Chapter 3 Neoplasia
Chapter 3 Neoplasms – Shirley
Zoë Soon
Creative Commons – Simple Pictures, Images, Video Clips, and/or Gifs that help illustrate any of the following:
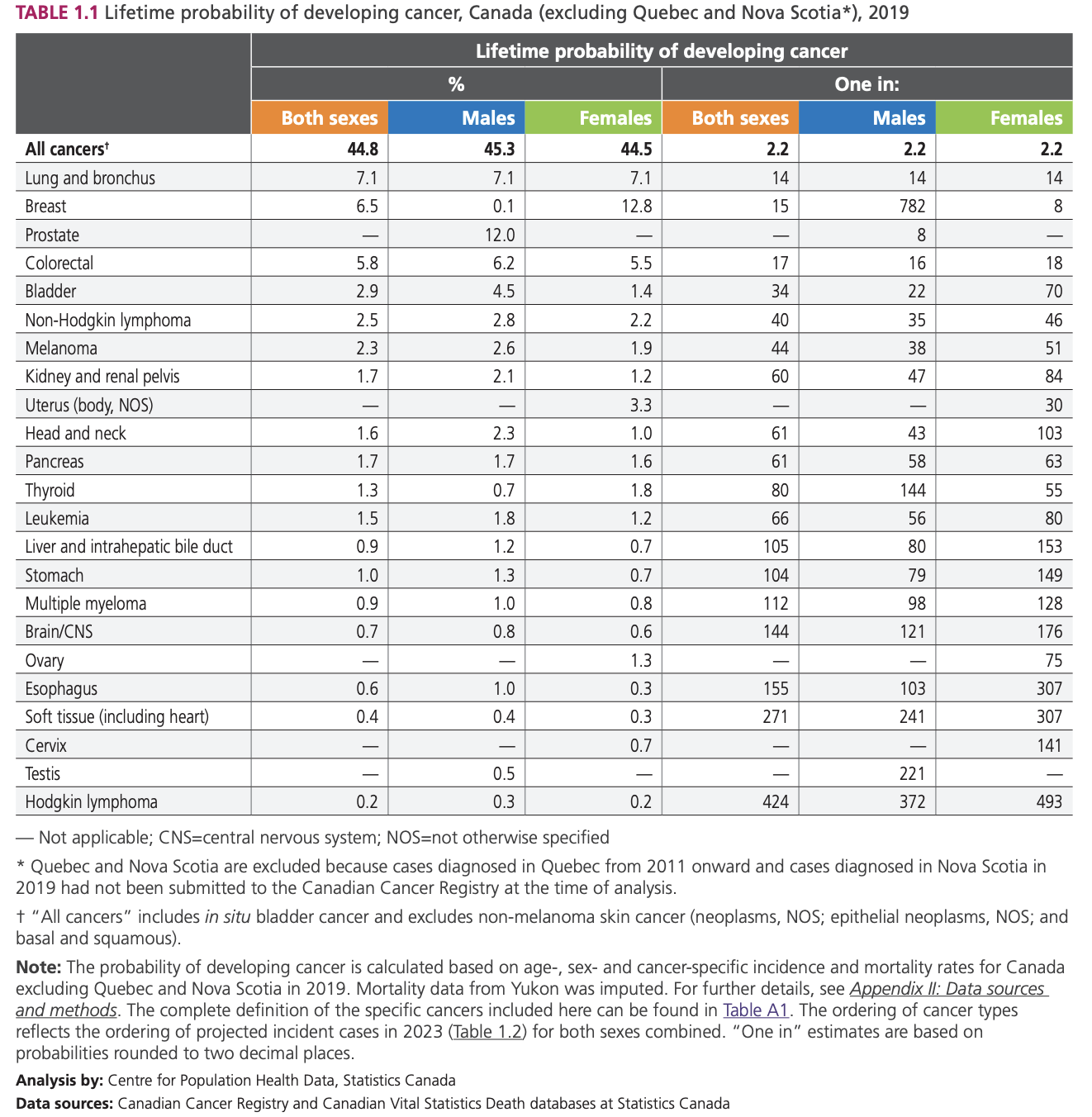
- Statistics Types of Cancer – Incidence and Prevalence Rates in Canada
-
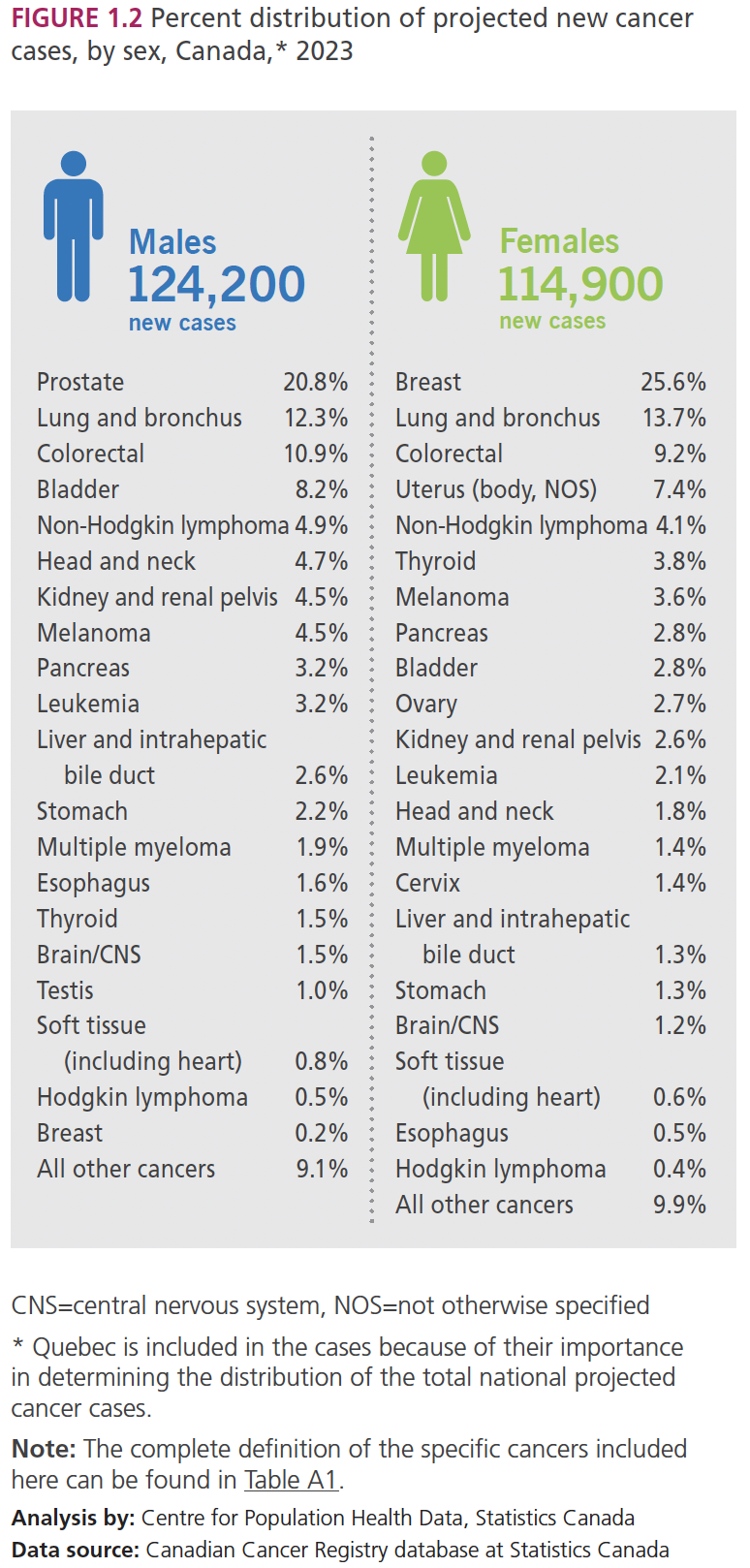
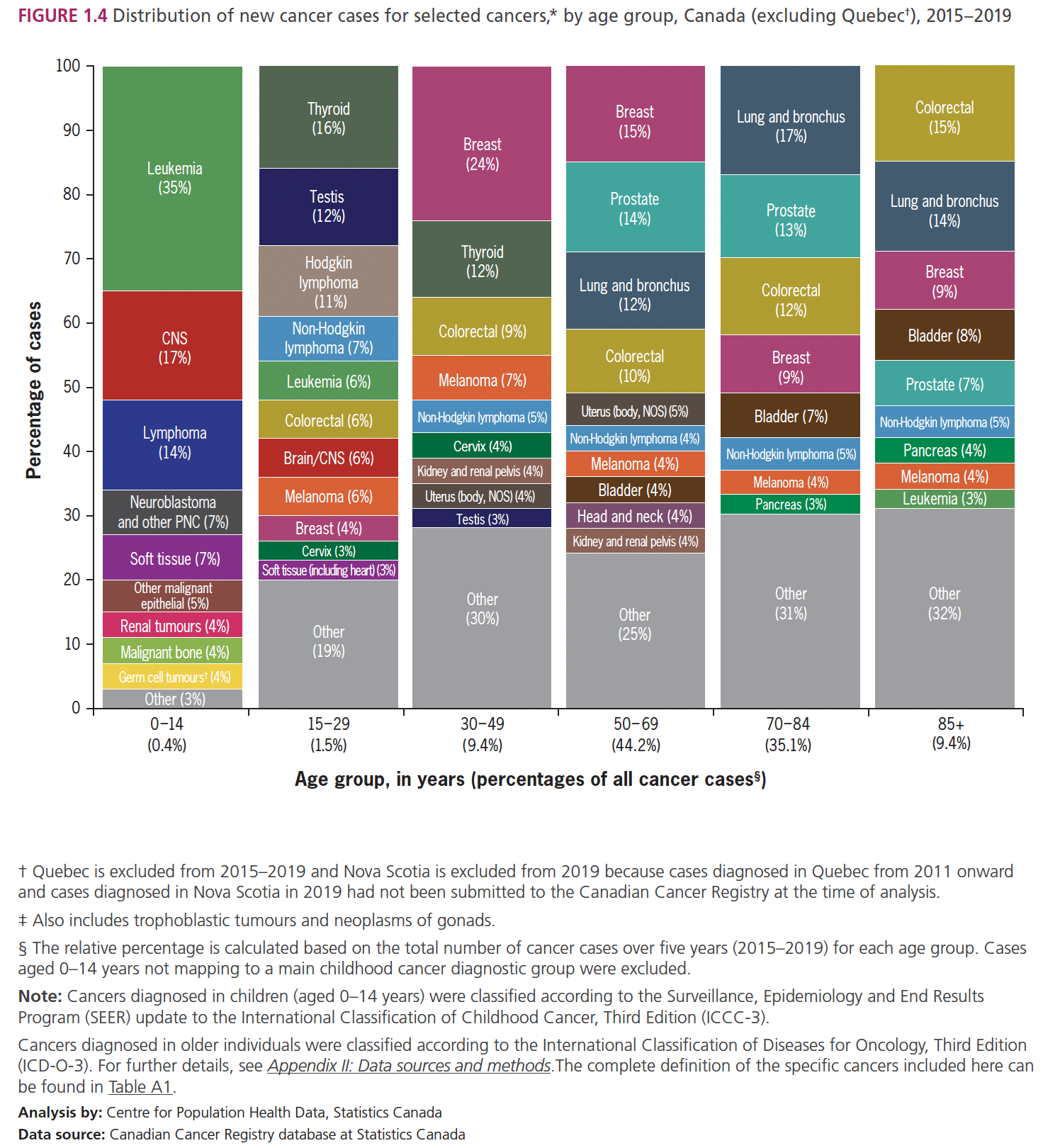
- Canadian Cancer Statistics 2023
-

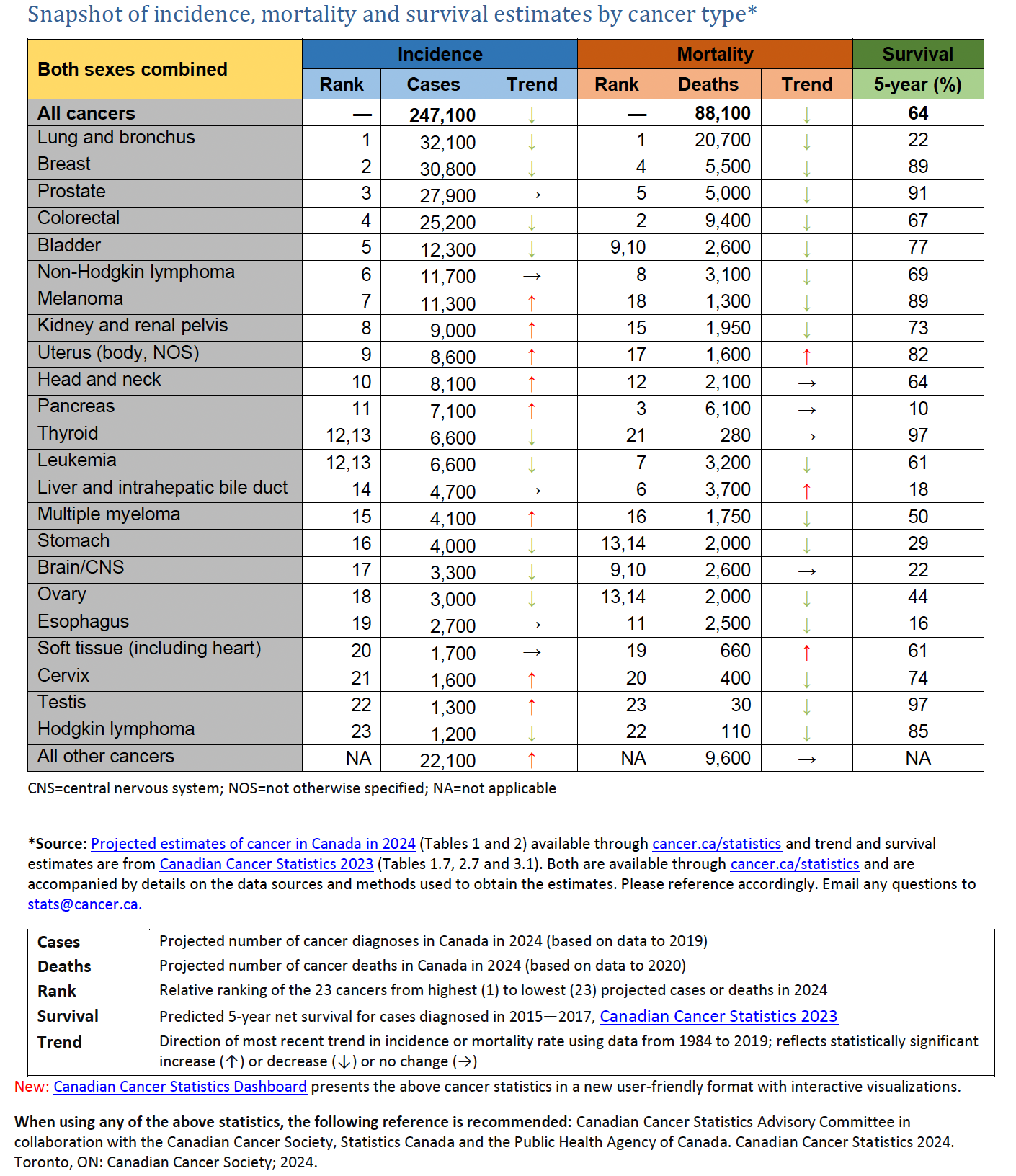
Snapshot of incidence, mortality and survival estimates by cancer type, males -
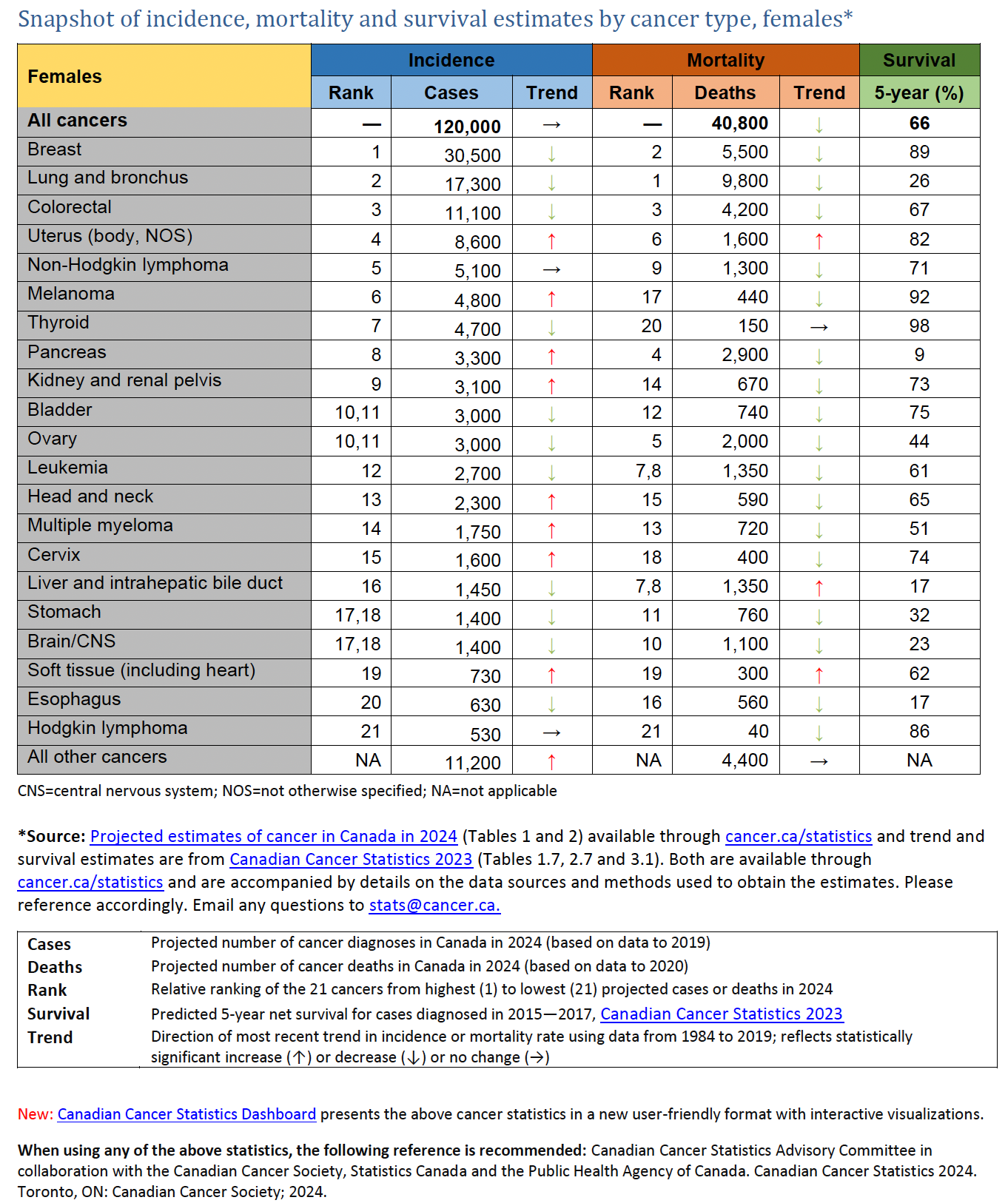
Snapshot of incidence, mortality and survival estimates by cancer type, females
- Quick Review of Cell Cycle and Mitosis including DNA duplication in S phase
-
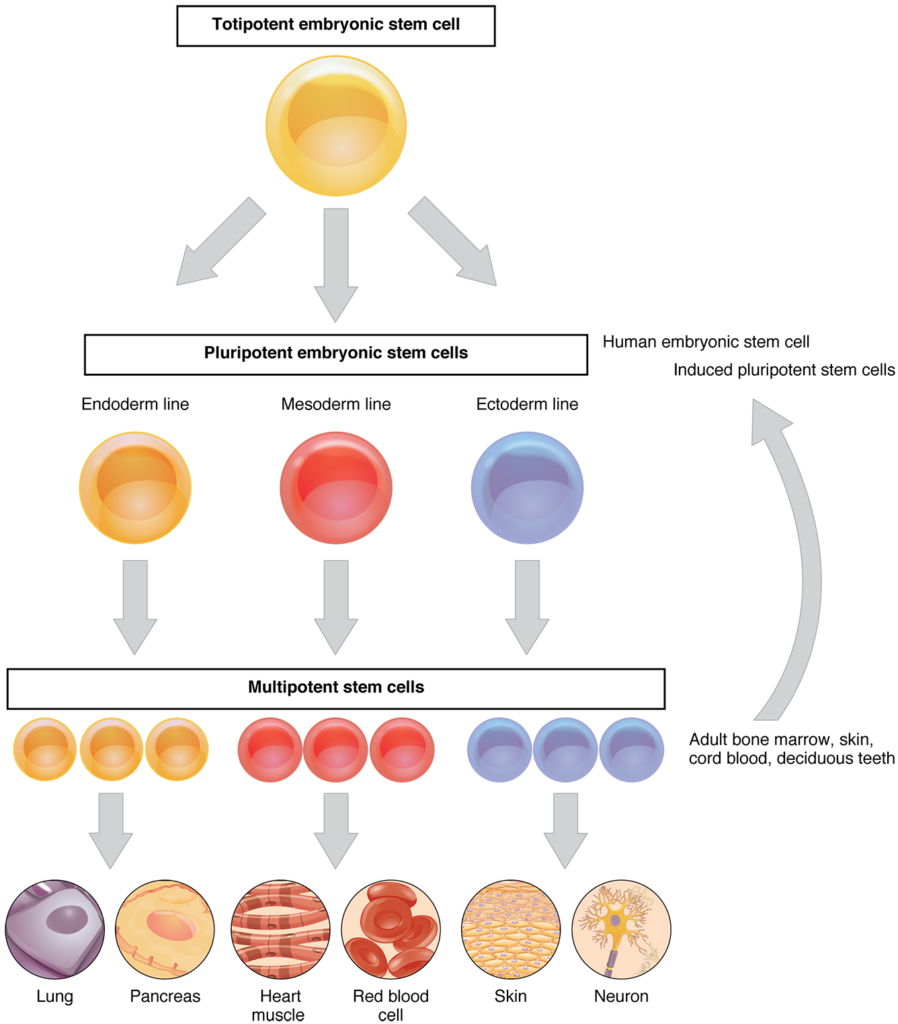
Different cell types & differentiation -
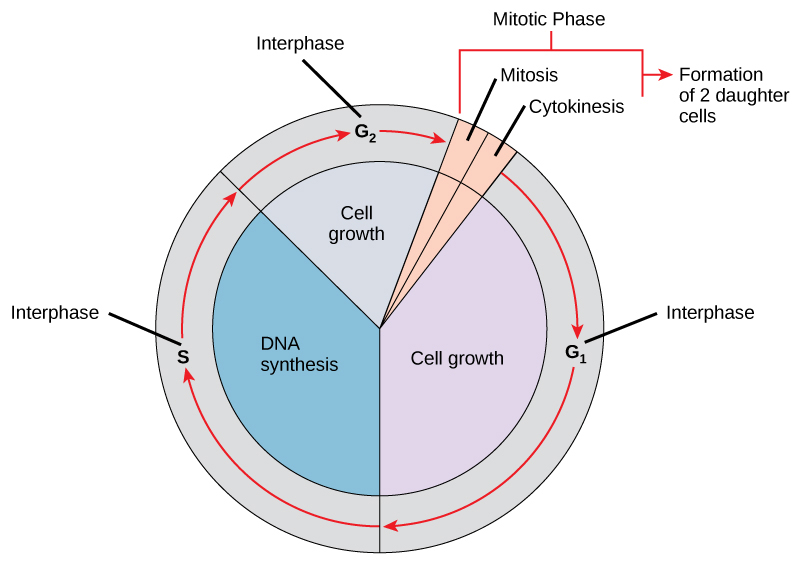
A cell moves through a series of phases in an orderly manner. During interphase, G1 involves cell growth and protein synthesis, the S phase involves DNA replication and the replication of the centrosome, and G2 involves further growth and protein synthesis. The mitotic phase follows interphase. Mitosis is nuclear division during which duplicated chromosomes are segregated and distributed into daughter nuclei. Usually the cell will divide after mitosis in a process called cytokinesis in which the cytoplasm is divided and two daughter cells are formed. -
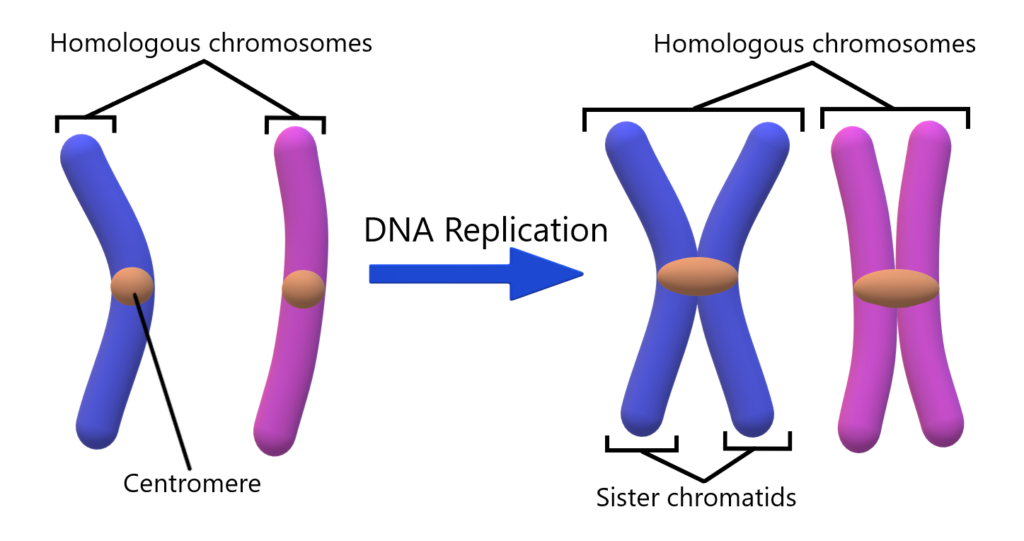
Outcome of S phase: The S phase is called synthesis because making a copy of the chromosome requires new DNA production, or synthesis.
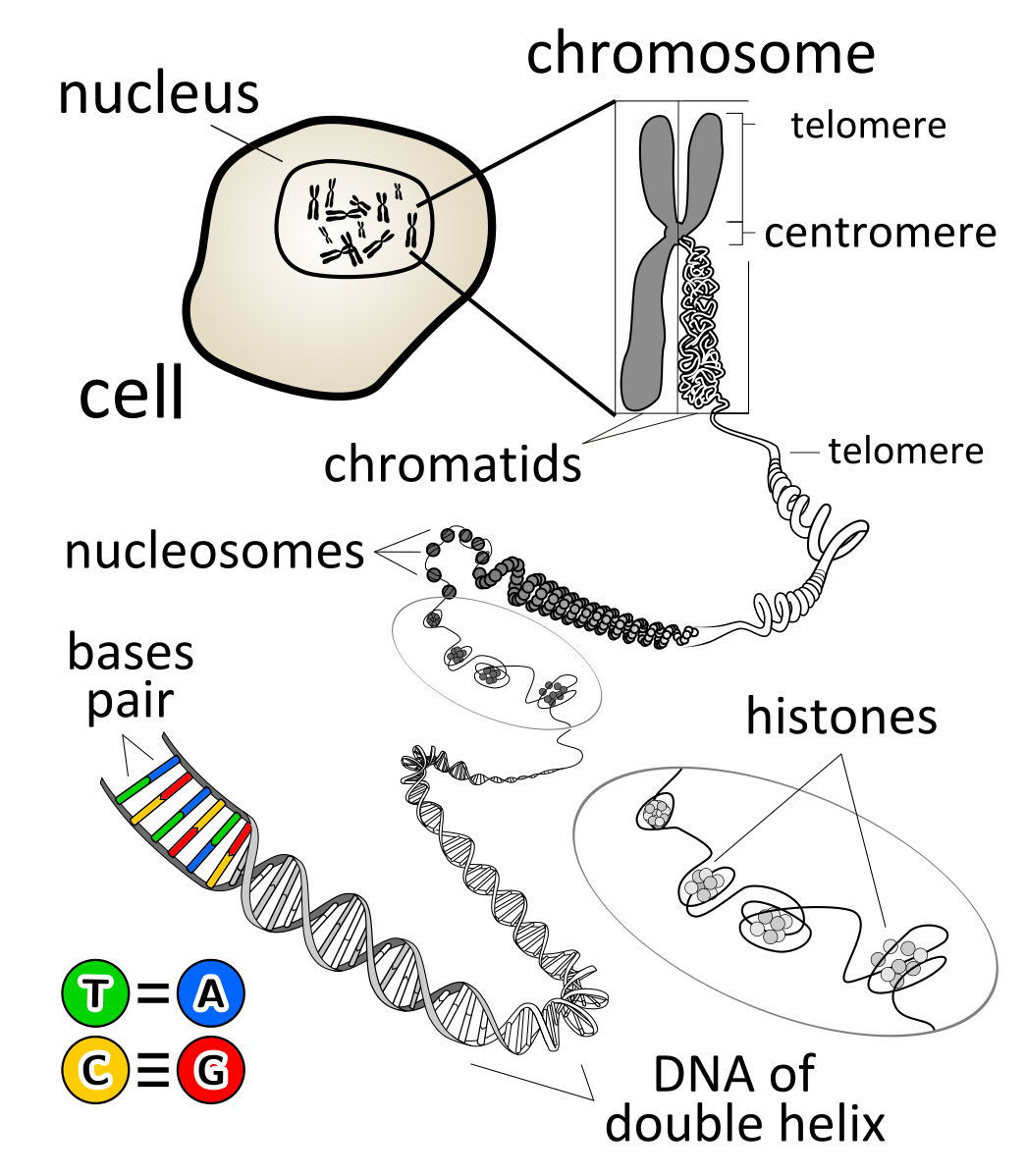
The two chromosomes that are exact copies are called sister chromatids and remain connected at one spot along their length; this spot is called the centromere, as shown in the illustration. -
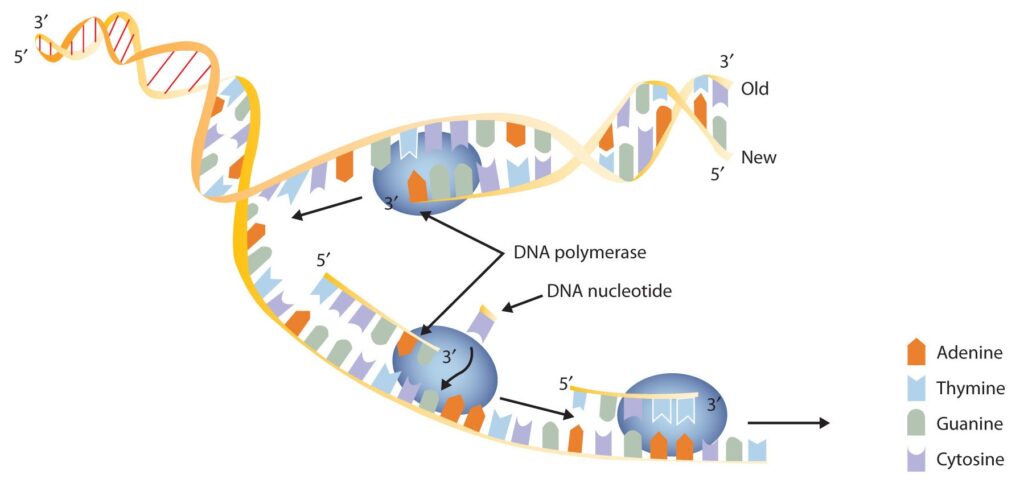
Schematic Diagram of DNA Replication. DNA replication occurs by the sequential unzipping of segments of the double helix. Each new nucleotide is brought into position by DNA polymerase and is added to the growing strand by the formation of a phosphate ester bond. Thus, two double helixes form from one, and each consists of one old strand and one new strand, an outcome called semiconservative replications. (This representation is simplified; many more proteins are involved in replication.) - ·
-
- The importance of telomeres and inactivation of telomerase during aging
-
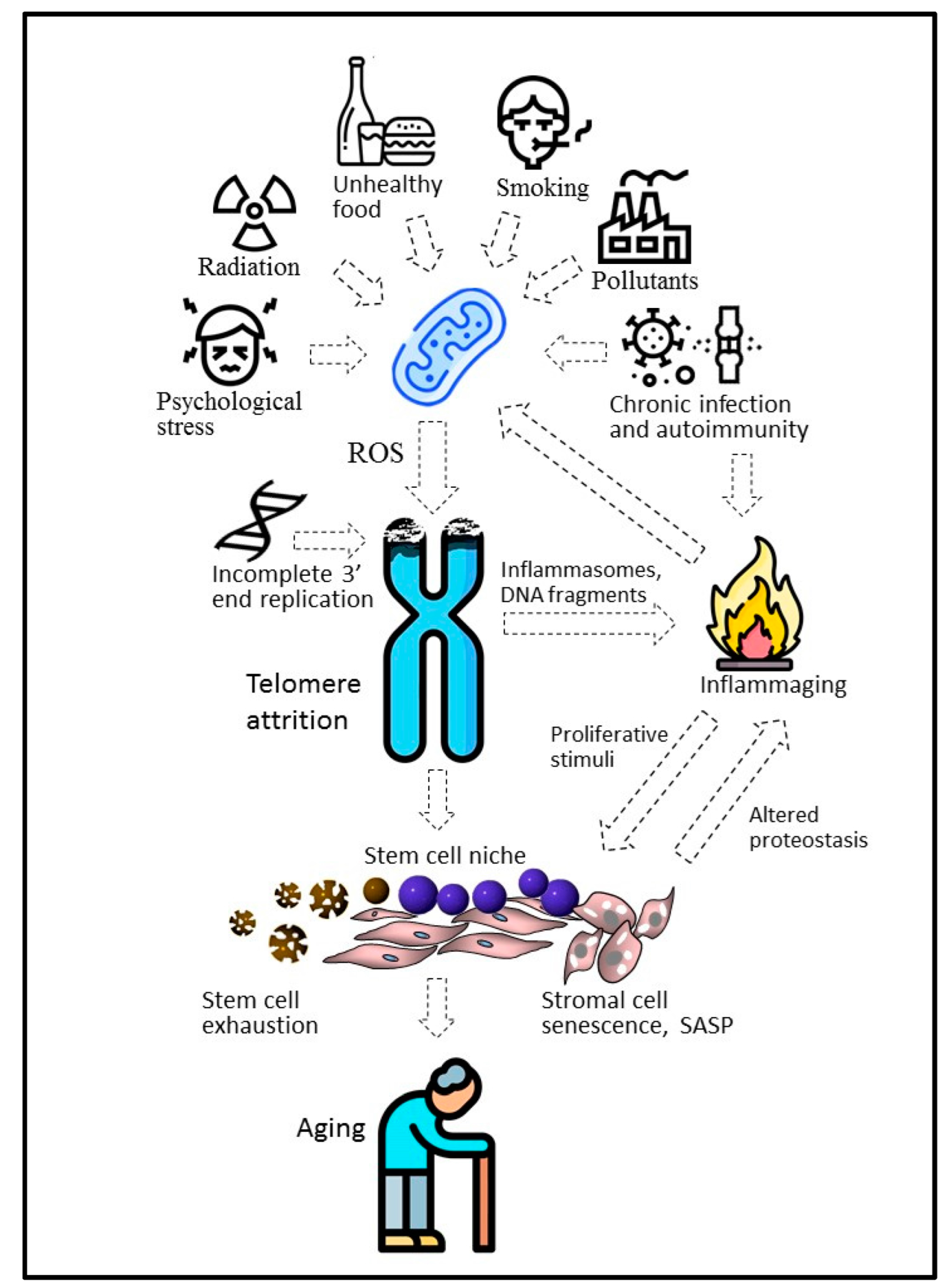
Telomere theory of aging: At the organismal level, chemical pollutants, radiation, infections, smoking, and even psychological stress or apnea can enhance telomere shortening -
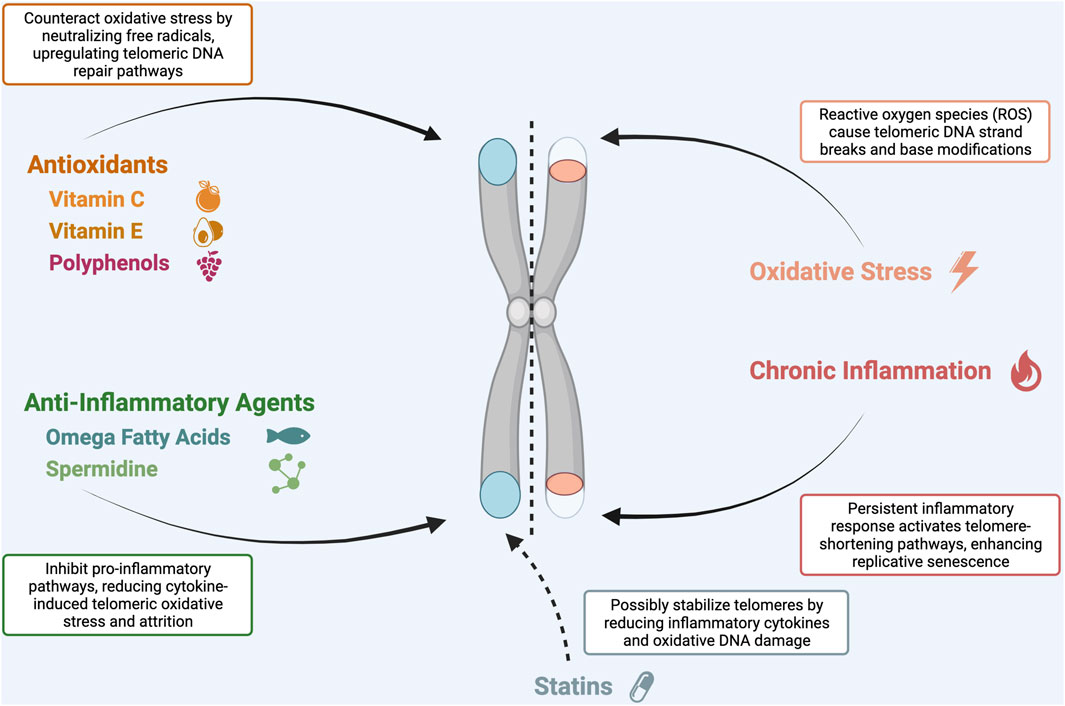
The role of antioxidants and anti-inflammatory agents in terlomere maintenance. -
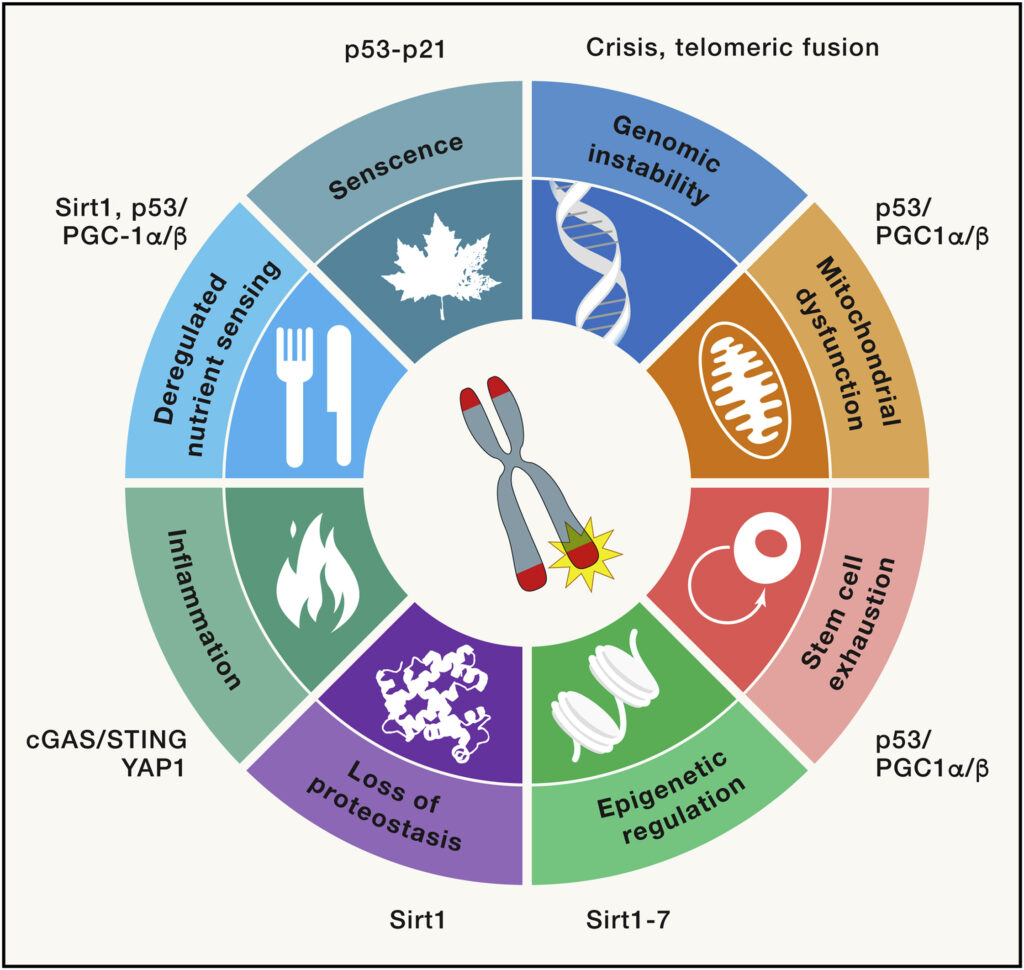
Relevance of telomere dysfunction to cellular aging hallmarks
Telomere dysfunction can drive the hallmarks of cellular aging. -

