Main Body
CHAPTER 3: FORENSIC ASSESSMENT IN CRIMINAL DOMAINS
Chapter Objectives
- Summarize the legal standards and procedures for determining fitness to stand trial.
- Summarize the legal standards and procedures for determining criminal responsibility or insanity.
- Describe the points at which risk is assessed, the three approaches to risk assessment, and the factors used to assess risk.
- Describe psychopathy and malingering and explain how they are assessed.
Psychologists and other mental health professionals are often called upon by the courts to assist in the determination of various legal issues. Although the final determination of any legal issue rests with the legal decision maker ( judge or jury), psychologists assist the court by providing information obtained through the assessment of the person for whom the court must make a determination. The legal issues to be decided by the courts may be either civil (e.g., involuntary hospitalization, personal injury, child custody) or criminal (e.g., adjudicative competency, criminal responsibility) in nature. This chapter focuses on the role of the psychologist in the assessment of criminal forensic issues; the next chapter focuses on assessment of civil forensic issues. Issues relating to juveniles or juvenile court will be discussed in Chapter 7.
3.1 Criminal Competencies
Introduction
Learning Objectives 3.1
criminal law law that relates to crime and involves prosecution by the government of a person who has been charged with a crime
adjudicative competency the umbrella term that encompasses all types of criminal competencies; most commonly referred to as fitness to stand trial
competency to proceed a general term that refers to the ability of a defendant to proceed through the criminal adjudication process
competency to be sentenced refers to the ability of an accused to understand the sentencing process and the reasons why he or she is being sentenced
Dating back to at least the 17th century, courts have recognized that it would be wrong to proceed through the criminal process if an accused person is unfit (incompetent). In addition to protecting the rights of the individual to participate meaningfully in the process, the fitness/competency doctrine also serves to protect the dignity and integrity of the court proceedings. Allowing an unfit individual to be tried and found criminally responsible would offend the dignity and integrity of criminal law court proceedings, and the public would see the court as unfair.
Questions concerning an accused person’s fitness (adjudicative competency; competency to proceed) may arise at any of the following stages of the criminal justice process: when the crime is committed, when an interrogation is conducted, when/if an accused person makes incriminating statements or confesses, when/if an accused person elects to represent him/herself at trial, at trial, and at sentencing (competency to be sentenced). Issues of competence do not always arise, however, because courts assume competence, and it is up to the side raising the issue to establish that competence should be assessed.1 Accordingly, in the criminal justice system, competence assessments are done to decide incompetence, not competence. The legal tests for incompetence proceed by identifying the abilities required of a competent person in the circumstances and deciding if those abilities are absent or seriously impaired in a particular person. As discussed in more detail below, the test is a “limited cognitive capacity test”; individuals must demonstrate profound deficiencies in the requisite abilities before they will be found unfit (incompetent) to proceed through that stage of the criminal justice process.
Overview of Fitness to Stand Trial
A finding that a person is incompetent to proceed through one stage of the criminal justice system requires proof of a mental disorder in two situations: an assessment of criminal responsibility and an assessment of fitness to stand trial.2 The presence of a mental disorder is necessary but not sufficient to prove incompetence.
There is one peculiar exception to this general principle. In the case of a disputed confession, the Crown must prove that the confession was given voluntarily. Competence to waive the right to silence is only one way that the voluntariness of a confession may be challenged. This is distinct from competence generally and will be discussed in more detail in Chapter 9.
“Fitness to stand trial” is the term most commonly used in Canada and other countries, such as Australia and the United Kingdom; “competence to stand trial” is the term used most commonly in the United States. “Fitness” and “competency” will be used interchangeably throughout this chapter
In addition to the presence of a mental disorder, it must be established that the person suffers from particular deficits that are described below. In other evaluations—for instance, of competency to waive the right to silence or competency to waive the right to counsel—the presence of a mental disorder is not necessary to establish incompetence. Certainly, the presence of a mental disorder may provide evidence that a person is incompetent to proceed through that stage of the process, but it will not establish incompetence nor is it a necessary element of the assessment.
In this chapter we focus on fitness to stand trial and criminal responsibility, and we are concerned with legal competence, not psychological competence. A legal determination of competence is made by the court. It will consider whether certain legal abilities are impaired, sometimes as a consequence of a mental dis- order, to the extent that the person is unfit to proceed through that stage of the criminal justice process. Not all impairments, no matter how profound, will lead to a finding of legal incompetence.
Harmony of Competencies
In R. v. Whittle (1994), the Supreme Court of Canada held that there should be a harmony of competencies. That is, there should not be myriad standards of competence that apply at different stages of the criminal process; a single standard should apply across evaluations. Whittle, who suffered from schizophrenia, was arrested for unpaid fines. At the time of his arrest, he was hearing voices in his head telling him to unburden himself. After waiving his right to counsel and his right to remain silent, he made several incriminating statements that led to charges of robbery and murder. At trial he was found fit to stand trial but his statements were not admitted as they were deemed not voluntary. He was acquitted. The acquittal was appealed to the Ontario Court of Appeal and a new trial was ordered. The Court of Appeal decision was appealed to the Supreme Court of Canada, where the justices held that,
In exercising the right to counsel or waiving the right, the accused must possess the limited cognitive capacity that is required for fitness to stand trial The level of cognitive ability is the same as that required with respect to the confession rule and the right to silence. The accused must have the mental capacity of an operating mind. (para 51)
In R. v. Swain (1991), the Supreme Court of Canada applied the limited cognitive capacity test to evaluations of a person’s competence to represent himself or herself at trial: individuals who are fit to stand trial must also be fit to conduct their own defence. Later, in R. v. M.A.W. (2008), the Ontario Court of Appeal extended this principle to the voluntariness of a guilty plea: “Courts apply the limited cognitive capacity standard to determine an accused’s fitness to stand trial, as well as to assess the voluntariness of an accused’s decision whether to exercise the right to silence and the right to counsel. Applying this same test to the voluntariness of a guilty plea would achieve a desirable degree of uniformity” (para 28).
competency to waive the right to counsel (proceed pro se) refers to the ability of a defendant to waive the right to the assistance of counsel and to proceed without an attorney (self-representation)
fitness (or competency) to stand trial refers to the ability of defendants to understand the nature and object of criminal proceedings and to assist counsel in their own defence
As you will see, the limited cognitive capacity test for competence to stand trial serves as a kind of proxy for some other competencies: if the accused is fit to stand trial, the accused is also fit to engage in other stages in the crim- inal process. It would be wrong, however, to conflate the level of competence required (i.e., limited cognitive capacity) with the particular deficits that must be proven (e.g., ability to communicate with your lawyer in evaluations of fitness to stand trial; ability to understand the consequences in assessments of competence to waive the right to silence). The particular deficits that must be established vary across competencies, but the level of competence required to meet the legal threshold is common—limited cognitive capacity.
Fitness to Stand Trial
Perhaps the most commonly cited case with respect to fitness to stand trial is the American case Dusky v. United States (1960). Dusky established the standard for competency to stand trial in the United States and has been widely cited as a source of precedent and case law. Each state has its own standard for fitness to stand trial, but Dusky forms the basis for each of these state standards as well as for the federal standard for competence in the United States. In Canada, a person is presumed to be fit to stand trial unless it can be shown, on balance of probabilities, that that individual is not fit to stand trial. Section 2 of the Criminal Code defines “unfit to stand trial” as follows:
Unable on account of metal disorder to conduct a defence at any stage of the proceeding before a verdict is rendered or to instruct counsel to do so, and, in particular, unable on account of mental disorder to: (a) understand the nature or object of the proceedings, (b) understand the possible consequences of the proceedings, or (c) communicate with counsel.
A formal inquiry into an accused’s competency status must occur whenever a bona fide doubt about an accused’s fitness/competency is raised. The issue of an accused’s fitness can be raised by either the defence, the Crown, or by the court more generally (Criminal Code, s. 672.12). Once the issue is raised, one or more mental health professionals will evaluate the accused and will submit their conclusions in a report to the court. Research has indicated that the court agrees with the conclusions of the mental health professional in upward of 95 percent of the cases. Thus, while a hearing on the issue of fitness may occur, it usually is not necessary. Case Study 3.1 describes the case of R. v. Taylor (1992, affirmed by the Supreme Court of Canada in R. v. Whittle, 1994), in which the Ontario Court of Appeal articulated the limited cognitive capacity test. Applied to fitness to stand trial, the court held that an accused is competent to communicate with his or her lawyer if “an accused can recount to his/her counsel the necessary facts relating to the offence in such a way that counsel can then properly present a defence. It is not relevant to the fitness determination . . . whether the accused ultimately makes decisions that are in his/her best interests” (para. 44).
CASE STUDY 3.1 – A SUSPENDED LAWYER IS FOUND UNFIT TO STAND TRIAL: R. V. TAYLOR, 1992
- Describe the difference between acting in one’s own best interests and the limited cognitive capacity test.
- List the three prongs of the Canadian standard for fitness, as set out in Section 2 of the Criminal Code of Canada.
The issue was whether Taylor was able to communicate with his lawyer in a way that was in his own best interests. The judge presiding over the 1992 fitness hearing held that
“[he] can communicate with counsel to the extent that he can speak to counsel, and do so in an articulate manner; however, it is abundantly clear from the opinion of the psychiatrists before me and from the conduct of the accused person during various appearances that have led up to this hearing and at this hearing, and in his evidence given before me, that his delusions are so pervasive and irrational that he is, unlike the accused in R. v. Trecroce, not merely capable of disagreeing with counsel whom he might instruct as to how the case should be conducted, but unable to perceive his own best interests and how those interests should be addressed in the conduct of a trial. I am content that the accused person in this case is not capable to rationally instruct counsel, or rationally conduct a case or rationally communicate with counsel because of this mental disorder” (para. 26).
