Main Body
CHAPTER 4: FORENSIC ASSESSMENT IN CIVIL DOMAINS
Chapter Objectives
- List and describe each of the three main domains of practice in civil forensic psychology.
- Describe civil commitment and the procedures and evaluations used for civil commitment.
- Describe parenting capacity, the issues involved, and how it is evaluated.
- Summarize the issue of child maltreatment and explain how the risk for child maltreatment is assessed by psychologists.
When most people think of law, they think about criminal law—statutes that specify proscribed acts that violate explicit and cherished social norms, procedures for determining when such acts have been committed, and punishments for the acts committed. Yet the vast majority of law is civil law. Civil law governs our lives from before we are born until we die; it even controls our actions after we die.
civil forensic assessment a psychological evaluation intended to assist decision making in matters of civil law
civil law law which is focused on regulating the day-to-day conduct of human affairs and, in particular, attempting to prevent and resolve conflicts between parties
civil forensic assessments are psychological evaluations intended to assist decision making in matters of civil law
The scope of forensic psychological practice with respect to civil law is as broad as the domain of civil law itself. There are too many specific types of civil forensic assessment to enumerate, let alone discuss. Instead, we begin by discussing some of the most common areas of practice in broad terms. We then provide a more detailed discussion of forensic assessment regarding three issues in civil law: civil commitment, parenting capacity, and child maltreatment.
The case of Britney Spears is an excellent illustration of how the civil justice system can be used to help resolve many different difficult situations, ranging from family disputes to concerns over people’s ability to manage their own business affairs or make decisions about health care. It also illustrates how psychologists (and other mental health professionals) can assist the justice system to resolve these disputes. Although the results of Spears’s men- tal health assessment and treatment remain private, there has been considerable speculation that she suffered from mood and substance-related disorders that played a major role in her personal problems. The good news is that there appears to have been a slow but steady improvement in her personal problems since her hospitalization in early 2008. She has regained some visitation rights, and the charges against her in connection with the motor vehicle accident were dismissed. She has even regained her former glory as an entertainer. Her 2008 album, Circus, and the associated concert tour had excellent sales, and her 2011 album, Femme Fatale, yielded several top-ten singles, resulting in many accolades and awards. Hopefully, the worst of Britney’s troubles are behind her.
CASE 4.1. BRITNEY SPEARS
1. Child custody decisions are among the most difficult ones faced by judges. What factors do you think should be considered in a decision about awarding sole or joint custody?
2. What consideration should be given regarding the wishes of the children?
4.1 Civil Forensic Assessment: Major Domains Of Practice
Learning Objective 4.1
List and describe each of the three main domains of practice in civil forensic psychology.
Think of an area of your life—any area—and you will discover that there are laws that govern it. There are also probably one or more forms of civil foren- sic assessment conducted by psychologists that are relevant to it. Let’s take a quick look at some of the questions addressed by psychologists in three major domains of practice in civil forensic psychology: health, children and families, and employment and education.
Health
Civil forensic assessments in the realm of health focus on evaluating the nature and severity of psychological impairment, such as mental disorder, to determine what caused it or whether it has made people unable to reach sound decisions or control their own behaviour. Specific legal issues include:
- Civil commitment. Do people pose a risk for harm on account of mental disorder to the extent that they require involuntary hospitalization or treatment? For example, should a 32-year-old man found by police walking on a bridge late at night be placed in a locked hospital ward against his wishes because he might attempt suicide?
- Competence to consent to treatment. Are people capable of expressing informed, rational, and voluntary preferences concerning their health care? For example, should a 15-year-old girl who has just learned she is pregnant be allowed to make a decision about whether she will have an abortion? A related issue is competence to refuse treatment, as Case Study 4.2 illustrates, later in this chapter.
- Personal injury. To what extent have people suffered emotional, cognitive, or physical harm due to others’ actions? For example, how severe is the neuro- psychological impairment demonstrated by an 8-year-old boy, to what extent can it be attributed to a recent motor vehicle accident, and what are the likely costs of rehabilitating and caring for the boy for the rest of his natural life?
Children and Families
The law governs how marriages and other civil unions are formed and dissolved, as well as what happens to the children of unions. Psychologists conduct civil forensic assessments concerning issues such as:
- Parenting capacity. Are parents capable of providing for a child’s current and future needs, and which childrearing arrangement is best for the child? For example, following the breakup of their marriage, should a mother and father be awarded shared custody of their children, or should custody be awarded to the mother, who plans to move the children to another province where they will have better living conditions?
- Guardianship. Are people capable of caring for themselves and living independently? For example, is a 75-year-old woman in the early stages of dementia able to manage her own finances, or should her 50-year-old son be given the power to make financial decisions on her behalf?
- Risk for maltreatment. Are children at risk for abuse or neglect in the family home and, if so, what should be done to minimize the risk? For example, a 15-year-old brother has inappropriately touched his 5-year-old sister; is the sister at risk for further victimization, or will the parents be able to take reasonable steps to prevent a recurrence?
Employment and Education
People have legal rights to pursue education and employment, even when they suffer from mental disorder. Psychologists are sometimes asked to help determine if such rights have been infringed on appropriately (e.g., in cases where the person poses a risk to safety due to mental disorder) or inappropriately (e.g., if people with mental disorder have been treated in a stereotypical or discriminatory manner). Specifically, psychologists may be asked to conduct assessments regarding
- Fitness for duty/Reasonable accommodation. Are people incapable of performing critical job duties on account of mental disorder, or are there some changes employers could make to their conditions of employment to accommodate mental disorder? For example, a 47-year-old man was placed on temporary leave from his job as a commercial airline pilot when he experienced an episode of depression. Following treatment and apparent resolution of the depression, is he now fit to return to work?
- Discrimination and harassment. Have people suffered discrimination or harassment on the basis of age, gender, or physical or mental disability? For example, is there evidence to support a 54-year-old woman’s claim that she was subjected to sexual harassment at her workplace, and that she suffered serious emotional distress as a result?
- Workplace violence. Are there reasonable grounds to believe that employees pose a risk to the health and safety of co-workers or members of the public? For example, a 28-year-old man got into an argument at work with another employee, during which he threw a stapler and screamed he was going to kill the other man. Does this employee actually pose a risk of harm, and, if so, what can or should the employer do to protect the other employees?
- Disability. Do people suffer from physical or mental disabilities to the extent that they are unable to engage in normal educational and employment activities and may require special assistance? For example, a 24-year-old woman was diagnosed with a schizophrenic disorder at the age of 17 and, despite being compliant with treatment, has not attended school or worked since. Is she capable of supporting herself, at least to a limited extent, or does she qualify for financial support from the government?
This list is by no means extensive or comprehensive; the topics that could be discussed are limitless. For example, specialized risk assessments may be conducted in the context of immigration and refugee hearings or firearms acquisition, or specialized competency evaluations may be carried out in the context of such things as entering into contracts, making a will, or testifying in civil court. But let’s turn now to a more detailed discussion of three issues: civil commitment, parenting capacity, and child maltreatment.
4.2 Civil Commitment
Learning Objective 4.2
Civil commitment is involuntary treatment or hospitalization of individuals on the grounds that they pose a risk to themselves or others on account of mental disorder (Winick, 2008). The issue is, in essence, one of public safety: Governments have a legal responsibility to protect citizens, and this includes the responsibility to protect them from the harmful consequences of physical or mental illness (Gostin, 2005). In a very real sense, then, civil commitment is about containing dangerous illnesses, rather than dangerous people.The responsibility of governments seems clear when it comes to physical illness. Take the example of a disease such as tuberculosis, some forms of which are very contagious and carry a high risk of morbidity and mortality. Various levels of government in Canada have enacted laws and established regulatory and enforcement agencies to help prevent and control the spread of infectious diseases such as tuberculosis. People entering the country may be screened for infectious tuberculosis; physicians may be mandated to report new cases to agencies responsible for surveillance; people diagnosed with the disease may be involuntarily detained (i.e., quarantined), even against their will; and healthy people living or working in certain areas may be required to undergo immunization if they might be or have been in contact with an infected person (Schwartzman & Menzies, 2000). When the illness is mental rather than physical, the underlying logic for civil commitment—to prevent harm to citizens—is the same.Laws that allow involuntary treatment and commitment of people with physical or mental illness clearly infringe on the basic rights and freedoms of citizens. This infringement may be legally justified on two grounds (Melton, Petrila, Poythress, & Slobogin, 2007; Morse, 2004; Schopp, 2001). First, govern- ments have parens patriae powers to act as guardian or caretaker for individuals who are deemed unable to make decisions about their own health and welfare because they are physically or mentally ill. Second, governments have police powers to control people who threaten public order, whether or not they are physically or mentally ill.
police powers powers that give police the authority to control people who threaten public order, whether or not they are physically or mentally ill
criminal commitment incarceration following conviction for a criminal offence
Civil commitment under mental health law does not require that people have any history of harmful behaviour; instead, it will be applied if a person poses an imminent risk of serious harm to self or others due to acute mental disorder. “Imminent” typically means that the harm is likely to occur in the immediate future (i.e., in the coming hours, days, or weeks). Harm that is more distant (e.g., likely to occur months or even years in the future) may be irrelevant. “Serious” typically means that the harm has the potential to result in serious injury or even death. Common examples of serious harm include life-threatening self-injurious or assaultive behaviour; relatively minor or indirect forms of harm (e.g., abusing alcohol, making superficial cuts on one’s own arm, threatening or slapping, dam- aging property) may be insufficient to justify civil commitment. Mental health law in some jurisdictions may permit civil commitment if individuals are at imminent risk for serious health problems because of failure to provide essential care for themselves (e.g., they cannot meet basic hygiene, nutritional, or health care needs).