Telomere/telomerase in aging, cancer, and potential therapy
- DNA duplication – potential for errors triggering apoptosis or permanent mutations
-
DNA replication -
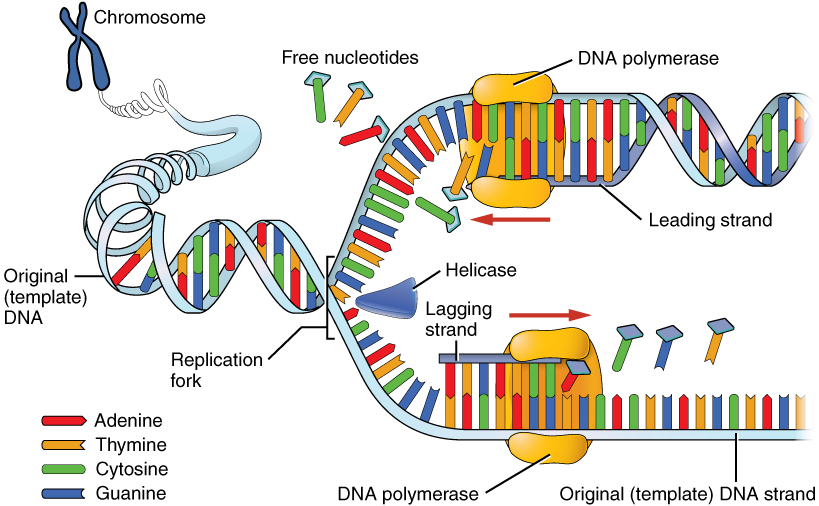
DNA Replication faithfully duplicates the entire genome of the cell. During DNA replication, a number of different enzymes work together to pull apart the two strands so each strand can be used as a template to synthesize new complementary strands. The two new daughter DNA molecules each contain one pre-existing strand and one newly synthesized strand. Thus, DNA replication is said to be “semiconservative.”
Stage 1: Initiation. The two complementary strands are separated, much like unzipping a zipper. Special enzymes, including helicase, untwist and separate the two strands of DNA.
Stage 2: Elongation. Each strand becomes a template along which a new complementary strand is built. DNA polymerase brings in the correct bases to complement the template strand, synthesizing a new strand base by base. A DNA polymerase is an enzyme that adds free nucleotides to the end of a chain of DNA, making a new double strand. This growing strand continues to be built until it has fully complemented the template strand.
Stage 3: Termination. Once the two original strands are bound to their own, finished, complementary strands, DNA replication is stopped and the two new identical DNA molecules are complete. -

General overview of DNA damage response networks activate by DNA damage. -
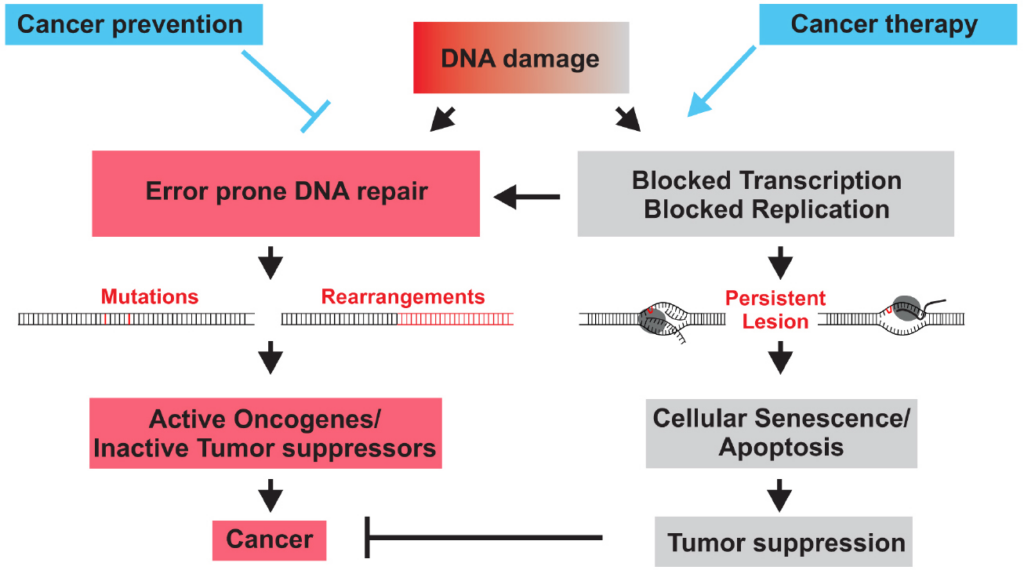
DNA damage causes cancer development when erroneous DNA repair leads to mutations of chromosomal aberration that activate oncogenes or inactivate tumor suppressors genes (red). - `
-
- DNA duplication – DNA sequence enzyme checkers
-
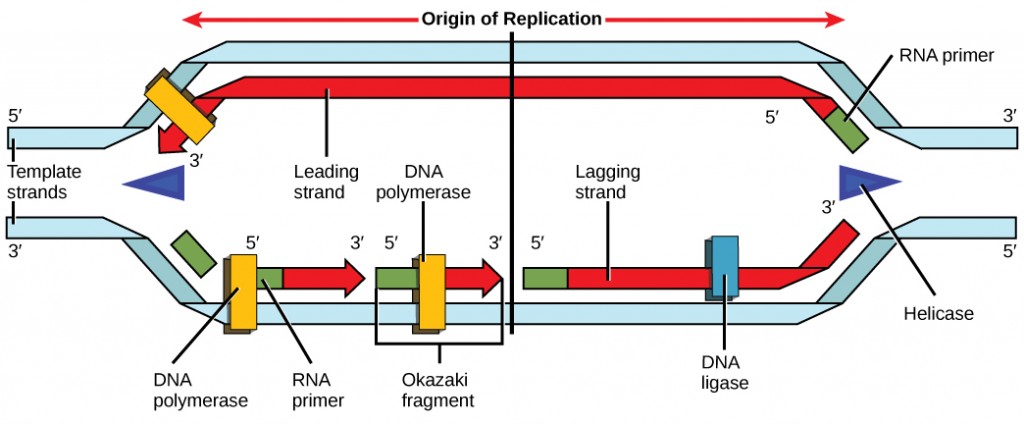
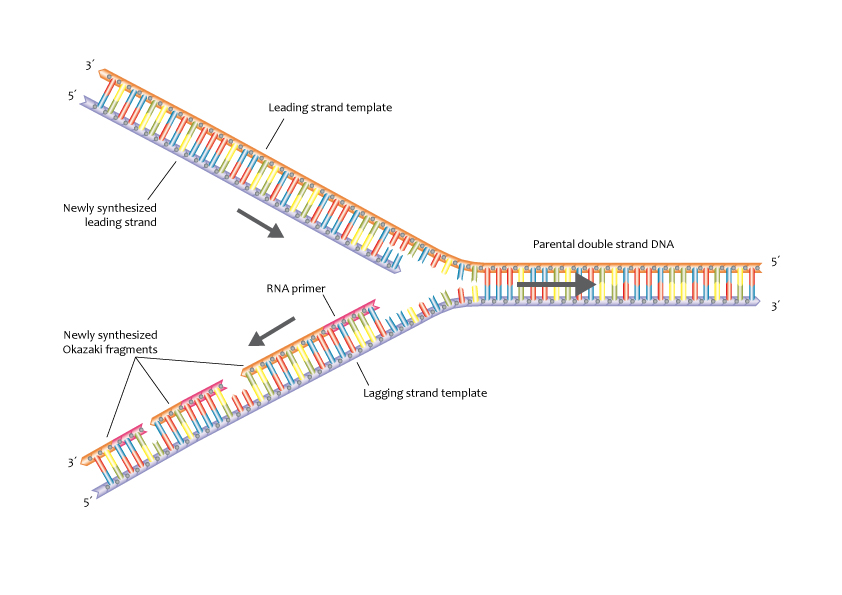
A replication fork is formed by the opening of the origin of replication, and helicase separates the DNA strands. An RNA primer is synthesized, and is elongated by the DNA polymerase. On the leading strand, DNA is synthesized continuously, whereas on the lagging strand, DNA is synthesized in short stretches. The DNA fragments are joined by DNA ligase (not shown). -
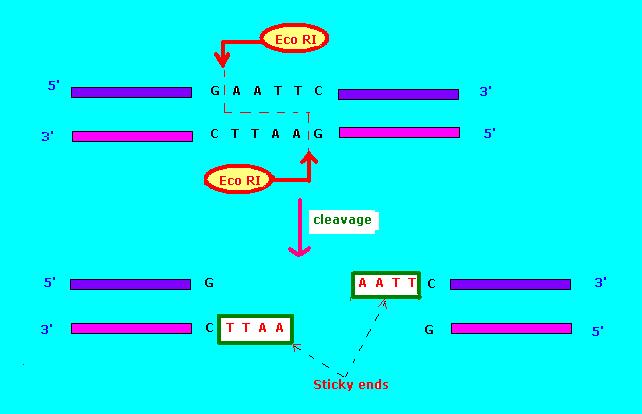
Restriction enzyme Eco RI - `
- `
- `
-
- Cell cycling regulation and Apoptosis regulation
-
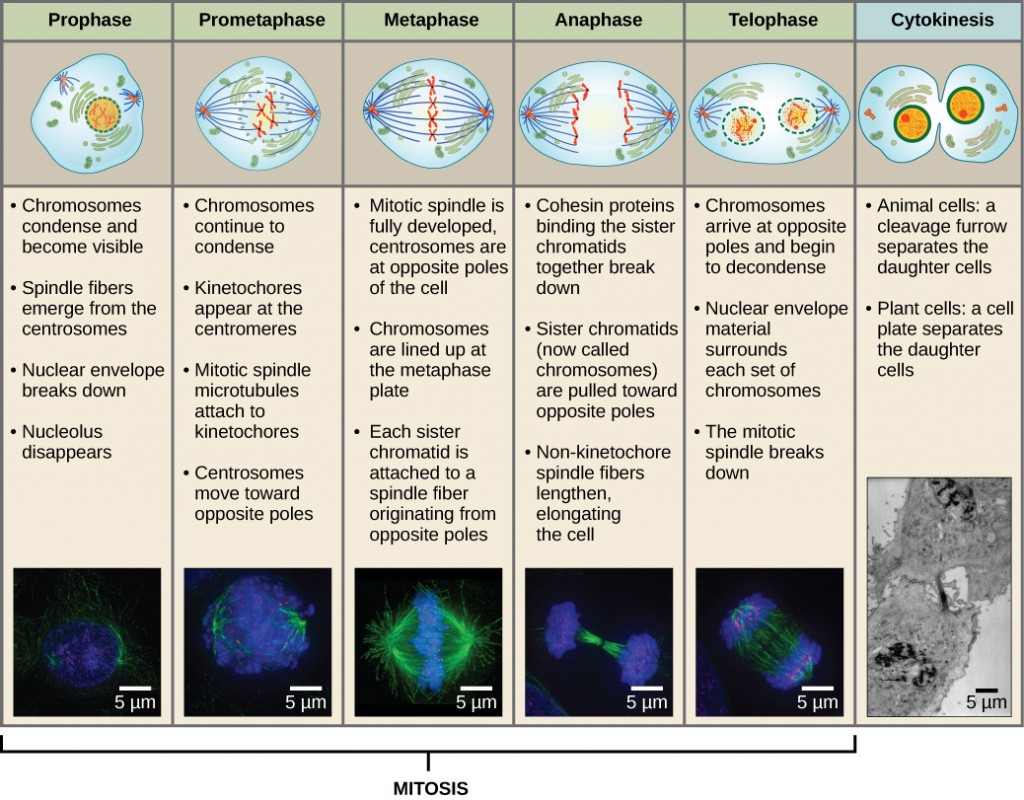
Animal cell mitosis is divided into five stages—prophase, prometaphase, metaphase, anaphase, and telophase—visualized here by light microscopy with fluorescence. Mitosis is usually accompanied by cytokinesis, shown here by a transmission electron microscope. (credit “diagrams”: modification of work by Mariana Ruiz Villareal; credit “mitosis micrographs”: modification of work by Roy van Heesbeen; credit “cytokinesis micrograph”: modification of work by the Wadsworth Center, NY State Department of Health; donated to the Wikimedia foundation; scale-bar data from Matt Russell) -
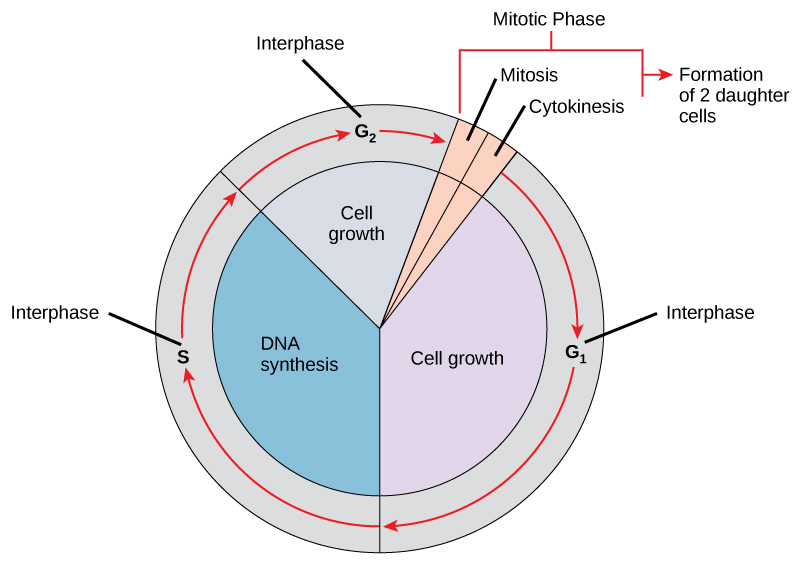
A cell moves through a series of phases in an orderly manner. During interphase, G1 involves cell growth and protein synthesis, the S phase involves DNA replication and the replication of the centrosome, and G2 involves further growth and protein synthesis. The mitotic phase follows interphase. Mitosis is nuclear division during which duplicated chromosomes are segregated and distributed into daughter nuclei. Usually the cell will divide after mitosis in a process called cytokinesis in which the cytoplasm is divided and two daughter cells are formed. -
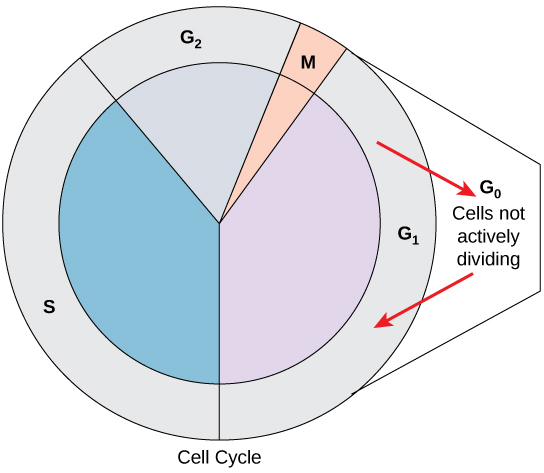
Cells that are not actively preparing to divide enter an alternate phase called G0. In some cases, this is a temporary condition until triggered to enter G1. In other cases, the cell will remain in G0 permanently. -

The cell cycle is controlled at three checkpoints. Integrity of the DNA is assessed at the G1 checkpoint. Proper chromosome duplication is assessed at the G2 checkpoint. Attachment of each kinetochore to a spindle fiber is assessed at the M checkpoint. - https://youtu.be/Z-r33PiKBLM
-
- Cell cycling regulation – growth factors and growth inhibiting factors
-

