – Design of and Use of?
If we pause to think about the design and use of diagnostic tests, we can start to imagine that there are a lot of ethical questions that are encountered.
a) For example how do you decide which tests to try to develop?
b) How much funding should be given to each test development research?
c) Once developed, how much should each test cost (to the patient and to the taxpayer)?
d) When and how often should each test be recommended?
Pause and Reflect: Most often tests are developed and used with the following priorities involved:
- a significant percentage of the population is at risk
- the development of a test is feasible,
- the test will be reliable (valid, repeatable),
- the test will be sensitive and/or specific,
- the test produced will be inexpensive/affordable,
- the test will be easy to store/deliver,
- the test will be user-friendly and not prone to human-error,
- ideally, the test is non-invasive (which also helps to make it less expensive and less time consuming).
Pause and Reflect: What is an example of a Non-invasive test?
Non-invasive tests include: blood test, urinalysis, sputum and stool sample analysis, x-rays (e.g. mammograms), physical exams.
Let’s brainstorm – what type of tests are you familiar with?
- Blood tests have many uses including:
- checking red blood cell (RBC) and white blood cell (WBC) numbers – RBC and WBC counts would give an indication of the status of red blood cell (erythrocyte) and white blood cell production and survival rates.
- monitoring plasma protein levels cand be a good way to check liver function, as the liver manufactures a lot of the blood proteins.
- the presence of abnormal proteins can be used to detect some types of cancer and organ damage or dysfunction.
- the presence of certain antibodies or pathogens can indicate disease.
- Heart and lung function tests and in those units, we will discuss:
- Spirometry measurements of lung volumes
- Imaging test can be helpful in viewing internal problems:
- X-rays are used to evaluate radio-dense materials in the body (e.g. bones and detection of bone fractures)
- CT (Computed Tomography, or CAT) scans a 3-dimensional (3D) x-ray provides more resolution than the traditional 2D X-ray
- MRI (Magnetic Resonance Imaging) scans are used to examine soft-tissues of the body
- Ultrasound can be used to take a close look at heart valves or heart wall movement in addition to fetal development
- ECG (EKG, electrocardiogram) examining cardiac conduction (the electrical waves) within the heart
- EEG (electroencephalogram) measures the electrical currents in the brain.
- EMG (electromyography) measuring skeletal muscle function (specifically the ability of a muscle to contract when electrically stimulated)