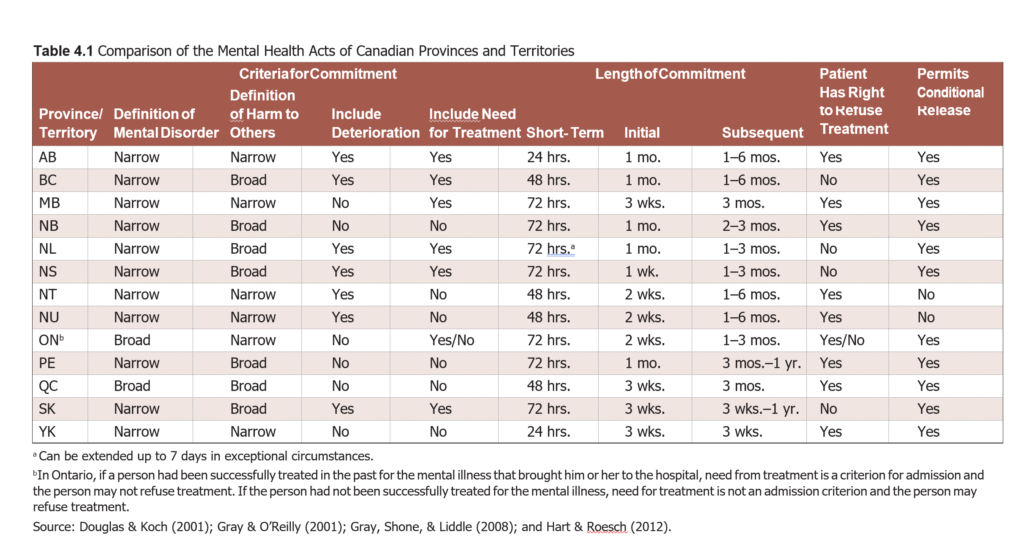
“Acute mental disorder” typically means a serious and often temporary disturbance of thought, affect, or behaviour that impairs people’s ability to make rational decisions or regulate their own actions. Laws may allow commitment only on an inpatient basis, or they may allow either inpatient or outpatient commitment. The time frame for commitment typically is short-term, with a time horizon of days to weeks, although the laws in most jurisdictions allow for extension, if necessary.Whether a person can be involuntarily treated after being involuntarily committed varies across jurisdictions. In some, a person who is involuntarily commit- ted is deemed incompetent to make treatment decisions and will be treated. (This is the case in British Columbia, Saskatchewan, Nova Scotia, and Newfoundland/ Labrador). In others, there is a separate test for competence to make treatment decisions, leading to the possibility that a person who was involuntarily commit- ted will not be treated (e.g., Alberta, Manitoba, Ontario, Quebec, New Brunswick, and Prince Edward Island). Also, in some jurisdictions, a person’s decision not to be treated can be appealed and may be overruled. Treatment that can be ordered is “normal” treatment; it does not include invasive intervention such as electroconvulsive therapy or psychosurgery.
There are no good data concerning civil commitment rates for Canada or, for that matter, most other countries. There are many reasons for this. One is that people’s legal status, as voluntarily or involuntarily committed or treated, is apparently not considered in health care statistic databases. Another reason is that keeping statistics is complicated by the existence of several forms of civil commitment (i.e., traditional, with or without involuntary treatment, ver- sus commitment of violent or sexually violent offenders). Yet another reason is that people’s legal status as voluntarily or involuntarily committed or treated can and does change frequently over time, even during the same course of care in a hospital or in the community, which means there are frequent errors in recording statistics. Estimated rates of civil commitment for a given country in a given year can differ greatly. Trying to compare rates within a given country over time or across countries at a given time is fraught with difficulty.
CASE STUDY 4.2. THE CASE OF PROFESSOR STARSON
The courts reviewed the evidence and found the hospital board had erred in its decision. First, although Professor Starson did not accept his condition was a mental disorder, he recognized that his brain did not function normally. Second, there was no evidence that he failed to appreciate the potential risks and benefits of treatment (or lack thereof). The court decisions in this case, including the final one by the Supreme Court of Canada to uphold those by the lower courts, were praised by some for protecting the rights of those with mental disorders, and condemned by others for permitting mental disorder to ruin the lives of people who suffer from it. But the decisions were not easy for the courts to make. For example, the Supreme Court of Canada decision was split: six justices voted with the majority, but three dissented. One of the dissenters was the Chief Justice, the Right Honorable Beverley McLachlin. She later made a rare public commentary about the challenges posed by this case (McLachlin, 2005):
Professor Starson may well never recover from the illness that afflicts him and may spend the rest of his life in custody or under the significant control of the criminal justice system. Hence the cruel paradox—freedom to refuse “medication” may in fact result in institutional confinement and continued debilitation . . . Our law governing hospitalization and consent continues to grapple with the challenges of appropriately balancing the autonomy and dignity of mentally ill persons with their right to treatment and the important objective of protecting the public from dangerous individuals . . . Laws cannot heal people . . . but the law can create a social and regulatory environment that assists medical professionals in delivering their services in a manner that is both ethical and respectful of the rights and needs of the mentally ill. Professor Starson ’s symptoms persisted without treatment, and the hospital once again went before the Ontario Consent and Capacity Board, which ruled that he was incapable of making decisions about treatment and should be medicated involuntarily. The treatment led to a marked improvement in Professor Starson ’s mental health. As of 2013, he was out of the hospital on a conditional discharge, with the provision that he continue to take anti-psychotic medication.
1. Finding a balance between individual rights and the responsibility of treatment providers to provide appropriate treatment is often difficult, as this case illustrates. Under what, if any, circumstances should an individual be forced to receive treatment?
2. Why do you think the Ontario Consent and Capacity Board decided that Starson should be medicated involuntarily?
Civil Commitment Procedures
As we noted previously, the specific procedures by which people in Canada are civilly committed differ across jurisdictions. These procedures, as set out in the mental health law of each province or territory, are summarized in Table 4.1.
- The person has the right to legal representation through the process.
- The person has the right to regular review of commitment.
- The party seeking civil commitment is responsible for proving the person satisfies the grounds for civil commitment.
- Decisions about civil commitment must respect the least restrictive alternative principle, which holds that the goal of protecting the person or the public must be accomplished in a way that minimizes any infringement on the person’s rights and freedoms.
- The person has the right to appeal the commitment decision.
Despite due process protections, civil commitment is an inherently coercive process. By definition, the person has expressed a preference not to be subjected to the hospitalization or treatment sought by others. Unsurprisingly, coercion works. Involuntary hospitalization and treatment are at least temporarily or moderately effective in containing the risks of harm posed by people who are subject to civil commitment, and may even lead to improvement in symptoms of mental disorder. But, also unsurprisingly, detaining people against their wishes risks interfering with attempts to establish and maintain a supportive and effective treatment relationship. Put simply, civil commitment can save lives, but it can also destroy the involuntarily committed person’s trust in and relationships with health care providers, family members, and others.
A third alternative is to provide better voluntary health care services, so that civil commitment is not necessary. For example, Greenfield, Stoneking, Humphreys, Sundby, and Bond (2008) investigated the effectiveness of a crisis residential program—an unlocked ward managed by mental health consumers (people who have experienced and received treatment for mental disorder). They randomly assigned 393 civilly committed people to either the crisis residential program or a traditional ward, which was locked and managed by health care providers. People were interviewed at admission and then at 30 days, six months, and one year after admission. People admitted to the crisis residential program exhibited significantly greater improvements in psychiatric symptoms, according to both self-report and observer ratings, than did those admitted to the traditional ward. In addition, satisfaction with health care services received was much higher among people admitted to the crisis residential program.
Evaluations for Civil Commitment
Psychologists in some provinces perform evaluations to determine whether people may be civilly committed. Psychology also has made important contributions to the development and evaluation of assessment procedures to assist evaluations for civil commitment. In this section, we take a look at civil commitment evaluations.
To reiterate, in all provinces, people may be civilly committed if they pose a risk to themselves or to others on account of mental disorder. Some provinces allow for civil commitment in other circumstances too, but this criterion is common across provinces. Analyses of this issue by numerous psycholegal scholars (Melton et al., 2007; Morse, 2004; Schopp, 2001) concur that three general requirements must be met. First, the person must currently suffer from a mental disorder. Second, the person must currently pose certain risks. And third, the risks must be due at least in part to the mental disorder, or, put differently, there must exist a discernible causal nexus or causal connection between the mental disorder and the risks. Let’s take a closer look at these requirements and how they are considered as part of civil commitment evaluations.