Hormonal Regulation of Growth. Growth hormone (GH) directly accelerates the rate of protein synthesis in skeletal muscle and bones. Insulin-like growth factor 1 (IGF-1) is activated by growth hormone and indirectly supports the formation of new proteins in muscle cells and bone. From Betts, et al., 2013. - `
-
- Mutation of genes responsible for regulating cell cycling and/or apoptosis can lead to cancer (Tumor Supressor Genes, Protooncogenes, Stability genes (e.g. p53)
-
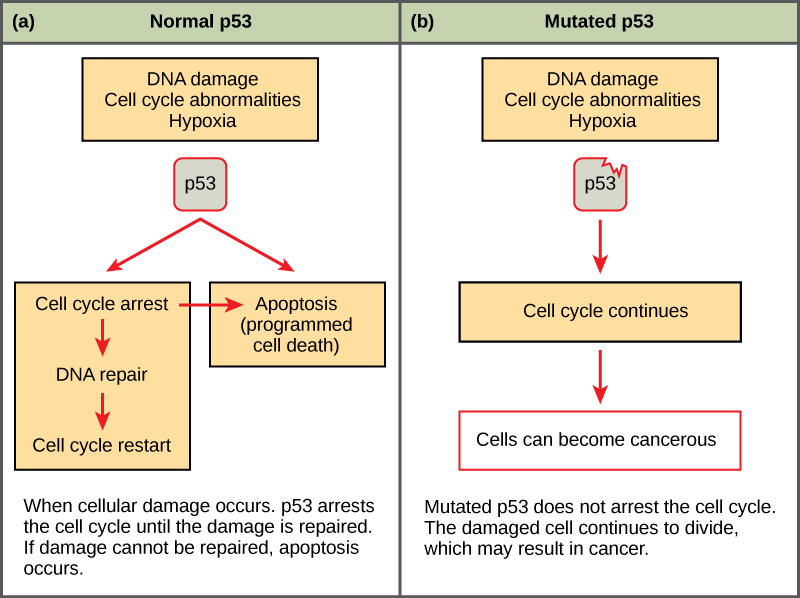
(a) The role of p53 is to monitor DNA. If damage is detected, p53 triggers Tumor suppressor gene protein p53: repair mechanisms. If repairs are unsuccessful, p53 signals apoptosis. (b) A cell with an abnormal p53 protein cannot repair damaged DNA and cannot signal apoptosis. Cells with abnormal p53 can become cancerous. (credit: modification of work by Thierry Soussi)
-
- DNA mutation – caused by Viruses, Radiation (UV, X-rays, gamma rays), Chemicals, spontaneous errors, inherited mutations
-
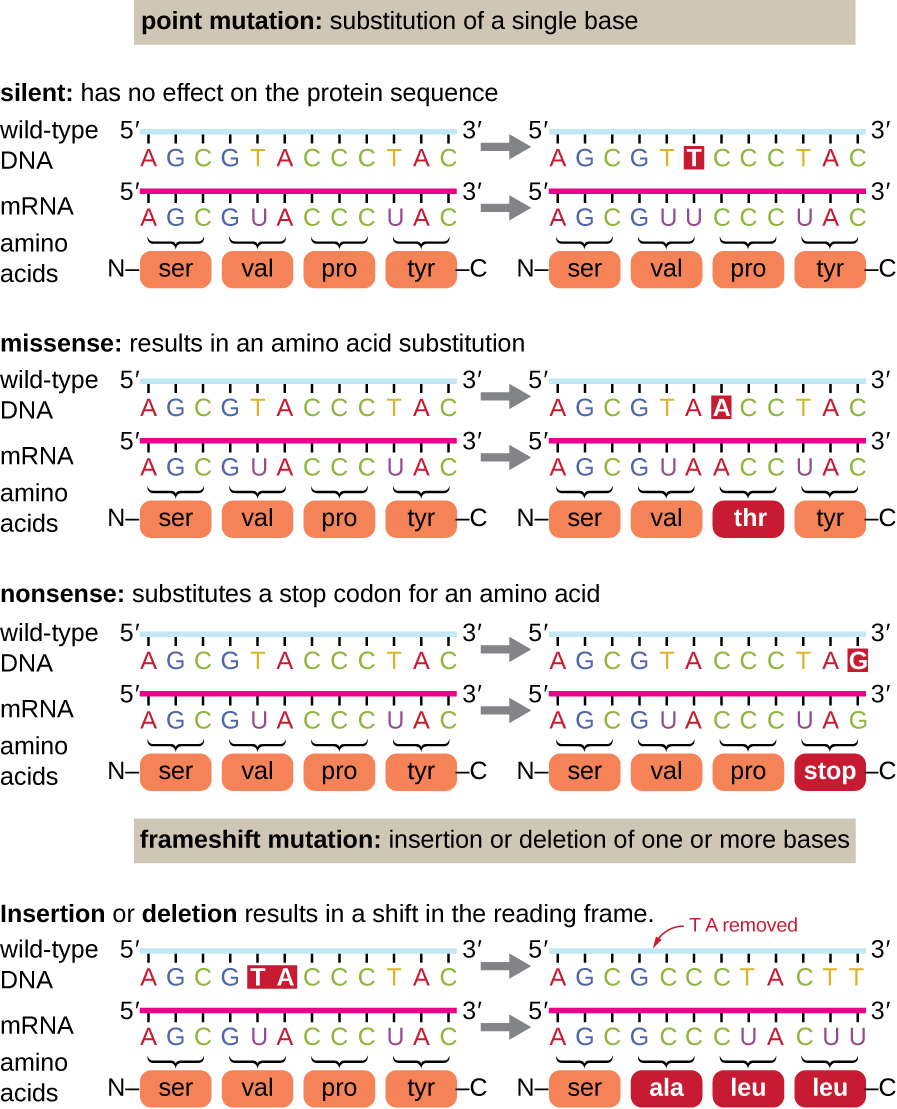
Mutations can lead to changes in the protein sequence encoded by the DNA. -
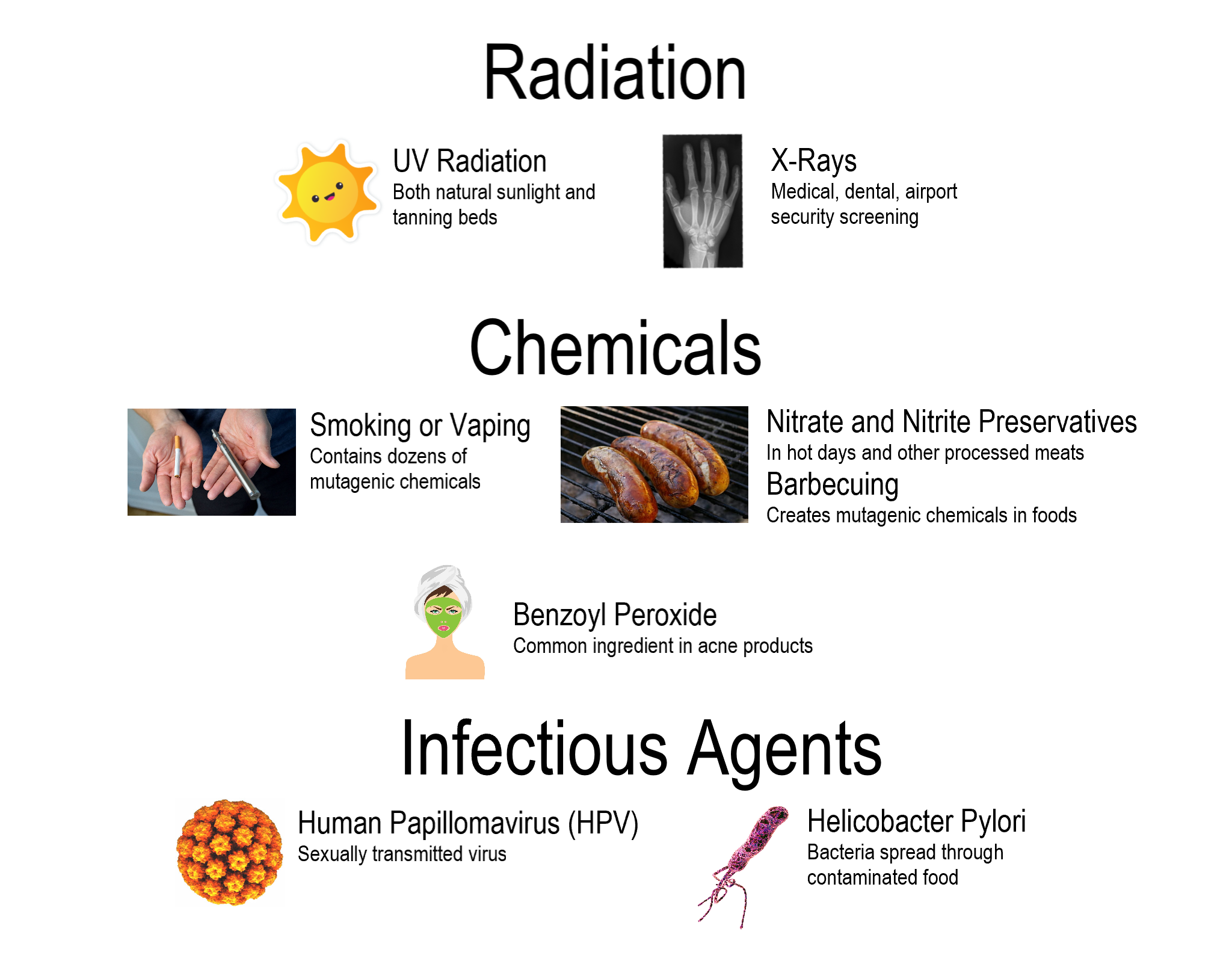
Examples of Mutagens. Types of mutagens include radiation, chemicals, and infectious agents. -
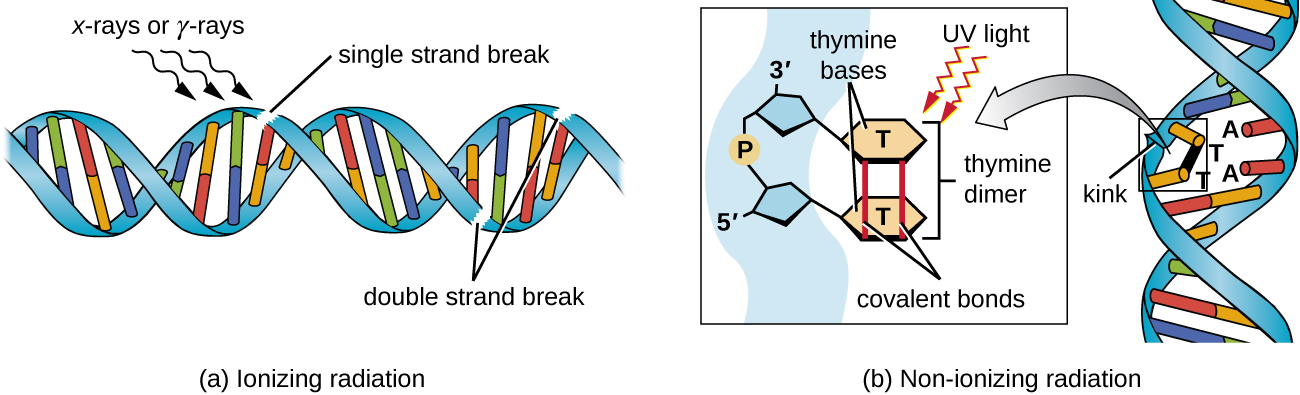
DNA mutation by radiation: (a) Ionizing radiation may lead to the formation of single-stranded and double-stranded breaks in the sugar-phosphate backbone of DNA, as well as to the modification of bases (not shown). (b) Nonionizing radiation like ultraviolet light can lead to the formation of thymine dimers, which can stall replication and transcription and introduce frameshift or point mutations.
-
- Risk factors for DNA mutations and therefore risks for cancer – continuous injury repair, exposure to carcinogens found in cigarette smoke, industrial pollutants, asbestos, cell types that divide frequently (eg. epithelial cells, followed by connective tissue cells), certain viruses, diet, age, chemicals,
-
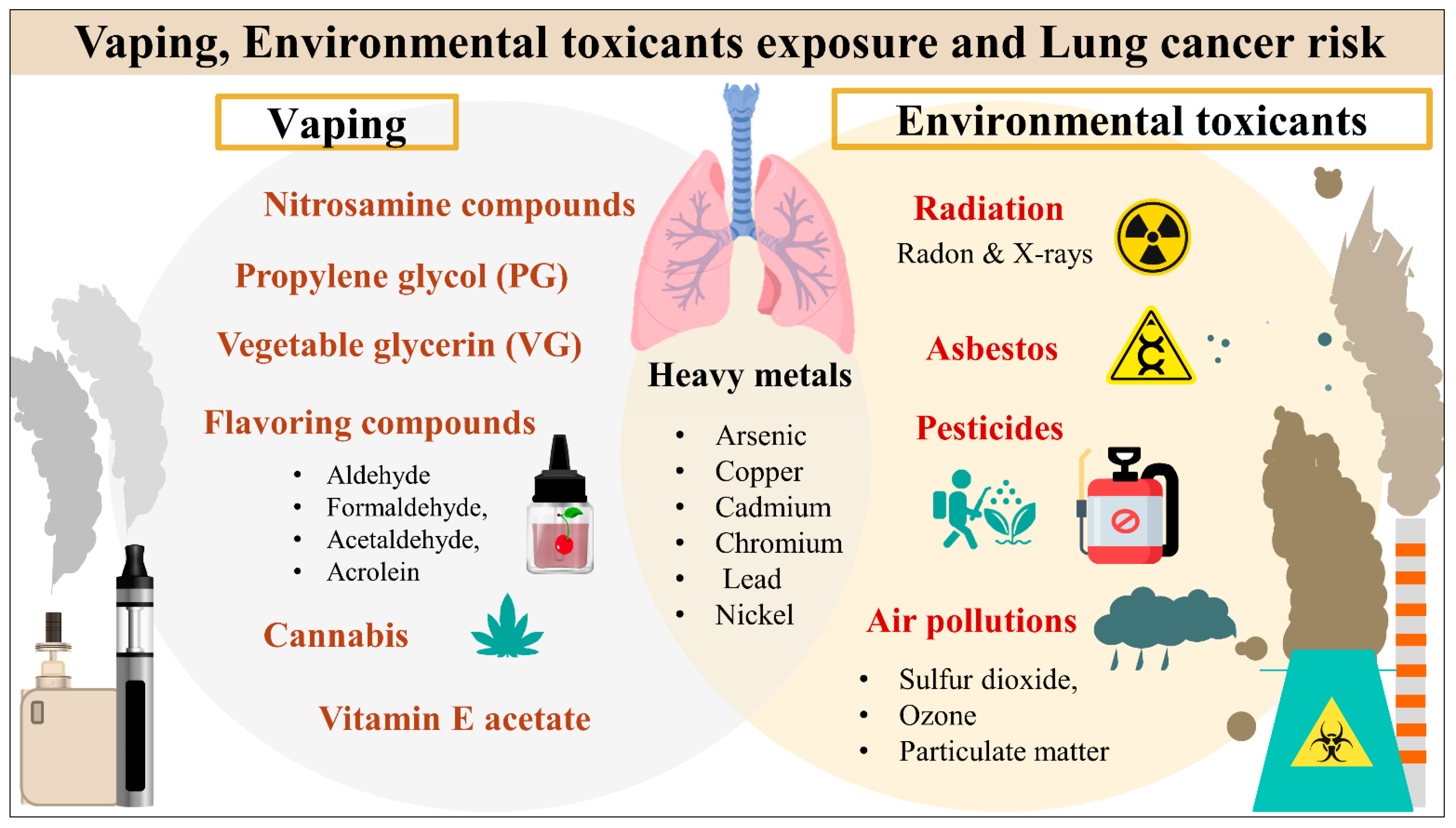
Vaping products and environmental toxicants exposure and lung cancer risk. - `
- `
-
- Types of DNA mutations – insertion, substitution, deletion, synonymous, non-synonymous
-
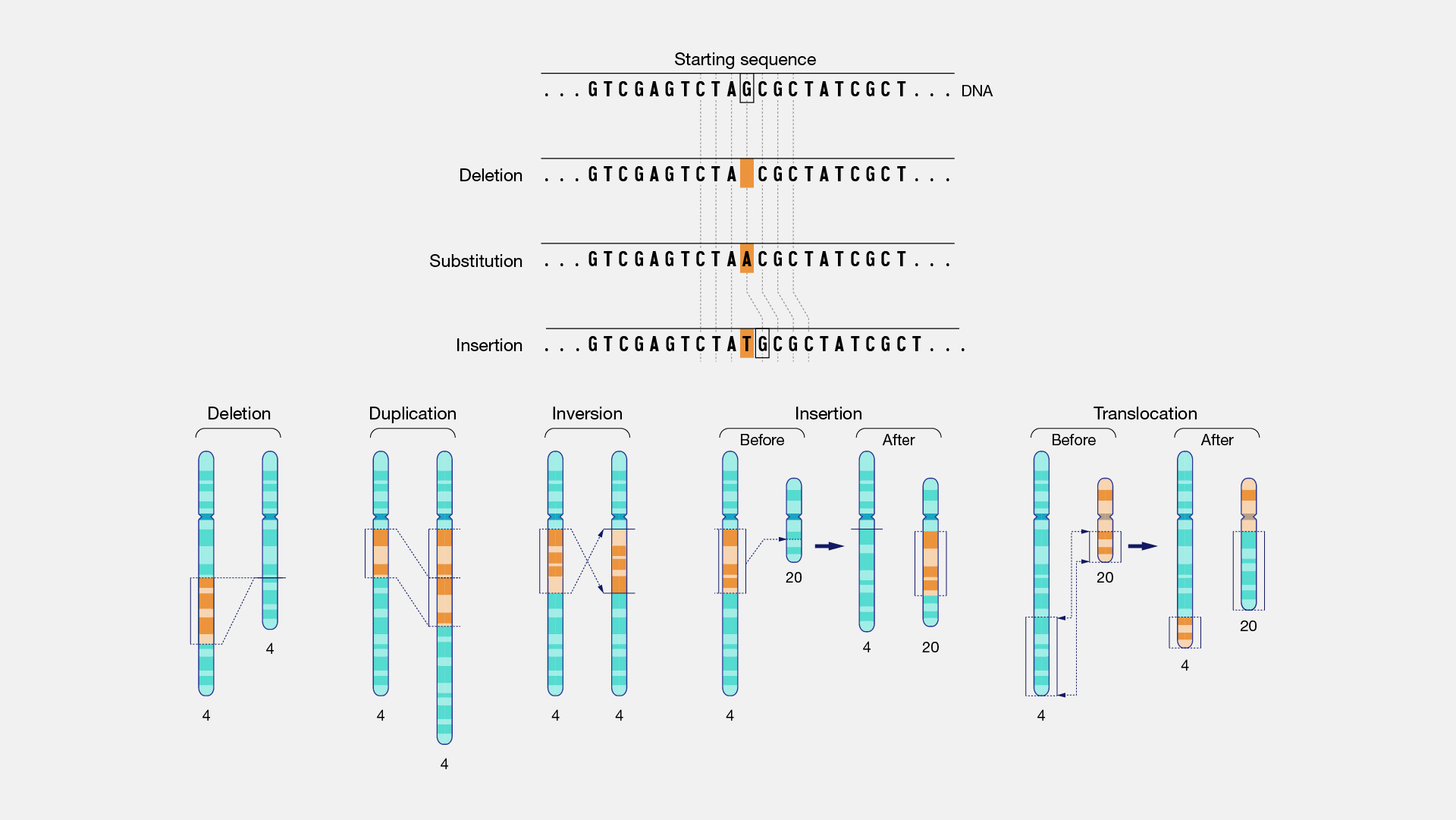
A mutation is a change in the DNA sequence of an organism. Mutations can result from errors in DNA replication during cell division, exposure to mutagens or a viral infection. -
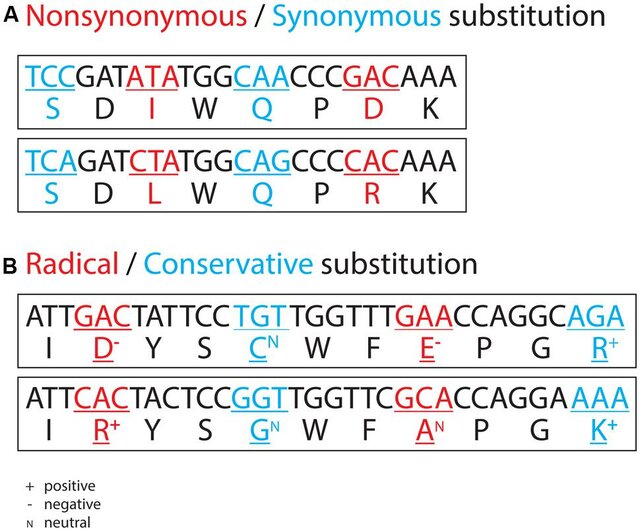
Examples of non-synonymous and synonymous nucleotide substitutions (A) and examples of radical and conservative non-synonymous nucleotide substitutions (B). In the former, a non-synonymous substitution leads to an amino acid replacement, and a synonymous substitution does not. In the latter, the 20 amino acids show different physicochemical properties, such as charge. A radical non-synonymous substitution leads to an amino acid replacement with a concomitant change in charge, and a conservative non-synonymous substitution leads to an amino acid replacement without a change in charge.
-
- Differences between benign tumors and malignant tumors
-
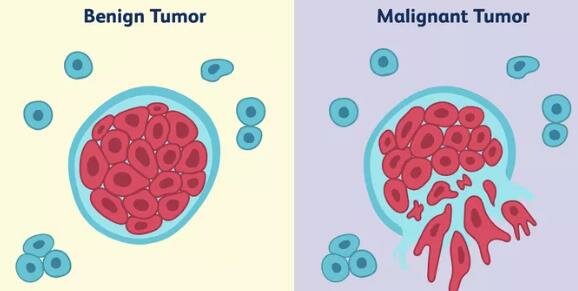
The benign and malignant tumor. -
Benign tumors Malignant tumors Cancer Not considered cancer Cancer Ability to invade and metastasize No Yes Differentiation Differentiated cells Undifferentiated, nonfunctional dysplastic cells Growth rate Slow Fast Reoccurance after removal No Yes Suffix -oma -carcinoma
-
- Naming of Malignant Tumors (Carcinomoa, Sarcoma, Glioma etc.)
- Carcinoma
- Adenocarcinomas: Adenocarcinomas start in glandular cells called adenomatous cells. Glandular cells produce fluids to keep tissues moist.
-
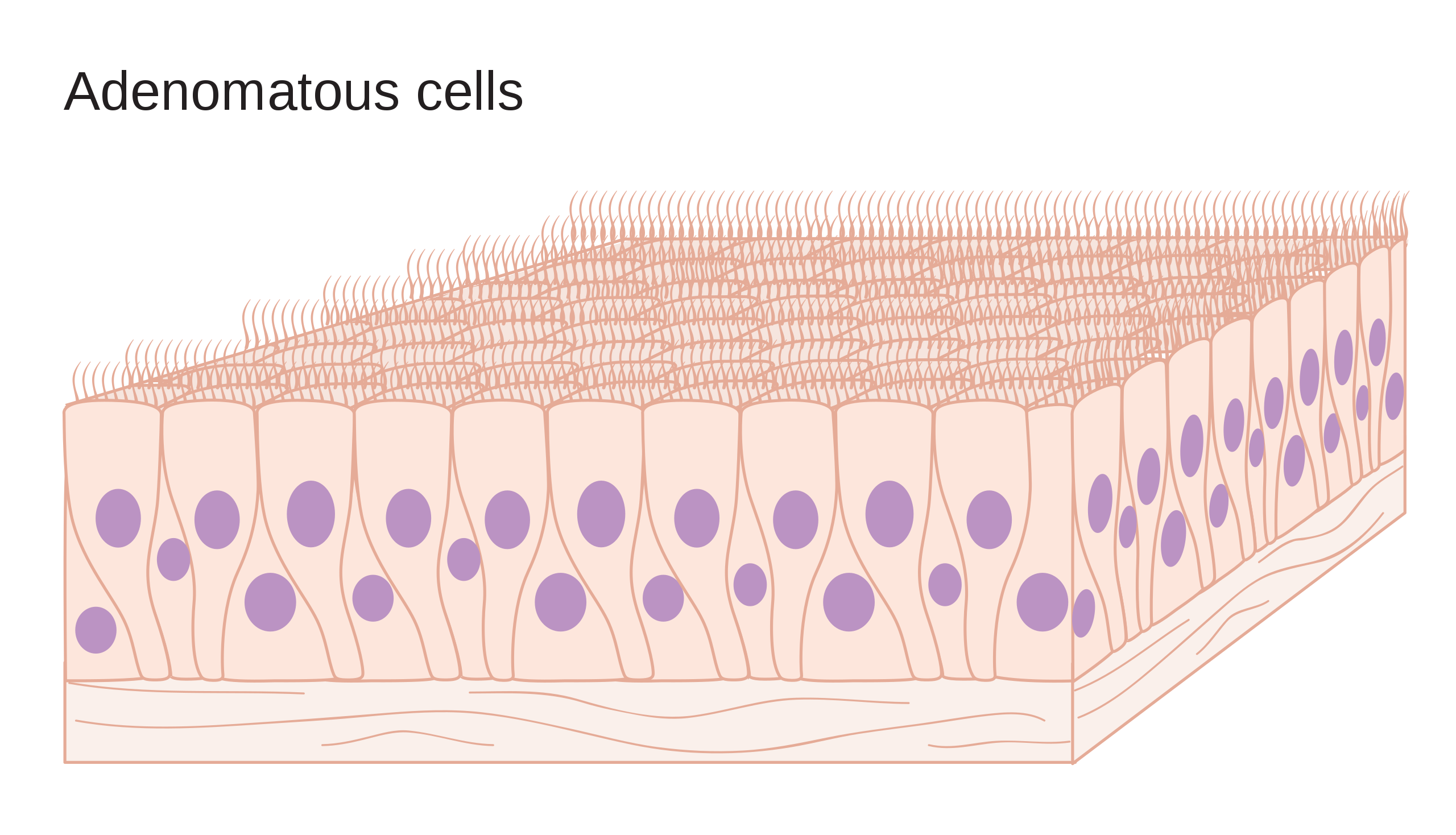
Diagram of glandular cells
-
- Squamous cell carcinoma: Squamous cell carcinoma starts in squamous cells. These are the flat, surface covering cells found in areas such as the skin or the lining of the throat or food pipe (oesophagus).
-
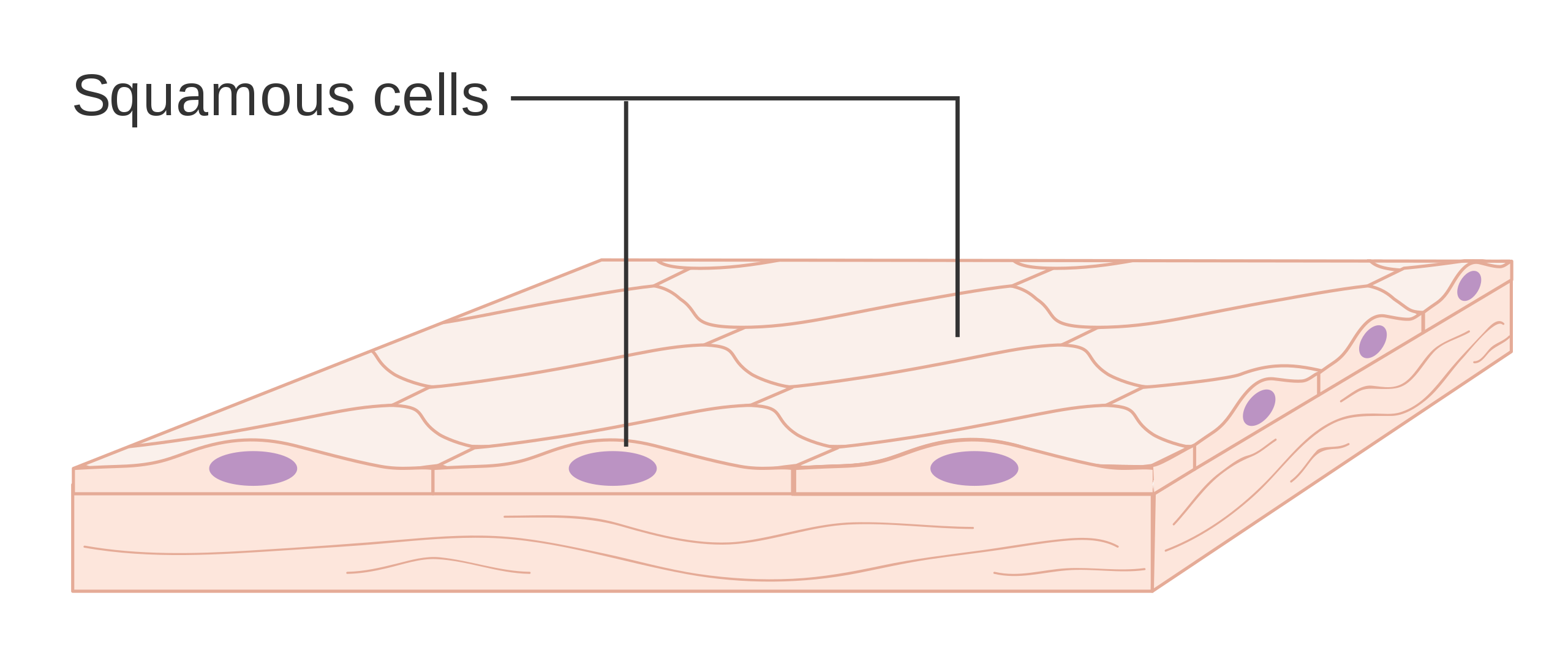
Diagram of squamous cells
-
- Melanomas: epithelial cancers originating in the melanocytes of the skin.
- Melanoma is cancer that begins in cells that become melanocytes, which are specialized cells that make melanin (the pigment that gives skin its color). Most melanomas form on the skin, but melanomas can also form in other pigmented tissues, such as the eye.
-
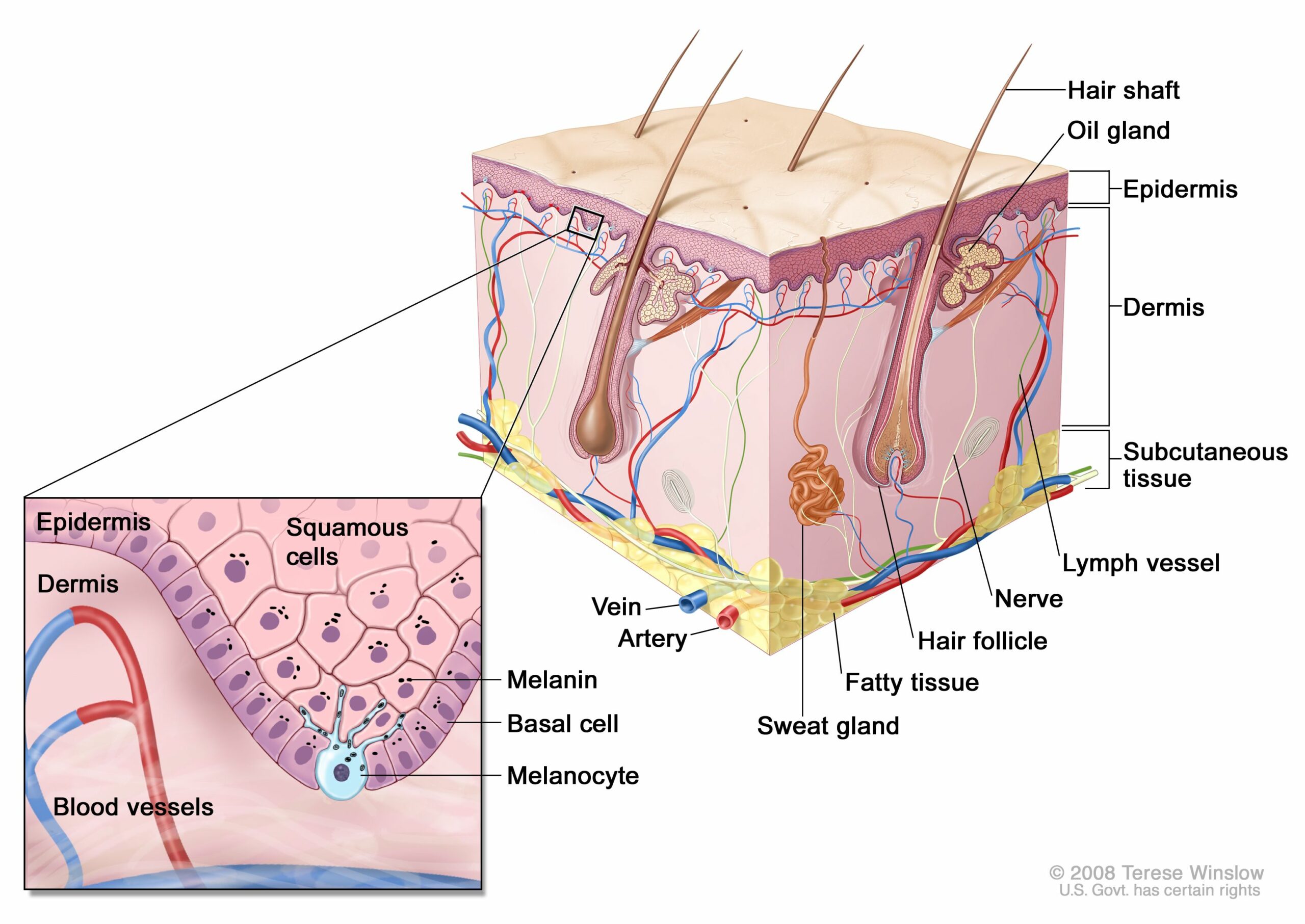
Diagram of melanocytes
- Adenocarcinomas: Adenocarcinomas start in glandular cells called adenomatous cells. Glandular cells produce fluids to keep tissues moist.
- Sarcoma
- Osteosarcoma: Sarcomas of bone start from bone cells.
-
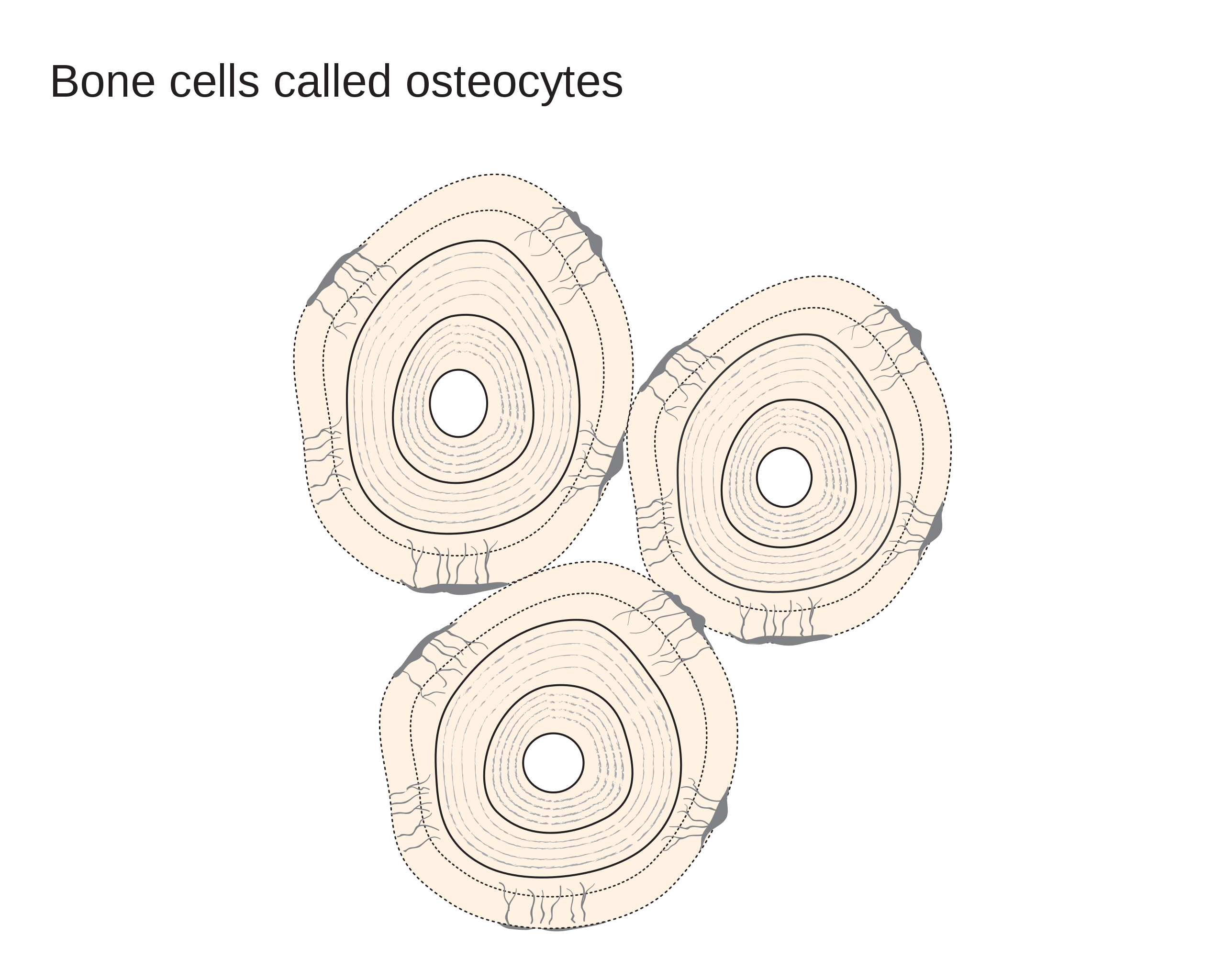
Diagram of osteocytes
-
- Rhabdomyosarcoma: Cancer of muscle cells is called rhabdomyosarcoma or leiomyosarcoma.
-
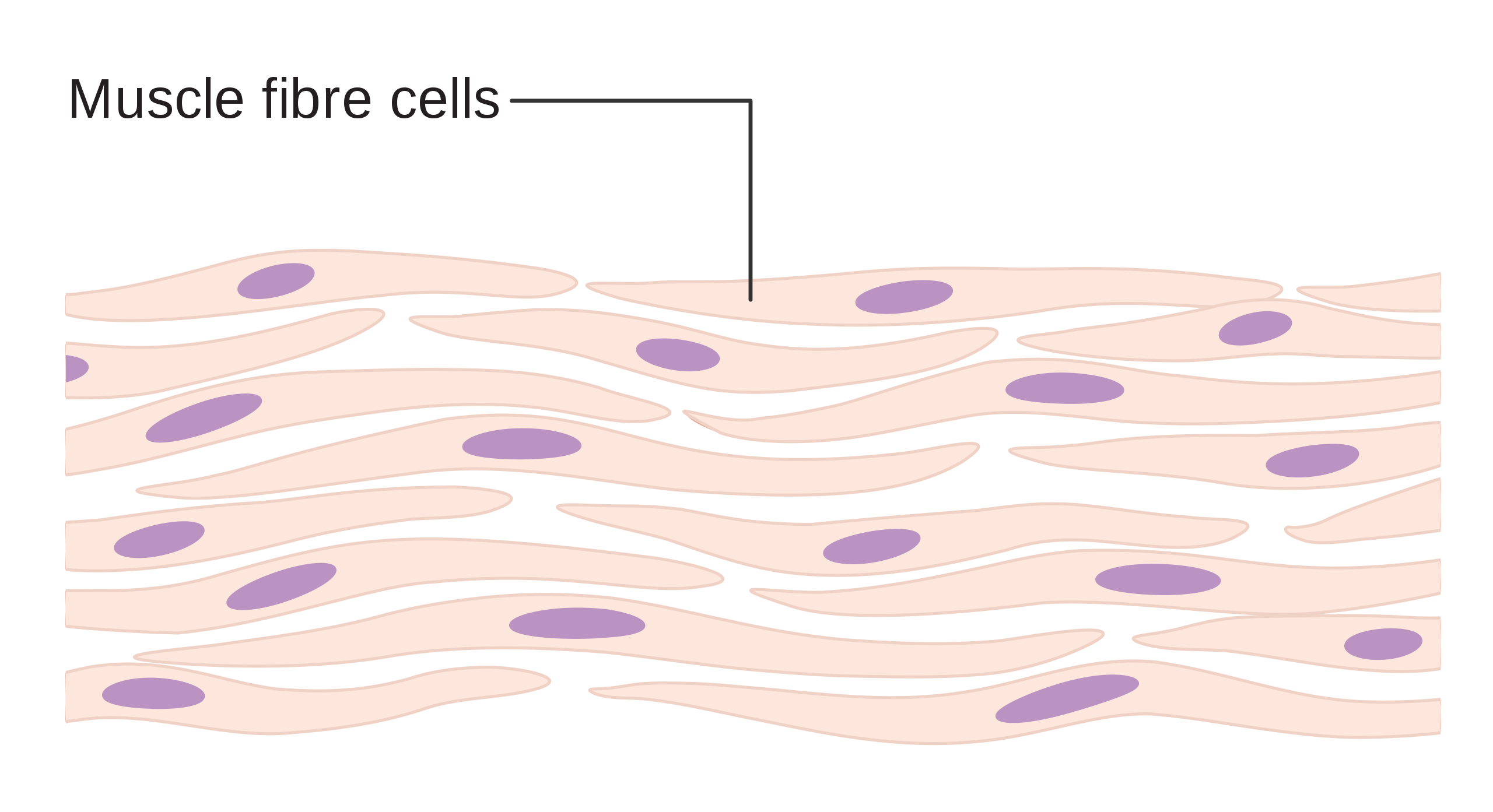
Diagram of muscle cells
-
- Chondrosarcoma: Cancer of the cartilage is called chondrosarcoma.
-