Fitness/Competency Assessment
Evaluations of fitness to stand trial are the most common form of criminal forensic assessment conducted. Each year more than 5,000 accused individuals in Canada undergo this type of evaluation. Mental health professionals are called upon by the courts to conduct fitness evaluations. In general, they can be conducted in a relatively short period of time on an outpatient basis, although they still occur on an inpatient basis in most jurisdictions. The focus of this type of evaluation is the accused’s current mental state (as opposed to the accused’s mental state at another point in time, such as at the time of the offence; that is the focus of a criminal responsibility evaluation, which is discussed later in this chapter).The evaluator conducts an interview with the accused in an attempt to assess the accused’s current mental state, and to assess whether the accused is able to demonstrate the specific abilities required in order to proceed with the case. Several forensic assessment instruments have been developed to help evaluators assess an accused’s fitness to stand trial. These instruments take many forms but, in general, they all serve to highlight those psycholegal abilities that are required of all accused in order to proceed.
INSIGHT 3.1. Forensic assessment instruments for competency to stand trial
Numerous forensic assessment instruments have been developed to evaluate various types of competencies. The following is a sampling of some of the most well-known instruments. Most of these instruments were developed for use in the United States; however, similar standards for competence allow for their use or adaptation in other countries, such as Canada, Australia, and parts of Western Europe.
Robey’s (1965) Checklist. This was the first foren- sic assessment instrument developed and consisted of a checklist of items to guide a clinician’s evaluations of competency to stand trial.
Competency Screening Test (CST; Lipsitt, Lelos, & McGarry, 1971). This 22-item, sentence-completion task was developed to identify those defendants who are clearly competent, so as to minimize the need for lengthy inpatient evaluations of competence.
Competency to Stand Trial Assessment Instrument (CAI; Laboratory of Community Psychiatry, 1973). This interview-based instrument contains 13 items related to legal issues and serves to provide structure to the evalua- tion of competency to stand trial.
Georgia Court Competency Test (GCCT; Wildman, White, & Brandenburg, 1990). The original version of this instrument contains 17 items, whereas the revision, the Georgia Court Competency Test—Mississippi State Hospital Revision (GCCT-MSH; Johnson & Mullett, 1987) contains 21 items. This instrument asks defendants to visually identify the location of various participants in the courtroom and to answer questions about the roles of various people in the courtroom. Defendants are also asked questions about the alleged crime, consequences, and their relationship with their attorney.
Competence Assessment for Standing Trial for Defendants with Mental Retardation (CAST-MR; Everington & Luckasson, 1992). This instrument, developed for use with this specialized population of defendants, contains 50 items that cover three areas: basic legal concepts, skills to assist defence, and understanding the case event. The first two sections are in multiple-choice format, while the last section comprises open-ended questions.
Interdisciplinary Fitness Interview (IFI; Golding, Roesch, & Schreiber, 1984). This instrument and its revision, the IFI-R (Golding, 1993), were developed to assess both the legal and psychopathological aspects of fitness to stand trial. The IFI-R covers 31 relatively specific psycho- logical abilities that are organized into 11 global domains
Fitness Interview Test (FIT; Roesch, Webster, & Eaves, 1984). This instrument and its revision, the FIT-R (Roesch et al., 2006), were developed to assist in the evaluation of fitness to stand trial by providing 70 questions in 16 different domains divided into three main areas: the abil- ity to understand the nature or object of the proceedings, the ability to understand the possible consequences of the proceedings, and the ability to communicate with counsel. MacArthur Competence Assessment Tool—Criminal Adjudication (MacCAT-CA; Poythress et al., 1999). This instrument contains 22 items that tap three competence-related abilities (understanding, reasoning, and appreciation). The first two sections of the instrument (understanding and reasoning) are evaluated by presenting a vignette to the defendant and asking various relevant questions. The MacCAT-CA uses structured administration and scoring and provides for normative information about a defendant’s competence-related abilities.
Evaluation of Competency to Stand Trial—Revised (ECST-R; Rogers et al., 2004). This instrument contains 18 items that assess four different areas: factual understanding of courtroom proceedings, rational understanding of court- room proceedings, ability to consult with counsel, and over- all rational ability. In addition, this instrument also contains 28 items that act as a screen for feigned incompetency.
Instruments for Assessing Understanding and Appreciation of Miranda Rights (Grisso, 1998). This series of four instruments evaluates various aspects involved in waiving one’s Miranda rights, including comprehension of Miranda rights, comprehension of Miranda-right recognition, comprehension of Miranda vocabulary, and function of rights in interrogation.
Checklist for Evaluations of Competence for Execution (Zapf, Boccaccini, & Brodsky, 2003). This is a checklist of 32 domains to be considered in the evaluation of an offender’s competency to be executed. This checklist contains questions for each of the domains, which can be broken down into four different areas: understanding of the reasons for punishment, understanding of the punishment, ability to appreciate and reason in addition to simple factual understanding, and ability to assist attorney.
Instruments such as the Fitness Interview Test—Revised (FIT-R: Roesch, Zapf, & Eaves, 2006; developed specifically for use in Canada) provide questions to be asked in 16 different domains relevant to proceeding with a criminal case; other instruments, such as the MacArthur Competence Assessment Tool—Criminal Adjudication (MacCAT-CA; Poythress, Monahan, Bonnie, & Hoge, 1999) or the Evaluation of Competency to Stand Trial—Revised (ECST-R; Rogers, Tillbrook, & Sewell, 2004), provide standardized administration and scoring for inquiries related to relevant psycho- legal abilities. These latter two instruments were developed for use in the United States, which has a standard for competency similar to Canada’s. (See Insight 3.1 for a list of competency assessment instruments; the reliability and validity of the assessment instrument should be considered by evaluators when they are selecting an instrument to use in any given case. Discussion of reliability and validity of these assessment instruments is beyond the scope of this chapter, but the interested reader is referred to Zapf & Roesch, 2009). In addition to interviewing the accused and administering any relevant forensic assessment instruments, evaluators may also seek third-party information, such as existing records regarding an accused’s mental health or interviews with family members or others who know the accused well and can speak about the individual’s current ability to function in the context of previous functioning. Once evaluators have completed the evaluation, they will usually write a report to the court detailing their opinions regarding the accused’s abilities. As indicated earlier in this chapter, the court will then either make a determination about the accused’s fitness to stand trial on the basis of the written report or hold a hearing on the issue of fitness and make a final disposition.
Characteristics of Unfit/Incompetent Defendants
Research has indicated that the most common characteristics of individuals who are evaluated with respect to their competency status include being male, single, and/or unemployed; living alone; having a history of contact with both the crim- inal justice and mental health systems; and being diagnosed with a major men- tal disorder (see, for example, Nicholson & Kugler, 1991; Pirelli, Gottdiener, & Zapf, 2011; Roesch & Golding, 1980; Zapf & Roesch, 1998). In a Canadian study of six jurisdictions, 84 percent of those remanded for evaluations of NCRMD, or fitness, were male with a median age of 35 years, and over half had a prior criminal conviction (Latimer & Lawrence, 2006). While women are less frequently remanded, a Québec study found women were twice as likely as men to be found unfit to stand trial (Crocker, Favreau, & Caulet, 2002). As a general statement, approximately 30 percent of those individuals whose fitness to stand trial has been questioned and who are evaluated with respect to their fitness will be found unfit to stand trial. Of course, the exact percentage varies by jurisdiction, but on average about 30 of every 100 accused individuals evaluated will be found unfit, thus leaving 70 of every 100 found fit to stand trial. Much of the research that has been conducted in this area has examined the differences between those deemed fit and those deemed unfit. When these two groups are compared, research indicates that unfit individuals are significantly more likely to be single, unemployed, charged with a minor offence, and diagnosed with a psychotic disorder. They are significantly less likely to be charged with a violent crime or to have substance use disorders than are fit individuals (Hubbard, Zapf, & Ronan, 2003). The majority of unfit accused show symptoms of psychosis, as approximately 60 percent of male unfit accused in the Latimer and Lawrence (2006) Canadian national study were diagnosed with either schizophrenia or delusional disorders. Research examining those variables that predict unfitness indicates that certain diagnoses, such as psychosis, mental retardation, schizophrenia, mood disorders, and organic brain disorders, are predictive of unfitness, as are certain psychiatric symptoms indicative of severe psychopathol- ogy (Nicholson & Kugler, 1991; Warren, Fitch, Dietz, & Rosenfeld, 1991).
Restoration of Fitness
As indicated earlier in this chapter, accused individuals who are deemed unfit to stand trial by the court are usually sent to a forensic hospital for the purposes of restoring them to fitness. The most common form of treatment involves the administration of psychotropic medication; however, some jurisdictions have also established treatment programs designed to increase accused individuals’ understanding of the legal process, or programs which address the problems that hinder their ability to participate in their defence (Bertman et al., 2003). The Criminal Code (s. 672.58) allows the judge to order treatment of a person found unfit to stand trial. The term “treatment” is not defined, but it most certainly includes administration of psychotropic drugs. As a general statement, most unfit accused are restored to fitness within six months, and the vast major- ity achieve fitness within one year.A comparison of unfit accused deemed not restorable with those deemed restorable indicated that those individuals considered restorable tended to be younger and were more likely to have a diagnosis of a nonpsychotic disorder, a previous criminal history, and a better understanding of the criminal justice system (Hubbard et al., 2003).In Canada, accused individuals who are found unfit to stand trial may be either detained in the hospital for the purposes of restoration to fitness or conditionally discharged. A court must review the case of each individual found unfit to stand trial every two years to determine whether sufficient evidence remains to bring the accused to trial (i.e., a prima facie case). In those cases where there is no longer enough evidence to bring an individual to trial, the charges will be dropped. The adoption of Bill C-10 in 2005 allows for one more possible outcome for an accused found unfit to stand trial: a stay of proceedings may be granted to an accused who is unlikely to ever become fit to stand trial and who poses no significant threat to the public. A stay of proceedings effectively terminates all further court inquiries into a prima facie case and the ongoing review board hearings for the permanently unfit individual.