Mental Disorder
Arguably, this should be the most straightforward part of civil commitment evaluations. In some provinces, the law recognizes that psychologists, by virtue of their education and the training they receive, have special expertise in the assessment and diagnosis of mental disorder (Melton et al., 2007). Psychologists typically evaluate the presence of mental disorder using a clinical interview and review of collateral information, but they can also utilize a wide range of tools. These tools include psychological tests, such as self-report inventories; structured interviews; and ratings scales, as well as standardized diagnostic criteria, such as those in the Diagnostic and Statistical Manual of Mental Disorders (DSM-V) (American Psychiatric Association, 2013), something psychologists had a hand in developing.
The task for evaluators, however, is a bit more complicated than it might appear on the surface. First, the definition of “mental disorder” used in psychology may be very different from that used in mental health law. To assist legal decision making, however, psychologists must use the definition of mental disorder that is set out in statutory or common law. A second complication is that the law is not interested in whether a person ever has suffered from a mental disorder, but rather whether a person currently suffers from a mental disorder. Lifetime diagnoses of mental disorder are generally more reliable than present-state diagnoses. Third, not all forms of mental disorder are assessed and diagnosed with equivalent reliability and validity, and the general level of reliability and validity for many disorders is far from ideal. Finally, not all forms of mental disorder are equally relevant to civil commitment. Evaluators need to pay careful attention to those forms of mental disorder that are established risk factors for harm to self through self-injury or self-neglect, harm to others, and incompetence to make decisions about treatment. For example, psychological research indicates that short-term risk of physical harm to others (i.e., violence) is more strongly associated with certain forms of cognitive, psychotic, and mood disorders than with other forms of mental disorder such as anxiety or adjustment disorders (Friedman, 2006; Sirotich, 2008); in contrast, long- term risk for sexual violence is most strongly associated with paraphilias and personality disorders (Hanson & Morton-Bourgon, 2005). Comorbid (i.e., co-occurring) substance-related disorders further increase risk for both types of violence.
Risk of Harm
Different jurisdictions define the nature and degree of harm that must be posed in different ways. As discussed previously, in all jurisdictions, risk of harm to self or others that is both imminent (i.e., occurring in the coming hours to days) and serious (i.e., life-threatening) will trigger mental health legislation. Some jurisdictions (e.g., Quebec) will only consider civil commitment in circumstances involving imminent and serious harm. Other jurisdictions, such as British Columbia, broaden the definition to include risk that is less serious (i.e., psychological harm, deterioration of physical or mental health).
The COVR and HCR-20 are potentially relevant to traditional civil commit- ment evaluations, whereas the STATIC-99 and SVR-20 are potentially relevant to sexually violent predator evaluations. Research supports the basic reliability and validity of all these tools: different evaluators who evaluate the same person tend to reach similar findings, and people rated as higher risk tend to have significantly higher rates of future violence or sexual violence than do people rated as lower risk (see Hanson & Morton-Bourgon, 2009). But all of them have serious limitations for use in civil commitment evaluations:
-
- The definition of “harm” used for each tool was not intended to match the legal definitions used in various jurisdictions. This means the findings are not necessarily legally relevant. For example, none of these instruments assesses risk for self-injury, suicide, or self-neglect.
- None of the tools is comprehensive. Evaluators must consider whether there are circumstances or risk factors in a given case that should be considered beyond those included in any tool. This means there is always an element of subjectivity or discretion in a risk assessment, even when actuarial instruments are used. For example, the presence of many risk factors may be rendered meaningless by the fact that the person has developed a permanent and disabling medical condition; the presence of few factors may be made more serious by the fact that the person has made clear and credible statements of intent to commit harm.
- It is impossible to estimate the specific probability that a given individual will commit harm in the future using any procedure. Actuarial instruments provide probability estimates that are based on statistical profiles of what happened in groups of other people in the past; they cannot directly calculate what a person will do in the future. Structured professional judgment guidelines do not even attempt to provide probability estimates, as they emphasize that risk of harm depends on future living circumstances.
Causal Nexus
Although civil commitment laws recognize that mental disorder may be associated with risk to self or others, it is not always or even often associated with risk. According to psychological research, the law is correct: most people with mental disorder do not commit serious violence, and the risk for harm to self or others associated with most forms of mental disorder is small (Choe, Teplin, & Abram, 2008). For this reason, it is not permissible under mental health law to civilly commit people solely because they have been diagnosed as suffering from men- tal disorder at some point in their lives. This would be stereotypical and legally discriminatory, infringing on the rights of an entire class of people (i.e., those suffering from certain mental disorders) because of problems with a few. As a consequence, civil commitment requires an individualized assessment, a demonstration that this person currently suffers from a mental disorder that causes this person to pose a risk for harm to self or others.But how does a psychologist determine whether or to what extent any risk of harm is attributable to mental disorder? As yet, no one has developed a tool that attempts to directly evaluate or quantify the causal nexus between mental disorder and risk of harm.
The problem is that a causal nexus does not exist physically, and it cannot be proved or disproved through physical evidence. Rather, a causal nexus is an explanation, interpretation, or account of evidence whose plausibility is judged according to the extent it coheres with the facts of the case, common- sense views of the world, and (where applicable) scientific research and theory. This explanation must be based on something more than the mere co-occurrence of mental disorder and risk of harm to self or others. (In this way, the law avoids discriminating against people with mental disorder.) Evaluators must instead attempt to rule out other plausible explanations, such as chance or the presence of some other factor responsible for the risks.
4.3 Parenting Capacity
Parenting capacity evaluations—also referred to as parenting responsibility and child custody evaluations—are psychological assessments of individuals’ suitability to act as caregivers for children (Ayoub & Kinscherff, 2006; Sparta & Stahl, 2006). They are conducted when individuals’ rights and responsibilities for child rearing are in conflict. On the one hand, parents or guardians have legal rights to raise their children as they see fit, but, on the other hand, they have responsibilities to provide the necessities of life to their children, and to provide an environment that protects the safety and well-being of children.
Learning Objective 4.3
Describe parenting capacity, the issues involved, and how it is evaluated.
Conflict regarding child rearing can take many different forms. One type of conflict arises when parents’ rights conflict with their responsibilities. This can happen when, for example, the religious beliefs of parents proscribe certain kinds of medical treatment that might save their child’s life. In such cases, another interested party, such as a hospital or child protection services agency, may ask courts to override the rights of parents and act as a substitute decision maker concerning treatment of the child. A second type of conflict arises when the rights of one parent conflict with the rights of another parent. This can happen when parents who are not living together cannot agree on who should have primary custody of their children. A third type of conflict is when the rights of parents conflict with the rights of their children. An example would be when children disagree with their parents about some health care decisions or about custody, access, or residence arrangements following divorce or separation. This is especially likely to happen as children grow older and their legal rights increase. A fourth type of conflict is when the rights and responsibilities of parents conflict with those of other interested parties, such as extended family members, police, or child protection agencies. For example, in some jurisdictions grandparents may have limited rights to petition courts for access to their grandchildren, despite the wishes of one or both parents.
Most parenting capacity evaluations are conducted in the context of custody or access disputes, which fall into the second type of conflict, already discussed. The typical scenario involves two parents who are in the process of dissolving their relationship (or have already done so) but disagree about where the children should reside, how much time the children should spend with each parent or other members of their extended families, or how to share responsibility for making decisions about the children’s health care and education. If these disputes cannot be resolved informally, the parties may go before the courts and seek a remedy under civil law.
INSIGHT 4.1. THE WORLDSAFE STUDY
Scope of the Problem
There is no way to determine how often parenting capacity evaluations are conducted in the context of custody or access disputes. To give some insight into the scope of the problem, Statistics Canada (2011) recently summarized information from the Civil Court Survey, based on data from court systems in seven reporting provinces and territories (AB, BC, NT, NS, NU, ON, and YT), representing 66 percent of Canada’s population, in the 2009/2010 fiscal year. According to this report, family law cases represent about 35 percent of all civil court cases.
Taken together, these findings suggest that custody and access disputes may be the single biggest issue in civil law. The picture is, however, not completely bleak. Bear in mind that perhaps 50 percent of all marriages and cohabiting relationships that involve children dissolve without dispute over custody or access. Even in cases that involve disputes, the majority—perhaps 60 to 90 percent—are settled before going to trial (Bow & Quinnell, 2004; Statistics Canada, 2011), sometimes without the need for parenting capacity evaluations. Requests for parenting capacity evaluations are typically triggered by the presence of certain factors, such as allegations that a child was abused or neglected, allegations that a parent has mental health or substance use problems, or an extreme level of conflict between parents (Bow & Quinnell, 2004).
Legal Issues
When there is dissolution of a relationship, the federal Divorce Act applies if the couple was married, and provincial statutes may apply if the couple was living together but not married. If there are children involved, married couples may resolve custody and access disputes through either the Divorce Act or provincial statutes, while couples who were not married must proceed under provincial statutes. In fact, the two statutes are very similar with respect to custody and access. The main difference is in the level of court that can hear the case: provincial superior courts hear cases under the Divorce Act, and provincial courts hear cases under provincial statutes.