Diagram of cartilage cells called chondroblasts
-
- Osteosarcoma: Sarcomas of bone start from bone cells.
- Glioma: Cancers of neuroglialcells (e.g. astrocytoma, ependyoma)
- The brain and spinal cord form the central nervous system. The brain is made up of billions of nerve cells called neurones. It also contains special connective tissue cells called glial cells that support the nerve cells.The most common type of brain tumour develops from glial cells. It is called glioma. Some tumours that start in the brain or spinal cord are non cancerous (benign) and grow very slowly. Others are cancerous and tend to grow and spread.
-
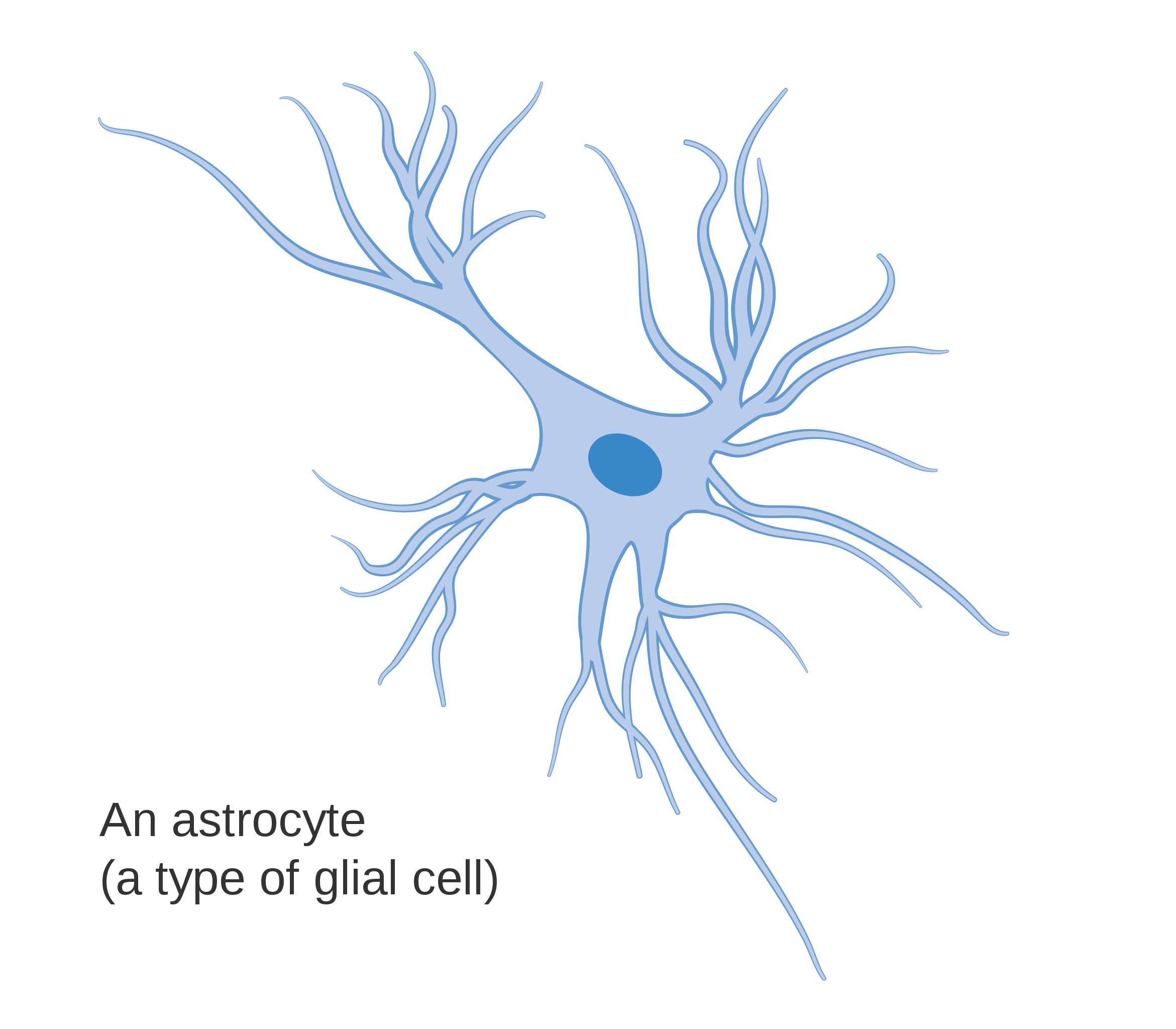
Diagram of an astrocyte
- Several malignant tumors have unique names: Hodgkin’s disease, Wilms’ tumor, Leukemia, Lymphoma
- Hodgkin’s disease: Hodgkin lymphoma is a type of blood cancer that affects white blood cells called lymphocytes. It is also called a cancer of the lymphatic system.
-
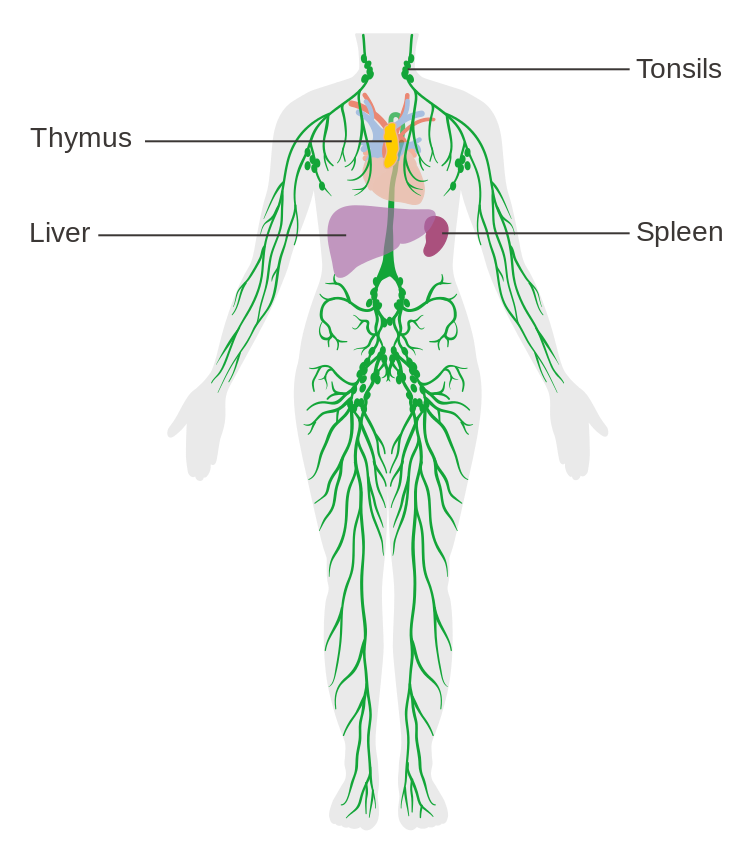
Diagram of the lymphatic system -
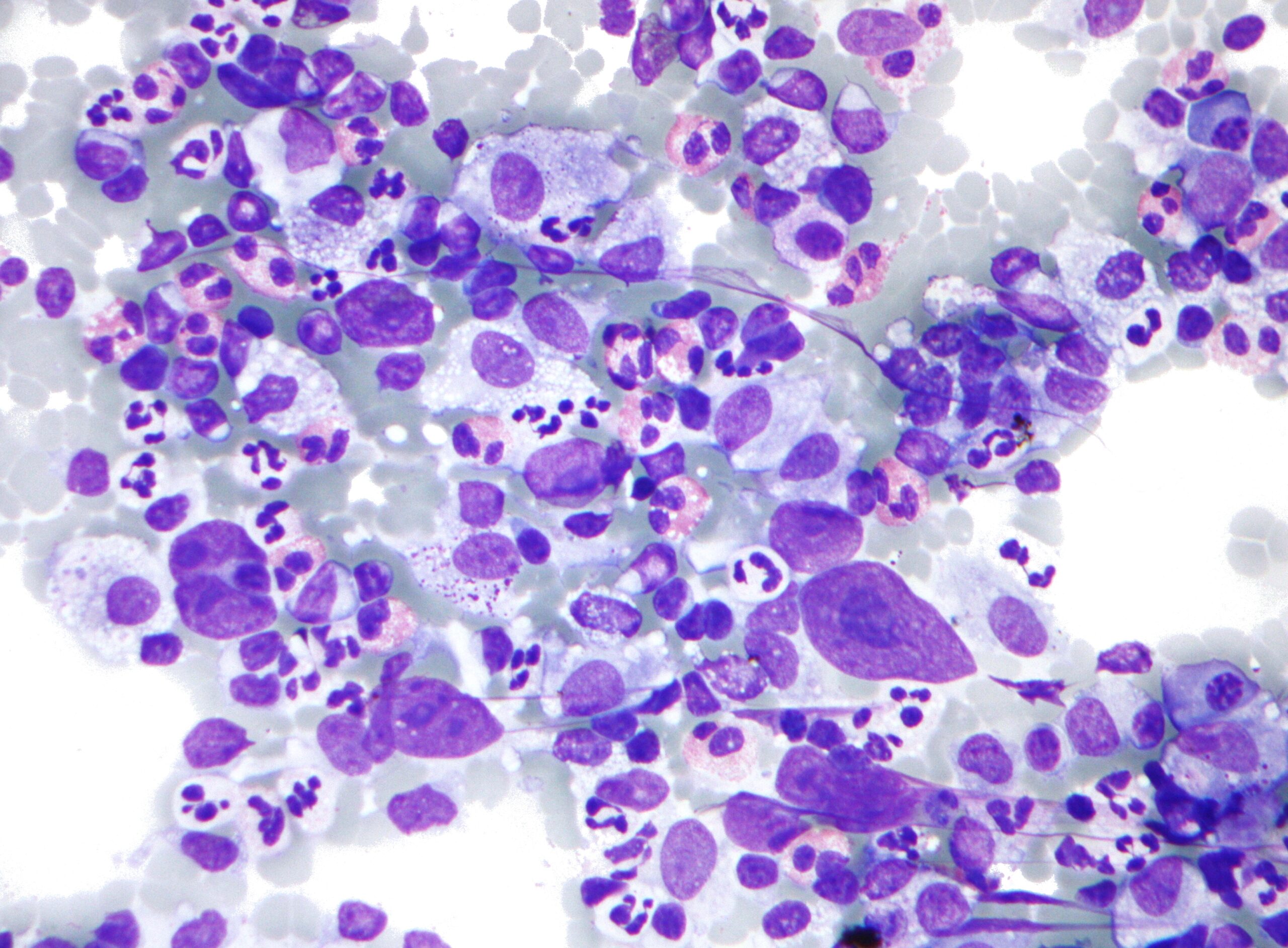
Micrograph of Hodgkin lymphoma, abbreviated HL. Lymph node FNA specimen. Field stain.
The micrograph shows a mixture of cells common in HL:
Eosinophils.
Reed-Sternberg cells.
Plasma cells.
Histocytes. -
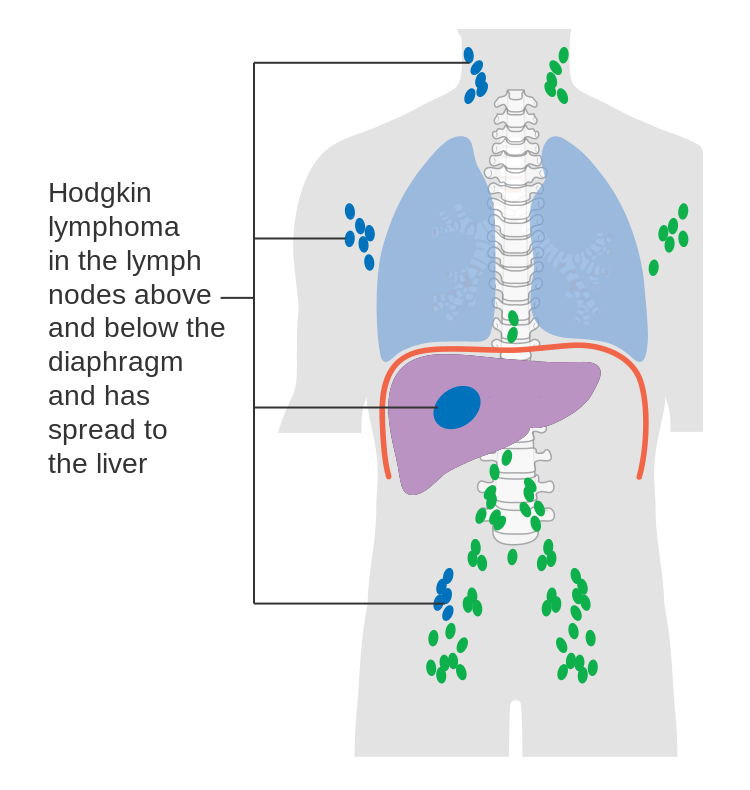
Diagram showing stage 4 Hodgkin’s lymphoma
-
- Wilms’ tumor: Wilms tumours are a type of kidney cancer that mainly affect children. Wilms tumours are also called nephroblastomas. They develop from cells called nephroblasts. Dr Max Wilms wrote the first medical paper about this condition. This is how it got its name.
-
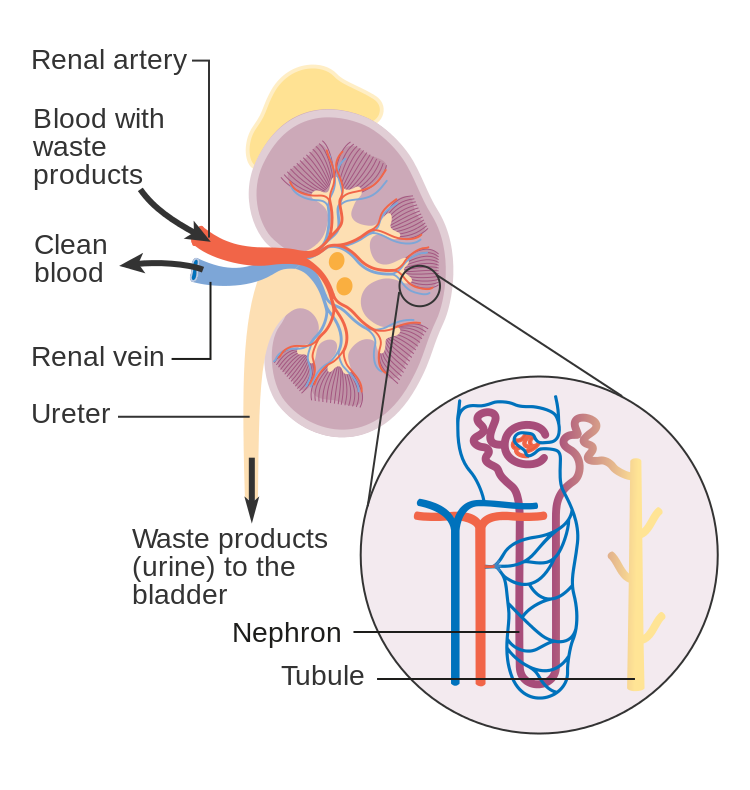
Diagram showing how the kidneys work
-
- Leukemia: Leukaemia is a type of blood cancer.
- Lymphoma: Lymphoma is a type of blood cancer that affects white blood cells called lymphocytes. There are 2 main types of lymphoma. These are called Hodgkin lymphoma and Non-Hodgkin lymphoma (NHL).
- Hodgkin’s disease: Hodgkin lymphoma is a type of blood cancer that affects white blood cells called lymphocytes. It is also called a cancer of the lymphatic system.
- Carcinoma
- Terms: Oncogenesis, carcinogenesis, tumorigenesis
-
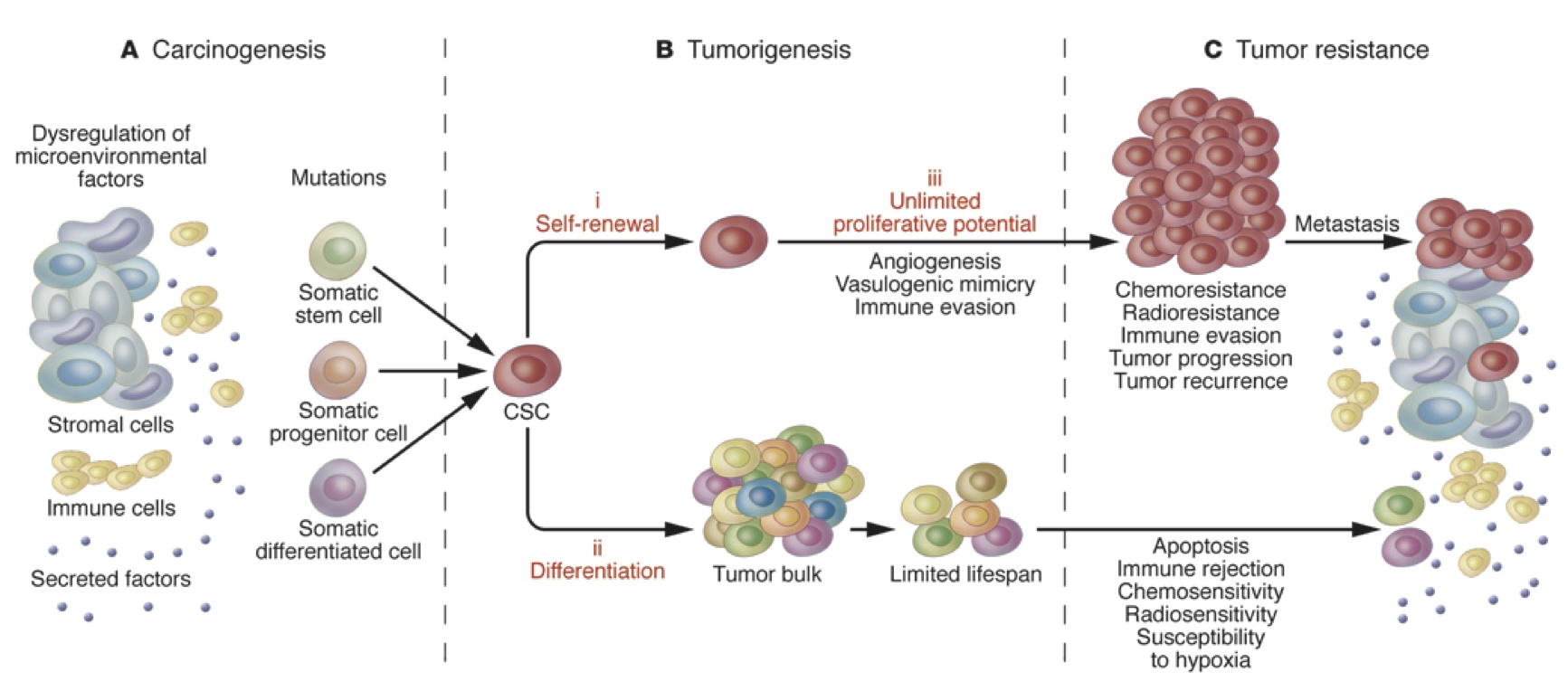
CSCs, carcinogenesis, tumorigenesis, and tumor resistance.(159) (Adapted with permission from American Society for Clinical Investigation).
-
- Metatstasis (lymphatic spread, hematogenous spread, peritoneal cavity spread)
- Lymphatic spread
-
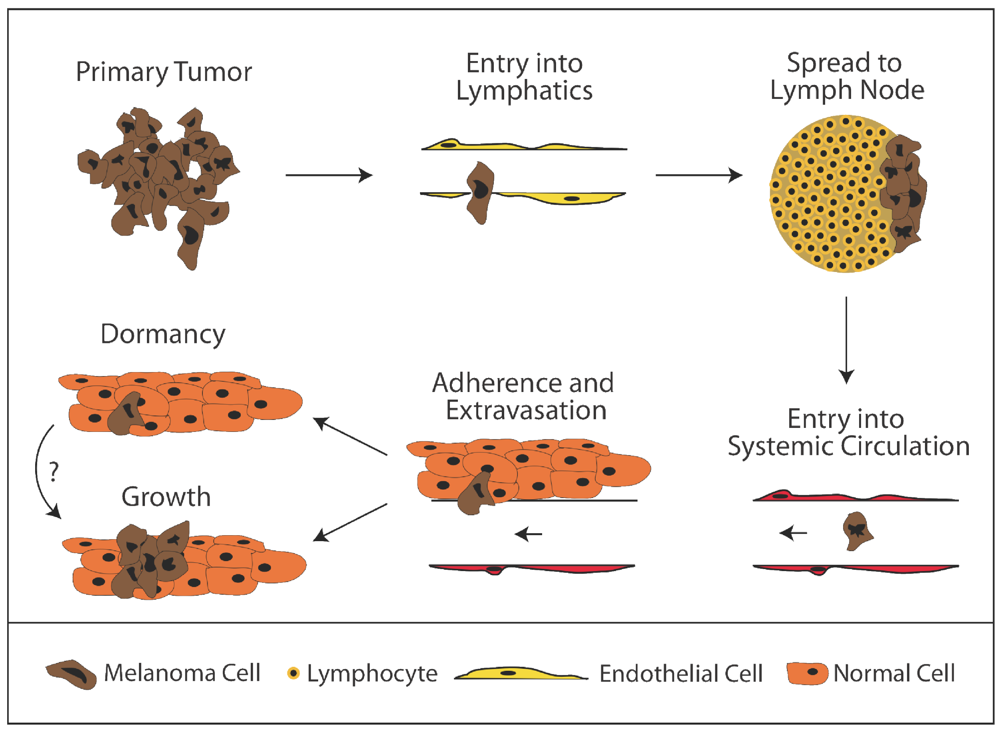
Example of lymphatic spread: Steps in Melanoma Metastasis. After formation of a primary tumor, melanoma cells are thought to enter into lymphatic vessels, traverse to the lymph node, and subsequently enter into systemic circulation via the thoracic duct. After reaching systemic circulation, cells must adhere to the microvasculature of a target organ, extravasate, and subsequently proliferate in order to form a clinically relevant metastasis. The mechanisms regulating either success or failure at any step are likely important and probably differ amongst different melanomas and different target organs.
-
- Hematogenous spread
-
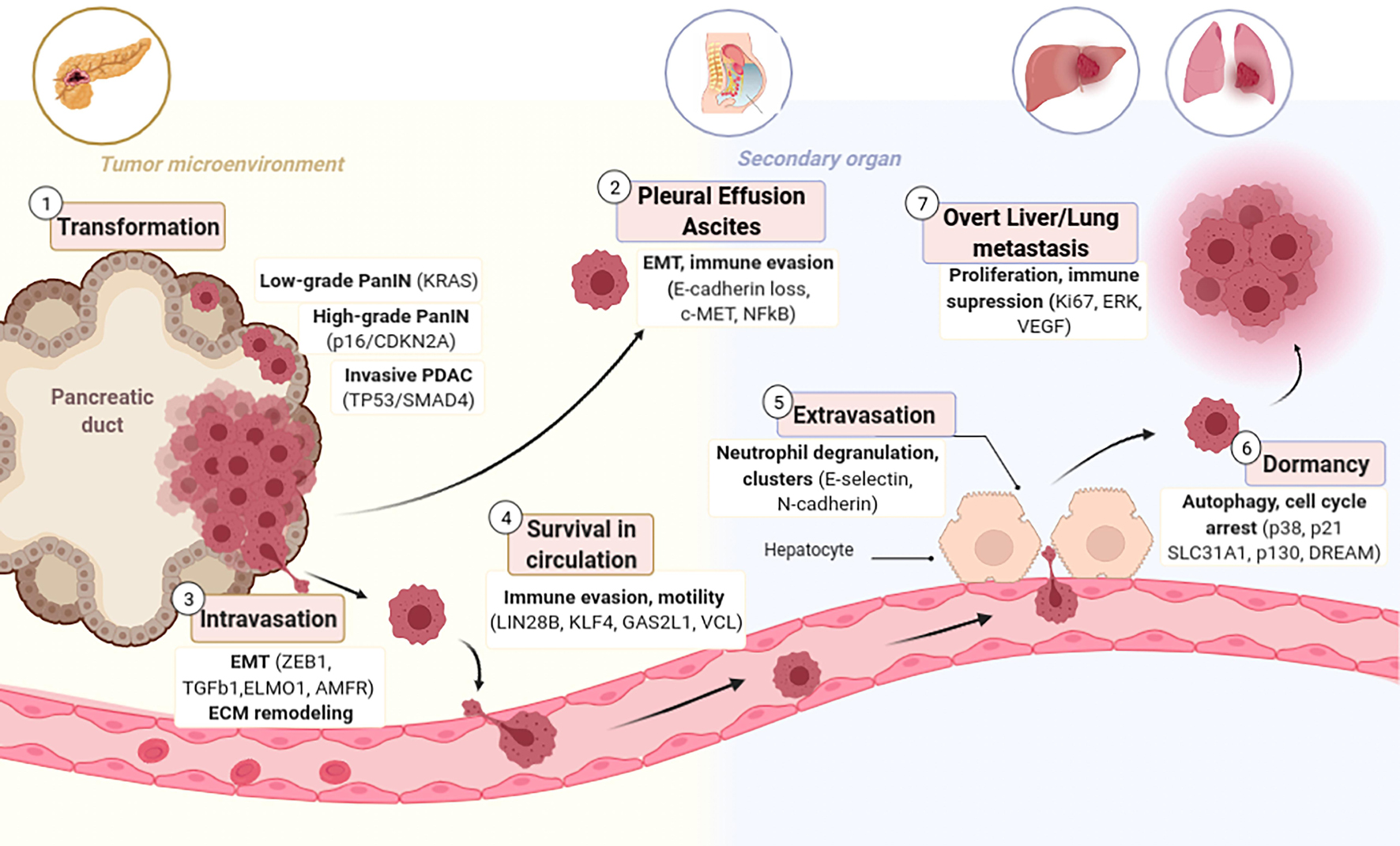
Stages of Metastatic Progression with candidate genes responsible per each stage. (1) Normal epithelial pancreatic ductal cells acquire an aggressive phenotype through serial mutations that transform them firstly to PanIN and lately to PDAC. (2) Transformed cells are capable of detaching and colonizing the Peritoneum forming Ascites or Pleural Effusion. (3) PDAC cells have enhanced motility due to EMT that allows them to invade blood or lymphatic vessels. (4) CTCs in circulation are abundant, but only few survive this pressure. (5) Several CTCs have tropism for the pre-metastatic niche (PMN) and are able to extravasate to a secondary organ where they might remain dormant (6) for several years and eventually relapse and form overt metastasis (7). -