3. 2 Criminal Responsibility
Learning Objective 3.2
Summarize the legal standards and procedures for determining criminal responsibility or insanity.
criminal responsibility refers to the mental state of the accused at the time of the crime
not criminally responsible on account of mental disorder (NCRMD) a defence in which a person is not held criminally responsible for an act committed while suffering from a mental disorder that made the person incapable of appreciating the nature and quality of the act or of knowing that it was wrong; colloquially known as the insanity defence
The issue of criminal responsibility relates to an accused’s mental state at the time of the alleged offence. In Canada, an accused can mount a defence called not criminally responsible on account of mental disorder (NCRMD), colloquially known as the insanity defence. The basic philosophy behind this defence is that to convict a person charged with a crime, that person must be considered responsible for his or her behaviour. Recall from Chapter 2 that for most crimes there are two elements the Crown must prove in order for an accused to be found guilty: the actus reus, or physical act of the crime, and the mens rea, or mental capacity and intention to commit the crime. Many scholars have conceptualized the “insanity defence” as negating the mens rea, although some conceptualize it as negating the actus reus (i.e., the voluntariness of actions). It is not necessary to resolve this debate here. We proceed on the basis that a ruling of NCRMD negates the mens rea. As a general statement, accused individuals for whom mental disease or defect has resulted in an inability to form the intention to commit a crime or has resulted in an inability to know or appreciate that it was wrong may be considered not criminally responsible for their actions and thus found NCRMD. Case Study 3.2 provides an example of an offender who was found NCRMD.
CASE STUDY 3.2 – TRAGEDY ABOARD BUS 1170
To many, this brutal crime might conjure images of Hannibal Lecter, the psychopathic killer played by Anthony Hopkins in the famous movie Silence of the Lambs. However, there is one important difference. In Silence of the Lambs, Hannibal Lecter was acutely aware of his actions and knew that what he was doing was wrong. As is explained below, this was not the case with Mr. Li. In fact, Mr. Li was suffering from a mental disorder which rendered him unable to appreciate the nature and quality of his actions and to know that they were wrong.At Mr. Li’s second-degree murder trial, which began nearly a year later on March 5th, 2009, the Crown and defence attorneys agreed to a number of facts. Among them was the fact that Mr. Li had few friends and those he did have described him as having had mental problems. In addition, his former wife described him engaging in bizarre behaviours, including sudden and unexplained absences, bus trips to unusual locations, and rambling talk. Despite his unusual behaviour, neither his friends nor his former wife had known him to be violent. One episode of unusual behaviour resulted in the Ontario Provincial Police picking him up on a busy highway. He was hospitalized briefly in the fall of 2005 before being released with medication. Both before and after this incident, friends and family were unable to convince him to seek medical help.At his trial, psychiatric assessments of Mr. Li were put into evidence. In particular, the assessments suggested that Mr. Li was suffering from schizophrenia. Schizophrenia is a mental illness whose symptoms can include hallucinations, delusions, and paranoia. According to the psychiatrists’ assessments, the voice of God had directed Mr. Li to move from Edmonton to Winnipeg. Moreover, the voice had led Mr. Li to believe, under a paranoid delusion, that the deceased victim was a threat to his own life, both before and after the deceased victim’s death. The judge accepted the assessments that Mr. Li was suffering from a mental disorder. In his decision, he said,
These grotesque acts are appalling. However, the acts themselves and the context in which they were committed are strongly suggestive of a mental disorder. He did not appreciate the actions he committed were morally wrong. He believed he was acting in self-defence.
Moreover, the judge stated,
Persons who are profoundly ill do not have the mental capacity to intentionally commit a crime. The goal of criminal law is to punish criminals, not persons who have a mental illness. Moreover, a person who is driven to act by severe psychotic delusions cannot be deterred by the fear of punishment, or public denouncement. In such cases, the only way to change the behaviour of a person who is driven to act by psychotic delusions is through treatment, and where the person poses an ongoing risk to society, through treatment in a secure institution.
As a result of these findings, the judge found Mr. Li not criminally responsible on account of mental disorder (NCRMD). Under Canadian law, no person is criminally responsible for an act committed while suffering from a mental disorder that rendered the person incapable of appreciating the nature and quality of the act or of knowing that it was wrong (Criminal Code of Canada, C-46, s. 16(1)). However, not all individuals who are suffering from a mental disorder will be found NCRMD. Rather, an indi- vidual will only be found NCRMD if the mental disorder, which is defined in law as a disease of the mind, ren- ders the person unable to differentiate between right and wrong. In Winko v. British Columbia (Forensic Psychiatric Institute), the Supreme Court of Canada put it this way:
“people who commit criminal acts under the influ– ence of mental illnesses should not be held crimi– nally responsible for their acts or omissions in the same way that sane responsible people are. No person should be convicted of a crime if he or she was legally insane at the time of the offence. . . . Criminal responsibility is appropriate only where the actor is a discerning moral agent, capable of making choices between right and wrong.”
In cases where individuals are found NCRMD, they are not admitted to jail or prison. Rather, their disposi- tion depends on a number of considerations, includ- ing the protection of the public, the individual’s mental condition, the reintegration of the individual into society, and the individual’s other needs. Disposition decisions are made by specially constituted Review Boards whose duty it is to weigh these considerations. The disposition of Mr. Li was decided by the Manitoba Review Board on September 15th, 2009. His disposition order required him to be detained in a locked ward of a psychiatric hospital in Manitoba. When the order was reviewed on May 31st, 2010, the Review Board again ordered him to be detained in a locked ward of a psychiatric hospital in Manitoba. However, this time they allowed for the possi- bility of escorted access to the hospital grounds (e.g., out- side yard). Disposition orders are reviewed by the Review Board at least annually. Mr. Li is currently being held at the Selkirk Mental Health Centre in Manitoba.
- Describe the difference between fitness to stand trial and criminal responsibility (insanity).
- List the ways in which Mr. Li (described above) is representative of the typical insanity acquittee
Legal Standards for Criminal Responsibility
M’Naghten
The oldest test of legal insanity stems from the case of Daniel M’Naghten, which took place in England in the early 1840s. Daniel M’Naghten was acquitted on a charge of murdering Edward Drummond, the secretary to the British prime minister, Sir Robert Peel, whom he shot in the back, thinking it was the prime minister. M’Naghten was labouring under the delusional belief that the prime minister was responsible for his personal and financial misfortunes. In this case, the court established what has come to be known as the M’Naghten standard, also called the knowledge/right-wrong test of insanity. This standard requires that, in order to establish a defence on the grounds of insanity,
it must be clearly proved that, at the time of the committing of the act, the party accused was labouring under such a defect of reason, from disease of the mind, as not to know the nature and quality of the act he was doing; or, if he did know it, that he did not know he was doing what was wrong. (M’Naghten’s Case, 1843, p. 722)
The M’Naghten test remains the standard in Canada. As you learned at the beginning of this chapter, the starting point is competence. All accused are assumed to be free of mental disorder unless otherwise proven, on balance of probabilities, by the party who raised the issue. The Criminal Code states that “[n]o person is criminally responsible for an act committed or an omission made while suffering from a mental disorder that rendered the person incapable of appreciating the nature and quality of the act or omission or of knowing that it was wrong” (s. 16). Take note of the fact that a mental disorder is a necessary condition for a finding of NCRMD, but it is not sufficient. The mental disorder must cause very particular deficits.
To “appreciate the nature and quality” involves more than knowing what you are doing; it must include a minimal understanding of the consequences of the action. In Cooper v. the Queen (1979) the accused was convicted of murder—he choked his victim, causing her death. The Supreme Court of Canada held that, due to the accused’s mental illness, he knew that he was choking the victim, but he did not know that the act could lead to her death. To be morally culpable, the accused must have some minimal understanding of the nature and quality of the act—in this case, that choking could lead to death. The appellant was convicted at trial but the Supreme Court of Canada overturned the conviction and ordered a new trial.
The meaning of “wrong” in the NCRMD criteria includes either legally wrong or morally wrong. In R. v. Chaulk (1990), a 15-year-old and a 16-year-old were charged with the murder of a homeowner whose home they broke into. The youths were suffering from a form of psychosis that led them to believe that they had the power to rule the world and that this killing was necessary to achieve this end. The youths knew the act was legally wrong, but they failed to understand that it was morally wrong. They believed they should rule the world and this was the only way to accomplish that goal. The trial judge held that the insanity defence (NCRMD) was not open to the accused because they understood that the act was legally wrong. The Supreme Court of Canada overturned the trial decision and ordered a new trial. It held that “wrong” means either the accused did not under- stand the act was legally wrong, or did not understand the act was morally wrong.