“tender years” doctrine the perspective that mothers should be granted custody due to their special abilities when it came to rearing young children
best interests of the child principle the perspective that legal decisions should provide children with childrearing environments that are most likely to ensure optimal development in light of their unique needs and circumstances
Although most divorces are settled amicably, there are a small number of cases in which there is high conflict between the parents. These cases may involve anger and distrust between parents, domestic violence, or alienation of the child resulting from the conduct or attitudes of one or both parents (Birnbaum & Bala, 2010; Jaffe, Crooks, & Bala, 2009). Once a custody and access dispute arises, how do Canadian courts decide the issue? In Young v. Young (1993) the Supreme Court of Canada summarized the history of custody and access law. Up until the mid-1800s, the decision was simple because children were viewed as the property of fathers, possibly a legacy of the lingering influence in British common law of the ancient Roman doctrine of paterfamilias. From the mid-1800s until the mid-1900s, this legal tradition was replaced by the “tender years” doctrine, which assumed mothers should be granted custody due to their special abilities when it came to rearing young children. But in the early to mid-1900s, the legal doctrine that emerged and eventually become dominant was the best interests of the child principle, which is now reflected in the laws of every jurisdiction in Canada and is to be the only consideration in resolving custody disputes. According to this principle, legal decisions should try to provide children with childrearing environments that are most likely to ensure optimal development in light of their unique needs and circumstances (Melton et al., 2007), and especially their psychological needs (Emery et al., 2005). To understand the elements that are considered when determining what is in the child’s best interest, Paetsch, Bertrand, and Hornick (2001) administered a survey to all participants at a Family Mediation Canada conference in Hull, Quebec, in 2000. There were 157 responses from lawyers, social workers, psychologists, educators, assessors, and judges. The vast majority of respondents practised family mediation. A list of the factors taken into consideration when mediating custody disputes is in Table 4.2, and this shows that the need to maintain a strong and stable relation- ship with both parents was ranked high by the vast majority of respondents. This is also reflected in court cases and has led some legal scholars to find that the new legal presumption is joint custody; the children live with each parent about half the time (Kurki-Suonio, 2000; Rhoades, 2002).
Evaluators need to determine what a child needs to grow and thrive, and whether or how the parents, working jointly or individually, can meet these needs of the child. An extensive list of specific areas addressed in parenting capacity evaluations is presented in Table 4.3.
| Table 4.2 Family Mediator Ratings of the Importance of Each “Best Interest of the Child” Criterion | |
|
Criterion |
Percent who rated criterion as “Very Important” |
| The potential for physical or psychological harm to the child | 96% |
| A strong and stable relationship with both parents | 91% |
| Emotional growth, health, stability, and physical care of the child | 80% |
| Guidance, education, basic needs, and other special needs of the child | 74% |
| Freedom from exposure to parental conflict | 73% |
| Each parent supporting a close relationship between the child and the other parent | 71% |
| Quality of the relationship the child has with the parent(s) | 58% |
| Willingness of parents to work together on important issues concerning the child | 56% |
| Characteristics and needs of the child | 54% |
| Ability to maintain relations with other members of the family | 53% |
| The sex of the parent should have no effect on the outcome | 51% |
| Whether the child can adjust to the parenting arrangement | 40% |
| Cultural, ethnic, and religious background of the child | 28% |
| Wishes of the child | 27% |
| The roles that each parent had prior to the breakup | 22% |
| Source: Paetsch, Bertrand, & Hornick (2001). | |
The Practice of Parenting Capacity Evaluations
The “best interests of the child” principle may sound both simple and sensible, but custody and access evaluators have found it difficult to observe in practice. The very things that make the principle attractive—for example, its respect for the diversity and uniqueness of children’s needs—also make it difficult to conduct evaluations in a systematic, consistent manner (Emery et al., 2005).
Table 4.3 Some Specific Areas Addressed in Parenting Capacity Evaluations
| Parent | Child | Parent-Child Relationship |
| Personality | Personality | Contact and interaction |
| Intellectual functioning | Intellectual functioning | Attachment |
| Childrearing experiences (including maltreatment) | Childrearing experiences (including maltreatment) | Nurturance and support |
| Relationships with intimate partners | Relationships with siblings | Supervision and discipline |
| Relationships with other family members | Relationships with other family members | Maltreatment |
| Parenting skills and attitudes | Peer relationships | |
| Relationships with peers and others | Educational functioning | |
| Educational functioning | Physical health | |
| Occupational functioning | Mental health | |
| Physical health | Substance use | |
| Mental health | Antisocial behaviour | |
| Substance use | Other special problems/needs | |
| Antisocial behaviour | ||
| Source: Ayoub & Kinscherff (2006) and Sparta & Stahl (2006). | ||
Historically, despite the frequent participation of psychologists and other mental health experts in custody and access matters, courts were often dissatisfied with the resulting reports and testimony (Bow & Quinnell, 2004; Melton et al., 2007). A major problem identified with parenting capacity evaluations was the tendency for evaluators to work with and advocate for one of the parents, rather than taking a neutral and objective stance. Second, evaluators had a tendency to use traditional procedures to assess the mental health of individual parents and children, rather than using specialized procedures to assess the children’s needs and the parents’ capacity to meet those needs. Third, evaluators did not make specific comments on, or recommendations that would help courts to make decisions regarding custody and access arrangements. And it wasn’t only courts that were unhappy with parenting capacity evaluations—parents were unhappy too, leading to frequent complaints to professional licensing or registration bodies. To help improve parenting capacity evaluations, in February 1994 the Council of Representatives of the American Psychological Association (APA) adopted practice guidelines drafted by the APA’s Committee on Professional Practice and Standards, with input from its Committee on Children, Youth, and Families. The Guidelines for Child Custody Evaluations in Divorce Proceedings were published later that same year (American Psychological Association, 1994). These guidelines, subsequently updated and renamed Guidelines for Child Custody Evaluations in Family Law Proceedings (American Psychological Association, 2010), are summarized as follows:
- Orienting Guidelines: Purpose of the Child Custody Evaluation:
- The purpose of the evaluation is to assist in determining the psychological best interests of the child.
- The child’s welfare is paramount.
- The evaluation focuses upon parenting attributes, the child’s psychological needs, and the resulting fit.
- General Guidelines: Preparing for the Child Custody Evaluation
- Psychologists strive to gain and maintain specialized competence.
- Psychologists strive to function as impartial evaluators.
- Psychologists strive to engage n culturally informed, nondiscriminatory evaluation practices.
- Psychologists strive to avoid conflicts of interest and multiple relationships in conducting evaluations.
- Procedural Guidelines: Conducting the Child Custody Evaluation
- Psychologists strive to establish the scope of the evaluation in a timely fashion, consistent with the nature of the referral question.
- Psychologists strive to obtain appropriately informed consent.
- Psychologists strive to employ multiple methods of data gathering.
- Psychologists strive to interpret assessment data in a manner consistent with the context of the evaluation.
- Psychologists strive to complement the evaluation with the appropriate combination of examinations.
- Psychologists strive to base their recommendations, if any, upon the psychological best interests of the child.
It appears that the efforts made by psychologists to improve parenting capacity evaluations in custody and access matters have had a substantial impact on practice. Evidence of this comes from surveys of evaluators undertaken before and after the publication of the APA’s first set of guidelines in 1994. First, the “before” picture: Keilin and Bloom (1986) analyzed the responses of 82 custody and access evaluators (78 percent of whom were psychologists) to a questionnaire that asked respondents to, anonymously, list the evaluation procedures they used and rank the specific factors they considered in terms of importance. Respondents indicated that they conducted evaluations as court-appointed experts only about 26 percent of the time. They spent an average of about 19 hours working on each evaluation. The most common assessment procedure used was interviewing. Evaluators reported that they conducted interviews of parents in 100 percent of cases, and interviews of children in 99 percent of cases (remember that some children are developmentally incapable of being interviewed). Evaluators administered psychological tests to parents in 76 percent of cases and to children in 74 percent of cases. Most were standard tests of intelligence or personality, and none were tests developed specifically for use in parenting capacity evaluations. Other assessment procedures included behavioural observations, interviews with collateral informants, and home and school visits. After completing the assessments, the evaluators typically spent about 2.8 hours writing the report, 1.4 hours consulting with attorneys, and about 2.3 hours testifying in court.
Now let’s turn to the “after” picture. Since the publication of the APA’s first set of guidelines, there have been several surveys that used methods similar to those of Keilin and Bloom (1986), including Ackerman and Ackerman (1997), Bow and Quinnell (2001), and LaFortune and Carpenter (1998). Some general conclusions can be drawn from the recent surveys about changes in the practice of parenting capacity evaluations:
-
- Evaluators more frequently act in the role of neutral, court-appointed evaluators.
- Evaluations are taking more time. The average number of hours spent on each case has increased by 10 to 20 percent, to about 21 to 24 hours.
- There have been changes in the assessment procedures used by evaluators. They still spend considerable time administering psychological tests, but they now commonly use tests that were designed specifically for use in, or are directly relevant to, parenting capacity evaluations. (Some examples of such tests are presented in Table 4.5.) Also, evaluators spend more time reviewing documentary evidence.
- Evaluators increasingly evaluate or make specific recommendations regarding custody and access arrangements in light of a child’s needs. (Not surprisingly, the time devoted to writing reports also has increased.)