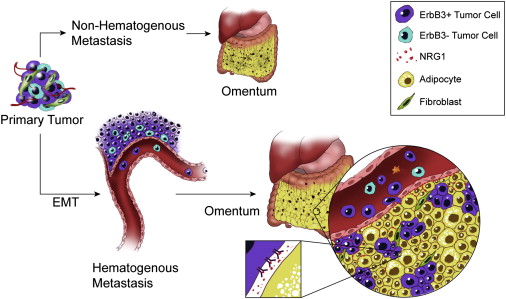
Example of hematogenous metastasis: Model of Ovarian Cancer Metastasis to Omentum:
(Top) Schematic representation of nonhematogenous metastasis to the omentum. Traditionally, epithelial ovarian cancer is thought to metastasize via direct surface spread.
(Bottom) Our results point to an alternative pathway that also involves hematogenous metastasis with strong tropism toward the omentum.
-
- peritoneal cavity spread
-
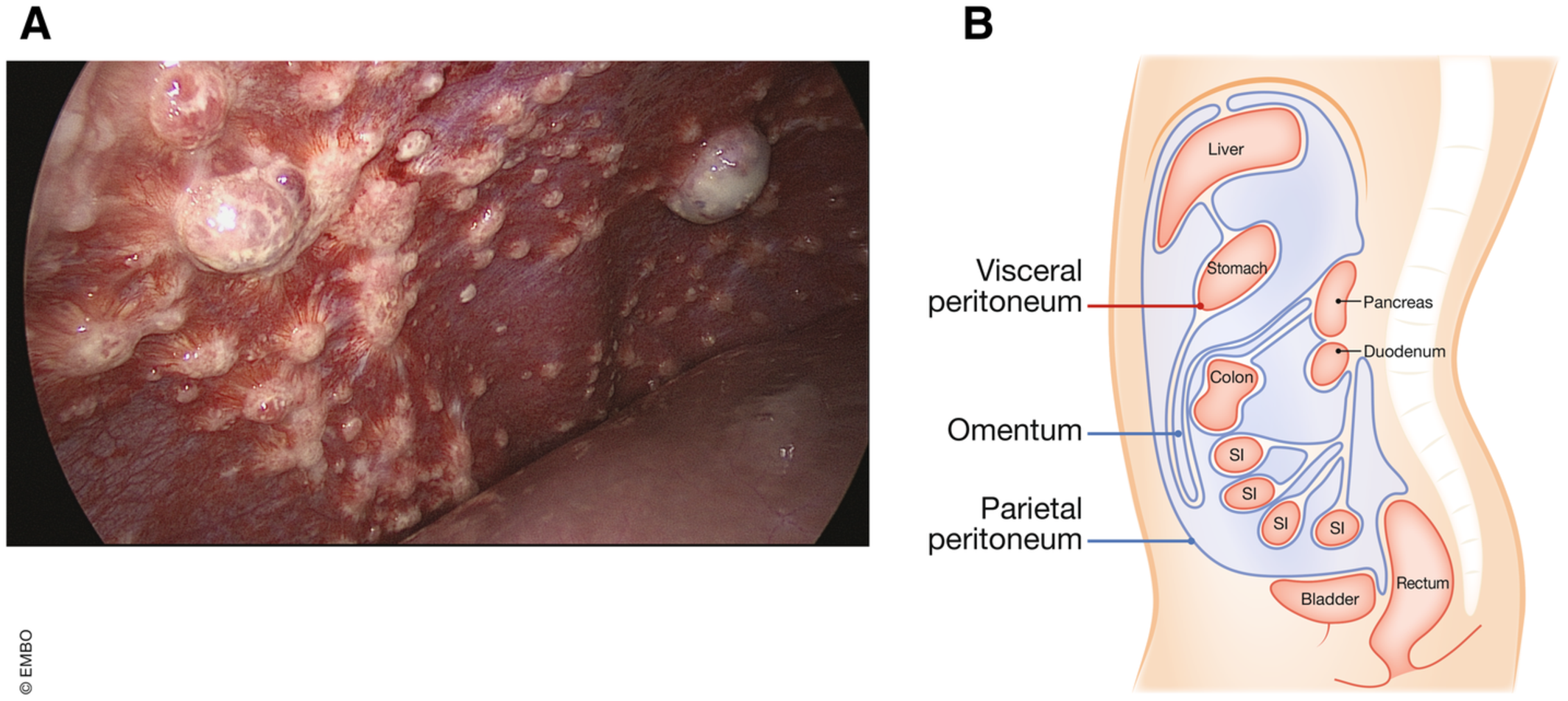
Anatomy of peritoneal metastases: (A) Diaphragmatic peritoneal metastases originating from colorectal cancer imaged during diagnostic laparoscopy. Scale approximately 1:2. Image courtesy of I. de Hingh. (B) Sagittal view of the abdominal cavity. The abdominopelvic wall and diaphragm are lined by the parietal peritoneum, whereas the visceral peritoneum lines the organs. The omentum is the largest peritoneal fold. SI, small intestine. -
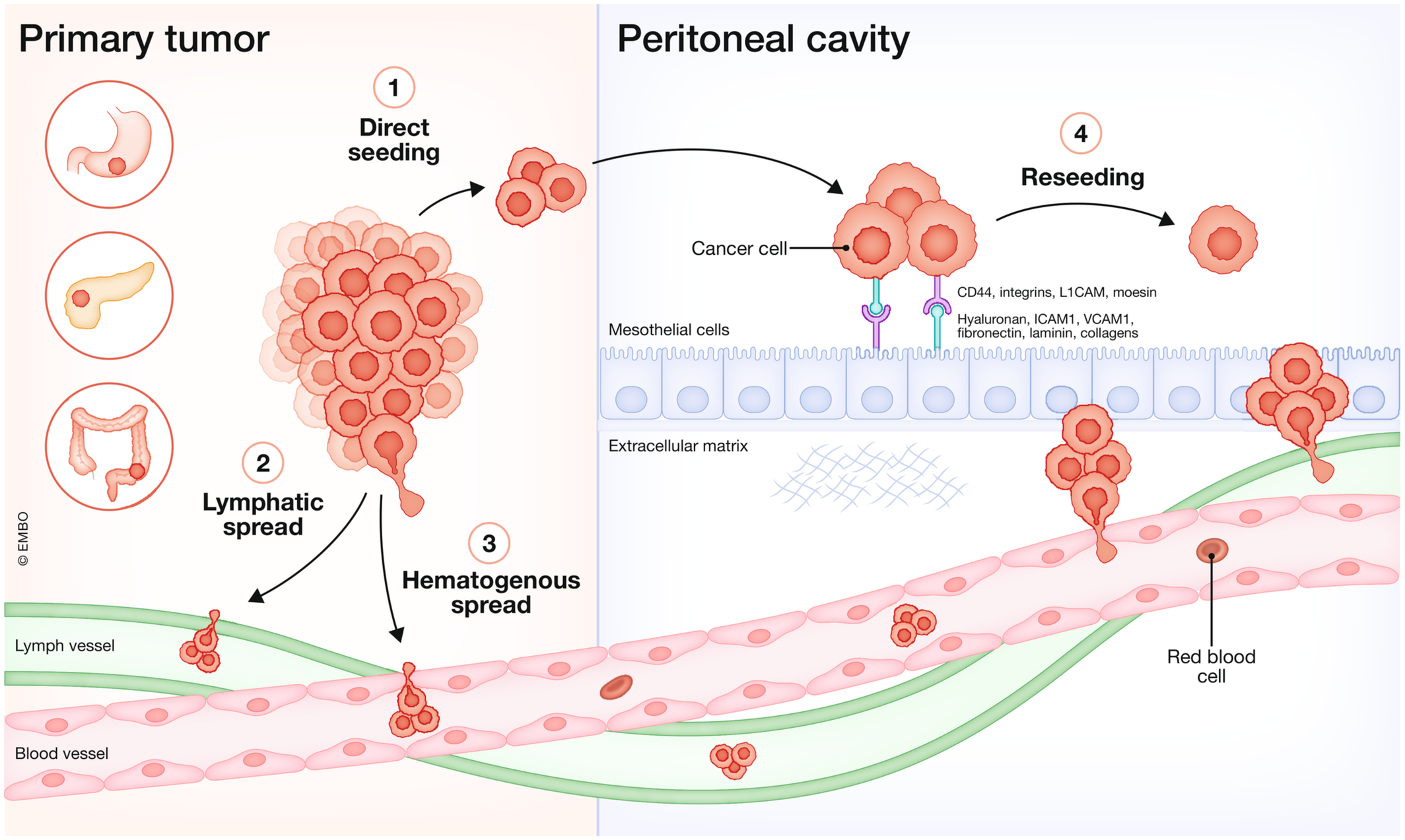
Cancer cell spread from the primary tumor to the peritoneum can occur via different routes: (1) direct seeding from the primary tumor into the peritoneal cavity, (2) via the lymphatic system, (3) via the hematogenous system, and (4) reseeding from existing PM lesions. Cancer cells interact with mesothelial cells via adhesion molecules. Created with BioRender.com. -
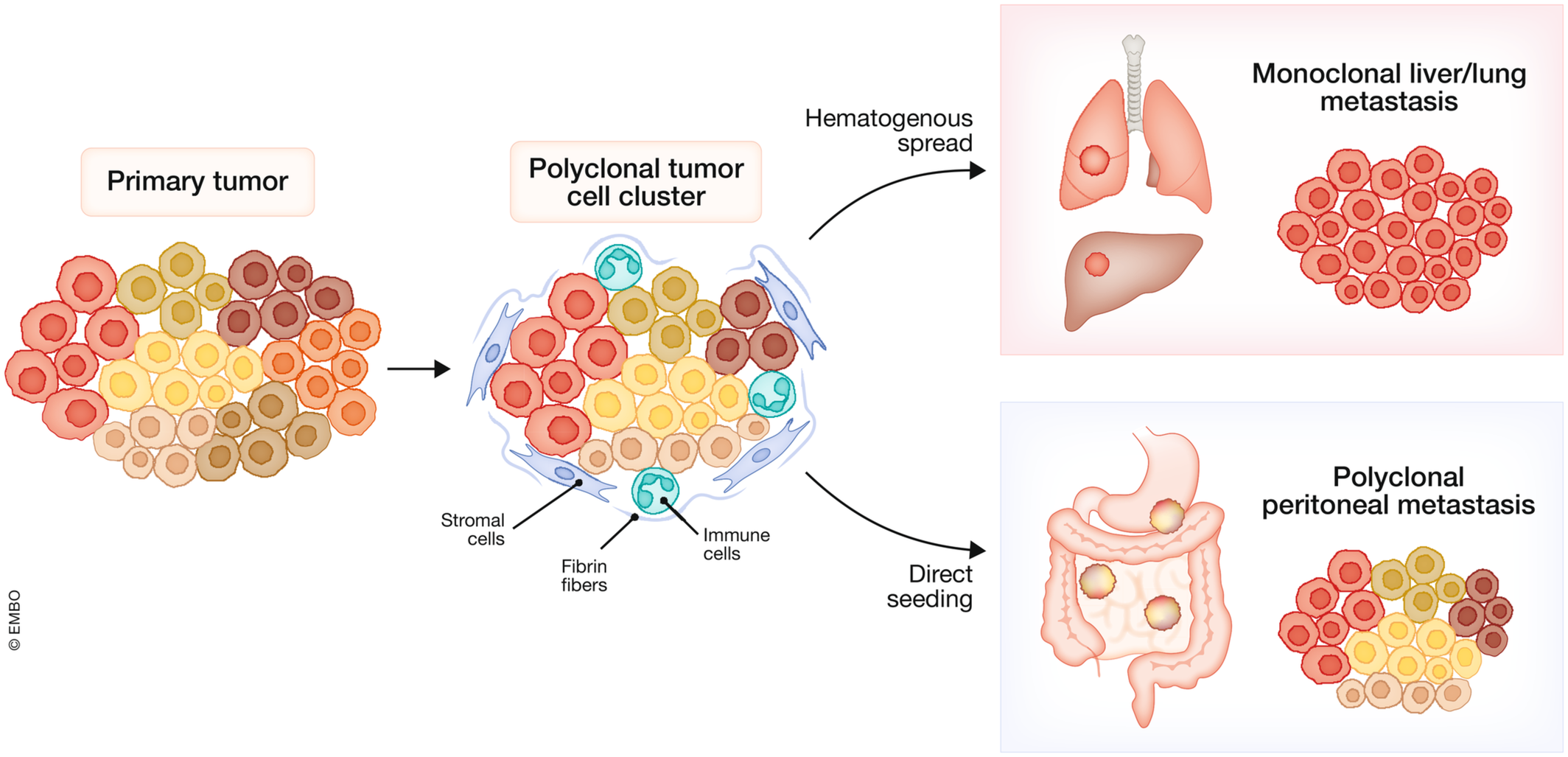
Polyclonal seeding and outgrowth of peritoneal metastases: Polyclonal cancer cell clusters shed from the primary tumor into the peritoneal cavity, bloodstream or lymphatic system, where they can interact with immune and stromal cells. The clonal heterogeneity of the primary tumor is retained in peritoneal metastases, while clonal selection leads to monoclonal outgrowth of lung and liver metastases.
-
- Lymphatic spread
- Why does cancer kill people? Mass compresses blood vessels, causes ischemia/hypoxia, resulting in necrosis and therefore inflammation, tumor can secrete proteolytic enzymes (e.g. collagenase) or hormones; loss of normal cells, replaced by cancerous cells,
-
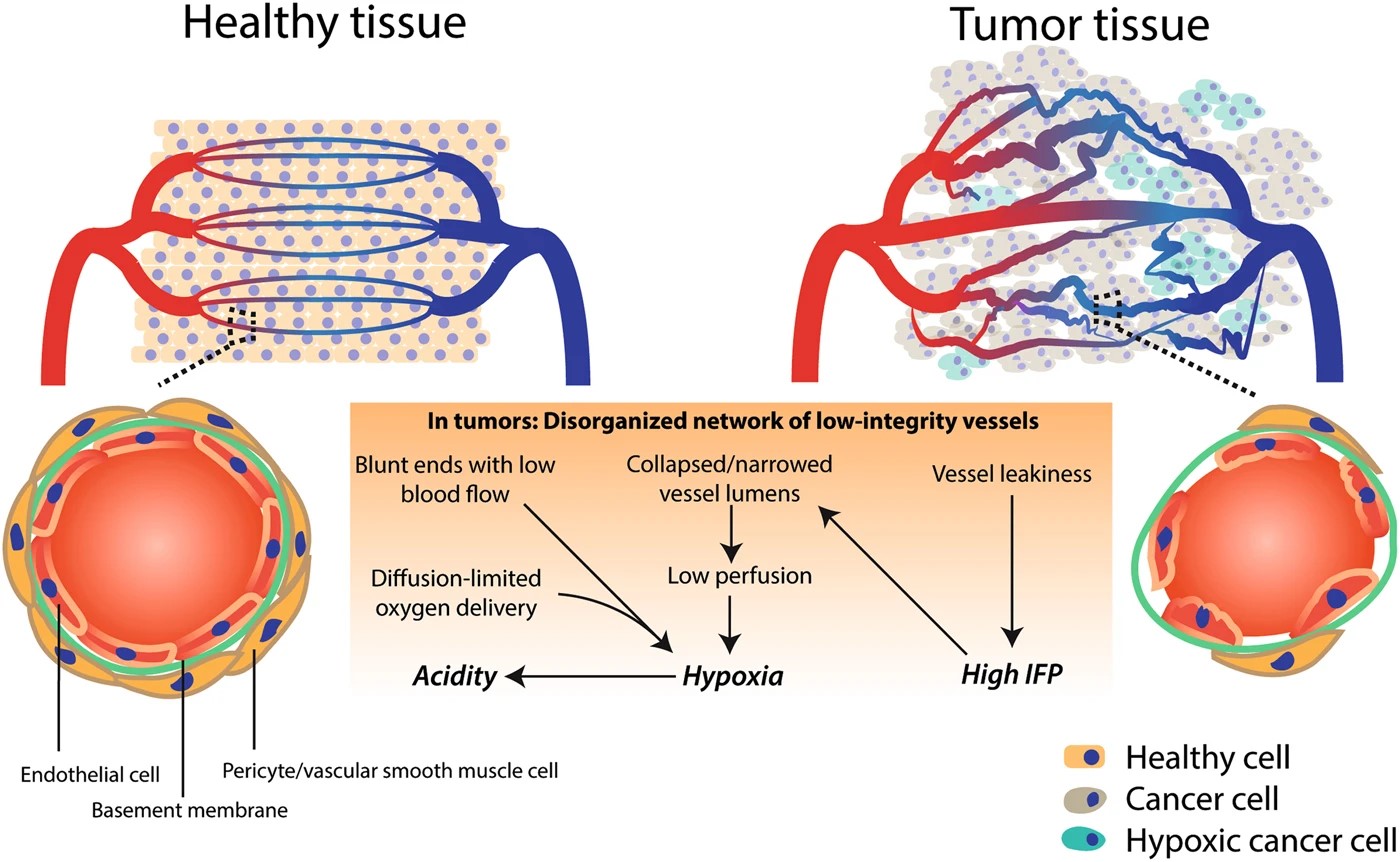
Tumor-associated blood vasculature is a major influencer of the tumor microenvironment (TME): (Upper left panel) A well-organized vessel network ensures full-covering of nutrient supply. (Lower left panel) These vessels are matured with an endothelial cell layer surrounded by a basement membrane and pericytes (like smooth muscle cells). The endothelial layer is characterized by tight intercellular junctions. Oppositely, due to high pro-angiogenic signaling, the network of tumor-associated blood vessels (upper right panel) is chaotic, low in pericyte coverage and has loose inter-endothelial cell junctions (lower right panel). This generates leaky vessels that increases interstitial fluid (IFP) pressure. Common blunt-ended or collapsed vessels results in tumor regions that are starved from nutrients including oxygen (hypoxic cells indicated in green). Moreover, the glycolytic nature of the (hypoxic) tumor cell acidifies the pH in the TME -
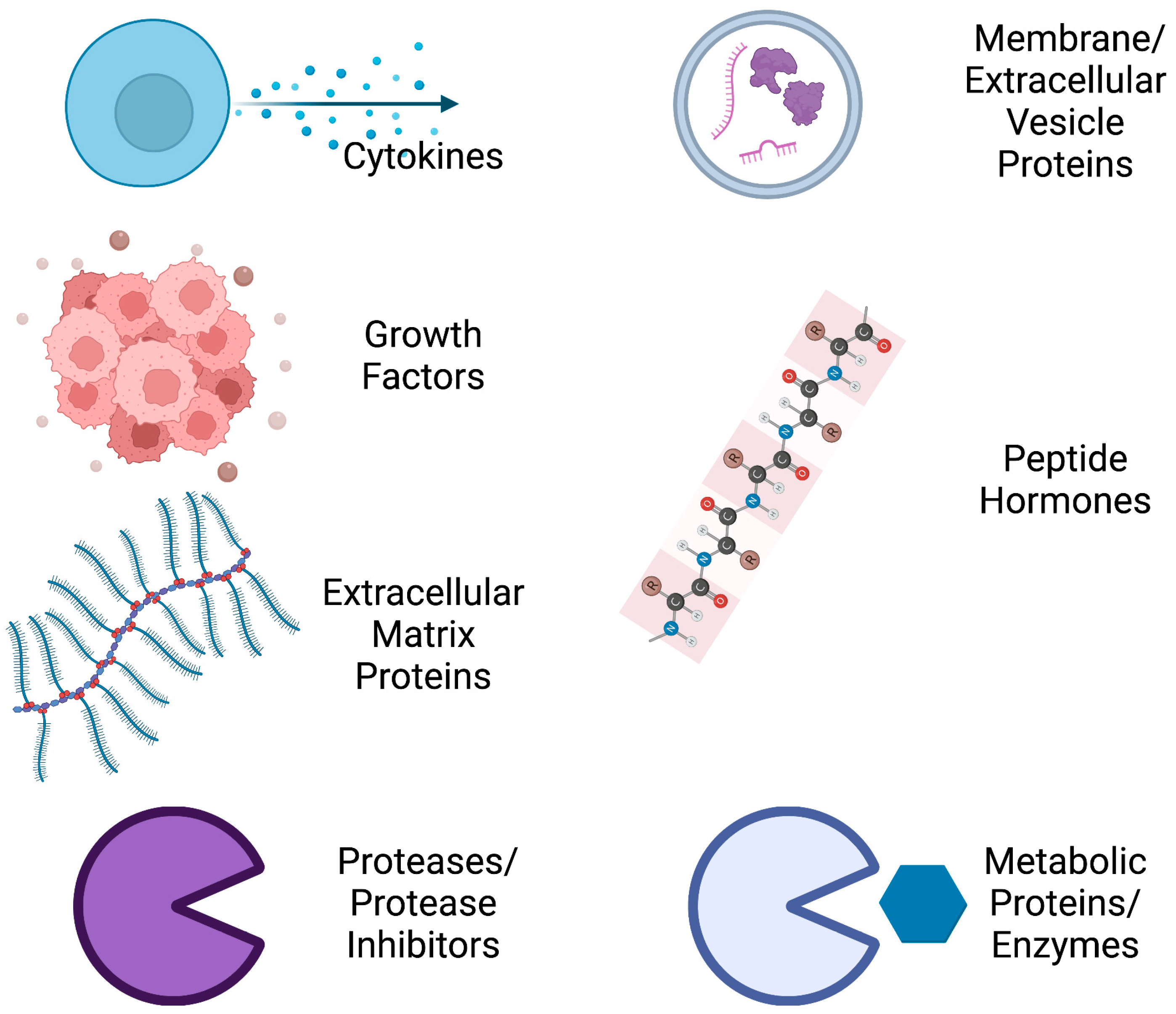
Proteins of the TNBC secretome. A large variety of functional proteins are secreted from (triple-negative breast cancer) TNBC cells and tumors -
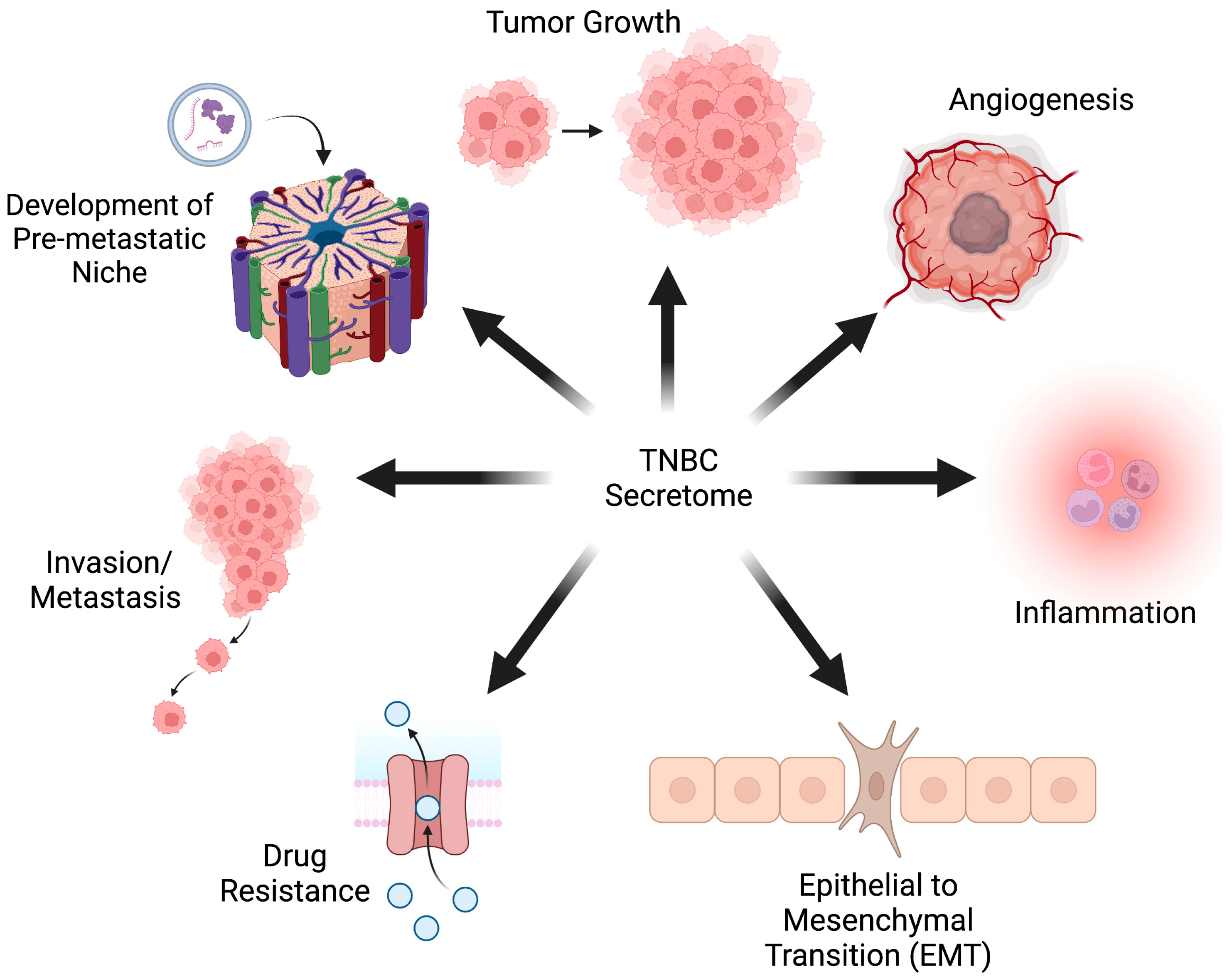
Effects of the TNBC secretome. Protein factors secreted by TNBC cells and tumors regulate cancer-promoting processes -
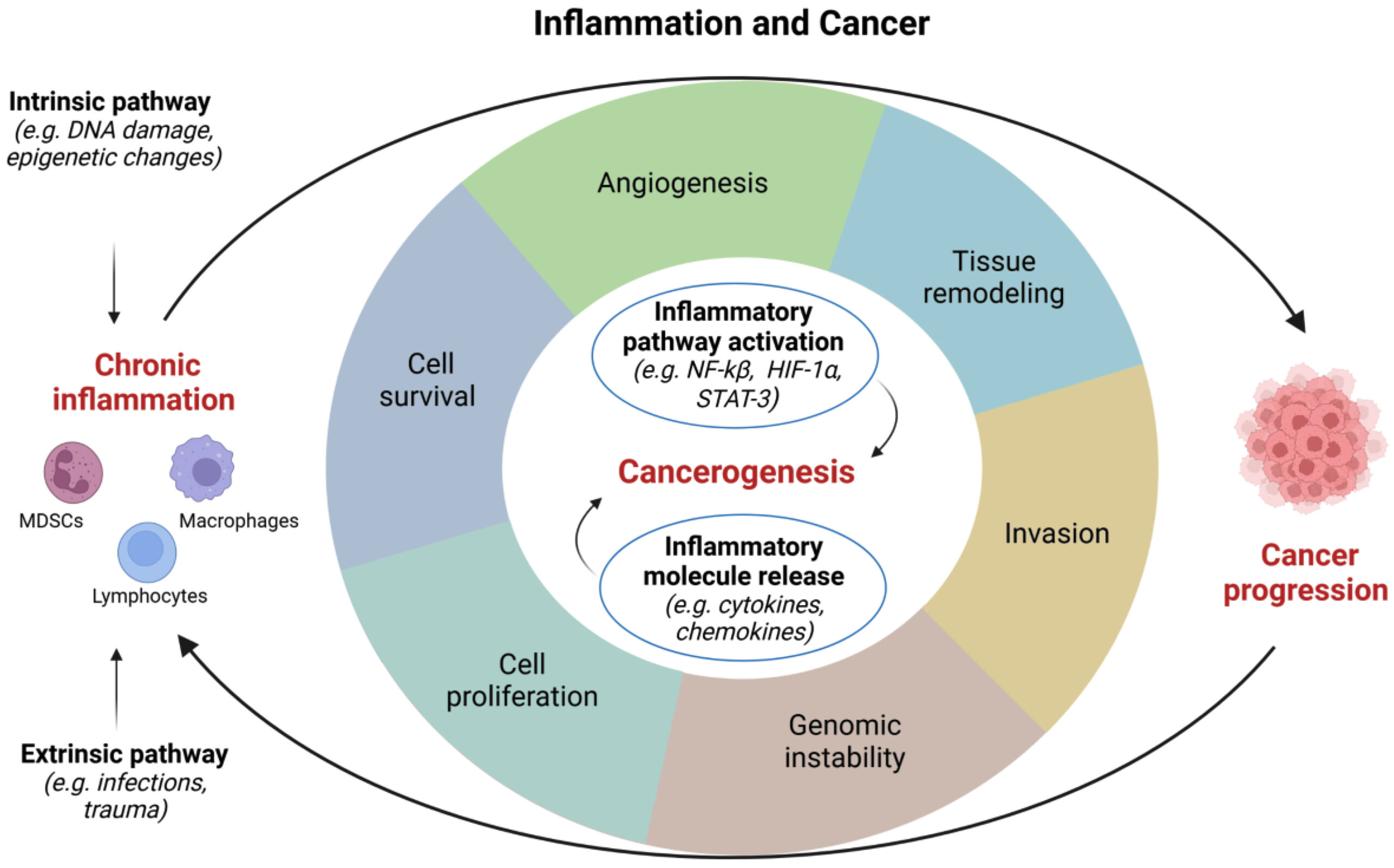
Correlations between inflammation and cancer. HIF, hypoxia inducible factor; NF, nuclear factor; STAT, signal transducer and activator of transcription. Image created with BioRender.com (accessed on 1 December 2022). -