This does not mean that the accused must appreciate the legal consequences of the act. In R. v. Abbey (1982), the accused imported drugs into Canada. He knew that it was wrong but was delusional and believed he was immune from prosecution. At trial he successfully raised the insanity defence; however, that decision was overturned at the Supreme Court of Canada, which held that the defence cannot be used if the accused believed he was immune from prosecution, even if that belief comes from a disease of the mind.
Who can raise the issue of the accused’s mental state at the time of the offence? Recall Case Study 3.1. In R. v. Taylor (1992), the verdict of not guilty by reason of insanity (as it was called in 1992) was overturned because the Crown raised the issue of the accused’s mental state at the time of the offence. In R. v. Swain (1991) the Supreme Court of Canada held that the Crown could raise the issue of the accused’s criminal responsibility in only a few particular circumstances: after a guilty verdict has been rendered, and if accused individuals raise the issue of their mental state for any purpose during trial. The court held that it would be unfair to allow the Crown to raise the issue of sanity for two reasons. First, it could influence how the trier of fact evaluates the evidence. Second, it is contrary to accused individuals’ right to fundamental justice to control their own defence.
Public Perceptions of the Insanity Defence
Much of the research on perceptions of the “insanity defence” has been done in the United States, and it provides the most relevant data available. Although the name of the defence is different (i.e., not guilty by reason of insanity), the essen- tial elements of the defence are similar.
Public perceptions of the insanity defence are that it is frequently used, frequently successful, and serves as a “loophole” guilty people use to go free (Hans, 1986). However, empirical research on whether these public perceptions are accurate reveals that the public overestimates both the use and success of the insanity defence and underestimates the length of confinement of insanity acquittees (Silver, Cirincione, & Steadman, 1994).
Although the exact rates of use and success vary by jurisdiction, as a general statement, the insanity defence is rarely used and is even more rarely successful. Silver and colleagues (1994) compared public perceptions of the insanity defence with empirical data on its actual use and found that the public estimates the use of the insanity defence to be 37 percent (or 37 times per 100 felony indictments), whereas the actual use is 0.9 percent (less than once per 100 felony indictments), representing a public estimate that is 41 times greater than its actual use. Similarly, with respect to estimates regarding the success of the insanity defence, these authors report that the public estimates the success rate to be 44 percent (or 44 acquittals per 100 insanity pleas) whereas the actual rate of success of 26 percent. As Silver et al. conclude, “This means that for every 1,000 felony cases, the public would estimate 370 insanity pleas of which 44% (163) would be estimated as successful. In fact, there are only nine insanity pleas for every 1000 felony cases of which 26% (about 2) are successful. The public’s estimate of the number of insanity acquittals is 81 times the actual number” (pp. 67–68).
Silver et al. (1994) also examined the distribution of charges for persons pleading insanity to determine whether the public’s perception—that the majority of accused pleading insanity are murderers—was accurate. These researchers reported that approximately 14 percent of accused individuals pleading insanity were charged with murder, whereas about 54 percent were charged with other violent offences and 32 percent were charged with nonviolent offences. Again, public perceptions of accused individuals pleading insanity greatly overestimate the proportion of accused charged with murder.
With respect to public perceptions regarding what happens to “successful” insanity acquittees, the public estimates that approximately half of these individuals are hospitalized, but Silver et al. (1994) report that, in reality, about 85 percent are hospitalized. Similarly, these authors report that the public overestimates the pro- portion of insanity acquittees who “go free” upon acquittal, with a public estimate of 26 percent going free compared to the actual rate of 15 percent. The authors also indicate that if conditional release and outpatient treatment are excluded from the definition of “going free,” the actual rate drops to a mere 1 percent.
When Silver et al. (1994) compared public estimates of the length of confine- ment of insanity acquittees to actual lengths of confinement, they found, again, that the public underestimates the actual length of confinement. The public estimates an average length of confinement of just under two years (21.8 months) versus an actual average length of confinement of over two and a half years (32.5 months) for all persons (regardless of charge), and almost six and a half years (76.4 months) for those charged with murder.
In Canada, the insanity defence (NCRMD) is rarely successful (Livingston, Wilson, Tien, & Bond, 2003). Research examining the impact of Bill C-30, which was introduced in 1992 to change the provisions for the evaluation and treatment of accused raising the issue of insanity or fitness in Canada (and which was thought to make the insanity plea more attractive to accused because of its emphasis on the community management of these individuals, as well as its proposed caps on the length of confinement for acquittees), indicates that the number of cases remanded for evaluation did indeed increase. Between 2002 and 2004 there was a 102 percent increase in the total number of admissions across Canada (Latimer & Lawrence, 2006). This was not due to an increase in the number of court cases, but to a real increase in the percentage of remanded cases, as the rate was 1.2 per 1,000 court cases in 1994/95 and 1.8 per 1,000 cases in 2003/04. It is expected that this trend will continue, as shown in Figure 3.3.
However, while the number of accused raising the insanity issue has increased, rates of acquittal have remained relatively constant (Arboleda-Florez, Nussbaum, Ohayon, & Roesch, 2000). It appears that the insanity defence is used even more rarely outside North America. In Ireland, for example, Gibbons, Mulryan, and O’Connor (1997) reported an average of one insanity acquittal per year since 1910, and indicate that this defence is used only for the most serious of offences (95 percent of acquittees had been charged with violent offences, 72 percent of which were infanticide or homicide) and is successful in only about 2 to 3 percent of homicides.
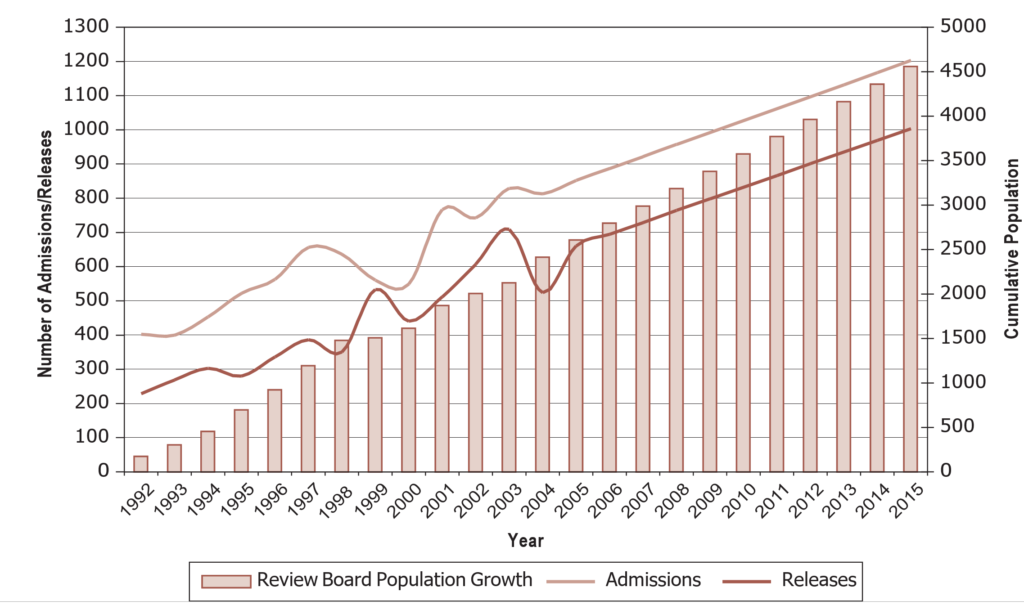
Note: 2005 to 2015 based on projections using existing trend
Source: Latimer, J., & Lawrence, A. (2006). The review board systems in Canada: Overview of results from the mentally disordered accused data collection study. Ottawa: Department of Justice Canada, p. 22. Retrieved from www.justice.gc.ca/eng/rp-pr/csj-sjc/
jsp-sjp/rr06_1/rr06_1.pdf, Justice Canada, 2006. Reproduced with permission of the Minister of Public Works and Government Services Canada, 2013.
Assessment of Criminal Responsibility
As discussed previously, the determination of fitness to stand trial is based on the accused’s mental state at the present time. Criminal responsibility, however, takes into consideration the accused’s mental state at the time of the alleged offence. Thus, in this type of evaluation, the psychologist or other mental health professional is attempting to assess the accused’s mental state at some earlier point in time— so this is a retrospective evaluation. Similar to evaluations of fitness to stand trial and other forensic issues, the evaluation of criminal responsibility or mental state at the time of the offence usually involves an interview with the accused and a review of relevant records (including any available mental health records), as well as the police report. Interviews may be conducted with individuals who know the accused well or who were with the accused at or around the time of the offence, and any relevant psychological tests or forensic assessment instruments can be administered. Evaluations of mental state at the time of the offence may take place on either an inpatient or an outpatient basis, depending on the rules of the jurisdiction in which the evaluation takes place.
Although several forensic assessment instruments have been developed for use in assessments of fitness to stand trial, there has only been one published instrument developed for use in assessments of criminal responsibility—Rogers Criminal Responsibility Assessment Scales (R-CRAS; Rogers, 1984). The R-CRAS was developed as a way to standardize the collection of information for evaluations of criminal responsibility using a U.S. standard known as the American Law Institute (1962) standard, but it can also be adapted for use with M’Naghten standards.
An accused who presents an insanity defence at trial will present evidence of mental impairment at the time of the offence, usually in the form of a written report by a psychologist or other mental health professional who has carried out an evaluation of the accused’s mental state at the time of the offence. If an accused raises the issue of mental state by using an insanity defence at trial (or by declaring the intention to pursue an insanity defence), the prosecution then has the right to have an evaluation of that accused’s mental state at the time of the offence conducted by an expert of its choosing. If the case proceeds to trial (recall that the vast majority of cases are resolved by a guilty plea or a plea bargain), experts for both sides (Crown and defence) may testify about the accused’s mental state, and the decision regarding whether the accused is to be held accountable for the actions in question rests with the legal decision maker in the case—the jury or, if there is no jury, the judge.