Despite some apparent improvements, there are still reasons to be concerned. One problem is that many parenting capacity evaluations do not pay enough attention to the legal context in which they are conducted. Evaluators too often ignore the need for their assessments to address specific legal criteria, set out clear opinions regarding issues relevant to the case at hand, and be structured in specific ways. For example, Bow and Quinnell (2004) surveyed 121 judges and attorneys in Michigan who specialized in family law issues. On the positive side, respondents rated the parenting capacity evaluation reports they reviewed as being generally quite useful, and they gave high marks to those components of the reports related to evaluators’ discussions of psychological testing results and the psychosocial histories of parents and children. But they gave low marks to evaluators’ recommendations concerning visitation and other issues, comparison of parents with respect to relevant legal criteria, and identification of information that formed the basis for their findings and opinions.
A second problem is that there is little scientific support for the reliability and validity of psychological tests commonly used in parenting capacity evaluations. As Emery and colleagues (2005) pointed out, some of these tests (e.g., projective tests) are not generally accepted as reliable and valid in any area of psychological practice; other tests (e.g., intelligence tests) are generally accepted as reliable and valid in other areas of psychological practice, but their relevance to parenting capacity evaluations is often unclear; and still other tests appear on the surface to be directly relevant to parenting capacity, but either their psychometric properties are unknown or the constructs they measure (e.g., parent alienation syndrome) are themselves unvalidated.
| Table 4.5 Examples of Specialized Psychological Tests Developed for Use in Parenting Capacity Evaluations |
|
| Test | Description |
| Ackerman-Schoendorf Parent Evaluation of Custody Test (ASPECT; Ackerman & Schoendorf, 1992) | A multi-item rating scale designed to index overall parenting capacity. Ratings are made by evaluators on the basis of interview, observation, and psychological testing of parents. Items were selected rationally. Item ratings are combined to yield an overall Parental Custody Index for each parent. |
| Bricklin Perceptual Scales (BPS; Bricklin, 1984) | A multi-item rating scale designed to tap children’s perceptions of their parents. Children respond to a series of questions related to parental competency, supportiveness, consistency, and character. Items were selected rationally. Item ratings are combined to yield three scores that compare perceptions of each parent. |
| Custody Quotient (CQ; Gordon & Peek, 1988) | A multi-item rating scale designed to index specific aspects of parent- ing capacity. Ratings are made by evaluators on the basis of interview, observation, and review of case history information. Items were selected rationally. Item ratings are combined to yield an overall Custody Quotient for each parent, as well as scores on 12 subscales. |
| Uniform Child Custody Evaluation System (UCCES; Munsinger & Karlson, 1994) | A systematic procedure for conducting parenting capacity evaluations. Materials include 25 forms to assist gathering, transcribing, and organizing essential information and assessing response validity. Procedures devel- oped rationally (to reflect legal and clinical considerations). Does not yield quantitative scores. |
A third problem is that decisions about parenting capacity are value laden. Which of a child’s needs are most important? How are they best met? To what extent should the wishes of the child and parents be respected? Answering these questions requires evaluators to exercise judgment. To the extent that evaluators understand and use the values inherent in relevant legal criteria, this is accept- able; but it is unacceptable if evaluators fail to make their values explicit, reject the values reflected in law, or introduce their own personal values in the process. A major challenge facing this area of civil forensic assessment is the development of assessment procedures or decision aids to help evaluators exercise their judgment in a way that will facilitate sound, legal decision making.
4.4 Child Maltreatment
Child maltreatment is the abuse or neglect of children by parents or other people in a position of power, trust, or responsibility. Child abuse is the commission of acts that deliberately or recklessly threaten the safety and well- being of children. Abusive acts often are divided into three categories depending on the nature of the acts and their (potential) consequences (Krug, Dahlberg, Mercy, Zwi, & Lozano, 2002). Physical abuse involves actual, attempted, or threatened injury of a child—basically, causing bodily harm or fear of bodily harm. Sexual abuse involves actual, attempted, or threatened sexual contact that is inappropriate due to the perpetrator’s age or relationship to a child. Contact includes physical contact (e.g., touching, assault) and communication, whether coercive or non-coercive. Emotional abuse involves actual, attempted, or threat- ened psychological or social harm of a child. It includes cruelty and exploitation. Cruelty is the intentional infliction of severe psychological distress (e.g., anxi- ety, fear, embarrassment). Exploitation is the use of children for commercial or sexual purposes (e.g., forced labour, military service, or prostitution) in a way that may impair their psychological or social development. In contrast, child neglect is the omission of necessary acts by a person who has a duty to care for the child, with the result that the safety and well-being of the child is deliberately or recklessly threatened (Krug et al., 2002). Neglect may involve failing to provide a child with the necessities of life, such as food, clothing, or medical care, or failing to provide a safe and secure physical environment for rearing a child.
Learning Objective 4.4
Summarize the issue of child maltreatment and explain how the risk for child maltreatment is assessed by psychologists.
child maltreatment the abuse or neglect of children by parents or other people in a position of power, trust, or responsibility
child abuse the commission of acts that deliberately or recklessly threaten the safety and well-being of children
child neglect the omission of acts, deliberately or recklessly threatening the safety and well-being of children
Although the definition of child maltreatment appears to be relatively straightforward, it is influenced heavily by cultural considerations. Culture may be defined as the sum of work and thought expressed or produced by members of a particular group or in a particular place, including their social practices, beliefs, institutions, and arts (Cross & Markus, 1999; Rogler, 1999). Although culture is a reflection of people and the collective physical and social environments in which they live, it also exerts a profound influence on those same individuals, helping them to define what is normal in terms of attitudes, emotions, and behaviour, including childrearing behaviour. In general, acts or omissions are considered child maltreatment when they are culturally abnormal or deviant, something that may be referred to as a “violation of community standards.” The impact of culture means that it is sometimes difficult to distinguish between harsh discipline and child maltreatment (Krug et al., 2002).
To illustrate the impact of culture on the definition of child maltreatment, consider the issue of physical or corporal punishment of children. Historically, it was acceptable in many European and North American cultures for caregivers— parents and other adults, including teachers—to discipline children by striking them with hands or even objects (e.g., wooden spoons, belts, rulers, or straps). But attitudes toward discipline with physical punishment have changed markedly. It is now unacceptable in some of these same cultures to strike children. For example, in Canada, the Supreme Court in Canadian Foundation for Children, Youth and the Law v. Canada (Attorney General) (2004) ruled that parents may use mild physical punishment, such as spanking, but its use is severely restricted: only for corrective and educational purposes; never with children under the age of 2; not with teenagers, as it may lead to aggressive or antisocial behaviour; not with children who are incapable of learning from punishment due to physical or mental disability; never in a way that causes harm or fear of harm (e.g., not with objects such as rulers or belts; not slaps or blows to the head); and not in a way that is psychologically cruel or demeaning. In the same ruling, the Court also held that corporal punishment is forbidden in schools. Laws in other countries, such as the United Kingdom and the United States, are somewhat more permissive. For example, at least 1,700 police departments in the United States have issued conducted electricity weapons, or Tasers®, to officers patrolling public schools. These weapons are used regularly not just to apprehend children who are breaking the law, but to control children, including some as young as 6 years old, who are simply breaking school rules by being unruly, disruptive, or truant. (See Insight 4.1 for further discussion of cross-cultural differences in childrearing practices.)
Scope of the Problem
Regardless of any definitional issues, child maltreatment is clearly a major pub- lic health concern due to its potentially serious consequences and high prevalence (Krug et al., 2002). The potential consequences of child maltreatment vary among individuals, depending on the severity and chronicity of maltreatment, as well as the age of the child, the child’s relationship to the abuser, the response to the child’s disclosure of maltreatment, the socioeconomic status of the family, and the social and community support available to the family. The effects include physical injuries ranging from minor bruises and welts to broken bones, severe neurological impairment, or death, and psychological injuries range from impaired cognition and academic achievement to mental disorder and increased risk of externalizing behaviour such as substance abuse, teenage pregnancy, running away, and criminality. These effects may persist into adulthood, leading to long-term need for and utilization of medical, mental health, social, and legal services (Krug et al., 2002).
Estimating the prevalence of child maltreatment is difficult due not only to definitional problems, as discussed previously, but also to the general problem that most incidents of child abuse and neglect, like other criminal behaviours, are not reported to police or other agencies. Looking first at official statistics, the third National Incidence Study of Child Abuse and Neglect (NIS-3) reported that more than 2.8 million children were victims of maltreatment in 1993 (Sedlak & Broadhurst, 1996). The most recent analysis of the National Child Abuse and Neglect Data System, reported by the U.S. Department of Health and Human Services (2008), estimated that there were about 3.6 million reports and about 905,000 substantiated cases of child maltreatment in the 2006 fiscal year. This represents a reporting rate of about 47.8 per 1,000 children per year, and a victimization rate of about 12.1 per 1,000 children. With respect to the type of maltreatment experienced, about 64 percent of victims experienced neglect, 16 percent experienced physical abuse, 9 percent experienced sexual abuse, and 7 percent experienced psychological abuse. In addition, 15 percent were recorded as having experienced “other” types of maltreatment. (These figures total more than 100 percent because some children were victims of more than one type of maltreatment.) In 90 percent of cases, the perpetrators of the abuse or neglect were the children’s parents. More than 1,500 children died as a result of maltreatment. Turning next to community surveys, Straus, Sugarman, and Giles-Sims (1997) examined child maltreatment in a nationwide study in the United States. They estimated the victimization rate for physical abuse at 49 per 1,000 children per year—more than 10 times higher than the rate estimated from official statistics. Other social surveys have yielded similar findings regarding the underestimate of child maltreatment, based on official statistics (e.g., Gallup, 1995). Although this number seems very large, it is only the tip of the iceberg, as annual incidence rates underestimate lifetime risk of child maltreat- ment. Hussey, Chang, and Kotch (2006) surveyed a nationally representative probability sample of 10,828 high school students and asked them about child maltreatment victimization experiences perpetrated by parents or other adult caregivers prior to the sixth grade. About 42 percent of adolescents said they had been negligently supervised on at least one occasion, and about 12 percent said their basic physical needs had been neglected on at least one occasion. In terms of child abuse, about 28 percent of adolescents said they had been physically assaulted on at least one occasion, and about 5 percent said they had been sexually assaulted on at least one occasion.