- Conduction tests are used to assess motor nerve function
- Endoscopy utilizes a camera on a flexible tube that can be inserted into the body to take a closer look at suspected areas of damage.
- Biopsy followed by Histology (with a microscope) to monitor changes in cellular morphology
- Microscopy to examine sputum, urine, feces for signs of pathogens or other abnormalities (e.g. crystals or protein casts in urine).
Degenerative Diseases and Microscopic Cellular Accumulations
Aging is a risk factor for several degenerative diseases, particularly those that affect the nervous system (e.g. Alzheimer’s, ALS, Parkinson’s) or a result of a lifetime of wear and tear (e.g. Osteoarthritis).
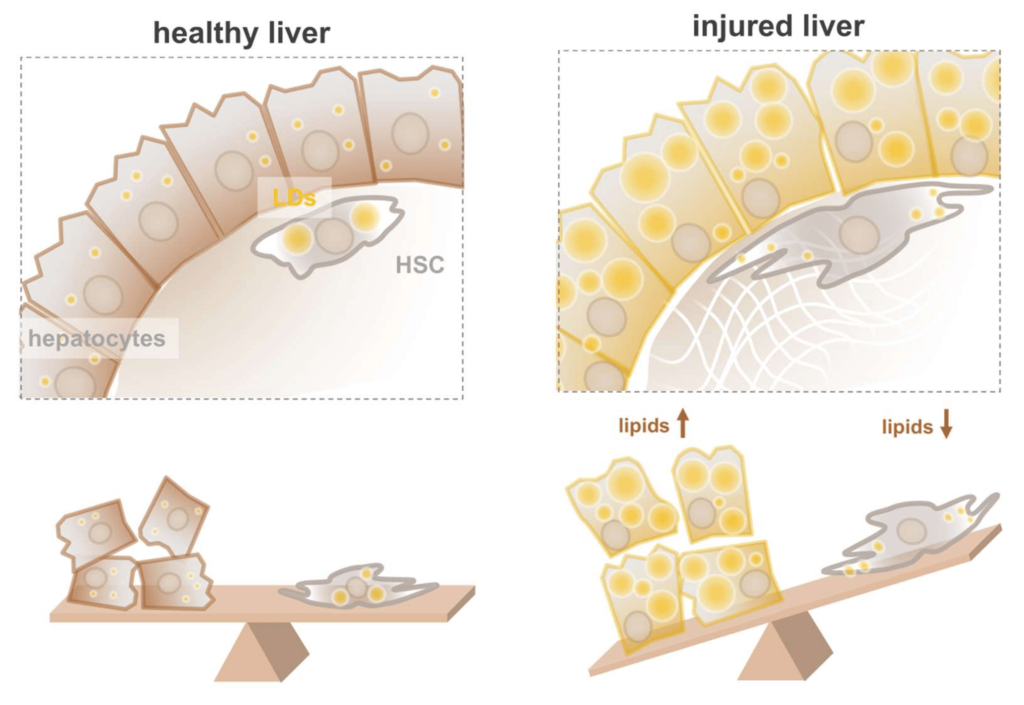
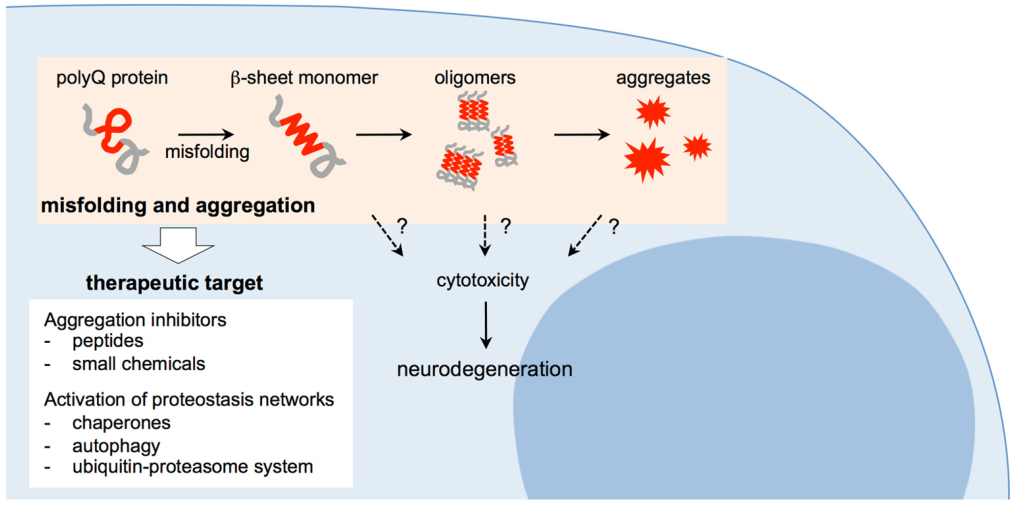
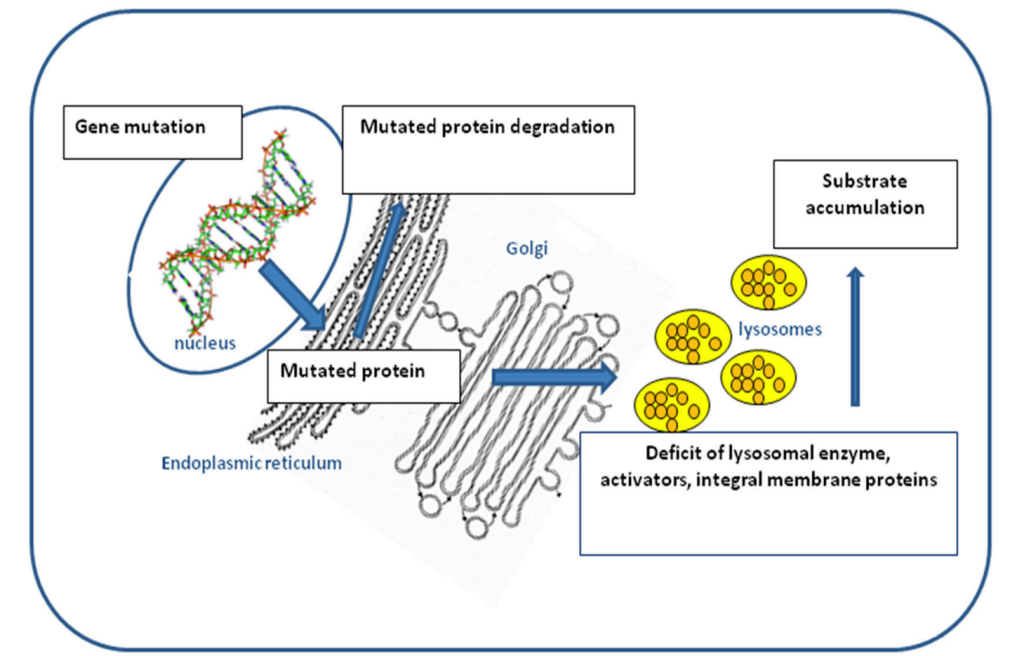
Some cells in the body have very have long life spans. For example, neurons and most heart and skeletal muscle cells are as old as you are. It may not be surprising that over time, these cells can accumulate different materials that become detrimental to their function. Cells can accumulate endogenous compounds such as lipids, proteins, carbohydrates, pigments, metabolic toxins. Endogenous means it’s accumulating a substance that’s part of you, it’s a normal part of you. Cells can also accumulate exogenous compounds from the environment such as lead or mercury.
So it might not be surprising that as your brain gets older, accumulating potentially some of these things, it becomes more susceptible to different forms of dementia, all of which are considered degenerative diseases.
Media Attributions
- T2D risk © Moldovan, A.; Waldman, Y.Y.; Brandes, N.; Linial, M. is licensed under a CC BY-SA (Attribution ShareAlike) license
- Distribution Plot of Heart Rate is licensed under a CC BY-NC (Attribution NonCommercial) license
- Cervical Cancer Screening © Chrysostomou, A.C.; Kostrikis, L.G. is licensed under a CC BY (Attribution) license
- PocketColposcope © Erica Skerrett is licensed under a CC BY-NC-SA (Attribution NonCommercial ShareAlike) license
- images_large_10.1177_11769351231161477-fig1 © Dash S, Sethy PK, Behera SK. is licensed under a CC BY-NC-SA (Attribution NonCommercial ShareAlike) license
- colposcopy © Xue, P., Ng, M.T.A. & Qiao, Y. is licensed under a CC BY-SA (Attribution ShareAlike) license
- Lipid Hepatocytes © Molenaar, M.R.; Penning, L.C.; Helms, J.B. Playing Jekyll and Hyde is licensed under a CC BY (Attribution) license
- ProteinMisfoldingAccumulation © Takeuchi, T.; Nagai, Y is licensed under a CC BY (Attribution) license
- LysosomeDysfunction © Dardis, Andrea & Buratti, Emanuele. is licensed under a CC BY (Attribution) license