Researchers have examined the process by which insanity pleas make it to court and whether insanity pleas are heard by judge or jury. Janofsky, Dunn, Roskes, Briskin, and Lunstrum (1996) examined the outcomes for all insanity pleas raised over a one-year period in Baltimore City’s district and circuit courts and found that almost 96 percent of the pleas did not make it to court. The vast majority of accused withdrew their insanity plea immediately after undergoing an insanity evaluation, while others either had their charges dropped before trial or were found unfit to proceed to trial. Only about 4 percent of the initial insanity pleas made it to court. In all these cases, the insanity pleas were not contested by either the prosecution or the defence, and the accused were found not criminally responsible.
Cirincione (1996) examined the processing of insanity pleas and determined that the vast majority of insanity cases were handled through either plea bargain (42.9 percent) or bench trial (42.7 percent), with relatively few (14.4 percent) handled via jury trial. The success of the insanity defence varied considerably by type of adjudication. Only about 16 percent of jury trials and 11 percent of plea bargains resulted in an insanity acquittal, compared to almost 55 percent of bench trials. In interpreting these results, Cirincione speculated that jury trials are more commonly used in contentious cases (involving severe crimes and less mental disorder), whereas bench trials are more likely when the prosecution does not contest the insanity claim or when the judge is more likely to be convinced by the defence’s arguments.
Characteristics of Insanity Defence Acquittees
Although there are always exceptions to any rule, a relatively consistent picture of the model insanity acquittee has emerged. Research examining the demographic characteristics of insanity acquittees in the United States(Cirincione, Steadman,& McGreevy, 1995) and Canada (Roesch et al., 1997) indicates that the typical insanity acquittee is male, between the ages of 20 and 29, single, unemployed, minimally educated, and diagnosed with a major mental illness; has had prior contact with the criminal justice and mental health systems; and is acquitted for a violent offence (see also Lymburner & Roesch, 1999).
In terms of the types of mental illness that insanity acquittees suffer from, research has consistently demonstrated that the majority of insanity acquit- tees are diagnosed with psychotic disorders. In the United States, Wack (1993) reported that 62 percent of insanity acquittees in New York were diagnosed with a psychotic disorder, whereas Bloom and Williams (1994) reported that 60 percent of insanity acquittees in Oregon were diagnosed with schizophrenia (a major mental disorder with prominent psychotic features). The situation is similar in Canada, with Roesch et al. (1997) reporting that over 50 percent of insanity acquittees in British Columbia and Hodgins (1993) reporting that 63 percent of insanity acquittees in Quebec were diagnosed with schizophrenia.
Treatment of Insanity Defence Acquittees
If a court finds that an accused is NCRMD, it may choose one of three dispo- sitions: an absolute discharge, a conditional discharge (i.e., the accused may live in the community but with conditions), or detention in hospital (with or without conditions). Alternatively, and very frequently, the court may refer the decision to the review board of the appropriate province or territory. Any disposition, other than an absolute discharge, must be reviewed by a review board each year until it determines that the accused is not a significant threat to the safety of the public and discharges the accused absolutely.
The majority of individuals found NCRMD are initially detained in psy- chiatric hospitals or forensic institutions for a period of confinement and treat- ment of their mental disorder. The length of the period of confinement varies considerably by jurisdiction. In addition, there does not appear to be a consistent pattern across jurisdictions in terms of whether insanity acquittees are held for longer or shorter periods than individuals convicted of the same type of crime— in some jurisdictions, insanity acquittees are held, on average, longer than convicted individuals; in other jurisdictions the reverse is true, while in others there is no difference.
3.3 Risk Assessment
The question of whether an accused is a risk to commit a future offence may arise at many points in the criminal justice system, although it most often comes up at either sentencing or release. Mental health professionals are increasingly being called upon by the criminal justice system to conduct assessments of an accused’s level of risk to commit a violent offence, a sexual offence, or some other type of criminal behaviour. Treatment options for the accused are partially determined by relevant risk factors for each individual. While the assessment of an individ- ual’s future risk may occur at any time, these assessments usually occur in one of two contexts: just before sentencing, when an individual’s level of risk may affect the type of sentence that is imposed and the type of treatment programming that is offered; and just before release, when they inform the court about strategies for reducing an offender’s level of risk, which may in turn affect the release decision or the conditions imposed upon that release. Risk assessment occurs in both the civil (e.g., risk for violence toward oneself or others) and criminal (e.g., risk for future sexual violence) arenas; however, the focus in this chapter is on the criminal arena. We begin this section by describing the various points at which a risk assess- ment may be conducted.
Learning Objective 3.3
Describe the points at which risk is assessed, the three approaches to risk assessment, and the factors used to assess risk.
Points at Which Risk Assessment Might Occur
Bail
Section 11(e) of the Canadian Charter of Rights and Freedoms states, “Any person charged with an offence has the right not to be denied reasonable bail without just cause.” Just cause exists if, for example, the accused poses a risk if released into the community. Accordingly, people in the criminal justice system must assess risk when an individual is brought before them to request bail. Often, these decisions are made quickly and without benefit of expert psychological evidence; however, the person making the decision to release does undertake a risk assessment.
Sentencing
Most offences carry maximum sentences but not minimum sentences, so judges have a great deal of discretion in terms of the length of sentence. The individual’s risk of offending in the future, as well as the possibility of managing this risk, are important factors to consider when deciding the most appropriate sentence in the circumstances.
Dangerous Offender Hearings
Section 753 (1) (a) of the Criminal Code states that a person may be designated a “dangerous offender” (and may be sentenced to detention in a penitentiary for an indeterminate period) if “the offence for which the offender has been convicted is a serious personal injury offence . . . and the offender constitutes a threat to the life, safety or physical or mental well-being of other persons.” Section 752 of the Criminal Code defines a “serious personal injury offence” as “an indictable offence, other than high treason, treason, first-degree murder or second-degree murder, involving the use or attempted use of violence against another person, or conduct endangering or likely to endanger the life or safety of another person or inflicting or likely to inflict severe psychological damage on another person, and for which the offender may be sentenced to imprisonment for ten years or more, or an offence or attempt to commit an offence [that is a sexual assault].”
Long-Term Offender Hearing
Section 753.1(1) of the Criminal Code allows for a designation of “long-term offender” (which orders that “the offender be subject to long-term supervision for a period that does not exceed 10 years” following the period of incarceration) when it would be appropriate to impose a sentence of imprisonment of two years or more for the offence for which the offender has been convicted, there is a substantial risk that the offender will reoffend, and there is a reasonable possibility of eventual control of the risk in the community. When you consider dangerous offender legislation and long-term offender legislation, you should note that an important distinction is the potential management of future risk.
Remand Assessments
A remand facility is a provincial institution that detains individuals who are serving a sentence of less than two years, were given a federal sentence and are remaining in remand until their appeal period expires, have outstanding charges or are awaiting transfer to another facility, or are detained for other administrative or legal reasons (e.g., immigration holds). In a remand facility, brief assessments are done with a particular focus on identifying major mental illnesses and/or the need for short-term urgent intervention.
Intake Assessment
Upon arrival at a federal institution (where people are held for sentences of two years of more), all offenders are immediately assessed for suicide risk, risk of harm to others, and other issues (e.g., health care needs). The purpose of intake assessment is to determine the level of security needed, the type and intensity of treatment, and the likelihood of recidivism.
Probation/Parole
Generally, probation refers to conditional release from a provincial sentence, and parole describes conditional release from a federal sentence. A period of probation may be passed as the entire provincial sentence or as part of a provincial sentence. An important consideration when assessing probation is the risk that the offender will reoffend if released into the community. Unless there is a minimum sentence (e.g., first-degree murder), offenders are eligible to apply for parole after serving only one-third of their sentence, and it may be granted if the offender can convince the parole board that release is appropriate. Except in cases where there is a minimum sentence, offenders must be released after serving two-thirds of their sentence—this is called statutory release—unless the Crown can establish that the offender should not be released. When a parole hearing is conducted, an assessment of future risk is essential if the parole board is to make its decision.
Not Criminally Responsible on Account of Mental Disorder (NCRMD)
Individuals who have been found to be NCRMD and detained in a psychiatric institution may be assessed and released only if, among other things, they no longer pose a significant threat to the safety of the public. These individuals are evaluated for their risk of violence to others and to themselves on a regular basis while institutionalized, and they can only be released if a risk assessment indicates that they are not a significant threat to themselves or to the public.
Approaches to Risk Assessment
There are three different approaches to risk assessment. The first is known as clinical decision making or unstructured clinical judgment. This approach is ideographic (that is, it focuses on the specific individual rather than on groups of individuals) and qualitative (it relies on subjective judgments) in nature. Thus, clinicians who are conducting violence risk assessments in this manner will use their best clinical judgment to gauge the likelihood that the examinee will be violent in the future. The risk markers that are taken into consideration vary by clinician, as does the weighting of each of the relevant factors for each specific case.
In contrast to the clinical decision-making approach is actuarial decision making. The actuarial approach is nomothetic (based on research involving large groups of people) and quantitative (statistical) in nature. Thus, clinicians who conduct violence risk assessments in this manner will use a formal, algorithmic, objective approach to make a decision regarding the likelihood that the examinee will be violent in the future. Clinicians must incorporate their professional experience by using a formulaic approach that takes into consideration specific risk markers, each given a specific weight. When directly compared with decisions made using unstructured clinical judgment, actuarial decisions have been found to be considerably more accurate.