One reason why it is so difficult to determine the rate of child maltreat- ment precisely is that the rate changes over time. For example, according to Jones, Finkelhor, and Halter (2006), the rate of substantiated cases increased in the 1980s and early 1990s, peaking in about 1992. Since then, there has been a marked decline in the rates of physical and sexual abuse, down about 36 percent and 47 percent, respectively, between 1992 and 2003, and a small decline in the rate of neglect, down only about 7 percent during the same period. The reasons for the fluctuation are not entirely clear. It is likely that the rise through 1993 was more apparent than real, a reflection of more reports of maltreatment, rather than more incidents. The increased reporting may have been stimulated by changes in public attitudes toward maltreatment resulting from public education campaigns. But assuming that public attitudes have not grown more tolerant of child maltreatment since 1993, the drop in rates probably reflects a true decrease in maltreatment. A true decrease could be due to various factors, including positive changes in prevention and response at the community level (Jones et al., 2006).
The negative consequences and high prevalence of child maltreatment combine to create staggering economic consequences. In Canada, McKenna, Bowlus, Day, and Wright (2003) estimated the total direct and indirect costs associated with the 135,500 child maltreatment cases investigated in 1998 to be more than $15 billion. In the United States, one study estimated the direct and indirect costs stemming from just one year of confirmed child maltreatment cases to be $124 billion (Fang, Brown, Florence, & Mercy, 2012).
The Role of Psychology in Child Protection
Governments have a mandate to protect children from harm not only by responding decisively to child maltreatment, but also by preventing it. This mandate is enshrined in legislation throughout the United States.
Perhaps the strongest support for governments’ mandate to protect children from maltreatment comes from the United Nations Convention on the Rights of the Child (UNCRC; United Nations, 1989). The UNCRC is a statement of the civil, political, economic, social, and cultural rights of children. It follows in the footsteps of previous international agreements, including the World Child Welfare Charter, endorsed by the General Assembly of the League of Nations (the forerunner to the United Nations) in 1924, and the Declaration of the Rights of the Child, adopted by the General Assembly of the United Nations in 1959. According to Article 19 of the UNCRC:
- Parties shall take all appropriate legislative, administrative, social and educational measures to protect the child from all forms of physical or men- tal violence, injury or abuse, neglect or negligent treatment, maltreatment or exploitation, including sexual abuse, while in the care of parent(s), legal guardian(s) or any other person who has the care of the child.
- Such protective measures should, as appropriate, include effective procedures for the establishment of social programmes to provide necessary sup- port for the child and for those who have the care of the child, as well as for other forms of prevention and for identification, reporting, referral, investigation, treatment and follow-up of instances of child maltreatment described heretofore, and, as appropriate, for judicial involvement.
Articles 32 to 36 prohibit other forms of maltreatment, including exploitation, and Article 39 sets out the responsibility for governments to provide appropriate services to promote physical and psychological recovery and social reintegration of victims of child maltreatment.
The UNCRC was adopted by the General Assembly of the United Nations in 1989. It is a legally binding instrument: member nations that ratify the UNCRC are bound to it by international law, and compliance is monitored by the United Nations Committee on the Rights of the Child. As of 2009, 193 countries, including Canada, have ratified the UNCRC.
In 2001, the American Psychological Association’s Council of Representatives approved a strongly worded resolution that declared the development of a national strategy for the protection of children to be “a matter of the highest urgency,” affirmed its intent to adopt both the spirit and the principles of the convention in the APA’s own activities, and urged all levels of government in the United States to do the same (American Psychological Association, 2001). Based on the APA resolution, one can identify several ways in which the practice of psychology is relevant to the issue of child protection. First, psychologists have a general ethical duty to promote the adjustment of children (and other people) and protect them from harm, as well as a legal mandate to report suspected child mal- treatment to the proper authorities. Second, psychological theory and research can further our understanding of children’s well-being and sense of dignity, both their nature and the conditions necessary for their development, a central focus of the UNCRC. Third, psychology can assist the development and evaluation of such services designed to prevent and respond to child maltreatment. Fourth, psychological research can assist in the development and evaluation of more general public policy concerning child maltreatment.
Assessing Risk for Child Maltreatment
One area in which psychologists contribute to child protection is in the assess- ment of risk for child maltreatment. Once a report of maltreatment is made to police or child protection services, it must be investigated to determine whether it can be substantiated and whether there is any risk for future maltreatment. Prevention of maltreatment requires courts, tribunals, or other decision makers to reach an opinion—based on the findings of a risk assessment—regarding what has happened in the past, which types of harm the child faces and in which kinds of situations, and what interventions should be implemented to ensure the health and safety of the child. The plans for intervention need to specify which services should be delivered and at what level of intensity or intrusiveness. A child who is at lower risk for maltreatment (i.e., a case in which the risk of serious abuse or neglect seems remote or unlikely) may be protected with interventions such as childrearing skills and anger management training for parents, financial aid or employment counselling for parents, assistance with housing needs for the family, regular home visits by child protection service workers to support the parents and monitor the child’s adjustment, or counselling health care for the child. This is what happens in the vast majority of cases. In a relatively small proportion of cases, the findings of the risk assessment may suggest that the child is at high risk for abuse or neglect, and the evaluator may recommend extreme protective measures, up to and including apprehension of the child. Apprehension may result in temporary or even permanent suspension of parental rights and placement of the child in alternative residential care (e.g., under the supervision of other family members or guardians, or in a foster home).
A child maltreatment risk assessment is similar to a parenting capacity evaluation in some important respects. One critical aspect of a risk assessment is to determine the unique needs of the child and whether the parents are able, either on their own or with assistance, to meet those needs. But a risk assessment also needs to consider factors that are associated, according to theory and research, with perpetration of child abuse and neglect. There is general consensus in the field that the risk assessment process should be structured to ensure critical risk factors and potential targets for intervention are considered systematically across cases (English & Pecora, 1994). The American Psychological Association (2013) published updated guidelines for conducting evaluations concerning child protection, similar to those it developed for conducting custody and access evaluations. These guidelines are summarized below.
- Orienting Guidelines
- The primary purpose of the evaluation is to provide relevant, professionally sound results or opinions in matters where a child’s health and welfare may have been and/or may be harmed.
- When psychologists conduct evaluations in child protection matters to address specific referral questions, they are aware that the interests of the parties in the case may differ from one another.
- When the referral question in the evaluation addresses concerns about the parent/ caretaker and child relationship, psychologists are mindful of: the parent/caretaker’s parenting capacities, including circumstances or factors relevant to maltreatment of the child; the child’s well-being and psychological needs; and the resulting fit.
- General Guidelines:
- The role of psychologists who conduct child protection evaluations is that of a professional expert who strives to maintain an unbiased, impartial approach to
the evaluation. - Psychologists strive to gain competence sufficient to provide effective and ethical forensic services when conducting child protection evaluations and when addressing case-specific issues that may require specialized professional knowledge, training, or skills.
- Psychologists strive to be aware of personal biases and societal prejudices and seek to engage in nondiscriminatory practice.
- Psychologists providing child protection evaluations strive to avoid role conflicts and multiple relationships that may compromise their objectivity, competence, or effectiveness, or that may otherwise risk harm or exploitation to the person or identified client (e.g., court, state child protection agency) with whom the professional relationship exists.
- The role of psychologists who conduct child protection evaluations is that of a professional expert who strives to maintain an unbiased, impartial approach to
- Procedural guidelines:
- Based on the nature of referral issues or questions that define the focus and scope of the evaluation, psychologists determine the methods that are appropriate to address the referral issues or question.
- In accordance with the APA Ethics Code, psychologists performing psychological evaluations in child protection matters obtain appropriate informed consent or assent from all adult participants, and as appropriate, inform the child participant.
- Psychologists use multiple methods of data gathering.
- Psychologists seek to properly interpret clinical or assessment data that inform or support their conclusions.
- Psychologists conducting a psychological evaluation in child protection matters strive to provide opinions only when they have obtained sufficient data to support those opinions.
- Recommendations, if offered, address the evaluation’s specific referral questions, which may encompass various concerns related to the child’s welfare and health in a child protection matter.
- Psychologists create and maintain records in accordance with ethical and legal standards.
Source: American Psychological Association. (2013). Guidelines for psychological evaluations in child protection matters. American Psychologist, 68, 20–21. Reprinted with permission.