The diagram displays the responses to reduced oxygenation within the tumor microenvironment. Hypoxia promotes tumor invasion, metastasis and resistance through several ways. a Hypoxia induces detachment of tumor cells by weakening the connections between cells and their extracellular matrix supporting them, and promotes dissemination of tumor cells to the various organs of the body. Thereby hypoxia triggers the metastatic spread of tumor. b Hypoxia stimulates angiogenesis, and provides more opportunity for detached tumor cell to inter into the circulation and migrate via the newly formed vessels. Thereby hypoxia enhances invasive and metastatic spread of solid tumors to another region. c Hypoxia induces EMT, in which tumor cells detach, lose the epithelial feature, acquire a mesenchymal phenotype and display the stemness properties including loss of differentiation, tumorigenesis and aggressiveness. EMT extensively contributes to promoting of tumor cell invasion and migration. d Hypoxia up-regulates CAFs that produce the excessive altered ECM, which supports tumor growth and metastasis. e Tumor hypoxia promotes secretion of cytokines and chemokines that recruit pro-tumor immune cell and suppress anti-tumor response of various types of immune cells. f In response to hypoxia, tumor cells exploit a number of mechanisms including, extrusion of cytotoxic drug by ABC-transporters, exhibiting quiescent state, acquiring metabolic adaptations and displaying stemness features, which can contribute in chemo-, radio- therapy failure. g Hypoxia acts as a niche condition, to accumulate the CSCs enhancing tumorigenesis and resistance. EMT epithelial to mesenchymal transition, CAF cancer-associated fibroblast, ECM extracellular matrix, MDSCs myeloid-derived suppressor cells, TAM tumor-associated macrophage, TAN tumor-associated neutrophil, Treg regulatory T lymphocyte, NK cell natural killer cell, CSC cancer stem cell -
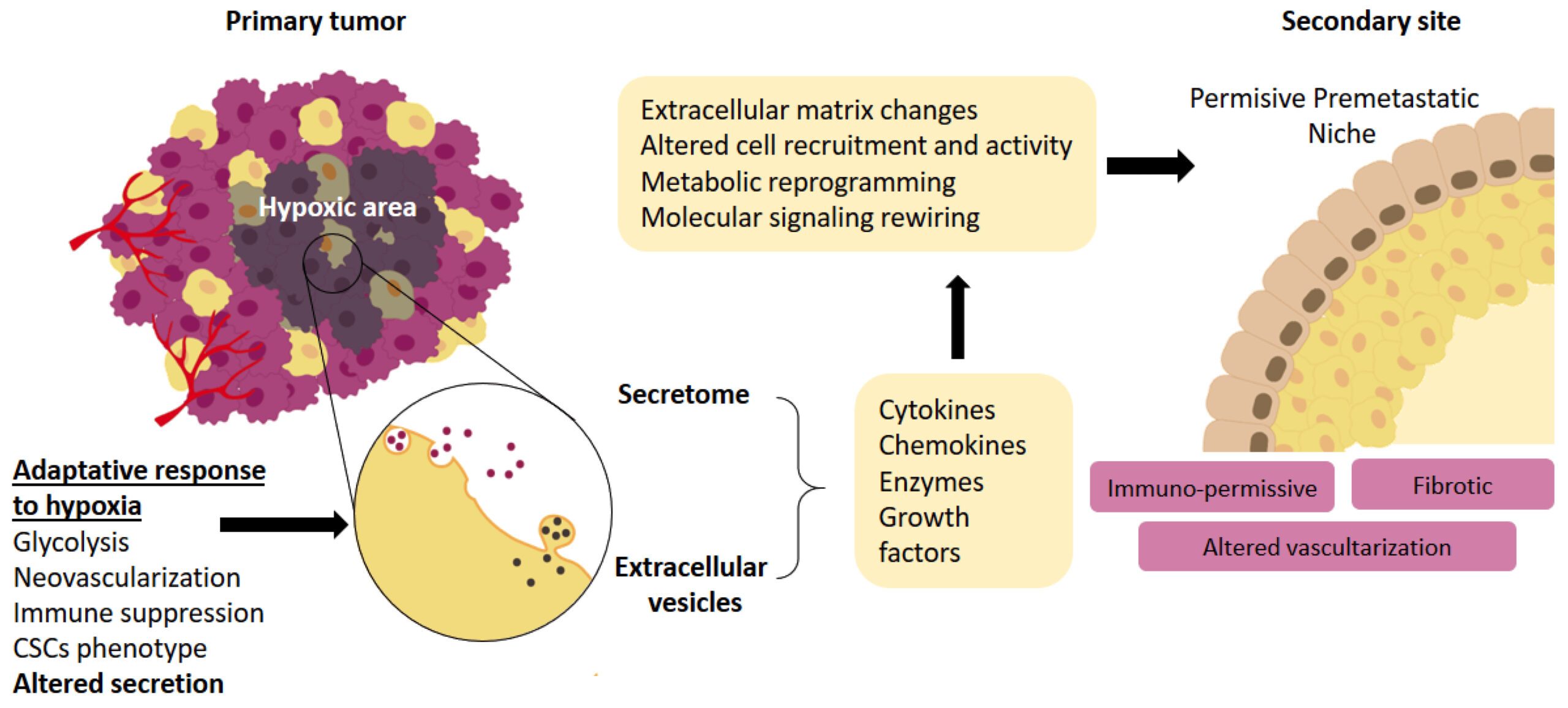
Schematic summary. As part of the adaptative response to hypoxic conditions, both tumoral and stromal cells alter the secretion of free molecules and extracellular vesicles, which upon arrival at the secondary site promote a series of changes that result in a permissive premetastatic niche.
-
- Signs and symptoms; pain, bleeding, lumps, obstructions, fatigue, immunosuppresion, anemia, weight loss, cachexia, paraneoplastic syndrome
-
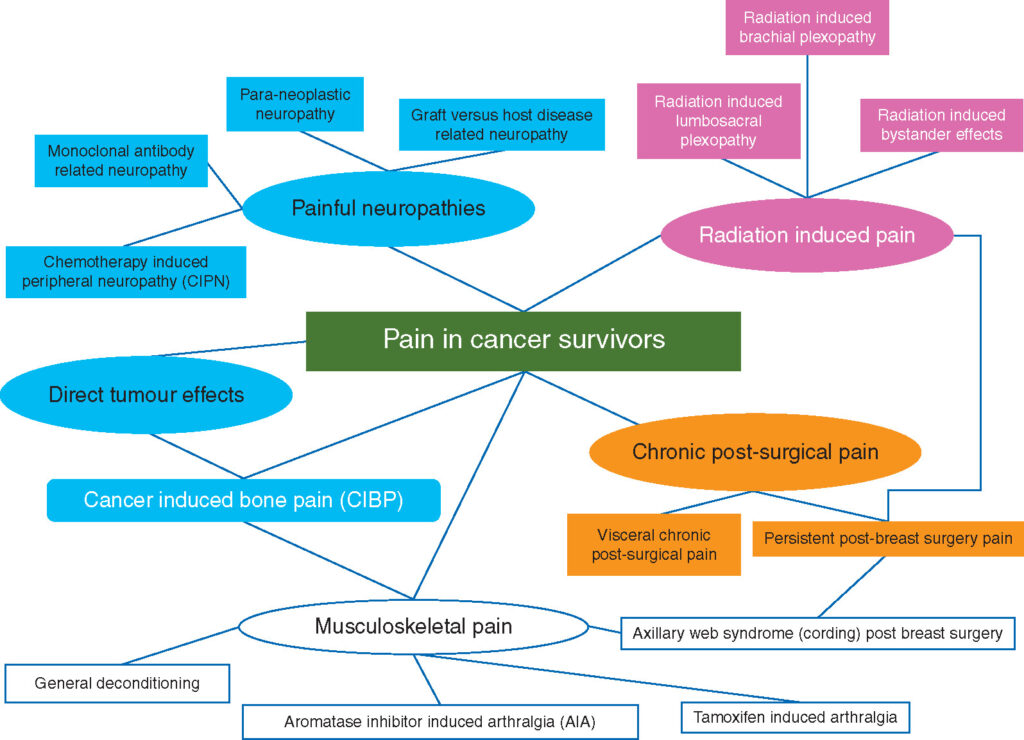
An outline of the different causes of pain in patients surviving cancer, related both to the disease itself, and the oncological treatment. -
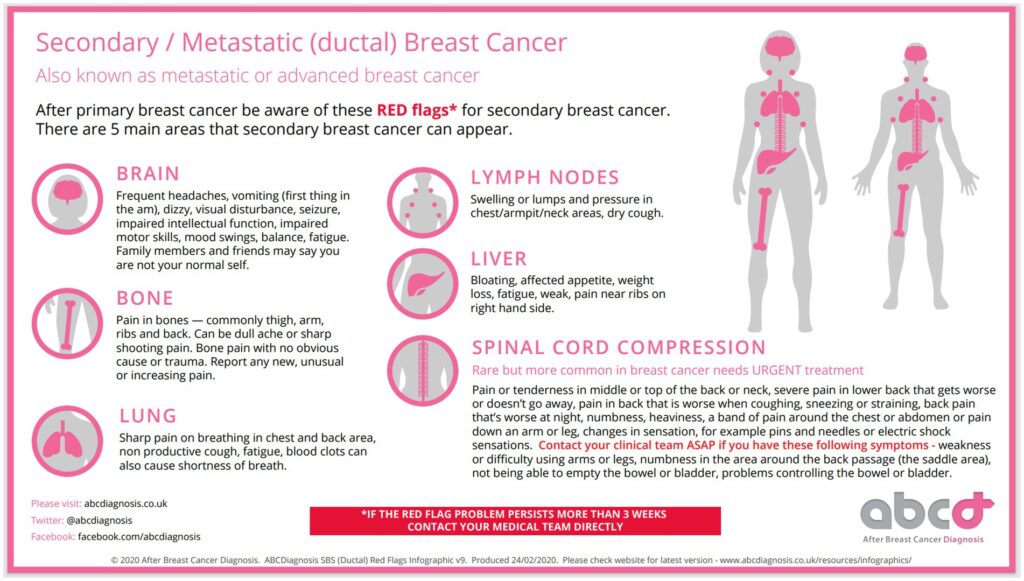
Signs of breast cancer include pains -
Breast cancer signs including lumps. - `
-
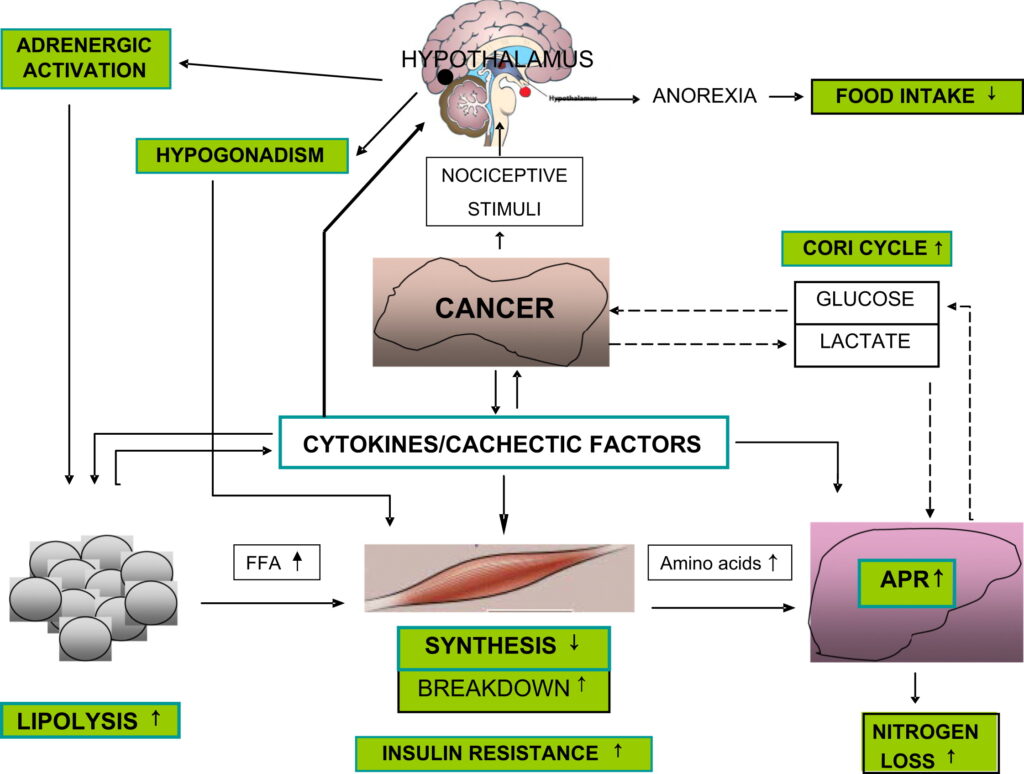
Integrative Physiology of Cancer Cachexia: The tumor is associated with activation of proinflammatory and neuroendocrine responses. These result in reduced food intake and metabolic change. Adrenergic activation and tumor-related lipolytic factors lead to enhanced lipolysis. The effects of hypogonadism, insulin resistance, adrenergic activation, and systemic inflammation coupled with semistarvation lead to muscle atrophy. Liver export protein synthesis is stimulated as part of the acute phase response. In addition, futile substrate cycles (such as the Cori cycle) contribute to hypermetabolism. -
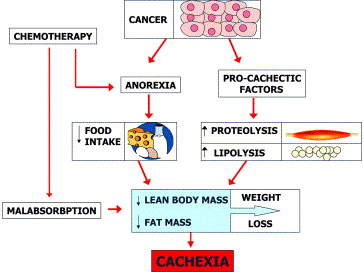
The pathogenesis of cancer cachexia is multifactorial, and includes reduced food intake, alterations in energy and substrate metabolism in the host and accelerated fat and muscle loss. - ·
-
- Diagnostic Tests – give examples of routine screening, self-examination, blood tests & tumor markers, genetic tests, imaging, cytological tests/biopsies,
-
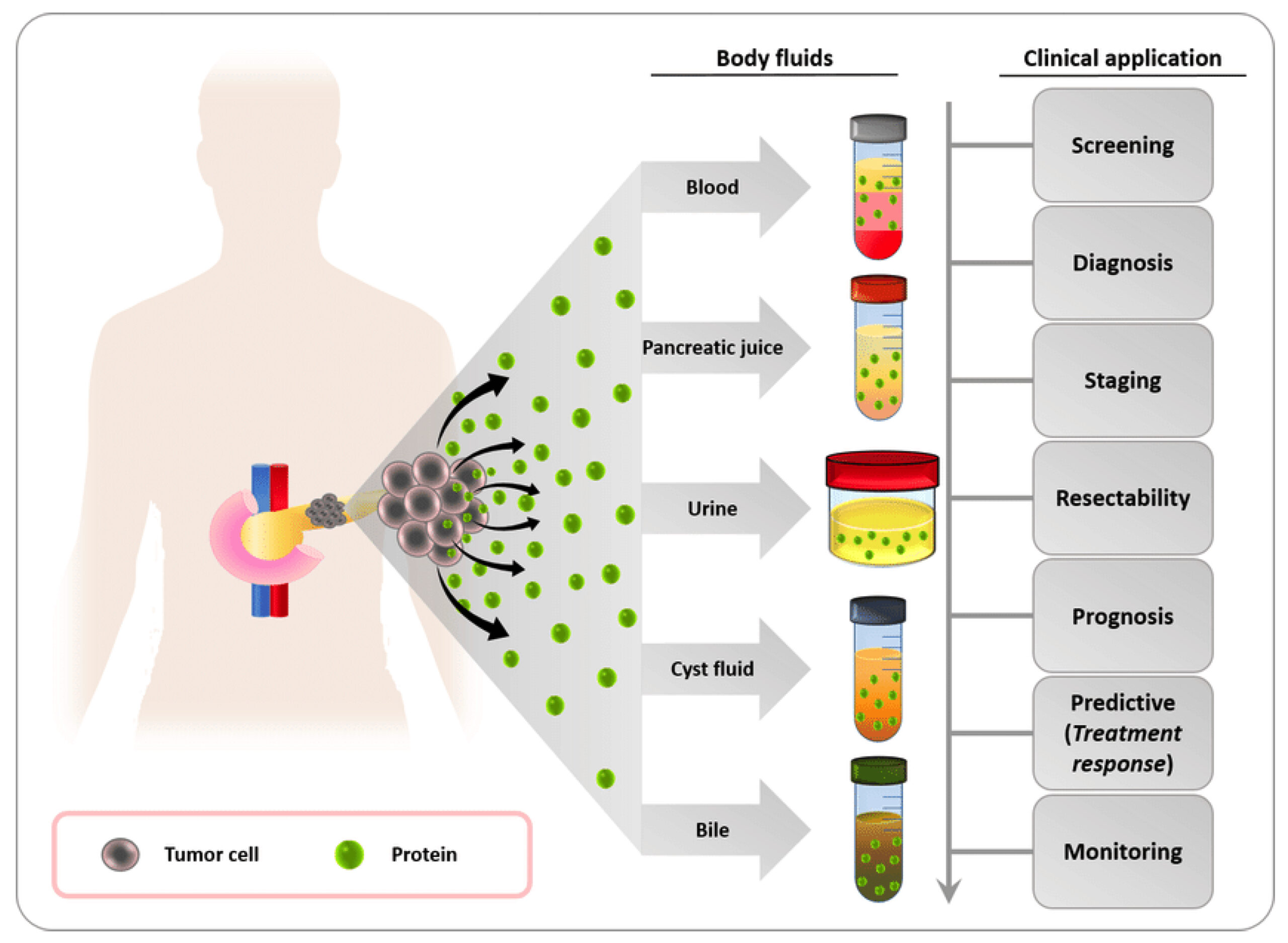
Identification of possible protein biomarkers for pancreatic cancer using bodily fluids. Bodily fluids that include cancer-derived proteins include bile, blood, pancreatic juice, urine, and pancreatic cyst fluid. For the management of pancreatic cancer patients, these proteins have a high potential as tumor biomarkers and a variety of clinical applications, including screening in high-risk populations for pancreatic cancer, early diagnosis, disease staging, the evaluation of tumor resection and prognosis, the prediction of therapy response to inform treatment decisions, and real-time patient monitoring. -