The third approach to risk assessment, structured professional judgment, involves a melding of the clinical and actuarial approaches. In this approach, a specific array of risk markers is considered, thus ensuring that all clinicians take into consideration the same set of risk factors for each examinee. In addition, clinicians are able to introduce their professional experience to temper or augment the actuarial prediction. Thus, the ztructured professional judgment approach to violence risk assessment ensures the consideration of a relatively comprehensive set of risk factors for every examinee and allows for additional, individual factors to be considered as a supplement to the structured assessment. It has long been recognized that the actuarial approach is superior to unstructured clinical judgment; however, a meta-analysis comparing the actuarial and structured professional judgment approaches indicated no distinct superiority for either actuarial or SPJ model (Guy, 2008). The author concluded that both models performed at comparably good levels of predictive accuracy, but that additional relevant factors should be considered when selecting an approach for clinical practice.
unstructured clinical judgment one of three approaches to risk assessment, and the least effective in predicting violence; in this approach clinicians use their best clinical judgment to gauge the likelihood that the examinee will be violent in the future; the risk markers that are taken into consideration vary by clinician, as does the weighting of each of the relevant factors for each specific case
actuarial decision making one of three approaches to risk assessment, based on actuarial data
structured professional judgment one of three approaches to risk assessment; in this approach, a specific array of risk markers is considered, and clinicians are also able to introduce their professional experience; structured professional judgment instruments are based on research identifying predictors of future risk that do not tell evaluators how risk factors should be weighted or combined and cannot be used to estimate the probability of future harm
Violence Risk Factors
Numerous risk factors have been identified as being related to an increased risk for violence. These risk factors include both static (stable, unchangeable) and dynamic (changeable) factors, as shown in Table 3.1.
These risk factors have formed the basis of a number of risk assessment instruments. Although many risk factors are important to consider across many contexts, the risk assessment instruments have, generally, been developed for a specific purpose. That is, some instruments have been developed to assist in the evaluation of risk for violence, while others focus specifically on intimate partner violence or sexual violence.
Risk assessment instruments fall into one of two categories—those that are actuarial and those that were developed to assist in structured professional judgments of risk for violence. Instruments such as the Violence Risk Appraisal Guide (VRAG; Quinsey, Harris, Rice, & Cormier, 2005) and the Violence Prediction Scheme (VPS; Webster, Harris, Rice, Cormier, & Quinsey, 1994) are actuarial, whereas the HCR-20 (Webster, Douglas, Eaves, & Hart, 1997), the Spousal Assault Risk Assessment Guide (SARA; Kropp, Hart, Webster, & Eaves, 1998), and the Sexual Violence Risk-20 (SVR-20; Boer, Hart, Kropp, & Webster, 1997) were developed to assist in structured professional evaluations of risk (see Insight 3.2 for a description of risk assessment instruments).
| Table 3.1 Violence Risk Factors |
|
|
Static (Stable, Unchangeable) Risk Factors |
Dynamic (Changeable) Risk Factors |
|
Past violent behaviour |
Lack of insight |
|
Young age |
Negative attitudes and personality states |
|
Relationship instability |
Psychiatric symptomatology |
|
Employment instability |
Behavioural and affective instability |
|
Substance use |
Unresponsiveness to treatment |
|
Major mental disorder |
Lack of feasible release plan |
|
Psychopathy (discussed later) |
Access to victims, weapons, drugs, and alcohol |
|
Early home or school maladjustment |
Lack of support and supervision |
|
Personality disorder |
Noncompliance with medication or other treatment |
|
Violations of conditional release |
Stress |
|
Escapes or attempted escapes from incarceration |
|
INSIGHT 3.2. Forensic assessment instruments for risk assessment
- HCR-20 (Webster, Douglas, Eaves, & Hart, 1997; Douglas, Hart, Webster, & Belfrage, 2013). This 20-item assessment tool includes information and criteria for evaluating 10 historical factors, 5 clinical factors, and 5 risk management factors, and encompasses past, present, and future risk considerations.
- SVR-20 (Boer, Hart, Kropp, & Webster, 1997). This 20-item assessment tool includes information and criteria for evaluating 11 psychosocial adjustment, 7 sexual offence, and 2 future plans variables for the evaluation of violence risk in sex offenders.
- Violence Risk Appraisal Guide (VRAG; Quinsey, Harris, Rice, & Cormier, 2005). This 12-item actuarial scale is used to predict the probability of violence within a particular time frame in offenders with mental disorders.
- Sex Offender Risk Appraisal Guide (SORAG; Quinsey, Harris, Rice, & Cormier, 2005). This 14-item instrument is used to predict the probability of violent and sexual recidivism in previously convicted sex offenders.Rapid Risk Assessment for Sex Offense Recidivism (RRASOR; Hanson, 1997). This brief, four-item screening instrument is used to evaluate risk for sexual violence in previously convicted sex offenders.
- STATIC-99/STATIC-2002 (Hanson & Thornton, 1999). These ten-item instruments are used to determine the long-term potential for sexual recidivism in male sex offenders.
- Sex Offender Need Assessment Rating (SONAR; Hanson & Harris, 2000). This nine-item scale is used to measure changes in the level of risk for sex offenders.Minnesota Sex Offender Screening Tool (MnSOST-R; Epperson, Kaul, & Hesselton, 1998). This 16-item instrument is used to determine level of risk for sexual recidivism among rapists and intrafamilial child molesters.
Psychopathy
Psychopathy is a personality type that encompasses both behavioural and affective (emotional) components. Individuals who exhibit psychopathy are, among other things, glib, grandiose, callous, remorseless, reckless, manipulative, impulsive, dishonest, parasitic, and unable to experience the normal range and depth of emotional experience. Psychopathy plays an important role in risk assessment, because the available research has consistently demonstrated a significant relationship between psy- chopathy and violence. That is, individuals with psychopathic personality styles are more likely to engage in general criminal behaviour and violent behaviour than their nonpsychopathic counterparts. Moderate to major associations between psychopathy and violence have been found (Hemphill, Hare, & Wong, 1998; Salekin, Rogers, & Sewell, 1996). As Douglas and Webster (1999) have concluded, “Psychopaths, in comparison with nonpsychopaths, are at an increased risk for acting violently and for doing so more quickly and in more diverse ways and across various settings, whether they are mentally disordered, sex offenders, young offenders, or just ’regular’ nonmentally ill offenders” (p. 204). Given the robustness of the relationship between psychopathy and violence, it is important to take this personality type into consideration in every risk assessment.
Violence Risk Assessment
Violence risk assessment attempts to take into consideration many different fac- tors, including (a) the nature of the violence or the types of violence that may occur; (b) the severity or seriousness of the violence; (c) the frequency of the violence, or how often violence might occur; (d) the imminence of violence, or how soon it might occur; and (e) the likelihood or probability that violence will occur. Evaluators are often called upon by the courts to assess an individual’s risk for violence, whether for sentencing or release purposes, and therefore must attempt to delineate each of these factors.
An informative and useful risk assessment will provide the court with information on the probability that the examinee will commit a particular type of violence within a particular time frame and under certain conditions. Thus, risk management is a crucial component of risk assessment. Risk management refers to the strategy of attempting to reduce the probability that an individual will be violent by describing the conditions under which that individual’s risk for violence may increase and those under which it may decrease. Thus, to manage an individual’s risk, one must know the conditions that may serve to increase and/or decrease the probability of violence so that these conditions can be monitored and/or adjusted accordingly. For instance, the use of alcohol or drugs may serve to increase an individual’s risk for violence; therefore, an appropriate risk management strategy would include treatment for substance abuse and careful monitoring to ensure that the individual abstains.
Sentencing and release decisions by the courts can then be made based on the information provided in a risk assessment, and specific sentencing and/or release conditions may be implemented in an attempt to manage the individual’s risk for future violence.
As in other types of criminal forensic evaluations, an interview with the offender as well as a review of all available records and interviews with other individuals who know the offender well are involved in an assessment of an offender’s risk for future violence. In addition, most risk assessments also entail the use of one or more of the specific forensic assessment instruments that have been developed to assist in making a determination about an offender’s level of risk.
3.4 Psychopathy and Malingering
There are two overarching issues that must be assessed, either formally or informally, by the examiner in any forensic evaluation: psychopathy and malingering (faking).
Learning Objective 3.4
Describe psychopathy and malingering and explain how they are assessed.
antisocial personality disorder (APD) a personality disorder consisting of a pervasive pattern of disregard for, and violation of, the rights of others
malingering the false production or exaggeration of symptoms of mental illness or cognitive deficit with the intention of obtaining some secondary gain
Psychopathy
Psychopathy is a constellation of affective, interpersonal, and behavioural characteristics. It arises as a clinical issue in the full range of criminal forensic assessments, with specific repercussions in the assessment of risk for violence (as discussed earlier). Psychopathy is an important concept in forensic evaluations, as the constellation of personality traits involved in psychopathy often has a significant impact on how individuals understand and function within their environment. Forensic evaluators must always consider the concept of psychopathy in any evaluation context, at least informally if not formally.
The modern concept of psychopathy was introduced by Hervey Cleckley in his classic text The Mask of Sanity (1941). Cleckley described the person with psychopathy as lacking emotional responsiveness, having no sense of shame, being superficially charming and manipulative, showing irresponsible behaviour, and being inadequately motivated. Many researchers, but especially Robert Hare and his colleagues, have continued to develop the concept of psychopathy throughout the last three decades and have been instrumental in describing how it is distinct from (and similar to) the concept of antisocial personality disorder (APD). Generally speaking, psychopathy is a broader concept than APD and encompasses an interpersonal/affective component in addition to the mainly behavioural component of APD.