Despite consensus about the need for structure, there is considerable controversy concerning the adequacy of risk assessment instruments. There has been a proliferation of instruments used by agencies in various jurisdictions, yet none of the instruments is generally accepted or well validated. Some instruments were developed and implemented without adequate research; others are simply modifications of existing instruments, made without a solid theoretical or research basis; and still others are used for purposes or with groups for which they were not intended and have not been validated (e.g., Stowman & Donohue, 2004).
An example of a structured approach to child maltreatment risk assessment is the Child Abuse Potential or CAP Inventory (Milner, 2006). The CAP Inventory is a 160-item self-report questionnaire designed to screen parents for risk of child abuse. It is used commonly in parenting capacity evaluations, in both custody and access and child protection contexts. The items in the CAP Inventory were selected on rational or empirical grounds: rational if they reflected potential causal risk factors for child abuse according to theory and research, empirical if they discriminated between known groups of abusive and non-abusive parents. Parents complete the CAP Inventory by responding “agree” or “disagree” to a series of statements. Item ratings are combined to yield scores on 12 scales. One scale reflects risk for physical abuse. Eight scales reflect parent and family characteristics (distress, rigidity, unhappiness, problems with child and self, problems with family, problems with others, ego strength, and loneliness). Three scales reflect response distortion (lying, inconsistent responding, and random responding).
Research on the CAP Inventory has focused primarily on the physical abuse scale (Milner, 2008). In general, this scale appears to have adequate internal consistency and short-term test-retest reliabilities. Predictive validity research is difficult to conduct, because intervention is expected to attenuate the association between risk and subsequent maltreatment. (In other words, we hope our interventions reduce risk.) There have been a few prospective studies in which the CAP Inventory physical abuse scale (or an abbreviated version of it) was administered to parents and correlated with subsequent physical health and psychological adjustment problems, some of which may have been due to child maltreatment. Other forms of validity research are much easier to conduct. Numerous studies have found that parents’ scores on the physical abuse scale of the CAP Inventory are associated with a wide range of child and family problems.
But the CAP Inventory also has some important limitations. First, it focuses on general physical abuse. It is questionable whether it is relevant to sexual abuse, emotional abuse, and neglect, let alone more specific forms of maltreatment (e.g., exposing a child to dangerous chemicals by operating a drug lab in the family home). Second, there has been no research examining potential bias (i.e., lack of structural or metric equivalence) in the CAP Inventory scores across group factors such as gender, age, and ethnicity. It is uncertain, for example, if the CAP Inventory is equally useful for mothers versus fathers, younger versus older parents, or cultural majority versus minority families. Third, even focusing on the primary use of the CAP Inventory, there is no research that clearly demonstrates its ability to predict future physical abuse of children. For these reasons, psychologists (as well as others working in the field of child maltreatment) continue to develop and evaluate risk assessment instruments.
Summary
Civil forensic assessment is actually a much broader and more diverse area of psychological practice than criminal forensic assessment, because civil law regulates virtually every aspect of daily life. Psychologists conduct evaluations of such matters as families, work, and health care. We focused in this chapter on three specific issues: civil commitment, parenting capacity, and child maltreatment. Although the legal questions that psychologists must try to answer in these areas are very different, a common theme is evident: a variety of assessment procedures have been developed in an effort to make sure psychological evaluations gather information that is scientifically reliable and legally relevant. As our modern societies become increasingly complex and litigious, no doubt the call for civil forensic assessment will continue to grow.
Discussion Questions
- Consider the possibility that you might develop a physical illness or mental dis- order that impairs your ability to make decisions about your health care. Do advanced treatment directives seem like a good idea to you? Why or why not?
- To demonstrate just how central values are to making decision in parenting capacity evaluations, answer the following questions posed by Beaber (1982, p. 319):
Should brothers and sisters be in the custody of the same parent?
-
- Should an older child, over age 12, have veto power in a custody dispute between two parents?
- Should boys be placed with fathers and daughters with mothers?
- Should young children, under age 5, be placed with mothers?
Should continuity of residence and school district control placement?
-
- Should children be placed with the parent who does not work outside the home or who works the fewest hours and/or the most convenient hours?
- Should children be placed in the home that does not have/will not have a step-parent?
- Many child protection services view exposing children to domestic violence—that is, physical violence between parents—as a form of child maltreatment. Does this seem fair to you? What about a scenario in which children are removed from the family home because a woman was repeatedly assaulted by her partner; is this child protection or victim blaming? Should exposing children to the use, manufacture, or distribution of illicit drugs also be considered a form of maltreatment?
- List and describe different forms of child abuse and harm.
- Describe the purpose, strengths, and limitations of the CAP Inventory in the context of child maltreatment risk assessment.
- List and describe more recently developed alternatives to traditional custodial civil commitment?
- What are the due process protections afforded people subject to civil commitment proceedings? Why are these important?
- What sorts of challenges might psychologists be faced with in diagnosing mental disorder in the context of civil commitment evaluations?
- Define civil commitment. What legal principles allow the government to restrict an individual’s civil liberties and freedom in this context?
Key Terms
actuarial instruments
best interests of the child principle
CAP Inventory
causal nexus
child abuse
child maltreatment
child neglect
civil commitment
civil forensic assessment
civil law
Classification of Violence Risk (COVR)
criminal commitment
HCR-20
least restrictive alternative principle
parens patriae powers
parenting capacity evaluations
police powers
structured professional judgment
“tender years” doctrine
References
Ackerman, M. J., & Ackerman, M. (1997). Custody evaluation practices: A sur- vey of experienced professionals (revisited). Professional Psychology: Research and Practice, 28, 137–145.
Ackerman, M. J., & Schoendorf, K. (1992). Ackerman-Schoendorf Scales for Parent Evaluation of Custody (ASPECT). Los Angeles: Western Psychological Services.
American Psychiatric Association. (2013). Diagnostic and statistical manual of men- tal disorders (5th ed.). Washington, DC: Author.
American Psychological Association. (1994). Guidelines for child custody evalu- ations in divorce proceedings. American Psychologist, 49, 677–682.
American Psychological Association. (2001). Resolution on UN Convention on the Rights of the Child and the convention’s optional protocols. Approved by the APA Council of Representatives, February 2001.
American Psychological Association. (2010). Guidelines for child custody evalu- ations in family law proceedings. American Psychologist, 65, 863–867.
American Psychological Association. (2013). Guidelines for psychological evalu- ations in child protection matters. American Psychologist, 68, 20–21.
American Psychological Association Committee on Professional Practice and Standards. (2011). Guidelines for psychological evaluations in child protection mat- ters. Washington, DC: American Psychological Association.
Ayoub, C., & Kinscherff, R. (2006). Forensic assessment of parenting in child abuse and neglect cases. In S. N. Sparta & G. P. Koocher (Eds.), Forensic mental health assessment of children and adolescents (pp. 330–341). New York: Oxford University Press.
Beaber, R. J. (1982). Custody quagmire: Some psychological dilemmas. Journal of Psychiatry and Law, 10, 309–326.
Birnbaum, R., & Bala, N. (2010). Towards the differentiation of “high conflict” families: An analysis of social science research and Canadian case law. Family Court Review, 48, 403–416.
Boer, D. P., Hart, S. D., Kropp, P. R., & Webster, C. D. (1997). Manual for the Sexual Violence Risk-20: Professional guidelines for assessing risk of sexual vio- lence. Burnaby, BC: Mental Health, Law, and Policy Institute, Simon Fraser University.
Bonnie, R. J., & Monahan, J. (2005). From coercion to contract: Reframing the debate on mandated community treatment for people with mental disorders. Law and Human Behavior, 29, 487–505.
Bow, J. N., & Quinnell, F. A. (2001). Psychologists’ current practices and proce- dures in child custody evaluations: Five years after American Psychological Association guidelines. Professional Psychology: Research and Practice, 32, 261–268.
Bow, J. N., & Quinnell, F. A. (2004). Critique of child custody evaluations by the legal profession. Family Court Review, 42, 115–127.
Bricklin, B. (1984). Bricklin Perceptual Scales. Furlong, PA: Village.
Canadian Foundation for Children, Youth and the Law v. Canada (Attorney General), SCC 4 [2004], 1 S.C.R. 76 (2004).
Choe, J. Y., Teplin, L. A., & Abram, K. M. (2008). Perpetration of violence, violent victimization, and severe mental illness: Balancing public health con- cerns. Psychiatric Services, 59, 153–164.
Cross, S. E., & Markus, H. R. (1999). The cultural constitution of personality. In L. A. Pervin & O. P. John (Eds.), Handbook of personality (pp. 378–396). New York: Guilford.
Divorce Act, R. S. C.1985, c. 3.
Douglas, K. A., & Koch, W. J. (2001). Civil commitment and civil competence: Psychological issues. In R. A. Schuller & J. R. P. Ogloff (Eds.), An intro- duction to psychology and law: Canadian perspectives (pp. 353–374). Toronto: University of Toronto Press.
Emery, R. E., Otto, R. K., & O’Donohue, W. T. (2005). A critical assessment of child custody evaluations: Limited science and a flawed system. Psychological Science in the Public Interest, 6, 1–29.
English, D. J., & Pecora, P. J. (1994). Risk assessment as a practice in child pro- tective services. Child Welfare, 73, 451–473.