Commonly used non-invasive techniques for examining biomarkers in solid tumors. -

(A) A visual representation of the numerous imaging methods that can be used to diagnose breast cancer. (B) New targeted medicines approved by the FDA for the treatment of molecular subtypes of breast cancer - `
- `
-
- Grading and Scaling Cancers
-
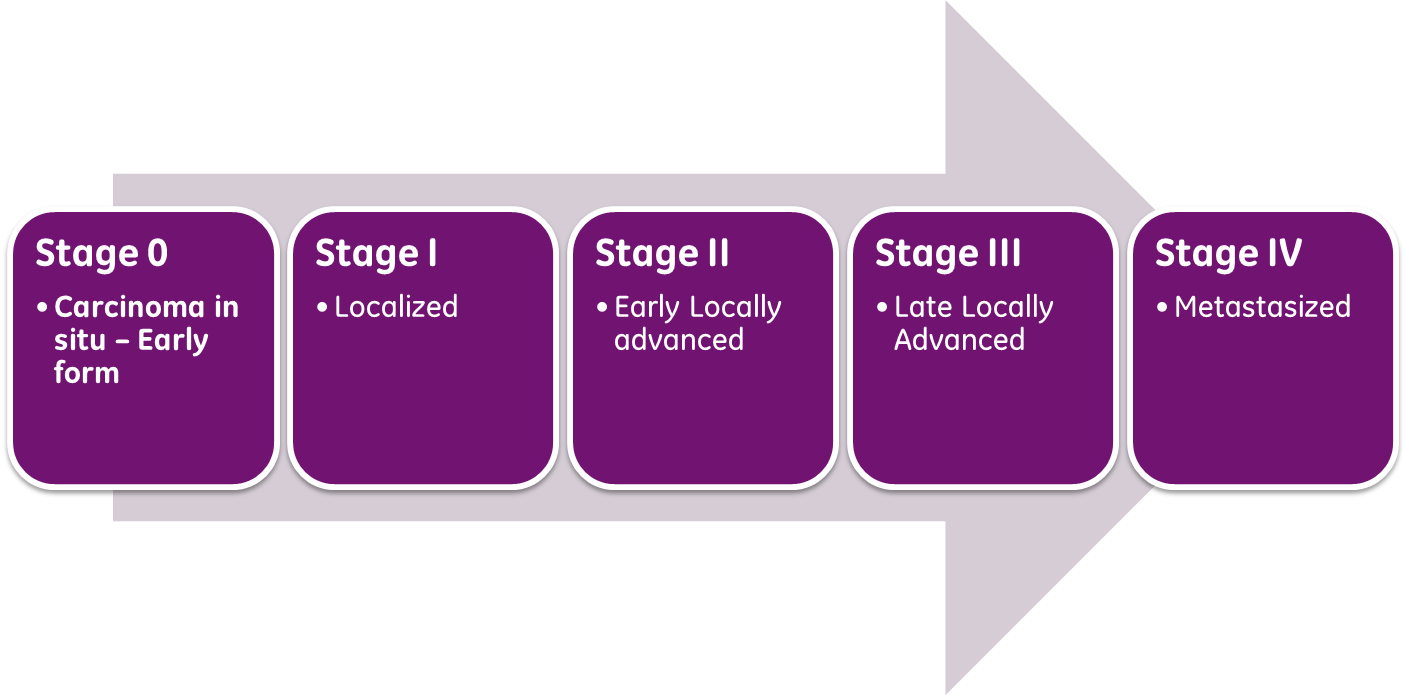
Stages of Cancer -
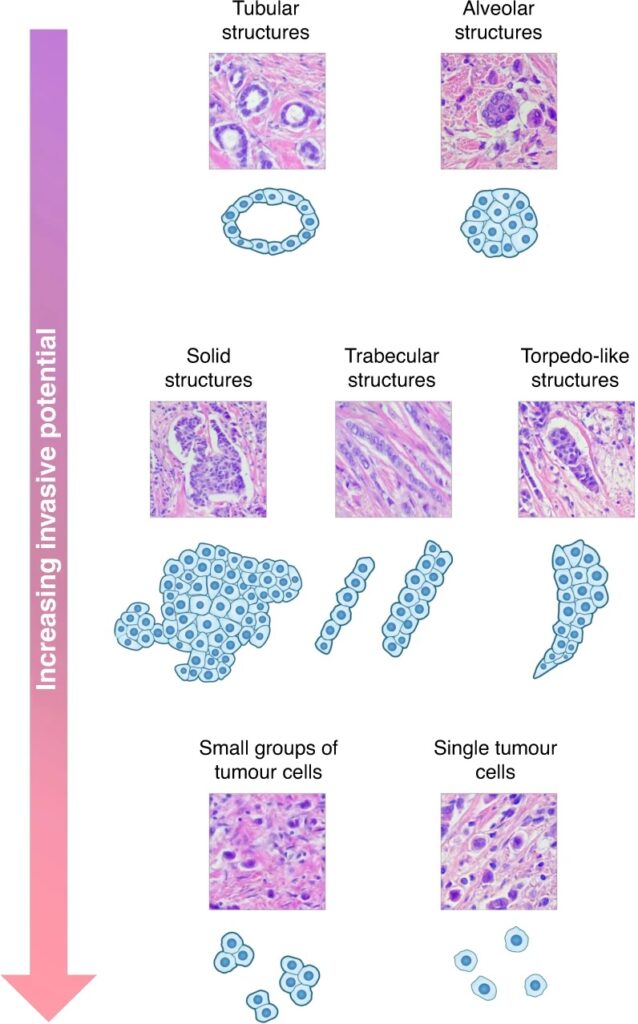
Intratumoural morphological heterogeneity of breast cancer as a model for studying the mechanisms of tumour cell invasion. -
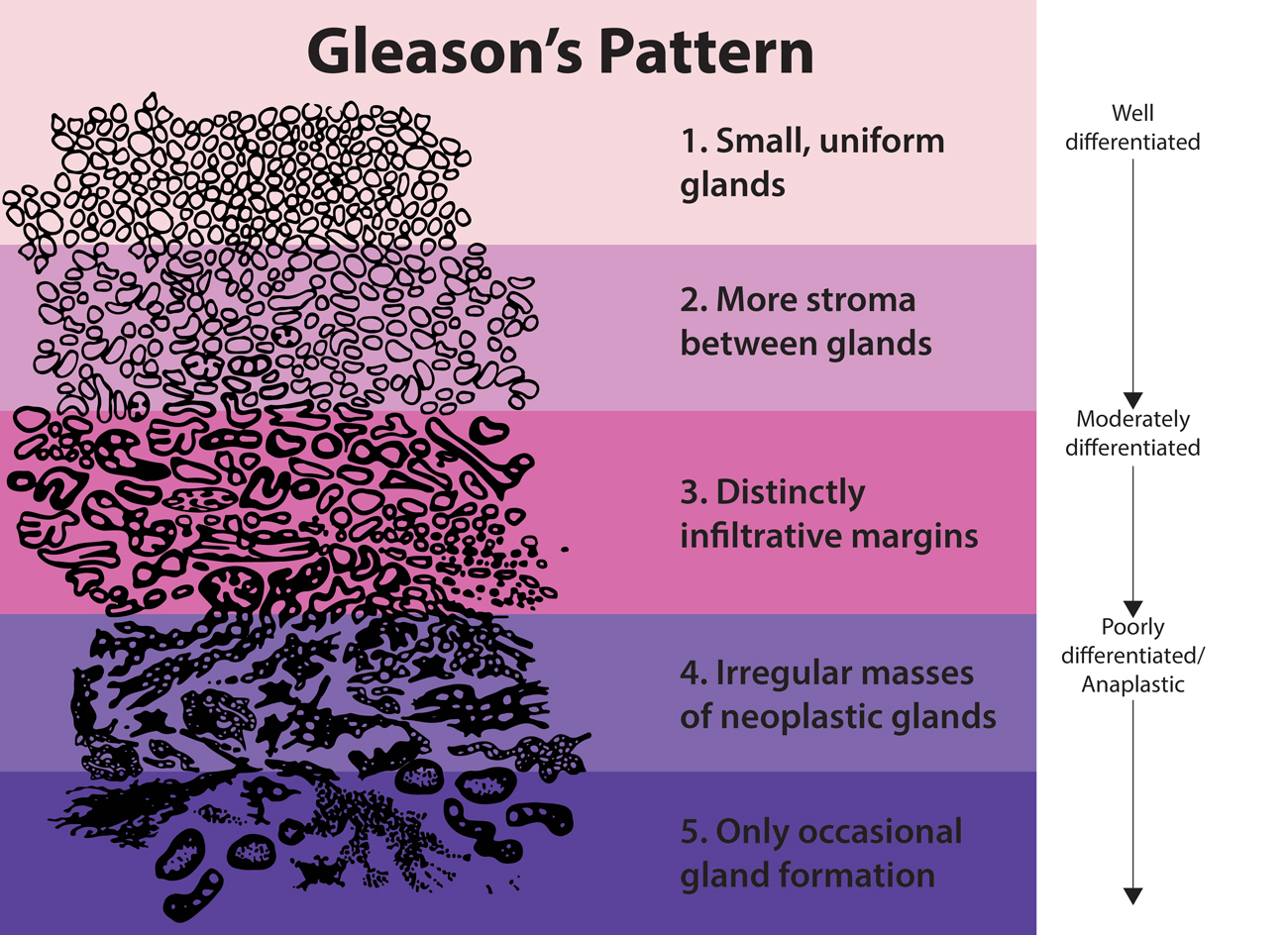
Gleason’s pattern – prostate cancer -
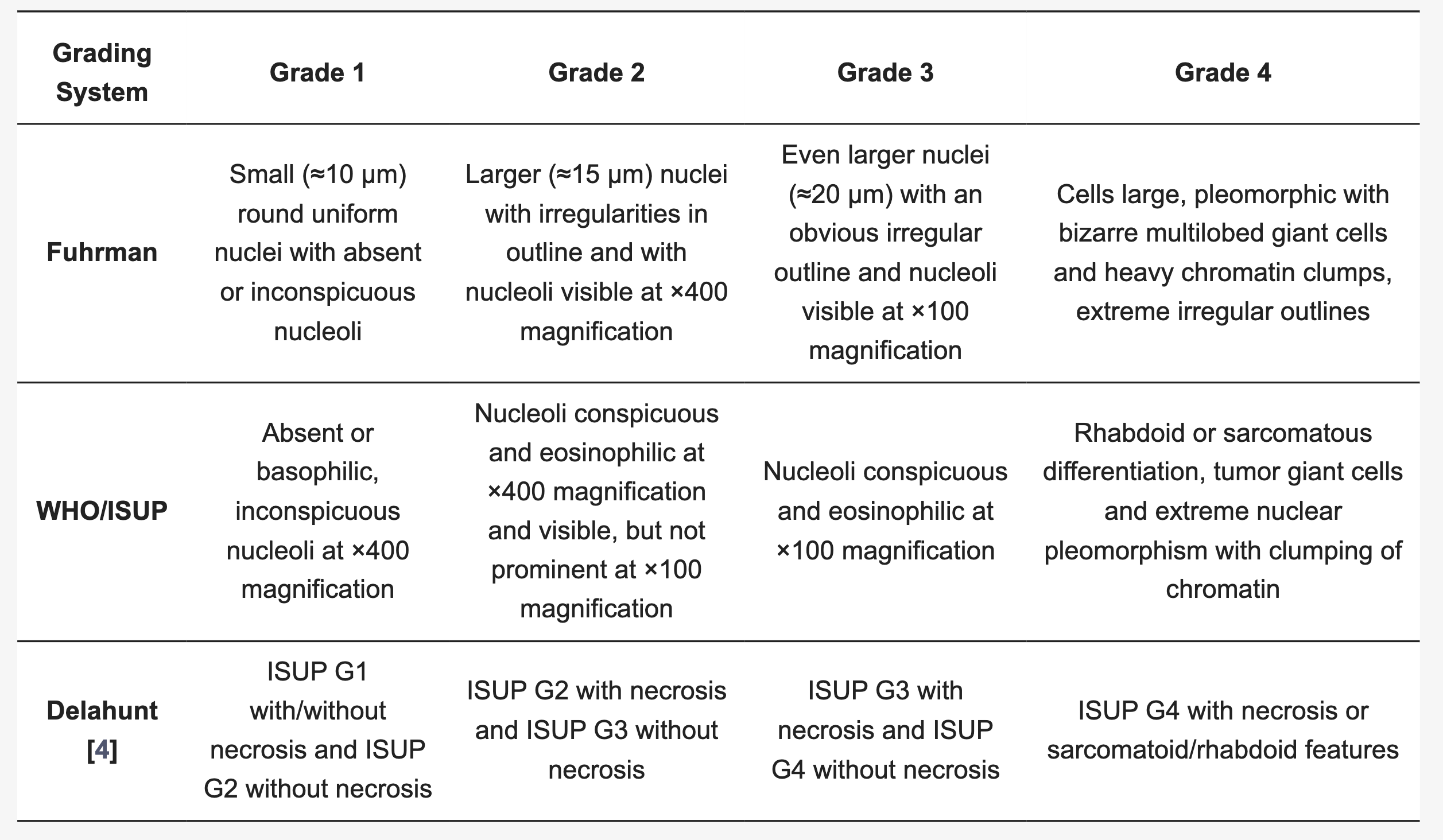
Overview of different grading systems -
Stage What it means Stage 0 Abnormal cells are present but have not spread to nearby tissue. Also called carcinoma in situ, or CIS. CIS is not cancer, but it may become cancer. Stage I, Stage II, and Stage III Cancer is present. The higher the number, the larger the cancer tumor and the more it has spread into nearby tissues. Stage IV The cancer has spread to distant parts of the body.
-
- Immunosupression, HIV – risk for cancer (e.g. Kaposi’s sarcoma and lymphoma)
-
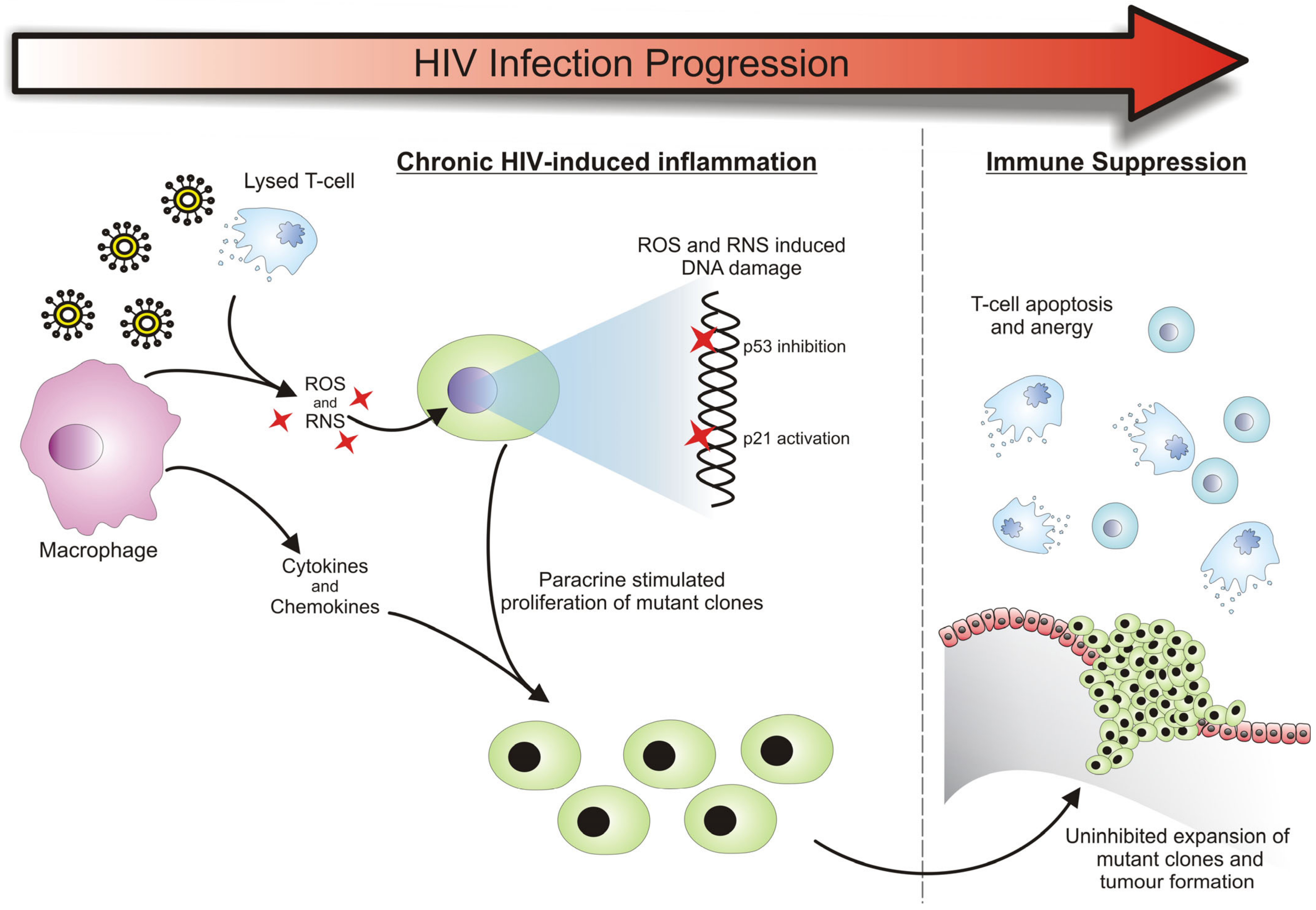
Cancer and HIV: The continual exposure of the immune system to constantly changing HIV antigens and the resultant inflammatory stress has been implicated in the accelerated aging of the immune system, which is usually only seen at the end of a healthy individual’s lifetime. This enhanced “inflammaging” leads to the depletion of the naïve T-cell population and the accumulation of differentiated and anergic T-cells. These essentially ineffective HIV-targeting T-cells have a reduced capacity to proliferate and are susceptible to activation-induced apoptosis. These changes render the immune system ineffective in eliciting a strong immune response towards new antigens that might arise, compromising the immune surveillance and eradication of new cancerous cells. This includes chronic HIV-induced inflammation. Various inflammatory mediators produced during HIV infection, such as ROS and RNS, contribute to carcinogenesis by modifying the growth and survival of normal cells or triggering the proliferation of cells with tumorigenic potential. -
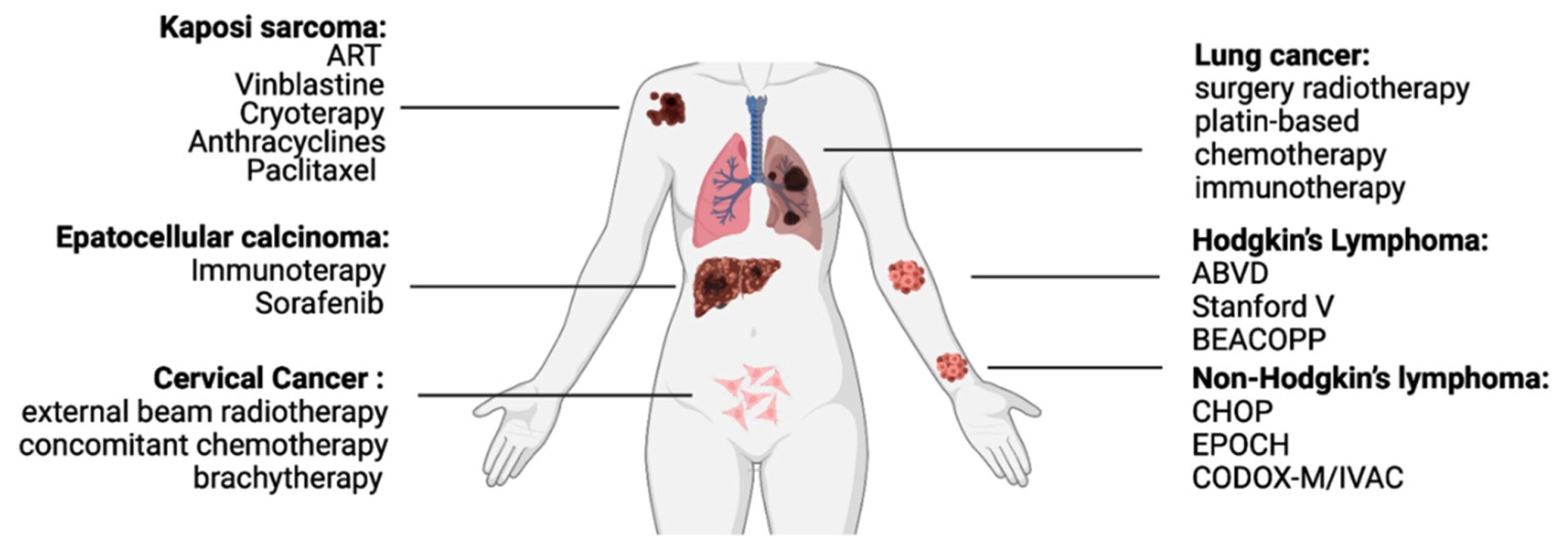
Most common type of tumor in HIV patients. -
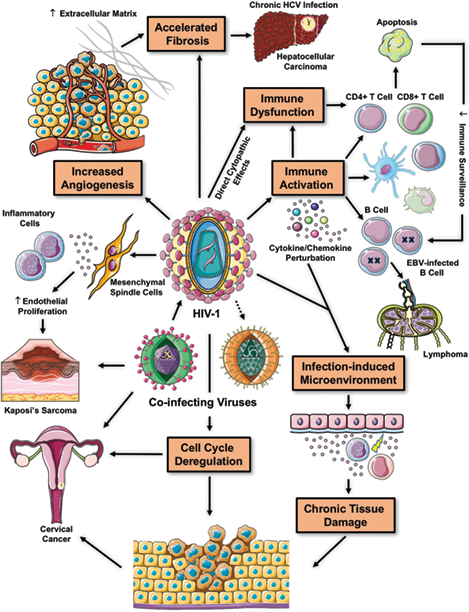
Mechanisms of HIV-1–associated cancer. Increased oncogenesis in the setting of HIV-1 disease usually involves co-infection with other viruses and immune dysfunction, accompanied by decreased immune surveillance. Persistent immune activation as a consequence of HIV-1 infection may lead to chronic tissue damage and the formation of infection-induced microenvironments that potentiate cancer induction. HIV-1 and its products may also influence oncogenesis (usually in the context of viral cooperativity) independently of immune suppression through cell cycle deregulation and/or influencing the nonimmune microenvironment (e.g., increased extracellular matrix, pro-fibrogenic factors and blood vessel formation).
-
- What is Leukemia?
- Cancers that begin in the blood-forming tissue of the bone marrow are called leukemias. These cancers do not form solid tumors. Instead, large numbers of abnormal white blood cells (leukemia cells and leukemic blast cells) build up in the blood and bone marrow, crowding out normal blood cells.
-
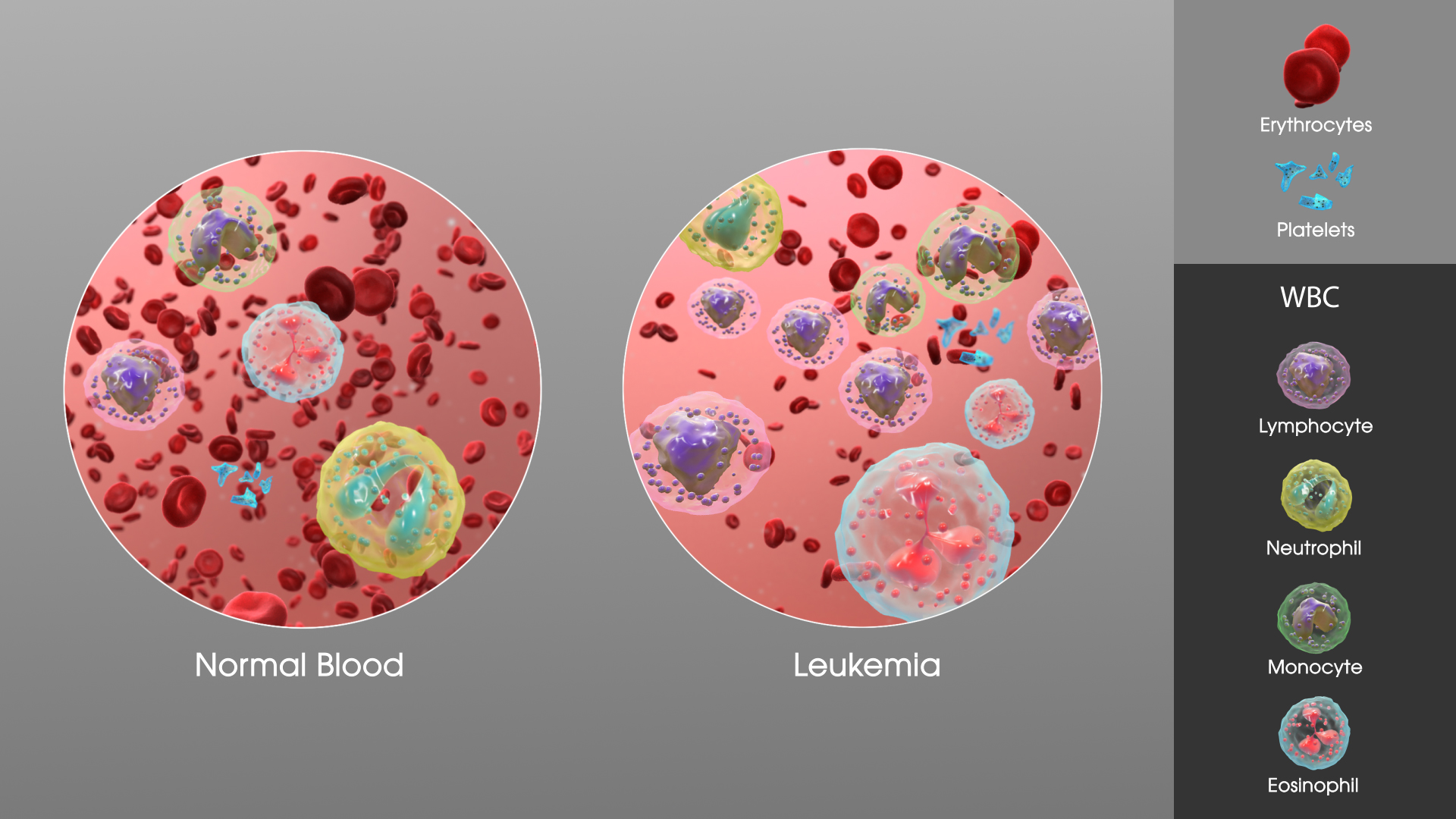
3D Medical Animation still showing an increase in white blood cells of a person suffering from Leukemia. -
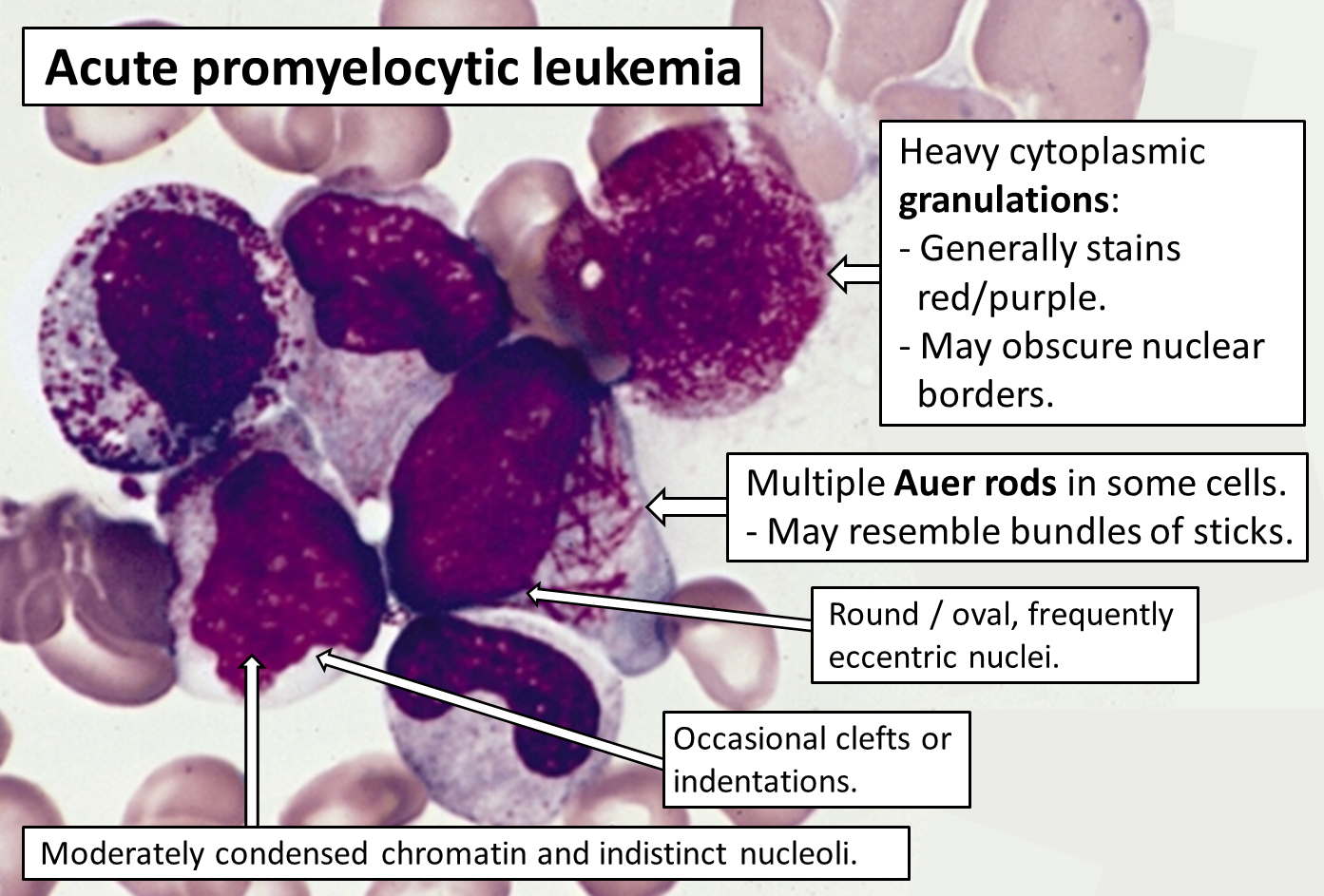
Cytology of acute promyelocytic leukemia -
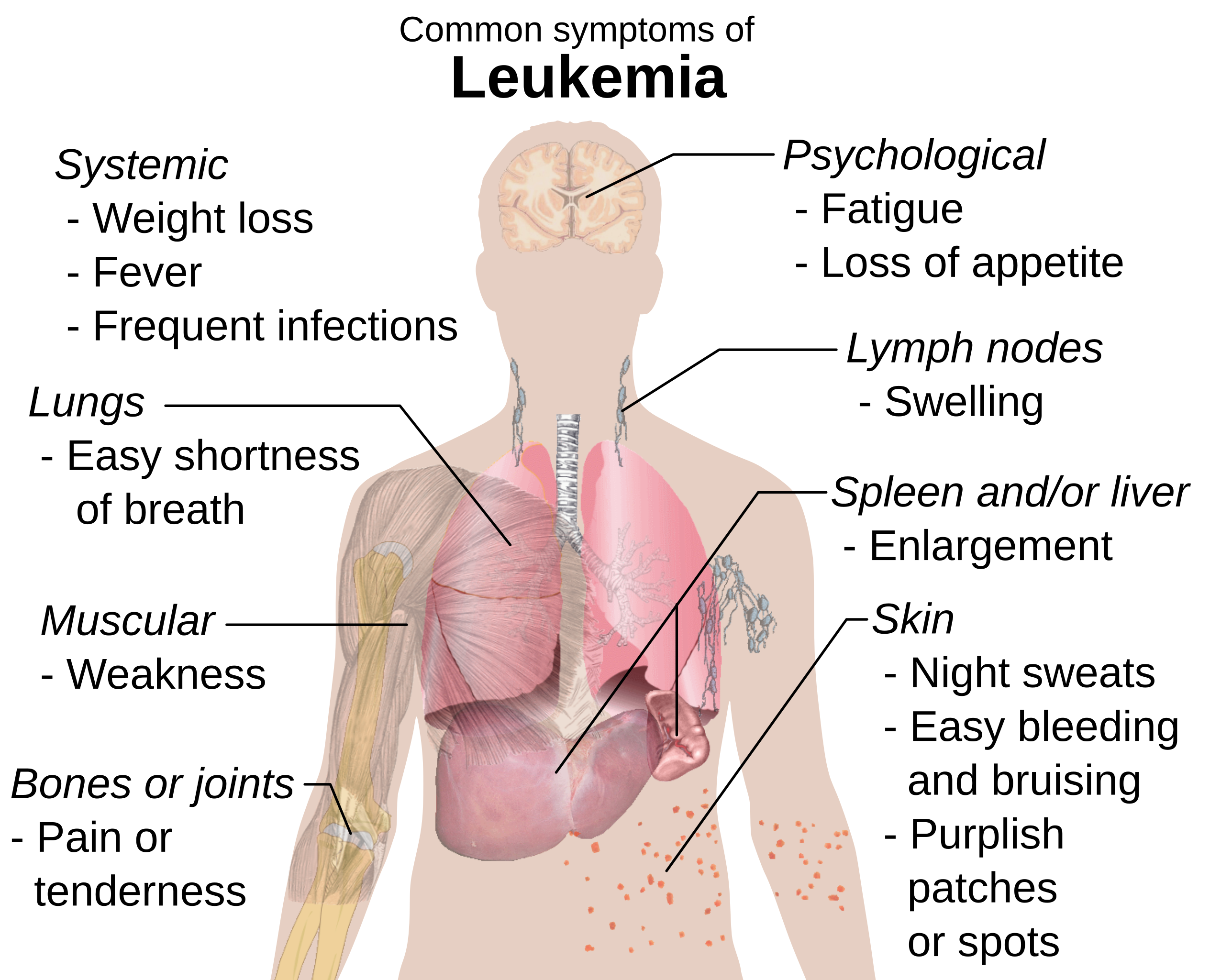
Common symptoms of chronic or acute leukemia. -
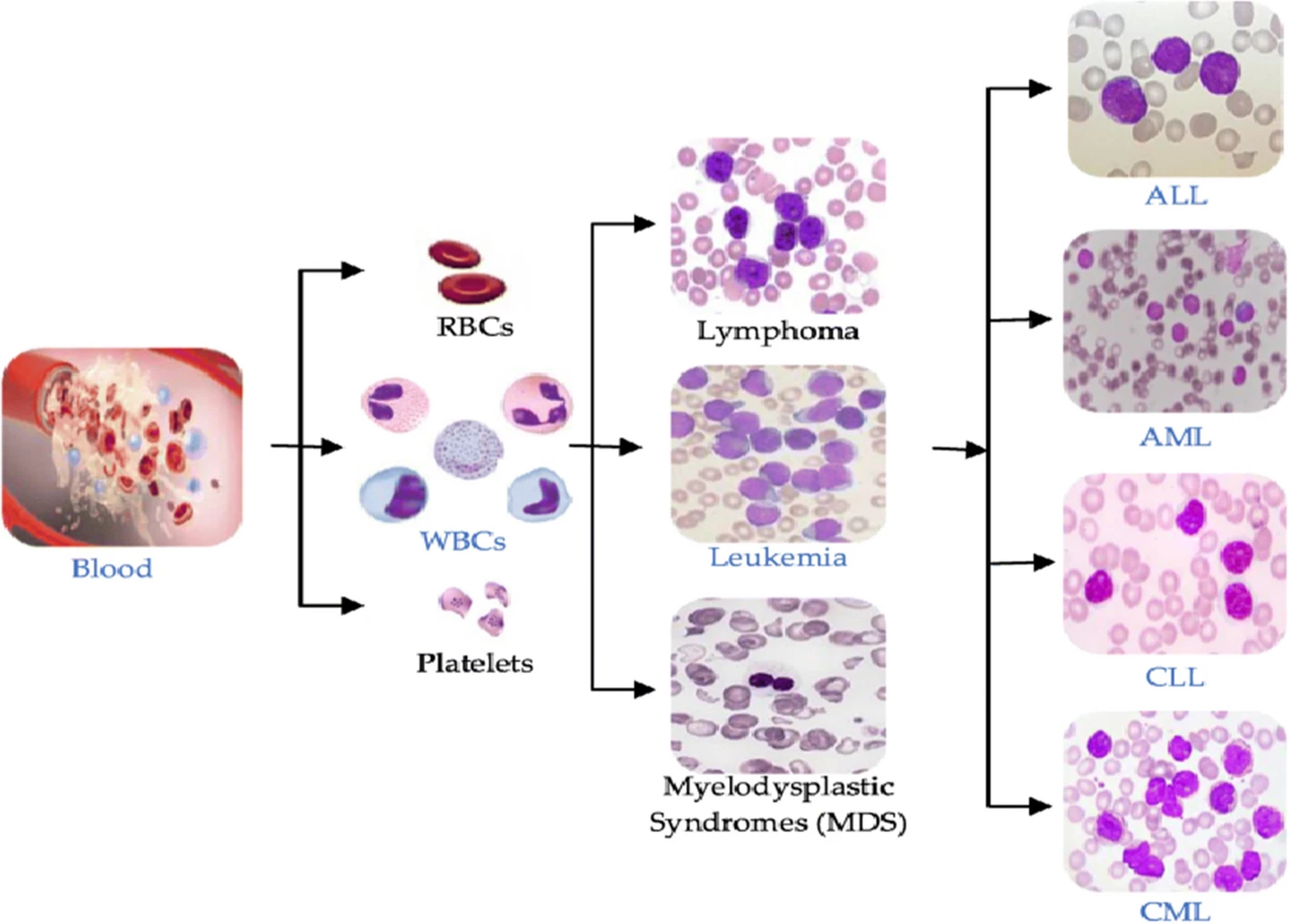
Leukemia is classified into four major categories, including acute myeloid leukemia (AML), acute lymphoblastic leukemia (ALL), chronic myeloid leukemia (CML), and chronic lymphocytic leukemia (CLL), in addition to several fewer common types. -
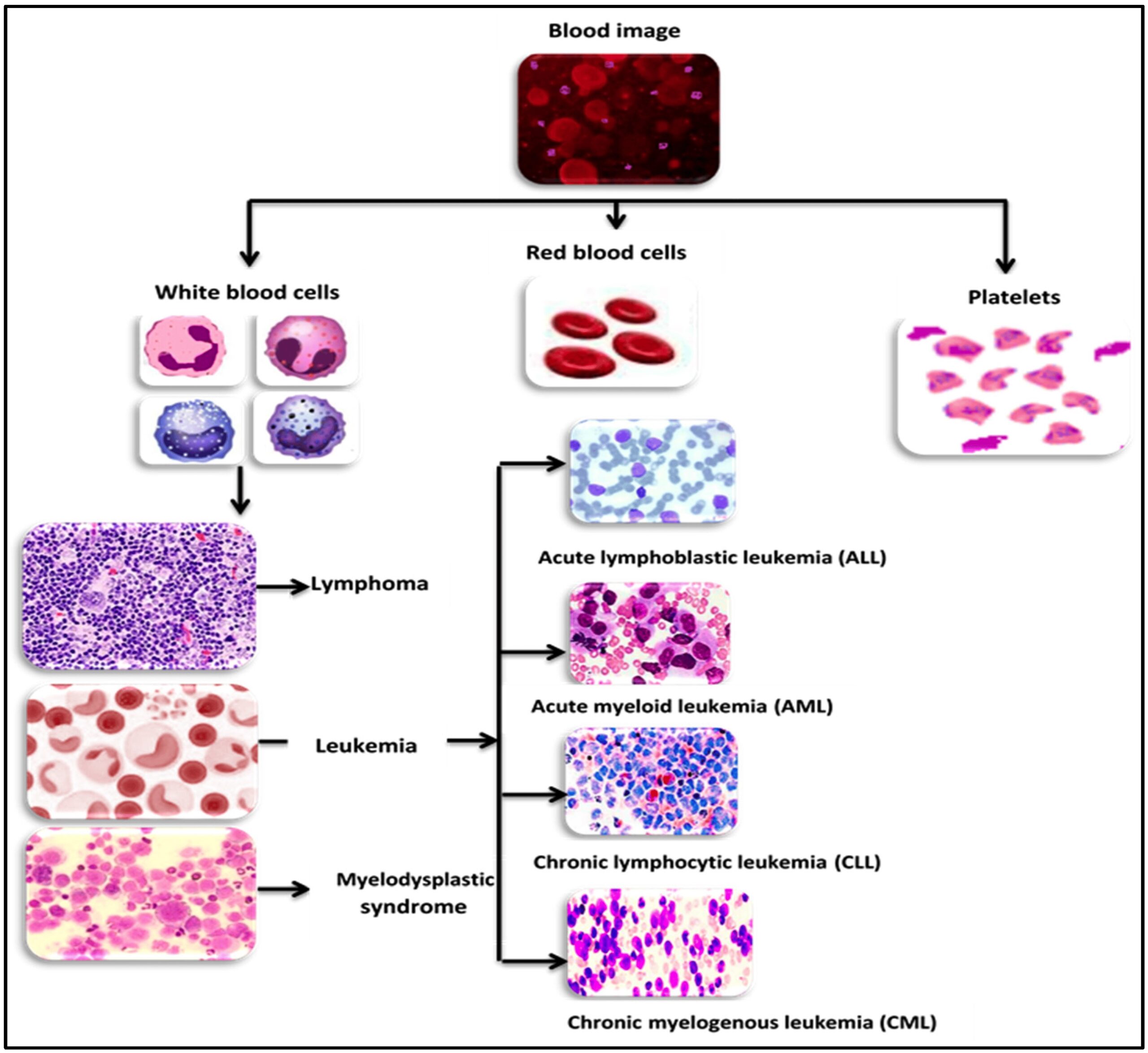
The most well-known leukemia classification system divides acute leukemia types into two groups according to the French–American–British model: acute myeloid leukemia (AML) and acute lymphoblastic leukemia (ALL). -
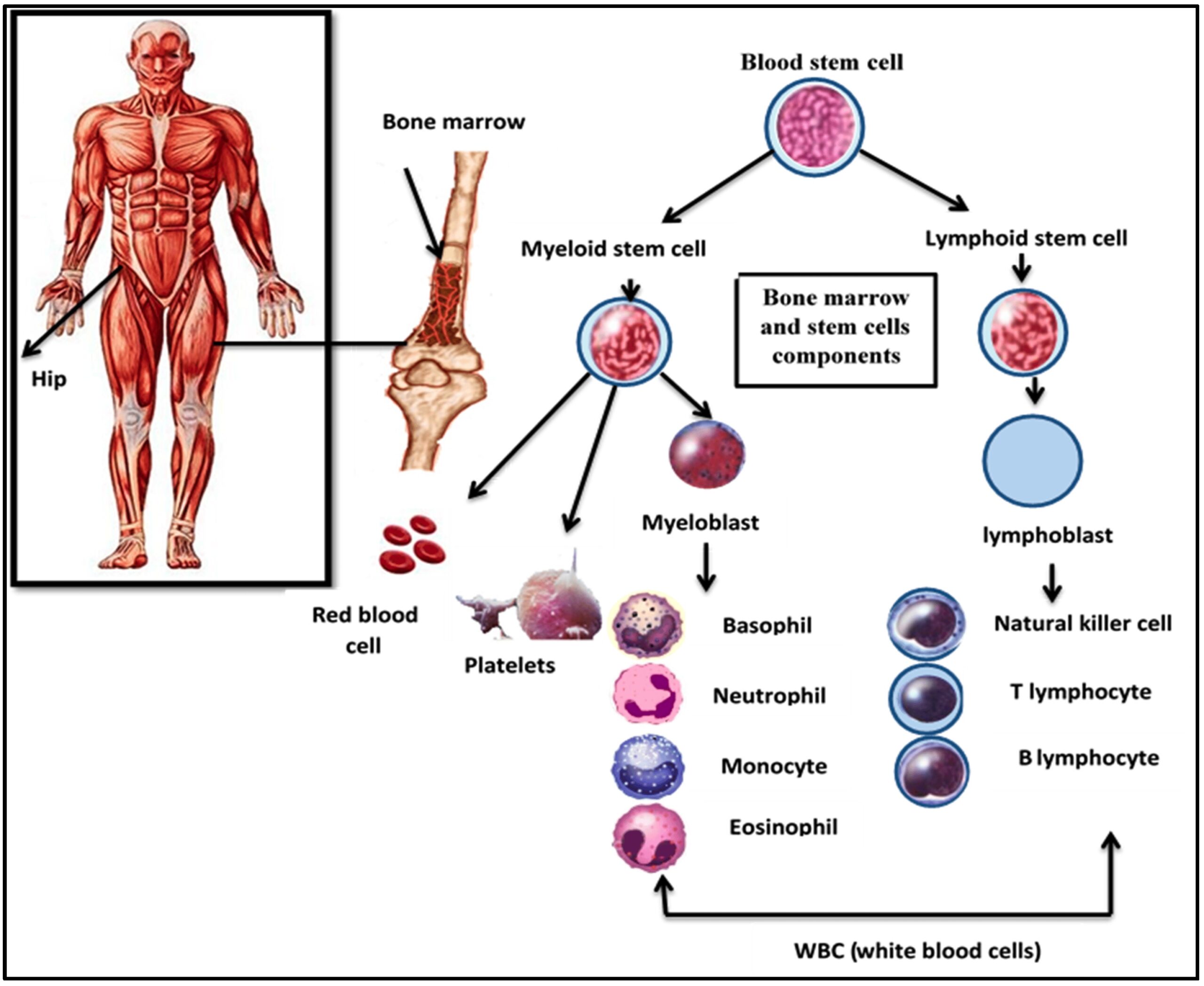
Bone marrow and stem cells components. Leukemia is a cancer of the bone marrow. -
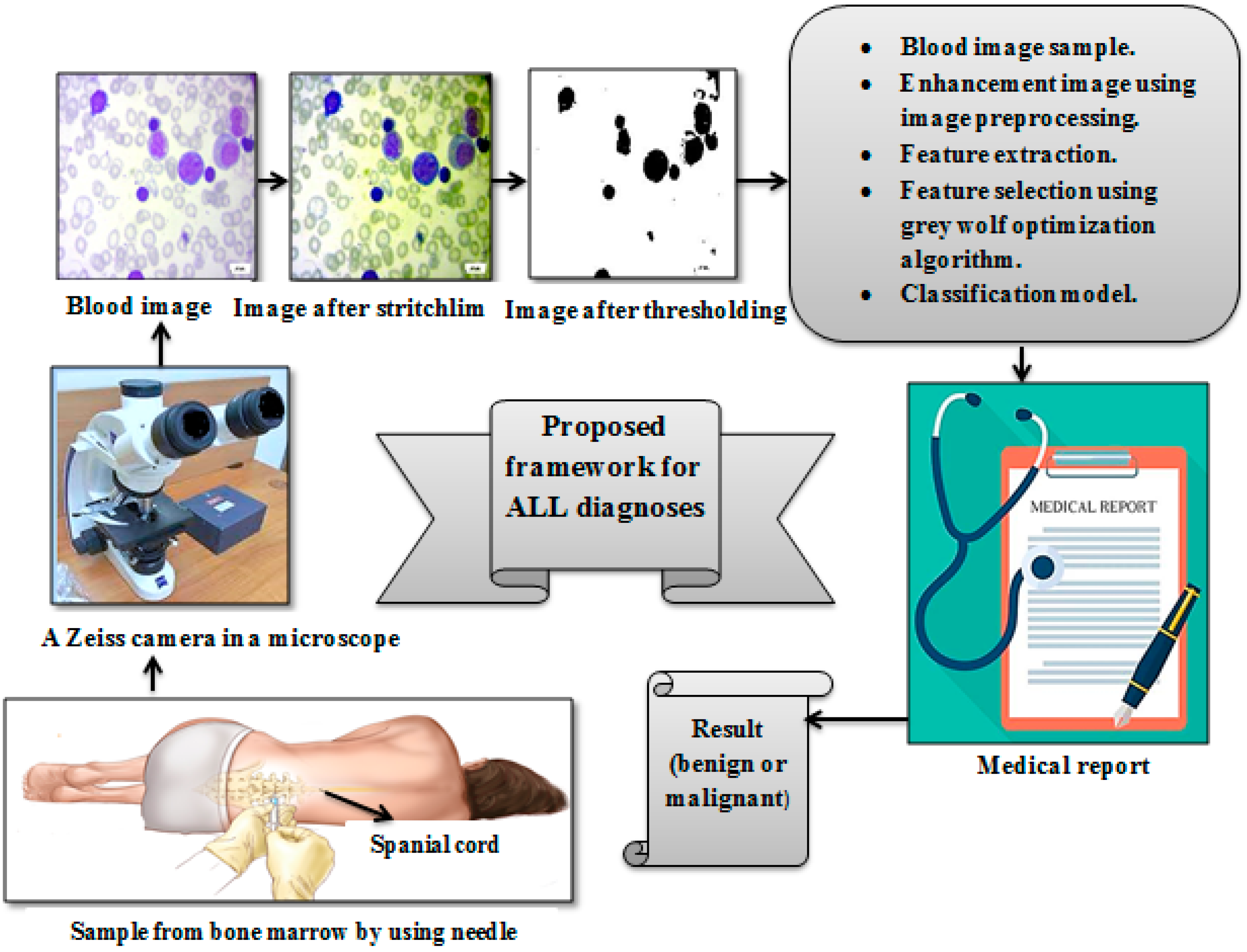
Proposed framework for leukemia diagnosis. - `
- What is Lymphoma?
-
- Lymphoma is cancer that begins in lymphocytes (T cells or B cells). These are disease-fighting white blood cells that are part of the immune system. In lymphoma, abnormal lymphocytes build up in lymph nodes and lymph vessels, as well as in other organs of the body.
-

Symptoms of Lymphoma: feel for swelling in your lymph nodes. -

Macroscopic aspect of the cut surface of a human lymph node replaced by lymphoma. The node was about 6 x 4 cm (2.5″ x 1.5″). The lymphoma is the nodules of pinkish tissue surrounded by yellowish fatty tissue. Upon histological examination, the node contained follicular lymphoma. -