Several instruments have been developed to assess the characteristics associated with psychopathy; however, there is none as well known as Hare’s Psychopathy Checklist–Revised (PCL-R: Hare, 1991, 2003). The PCL-R consists of 20 items that are rated on the basis of file information and an interview with the examinee. Scores on the PCL-R range from 0 to 40, with a cutoff of 30 commonly used to denote psychopathy. In addition to the PCL-R, a screening version (PCL:SV; Hart, Cox, & Hare, 1995) and a youth version (PCL:YV; Forth, Kosson, & Hare, 2003) have been developed.
Malingering
Malingering is the feigned production or exaggeration of psychological or physical symptoms to achieve some external incentive. It must be ruled out in every legal context. The American Psychiatric Association (2000) defines malingering as “the intentional production of false or grossly exaggerated physical or psycho- logical symptoms, motivated by external incentives such as . . . evading criminal prosecution” (p. 739). Further, malingering is to be “strongly suspected” in a “medicolegal context” (p. 739), which, of course, includes all criminal forensic evaluations.
The validity of psychological assessment instruments hinges on examinees being honest and forthright in their effort and responses, and the same is true for most forensic assessment instruments. In order for results to be valid, examinees must be honest and sincere in their effort and responses. The formal evaluation of malingering might include the use of a forensic assessment instrument developed specifically for the purposes of detection of malingering. In contrast, an informal evaluation of malingering might involve only a very close scrutiny of self-reported information and various collateral sources of information, without any specific testing targeted toward the issue of malingering.
There are two areas where an individual might attempt to malinger: the display of psychiatric symptoms or of cognitive impairment. Malingering psychiatric symptoms would involve pretending to be experiencing symptoms of a mental disorder; malingering cognitive impairment would involve pretending to be experiencing memory or other mental impairment. Several assessment instruments have been developed to help in evaluating the likelihood that an individual is malingering either psychiatric symptomatology or cognitive impairment. The Structured Interview of Reported Symptoms (SIRS; Rogers, Bagby, & Dickens, 1992) and the Miller Forensic Assessment of Symptoms Test (M-FAST; Miller, 1995) are two instruments that have been developed for the assessment of malingering of psychiatric impairment, whereas the Test of Memory Malingering (TOMM; Tombaugh, 1996) and the Validity Indicator Profile (VIP; Frederick, 1997) are two that have been developed to evaluate malingering of cognitive impairment. Regardless of whether the evaluation of malingering is formal or informal, the forensic examiner must make some assessment of this issue in every case. The results of this assessment will be useful to the evaluator in determining how much weight to put on the accused’s self-reports and testing results.
3.5 Summary
Psychologists and other mental health professionals assist the criminal courts in understanding issues relevant to psychology and the legal system. The courts call upon psychologists to conduct a wide variety of assessments, both formal (using assessment tools) and informal. By far the most common type of criminal forensic assessment is an assessment of fitness/competency to stand trial, which focuses on the present abilities of the accused. Only about 30 percent of accused who have had their fitness questioned are actually found unfit to proceed.
Another common type of evaluation that psychologists are called upon to conduct is an assessment of an accused’s criminal responsibility or mental state at the time of the offence (insanity). Unlike fitness to stand trial, this type of evaluation focuses on the accused’s mental state at an earlier point in time (the time of the offence); therefore, it is retrospective. Public perceptions of the insanity defence are that it is used often and is frequently successful. In reality, this defence is rarely used and is even more rarely successful.
Psychologists are also called upon to conduct evaluations of an offender’s risk to commit future violence. In this type of assessment, risk factors for violence are identified and evaluated in order to determine the offender’s level of risk and the most appropriate means of reducing or managing future risk.
Each type of evaluation involves an interview with the accused as well as the collection of additional and varied sources of information about the accused. Specialized forensic assessment instruments may also be used to help the evaluator develop an opinion regarding the accused’s fitness to stand trial, criminal responsibility, or future risk for violence.
Discussion Questions
- What are the various types of criminal competencies that may become an issue during the course of an individual’s legal proceedings and what is required of the defendant for each?
- How does fitness to stand trial differ from the issue of criminal responsibility?
- Describe at least two instruments that have been developed for use in evaluations of fitness to stand trial.
- Describe the typical characteristics of an accused who is referred for a fitness evaluation. Describe the typical characteristics of an accused found NCRMD.
- Describe the differences between unstructured clinical judgment, actuarial decision making, and structured professional judgment with respect to risk assessment approaches.
- Describe the difference between risk assessment and risk management.
- Describe the personality traits of someone who is high on the scale for psychopathy. How does this personality type impact their risk for future violence?
- Why is it important to evaluate a defendant for malingering in forensic con- texts? Describe two tools an evaluator might use to assist in this type of assessment.
- Describe the differences between public perceptions of the insanity defence and research findings.
Key Terms
actuarial decision making
adjudicative competency
antisocial personality disorder (APD)
competency to be executed
competency to be sentenced
competency to proceed
competency to waive the right to counsel (proceed pro se)
criminal law
criminal responsibility
fitness (or competency) to stand trial
M’Naghten standard
malingering
not criminally responsible on account of mental disorder (NCRMD)
psychopathy
risk management
structured professional judgment
unstructured clinical judgment
References
American Law Institute. (1962). Model penal code. Washington, DC: Author.
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (4th ed., text rev.). Washington, DC: Author.
Arboleda-Florez, J., Nussbaum, D., Ohayon, M. M., & Roesch, R. (2000). Research on the impact of the 1992 Criminal Code amendments on remands for fitness to stand trial and criminal responsibility. In D. Eaves, J. R. P. Ogloff, and R. Roesch (Eds.), Mental disorders and the Criminal Code: Legal background and contemporary perspectives (pp. 101–160). Burnaby, BC: Mental Health, Law, and Policy Institute.
Bertman, L. J., Thompson, J. W. Jr., Waters, W. F., Estupinan-Kane, L., Martin, J. A., & Russell, L. (2003). Effect of an individualized treatment protocol on restoration of competency in pretrial forensic inpatients. Journal of the American Academy of Psychiatry and Law, 31, 27–35.
Bloom, J. D., & Williams, M. H. (1994). Management and treatment of insanity acquittees: A model for the 1990s. Washington, DC: American Psychiatric Press. Boer, D. P., Hart, S. D., Kropp, P. R., & Webster, C. D. (1997). Manual for the Sexual Violence Risk-20. Vancouver: British Columbia Institute Against Family Violence.
Cirincione, C. (1996). Revisiting the insanity defense: Contested or consensus? Bulletin of the American Academy of Psychiatry and Law, 24, 165–176.
Cirincione, C., Steadman, H. J., & McGreevy, M. A. (1995). Rates of insanity acquittals and the factors associated with successful insanity pleas. Bulletin of the American Academy of Psychiatry and Law, 23, 399–409.
Cleckley, H. M. (1941). The mask of sanity. Oxford, England: Mosby.
Cooper v. R., 1 S.C.R. 1149 (1979).
Crocker, A. G., Favreau, O. E., & Caulet, M. (2002). Gender and fitness to stand trial: A 5-year review of remands in Québec. International Journal of Law and Psychiatry, 25, 67–84.
Douglas, K. S., Hart, S. D., Webster, C. D., & Belfrage, H. (2013). HCR-20 V3 assessing risk for violence. Burnaby, BC: Mental Health, Law, and Policy Institute, Simon Fraser University.
Douglas, K. S., & Webster, C. D. (1999). Predicting violence in mentally and personality disordered individuals. In R. Roesch, S. D. Hart, & J. R. P. Ogloff (Eds.), Psychology and law: The state of the discipline (pp. 175–239). New York: Kluwer Academic/Plenum.
Dusky v. United States, 362 U.S. 402 (1960).
Epperson, D. L., Kaul, J. D., & Hesselton, D. (1998, October). Final report of the development of the Minnesota Sex Offender Screening Tool—Revised (MnSOST-R). Presentation at the 17th Annual Research and Treatment Conference of the Association for the Treatment of Sexual Abusers, Vancouver, British Columbia.
Everington, C. T., & Luckasson, R. (1992). Competence assessment for standing trial for defendants with mental retardation. Ohio: IDS Publishing Corporation.
Forth, A. E., Kosson, D. S., & Hare, R. D. (2003). Hare Psychopathy Checklist: Youth Version (PCL:YV) technical manual. Toronto: Multi-Health Systems.
Frederick, R. I. (1997). Validity Indicator Profile (VIP) manual. Minneapolis, MN: NCS Pearson.
Gibbons, P., Mulryan, N., & O’Connor, A. (1997). Guilty but insane: The insan- ity defense in Ireland, 1850–1995. British Journal of Psychiatry, 170, 467–472. Golding, S. L. (1993). Interdisciplinary Fitness Interview—Revised: A training manual. Salt Lake City: State of Utah Division of Mental Health.
Golding, S. L., Roesch, R., & Schreiber, J. (1984). Assessment and conceptualization of competency to stand trial: Preliminary data on the Interdisciplinary Fitness Interview. Law and Human Behavior, 8, 321–334.
Grisso, T. (1998). Instruments for assessing understanding and appreciation of Miranda rights. Sarasota, FL: Professional Resource Press.
Guy, L. S. (2008). Performance indicators of the structured professional judge- ment approach for assessment risk for violence to others: A meta-analytic survey. (Unpublished doctoral dissertation). Simon Fraser University, Burnaby, BC, Canada.