Fang, X., Brown, D. S., Florence, C. S., & Mercy, J. A. (2012). The economic burden of child maltreatment in the United States and implications for pre- vention. Child Abuse and Neglect, 36, 156–165.
Friedman, R. A. (2006). Violence and mental illness—How strong is the link?
New England Journal of Medicine, 355, 2064–2066.
Gallup. (1995). Gallup poll finds far more of America’s children are victims of physical and sexual abuse than officially reported. Princeton, NJ: Author.
Geller, J. L., Fisher, W. H., Grudzinskas, A. J., Clayfield, J. C., & Lawlor, T. (2006). Involuntary outpatient treatment as “deinstitutionalized coercion”: The net-widening concerns. International Journal of Law and Psychiatry, 29, 551–562.
Gordon, R., & Peek, L. A. (1988). The custody quotient. Dallas, TX: Wilmington Institute.
Gray, J. E., & O’Reilly, R. L. (2001). Clinically significant differences among Canadian mental health acts. Canadian Journal of Psychiatry, 46, 315–321.
Gray, J. E., Shone, M. A., & Liddle, P. F. (2008). Canadian mental health law and policy (2nd ed.). Markham, ON: LexisNexis.
Greenfield, T. K., Stoneking, B. C., Humphreys, K., Sundby, E., & Bond, J. (2008). A randomized trial of a mental health consumer-managed alterna- tive to civil commitment for acute psychiatric crisis. American Journal of Community Psychology, 42, 135–144.
Hanson, R. K., & Morton-Bourgon, K. E. (2005). The characteristics of per- sistent sexual offenders: A meta-analysis of recidivism studies. Journal of Consulting and Clinical Psychology, 73, 1154–1163.
Hanson, R. K., & Morton-Bourgon, K. E. (2009). The accuracy of recidivism risk assessments for sexual offenders: A meta-analysis. Psychological Assessment, 21, 1–21.
Hanson, R. K., & Thornton, D. (1999). STATIC-99: Improving actuarial risk assess- ments for sex offenders. Ottawa: Ministry of the Solicitor General of Canada.
Hart, S. D., & Roesch, R. (2012). Mental disorder and the law. In D. J. A. Dozois (Ed.), Abnormal psychology: Perspectives (5th ed., pp. 486–508). Toronto: Pearson.
Henderson, C. R., Swanson, J. W., Szmukler, G., Thornicroft, G., & Zinkler, M. (2008). A typology of advance statements in mental health care. Psychiatric Services, 59, 63–71.
Hussey, J. M., Chang, J. J., & Kotch, J. B. (2006). Child maltreatment in the United States: Prevalence, risk factors, and adolescent health consequences. Pediatrics, 118, 933–942.
Jaffe, P. G., Crooks, C. V., & Bala, N. (2009). A framework for addressing allega- tions of domestic violence in child custody disputes. Journal of Child Custody, 6, 169–188.
Jones, L. M., Finkelhor, D., & Halter, S. (2006). Child maltreatment trends in the 1990s: Why does neglect differ from sexual and physical abuse? Child Maltreatment, 11, 107–120.
Keilin, W. G., & Bloom, L. J. (1986). Child custody evaluation practices: A sur- vey of experienced professionals. Professional Psychology: Research and Practice, 17, 338–346.
Kisely, S., Campbell, L. A., Scott, A., Preston, N., & Xiao, J. (2006). Randomized and nonrandomized evidence for the effect of compulsory community and involuntary outpatient treatment on health service use: Systematic review and meta-analysis. Psychological Medicine, 37, 3–14.
Krug, E. G., Dahlberg, L. L., Mercy, J. A., Zwi, A. B., & Lozano, R. (Eds.). (2002). World report on violence and health. Geneva: World Health Organization. Accessed August 14, 2013 at www.who.int/violence_injury_prevention/ violence/world_report/en.
Kurki-Suonio, K. (2000). Joint custody as an interpretation of the best interests of the child in critical and comparative perspective. International Journal of Law, Policy, and Family, 14, 183–205.
LaFortune, K. A., & Carpenter, B. N. (1998). Custody evaluations: A survey of mental health professionals. Behavioral Sciences and the Law, 16, 201–224.
McKenna, K., Bowlus, A., Day, T., & Wright, D. (2003). The economic costs and consequences of child abuse in Canada. Ottawa: Law Commission of Canada.
McKorkell v. Riverview Hospital (Director), [1993] B. C. J. No. 1518. (S. C.).
McLachlin, B. (2005). Medicine and the law: The challenges of mental illness. Retrieved May 31, 2013, from the Supreme Court of Canada website, www
.scc-csc.gc.ca/court-cour/ju/spe-dis/bm05-02-17-eng.asp.
Melton, G. B., Petrila, J., Poythress, N., & Slobogin, C. (2007). Psychological eval- uations for the courts: A handbook for attorneys and mental health professionals (3rd ed.). New York: Guilford.
Milner, J. S. (2006). The Child Abuse Potential Inventory manual (2nd ed.). Lutz, FL: Psychological Assessment Resources.
Milner, J. S. (2008). Child Abuse Potential (CAP) Inventory. Encyclopedia of psy- chology and law (pp. 69–70). Thousand Oaks, CA: Sage.
Monahan, J. A., Steadman, H. J., Appelbaum, P. S., Grisso, T., Mulvey, E. P., Roth, . . . Silver, E. (2005). Classification of Violence Risk (COVR). Lutz, FL: Psychological Assessment Resources.
Morse, S. J. (2004). Preventive confinement of dangerous offenders. Journal of Law, Medicine, and Ethics, 32, 56–72.
Munsinger, H. L., & Karlson, K. W. (1994). Uniform child custody evaluation sys- tem. Lutz, FL: Psychological Assessment Resources.
O’Neill, J., & Fischer, D. (2005). Fighting for the right to refuse treatment. The Ottawa Citizen, June 11.
Paetsch, J. J., Bertrand, L. D., & Hornick, J. P. (2001). Family Mediation Canada consultation on custody, access, and child support. Ottawa: Department of Justice. Quinsey, V. L., Harris, G. T., Rice, M. E., & Cormier, C. A. (2006). Violent offenders: Appraising and managing risk (2nd ed.). Washington, DC: American
Psychological Association.
Rhoades, H. (2002). The rise and rise of shared parenting laws: A critical reflec- tion. Canadian Journal of Family Law, 19, 75–115.
Roesch, R., Zapf, P. A., & Hart, S. D. (2010). Forensic psychology and law. Hoboken, NJ: Wiley.
Rogler, L. H. (1999). Methodological sources of cultural insensitivity in mental health research. American Psychologist, 54, 424–433.
Schopp, R. F. (2001). Competence, condemnation, and commitment: An integrated theory of mental health law. Washington, DC: American Psychological Association.
Schwartzman, K., & Menzies, D. (2000). Tuberculosis screening of immigrants to low-prevalence countries. American Journal of Respiratory and Critical Care Medicine, 161, 780-789.
Sedlak, A. J., & Broadhurst, D. D. (1996). Third national incidence study of child abuse and neglect. Washington, DC: U.S. Department of Health and Human Services.
Sirotich, F. (2008). Correlates of crime and violence among persons with mental disorder: An evidence-based review. Brief Treatment and Crisis Intervention, 8, 171–194.
Sparta, S. N., & Stahl, P. N. (2006). Psychological evaluation for child custody. In S. N. Sparta & G. P. Koocher (Eds.), Forensic mental health assessment of children and adolescents (pp. 203–229). New York: Oxford University Press.
Starson v. Swayze [2003] 1 SCR 722.
Statistics Canada. (2011). Family court cases involving child custody, access and support arrangements, 2009/2010. Ottawa: Ministry of Industry.
Stowman, S. A., & Donohue, B. (2004). Assessing child neglect: A review of stan- dardized measures. Aggression and Violent Behavior, 10, 491–512.
Straus, M. A., Sugarman, D., & Giles-Sims, J. (1997). Spanking by parents and subsequent antisocial behavior of children. Archives of Pediatric and Adolescent Medicine, 151, 761–767.
United Nations. (1989). Convention on the rights of the child. Adopted and opened for signature, ratification, and accession by General Assembly resolution 44/25 of November 20, 1989.
U.S. Department of Health and Human Services, Administration on Children, Youth and Families. (2008). Child maltreatment 2006. Washington, DC: Author.
Webster, C. D., Douglas, K. S., Eaves, D., & Hart, S. D. (1997). HCR-20: Assessing risk for violence (Version 2). Burnaby, BC: Simon Fraser University.
Winick, B. J. (2008). Civil commitment. In B. Cutler (Ed.), Encyclopedia of psy- chology and law (pp. 89–92). Thousand Oaks, CA: Sage.
Young v. Young, [1993] S. C. J. No. 112.
Suggested Readings and Websites
Justice Canada. (2011). Child abuse: A fact sheet from the Department of Justice Canada. Available at www.justice.gc.ca/eng/pi/fv-vf/facts-info/child-enf. html.
National Clearinghouse on Family Violence. (2001). The Canadian incidence study of reported child abuse and neglect. Ottawa: Health Canada. Available at the Public Health Agency of Canada website, www.phac-aspc.gc.ca/pub- licat/cisfr-ecirf/index-eng.php.