Hans, V. P. (1986). An analysis of public attitudes toward the insanity defense. Criminology, 4, 393–415.
Hanson, R. K. (1997). The development of a brief actuarial risk scale for sexual offense recidivism. Ottawa: Department of the Solicitor General of Canada.
Hanson, R. K., & Harris, A. (2000). The Sex Offender Need Assessment Rating (SONAR): A method for measuring change in risk levels. User Report 2000– 2001. Ottawa: Department of the Solicitor General of Canada.
Hanson, R. K., & Thornton, D. (1999). Static-99: Improving actuarial risk assess- ments for sex offenders. User Report 1999–2002. Ottawa: Department of the Solicitor General of Canada.
Hare, R. D. (1991). Hare Psychopathy Checklist—Revised (PCL-R). Toronto: Multi- Health Systems.
Hare, R. D. (2003). Hare Psychopathy Checklist—Revised (PCL-R) technical manual
(2nd ed.). Toronto: Multi-Health Systems.
Hart, S. D., Cox, D. N., & Hare, R. D. (1995). Hare Psychopathy Checklist: Screening Version (PCL:SV) technical manual. Toronto: Multi-Health Systems.
Hemphill, J. F., Hare, R. D., & Wong, S. (1998). Psychopathy and recidivism: A review. Legal and Criminological Psychology, 3, 139–170.
Hodgins, S. (1993). Mental health treatment services in Quebec for persons accused or convicted of criminal offenses. International Journal of Law and Psychiatry, 16, 179–194.
Hubbard, K. L., Zapf, P. A., & Ronan, K. A. (2003). Competency restoration: An examination of the differences between defendants predicted restorable and not restorable to competency. Law and Human Behavior, 27, 127–139.
Janofsky, J. S., Dunn, M. H., Roskes, E. J., Briskin, J. K., & Lunstrum, R. M. (1996). Insanity defense pleas in Baltimore City: An analysis of outcome. American Journal of Psychiatry, 153, 1464–1468.
Johnson, W. G., & Mullett, N. (1987). Georgia Court Competency Test—R. In M. Hersen & A. S. Bellack (Eds.), Dictionary of behavioral assessment tech- niques. New York: Pergamon Press.
Kropp, P. R., Hart, S. D., Webster, C. D., & Eaves, D. (1998). Manual for the spousal assault risk assessment guide (3rd ed.). Toronto: Multi-Health Systems.
Laboratory of Community Psychiatry, Harvard Medical School. (1973). Competency to stand trial and mental illness (DHEW Publication No. ADM77–103). Rockville, MD: Department of Health, Education and Welfare.
Latimer, J., & Lawrence, A. (2006). The review board systems in Canada: Overview of results from the mentally disordered accused data collection study. Ottawa: Department of Justice Canada.
Lipsitt, P., Lelos, D., & McGarry, A. L. (1971). Competency for trial: A screen- ing instrument. American Journal of Psychiatry, 128, 105–109.
Livingston, J. D., Wilson, D., Tien, G., & Bond, L. (2003). A follow-up study of persons found not criminally responsible on account of mental disorder in Canada. Canadian Journal of Psychiatry, 48, 408–445.
Lymburner, J. A., & Roesch, R. (1999). The insanity defense: Five years of research (1993–1997). International Journal of Law and Psychiatry, 22, 213–240.
Miller, H. A. (1995). Miller Forensic Assessment of Symptoms Test (M-FAST) profes– sional manual. Odessa, FL: Psychological Assessment Resources.
M’Naghten’s Case, 8 Eng. Rep. 718 (1843).
Nicholson, R. A., & Kugler, K. E. (1991). Competent and incompetent crimi- nal defendants: A quantitative review of comparative research. Psychological Bulletin, 109, 355–370.
Otto, R. K., & Douglas, K. S. (2009). Handbook of violence risk assessment. New York: Routledge.
Pirelli, G., Gottdiener, W. H., & Zapf, P. A. (2011). A meta-analytic review of comparative competency to stand trial research. Psychology, Public Policy, and Law, 17, 1–53.
Poythress, N. G., Monahan, J., Bonnie, R. J., & Hoge, S. K. (1999). MacArthur Competence Assessment Tool—Criminal Adjudication. Odessa, FL: Psychological Assessment Resources.
Quinsey, V. L., Harris, G. T., Rice, M. E., & Cormier, C. A. (2005). Violent offenders: Appraising and managing risk (2nd ed.). Washington, DC: American Psychological Association.
R. v. Abbey, 2 S.C.R. 24 (1982).
R. v. Chaulk, 3 S.C.R. 1303 (1990).
R. v. Demers, 2 S.C.R. 489 (2004).
R. v. M.A.W., 237 C.C.C. (3d) 560 (2008).
R. v. Swain, 1 S.C.R. 933 (1991).
R. v. Taylor, 77 C.C.C. (3d) 551 (1992).
R. v. Trecroce, 55 C.C.C. (2d) 202 (1980).
R. v. Whittle, 2 S.C.R. 914 (1994).
Robey, A. (1965). Criteria for competency to stand trial: A checklist for psychia- trists. American Journal of Psychiatry, 122, 616–623.
Roesch, R., & Golding, S. L. (1980). Competency to stand trial. Urbana: University of Illinois Press.
Roesch, R., Ogloff, J. R. P., Hart, S. D., Dempster, R. J., Zapf, P. A., & Whittemore, K. E. (1997). The impact of Canadian Criminal Code changes on remands and assessments of fitness to stand trial and criminal responsi- bility in British Columbia. Canadian Journal of Psychiatry, 42, 509–514.
Roesch, R., Webster, C. D., & Eaves, D. (1984). The Fitness Interview Test: A method for examining fitness to stand trial. Toronto: Research Report of the Centre of Criminology, University of Toronto.
Roesch, R., Zapf, P. A., & Eaves, D. (2006). Fitness Interview Test—Revised: A structured interview for assessing competency to stand trial. Sarasota, FL: Professional Resource Press.
Rogers, R. (1984). Rogers Criminal Responsibility Assessment Scales (RCRAS) and test manual. Odessa, FL: Psychological Assessment Resources.
Rogers, R., Bagby, R. M., & Dickens, S. E. (1992). Structured Interview of Reports Symptoms (SIRS) and professional manual. Odessa, FL: Psychological Assessment Resources.
Rogers, R., Tillbrook, C. E., & Sewell, K. W. (2004). Evaluation of Competency to Stand Trial—Revised (ECST-R). Lutz, FL: Psychological Assessment Resources.
Salekin, R. T., Rogers, R., & Sewell, K. W. (1996). A review and meta-analysis of the Psychopathy Checklist and Psychopathy Checklist—Revised: Predictive validity of dangerousness. Clinical Psychology: Science and Practice, 3, 203–215. Silver, E., Cirincione, C., & Steadman, H. J. (1994). Demythologizing inaccurate perceptions of the insanity defense. Law and Human Behavior, 18, 63–70.
Tombaugh, T. N. (1996). Test of Memory Malingering (TOMM) manual. Toronto: Multi-Health Systems.
Wack, R. C. (1993). Forensic treatment in the United States: A survey of selected forensic hospitals. Treatment services at the Kirby Forensic Psychiatric Center. International Journal of Law and Psychiatry, 16, 83–104.
Warren, J., Fitch, W. L., Dietz, P., & Rosenfeld, B. (1991). Criminal offense, psychiatric diagnoses and psycho-legal opinion: An analysis of 894 referrals. The Bulletin of the American Academy of Psychiatry and the Law, 19, 63–69.
Webster, C. D., Douglas, K. S., Eaves, D., & Hart, S. D. (1997). HCR-20: Assessing risk for violence (Version 2). Vancouver: Mental Health, Law, and Policy Institute, Simon Fraser University.
Webster, C. D., Harris, G. T., Rice, M. E., Cormier, C. A., & Quinsey, V. L. (1994). The violence prediction scheme: Assessing dangerousness in high risk men. Toronto: University of Toronto, Centre of Criminology.
Wildman, R. W., II, White, P. A., & Brandenburg, C. A. (1990). The Georgia Court Competency Test: The base rate problem. Perceptual and Motor Skills, 70, 1055–1058.
Suggested Readings and Websites
Hart, S. D., & Logan, C. (2011). Formulation of violence risk using evidence-based assessments: The structured professional judgment approach. Chichester, UK: Wiley-Blackwell.
Forensic Psychiatry.ca: www.forensicpsychiatry.ca.
Government of Canada Justice Laws: www.laws-lois.justice.gc.ca.
Litwack, T., Zapf, P. A., Groscup, J. L., & Hart, S. D. (2006). Violence risk assess- ment: Research, legal, and clinical considerations. In I. B. Weiner & A. K. Hess (Eds.), Handbook of forensic psychology (3rd ed., pp. 487–533). New York: Wiley.
Mental Competency Best Practices Model, www.mentalcompetency.org. The Historical Clinical Risk Management-20 Version 3, http://hcr-20.com.
Zapf, P. A., Golding, S. L., & Roesch, R. (2006). Criminal responsibility and the insanity defense. In I. B. Weiner & A. K. Hess (Eds.), Handbook of forensic psychology (3rd ed., pp. 332–363). New York: Wiley.
Zapf, P. A., & Roesch, R. (2006). Competency to stand trial: A guide for evalua- tors. In I. B. Weiner & A. K. Hess (Eds.), Handbook of forensic psychology (3rd ed., pp. 305–331). New York: Wiley.