Spleen, Diffuse Large B Cell Lymphoma: Elderly man who presented with abdominal pain. On laparotomy, the spleen had a tumor that had invaded through the capsule and was adherent to the diaphragm. - `
-
- Different types of treatment; Curative, Palliative
- Surgery: laparoscopic, radiofrequency ablation,
-
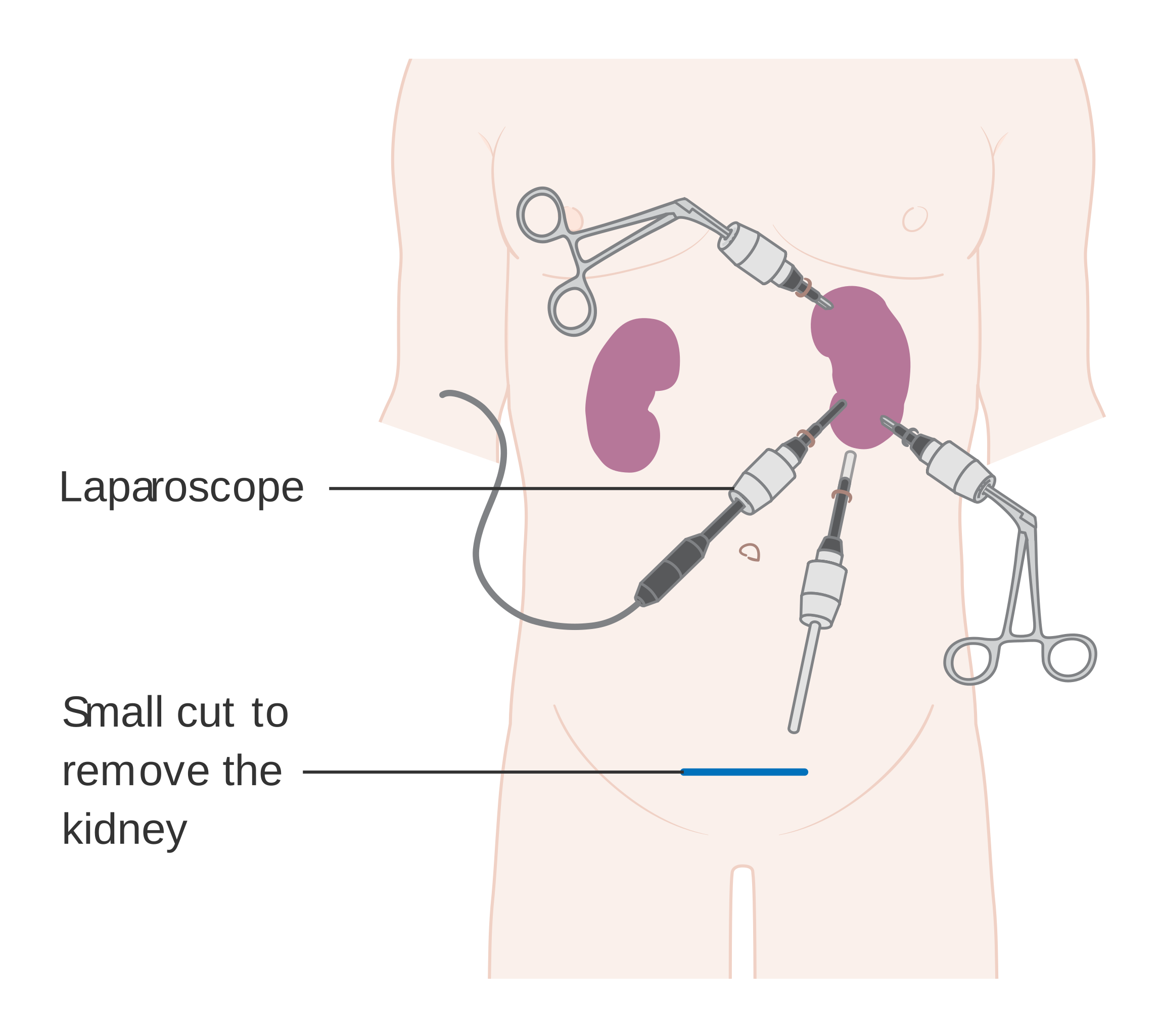
Diagram showing laparoscopic surgery for kidney cancer -
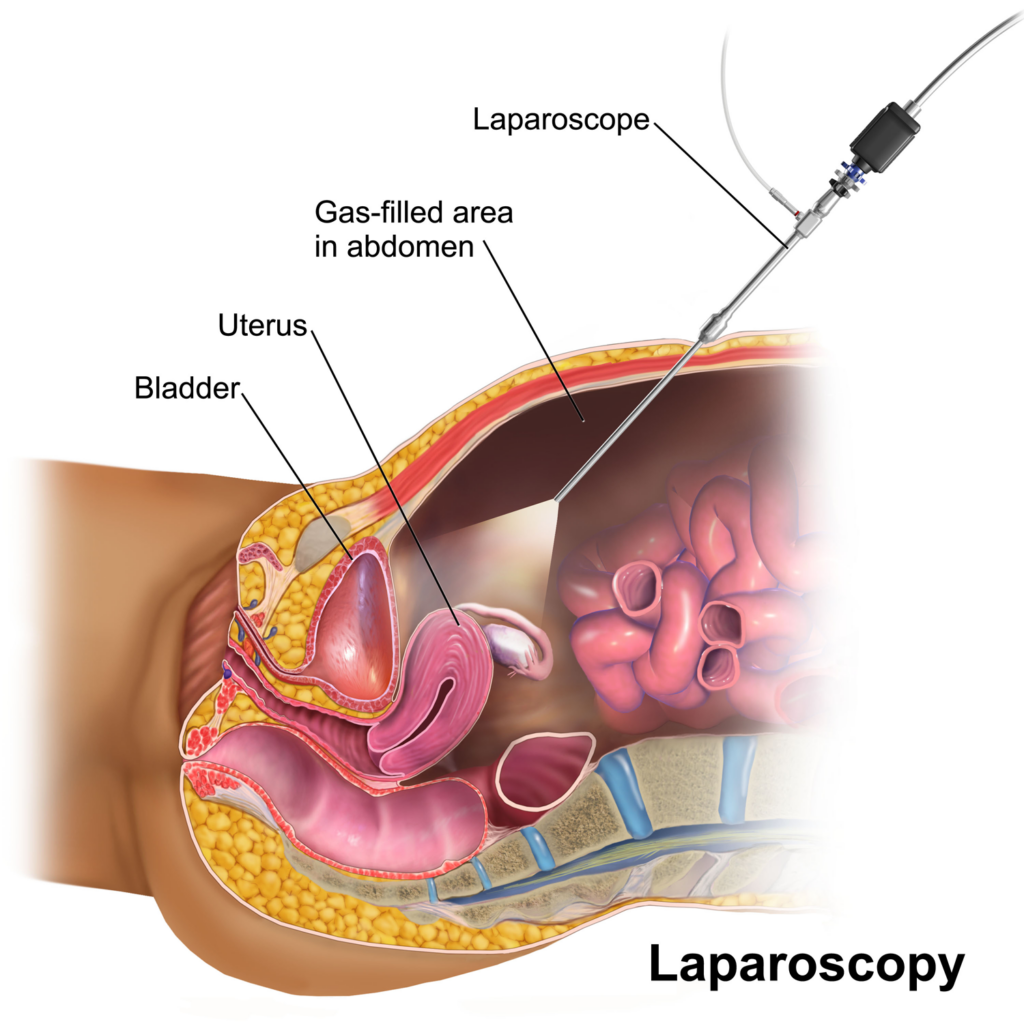
Illustration of Laparoscopy -
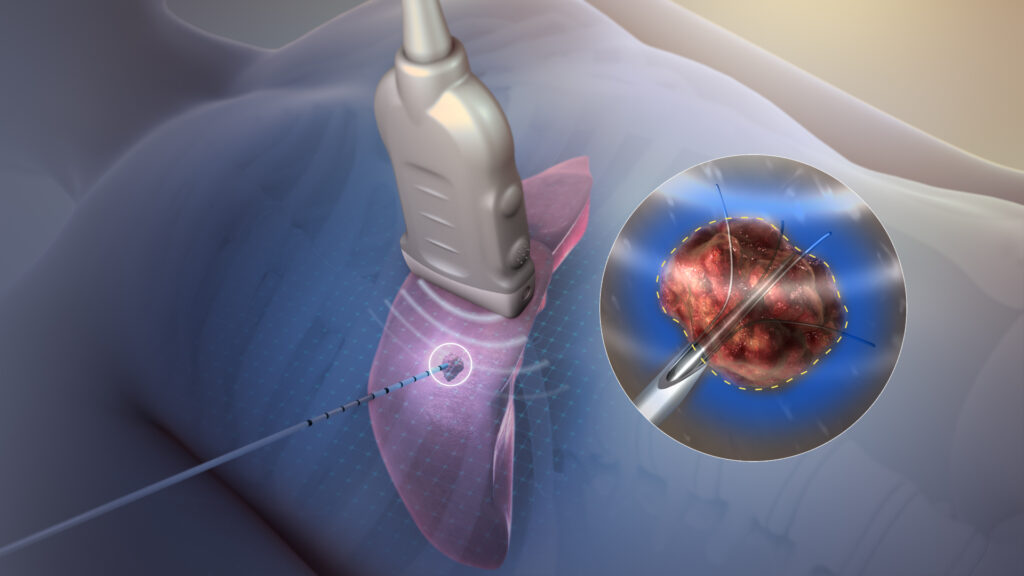
An electric current produced by radiofrequency ablates the tumor. -

Description of Liwen RF™ ablation system and main findings. Liwen RF™ (Hangzhou Nuo Cheng Medical Instrument Co., Ltd., Hangzhou, Zhejiang, China) is a novel radiofrequency ablation system with a stepless adjustable length needle electrodes for percutaneous intramyocardial septal radiofrequency ablation (PIMSRA). The device is an integrated system, comprising ablation electrode kit, ablation generator, cooling system, and patient circuit. -
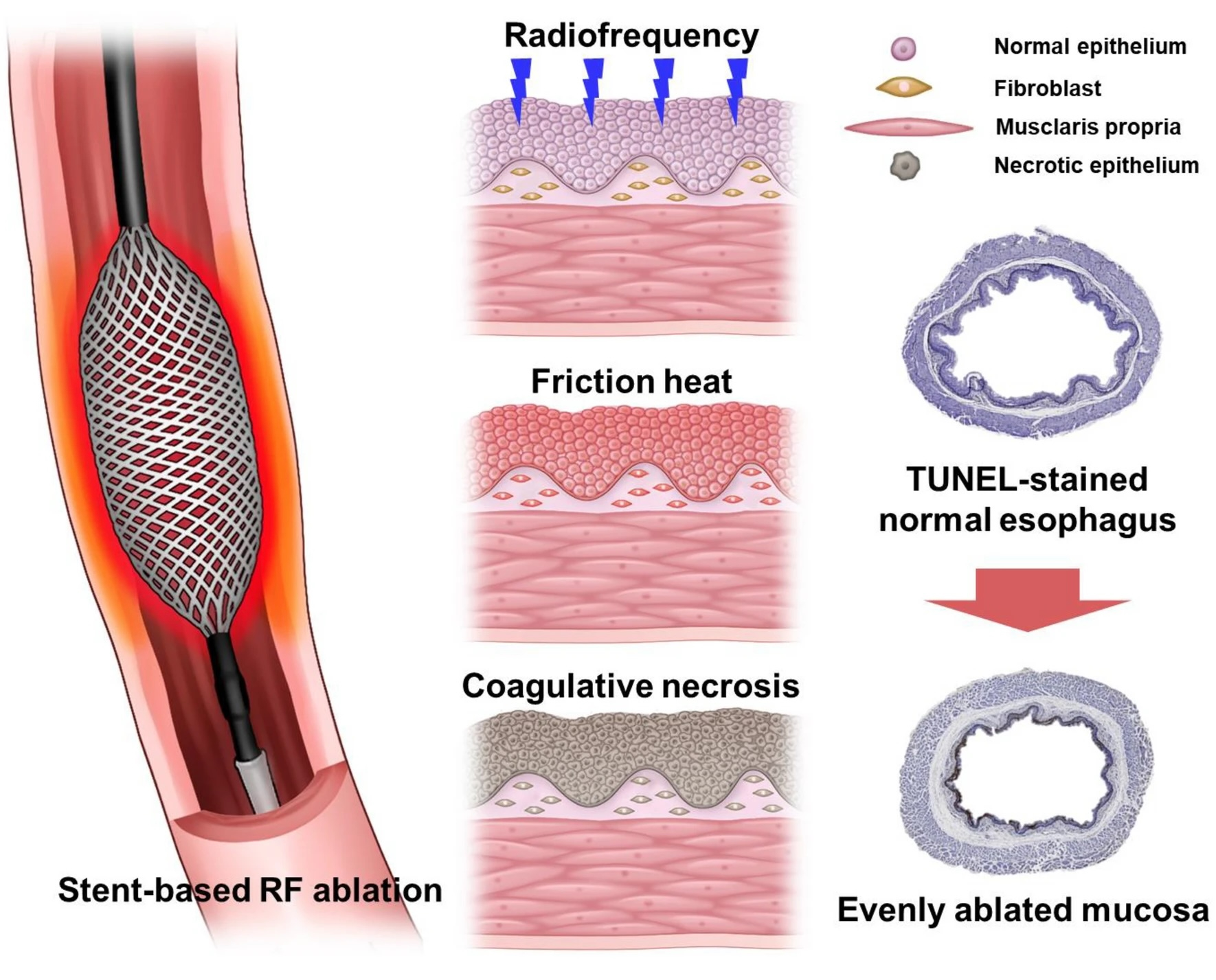
Schematic illustration of the radiofrequency ablation using the stent-based electrode in the rat esophagus and representative TUNEL-stained images indicating the resulting therapeutic effects. - `
-
- Chemotherapy – main types – and how does chemotherapy kill cancerous cells
- Types of Chemotherapy Delivery (oral, subcutaneous, intravenous, intramuscular, intralesional, intrathecally(subarachnoid), intraperitoneal, intraventricular)
-
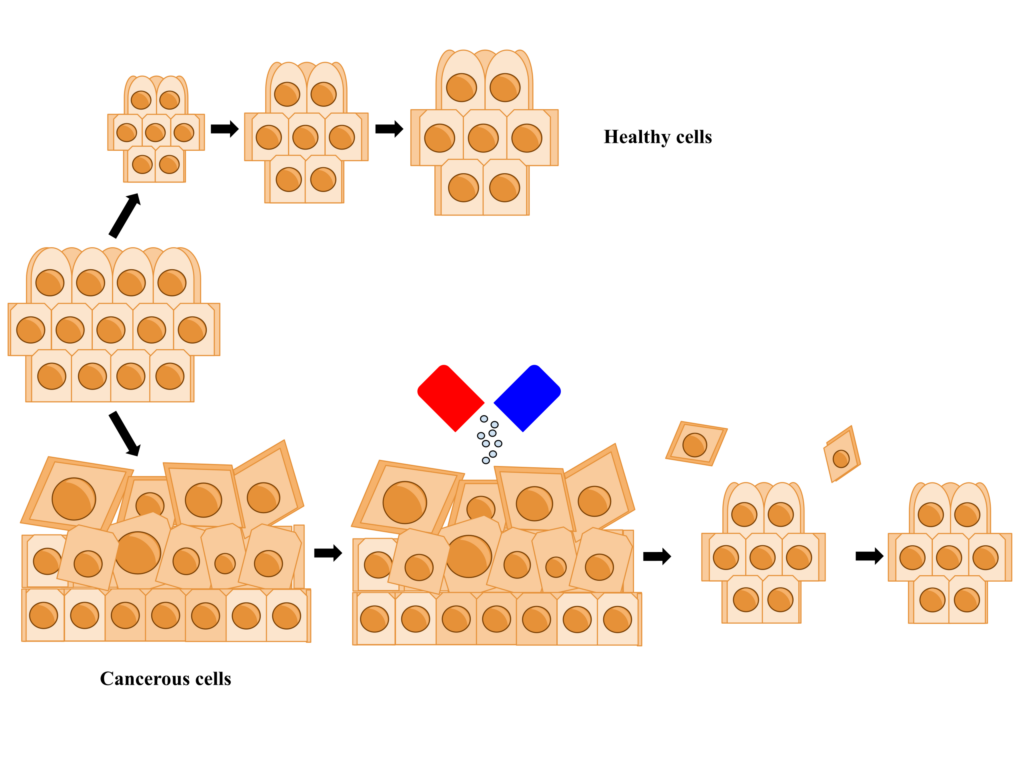
Development and Elimination of Cancer Cells as Chemotherapy is Applied: The cells shown either reproduce and grow into other healthy cells, or develop a tumor through the quick replication of damaged cells. A chemotherapy drug is applied to inhibit the growth and replication only of the damaged cells. -

Intravenous chemotherapy: another type of chemotherapy is injected straight into your veins. -

Chemotherapy intrathecally: This treatment is another type of chemotherapy which is injected into your spinal cord and brain instead of into your blood. -
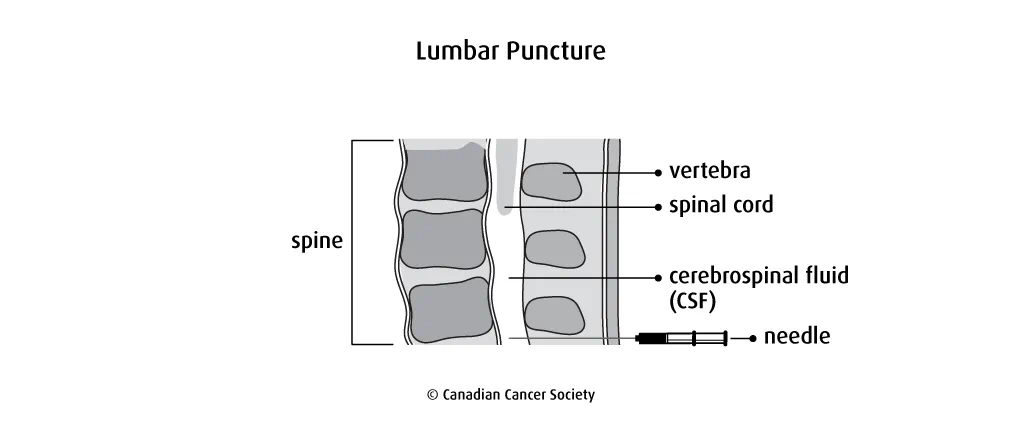
Chemotherapy may be given through a lumbar puncture into the space around the spinal cord containing the CSF. -
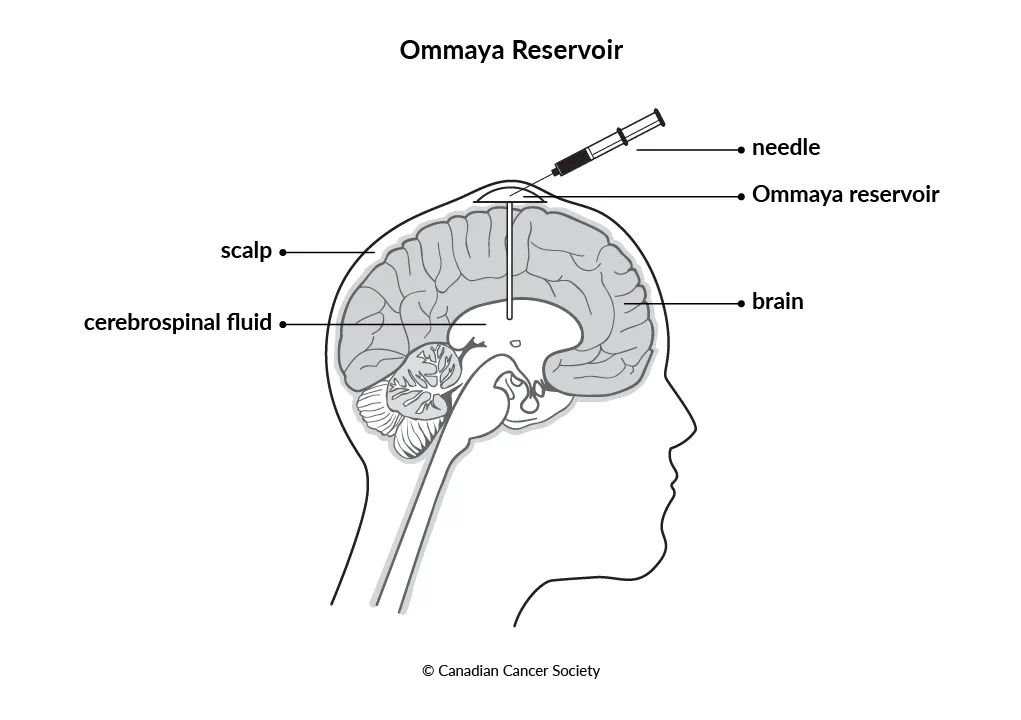
Intraventricular chemotherapy:
Chemotherapy for brain tumours may be given directly into the CSF in the ventricles of the brain. It is given through an Ommaya reservoir, which is a small, dome-shaped device with a short tube (catheter) attached to it that is placed during surgery. The chemotherapy drug is injected using a small needle inserted through the scalp into the Ommaya reservoir. -
Drug delivery, diffusion and consumption in tumor. -

One way to take chemotherapy is an oral pill. -
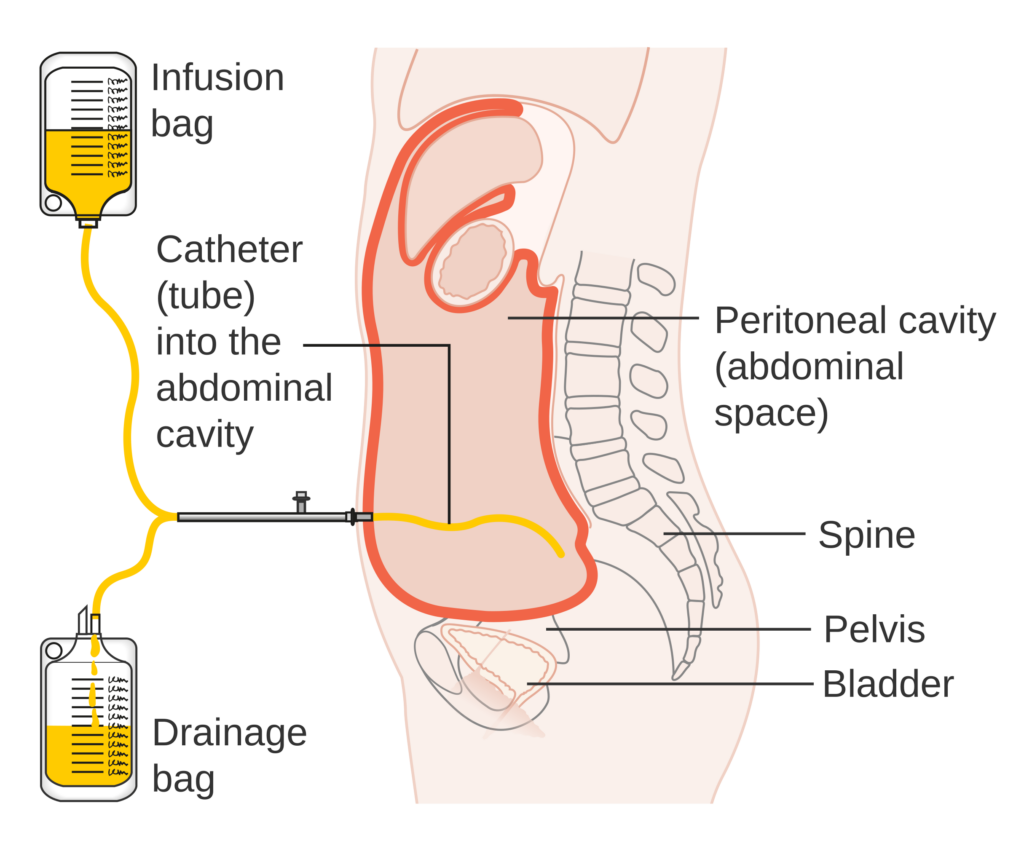
Intraperitoneal chemotherapy: this diagram showing how you have chemotherapy into the abdomen -
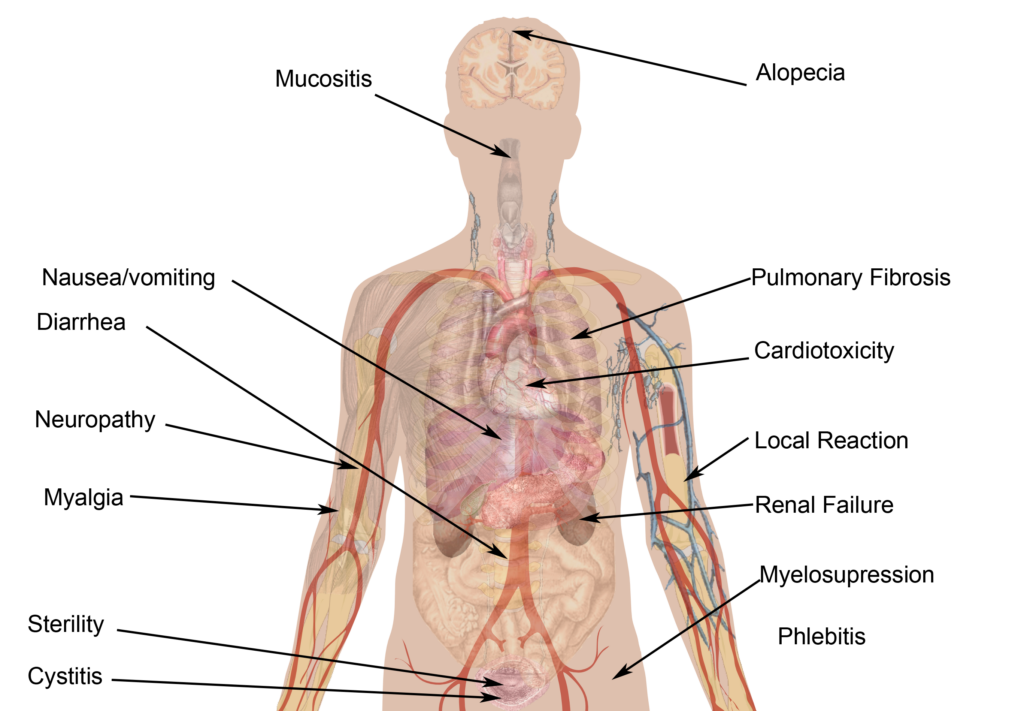
Side Effects of Chemotherapy - `
- Radiation – main types – Radiation waves (e.g. Cobalt machine), Radioactive isotope seeds/salts/solutions/pills and how does radiation kill cancerous cells
-
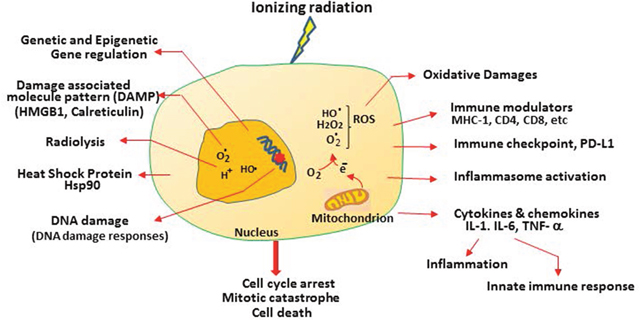
Multiple features of radiation-induced cellular responses in cancer cells. -
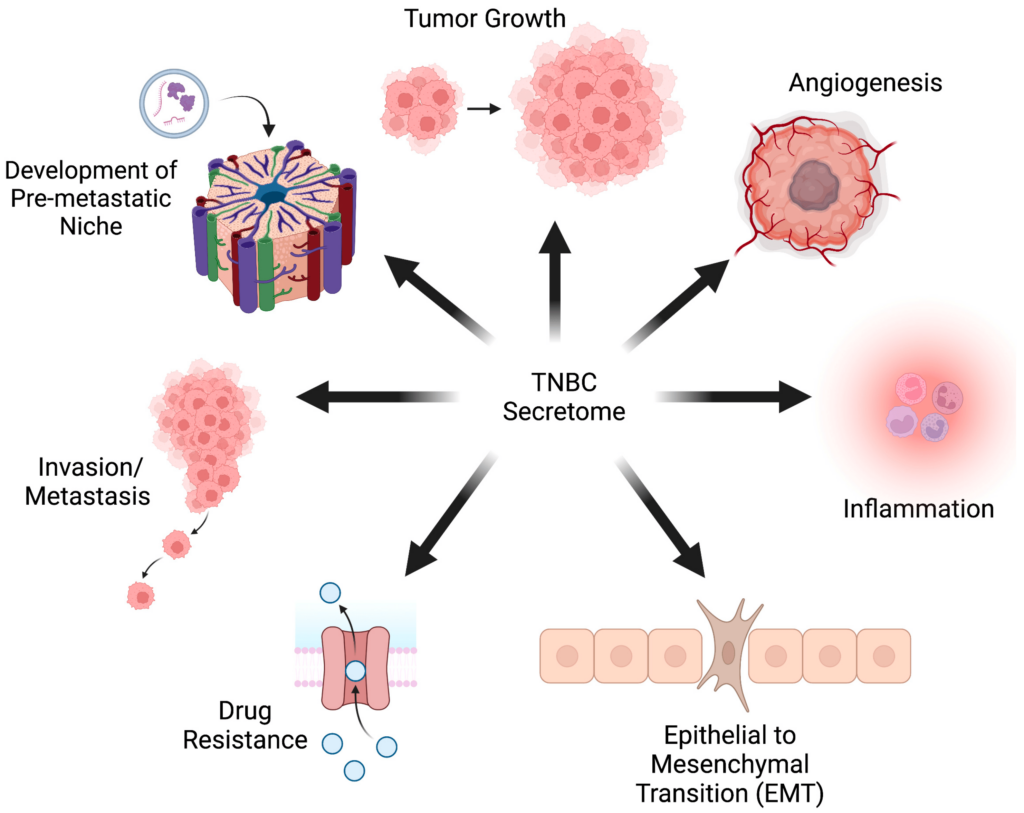
Effects of the TNBC secretome. Protein factors secreted by TNBC cells and tumors regulate cancer-promoting processes -
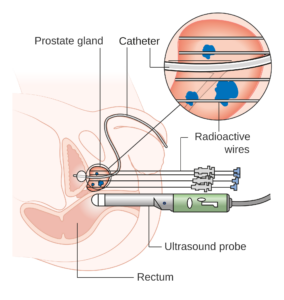
By placing the radioactive source inside the body, brachytherapy can target tumors more directly than external beam radiotherapy -
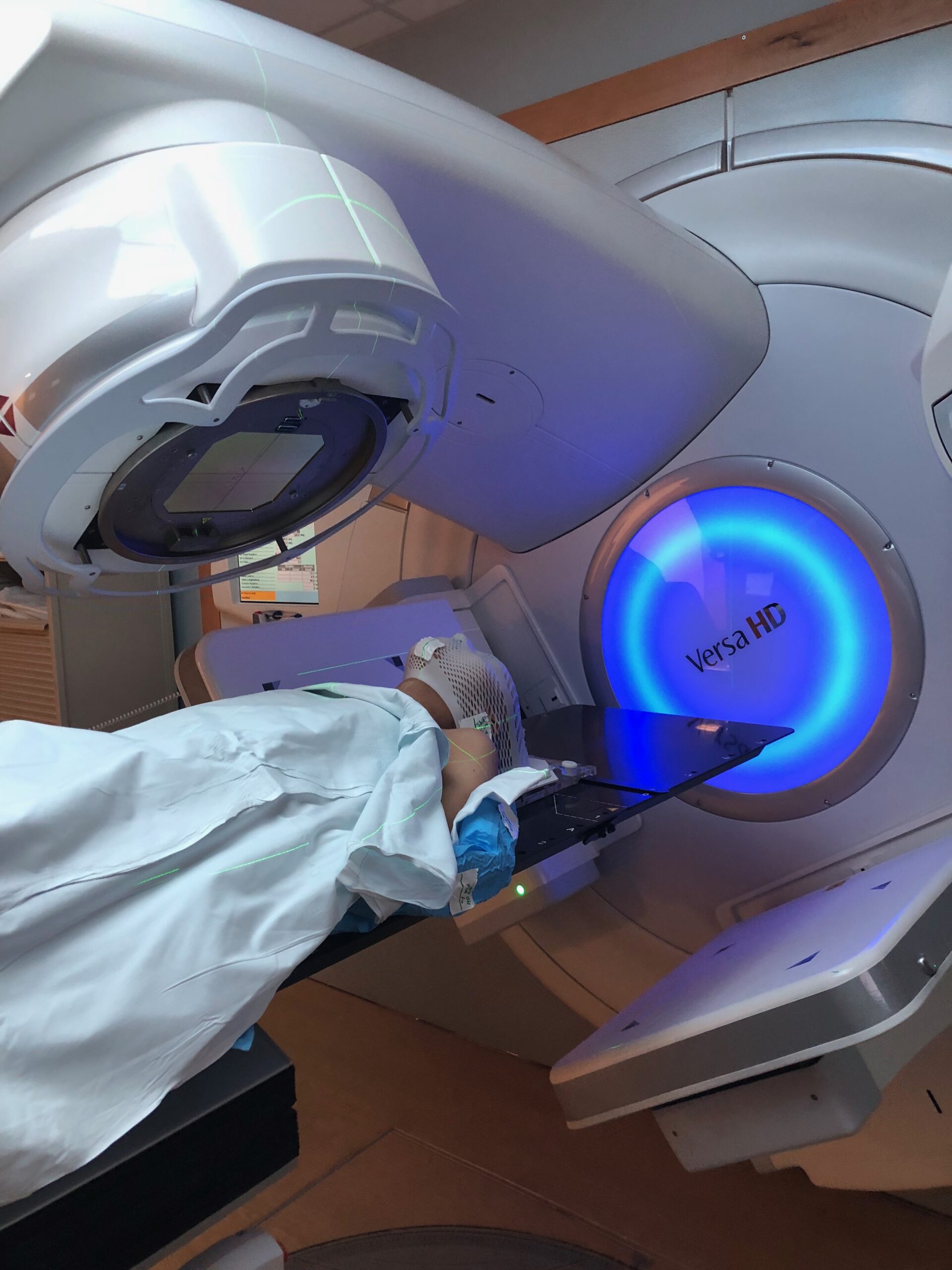
Radiation therapy for Hodgkin’s Lymphoma in a Versa HD. -
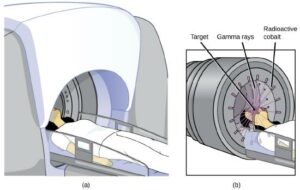
The cartoon in (a) shows a cobalt-60 machine used in the treatment of cancer. The diagram in (b) shows how the gantry of the Co-60 machine swings through an arc, focusing radiation on the targeted region (tumor) and minimizing the amount of radiation that passes through nearby regions.
A. A woman lies down as she goes into a dome shaped medical machine. B. A closer view of the women’s head shows gamma rays from radioactive cobalt attacks the target on the woman’s head. - `
-
- Anti-angiogenic treaments
- Nutrition, Counselling, Physiotherapy, Speech Therapy, massage, meditation, healthy diet
- Hormone therapy – what types and why does it work?
- Glucocorticoid (prednisone)
-
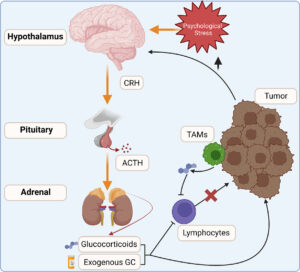
The HPA axis integrates internal and external cues to modulate glucocorticoid production. Increased glucocorticoid signaling is commonly associated with cancers. Increased stress and tissue damage act on the hypothalamus to stimulate the release of corticotropin-releasing hormone (CRH), which in turn stimulates adrenocorticotropic hormone (ACTH) release into circulation. ACTH acts on steroidogenic cells within the adrenal cortex to increase endogenous glucocorticoid production. Exogenous corticosteroids are also commonly co-administered with anti-cancer therapies. Within the tumor, infiltrating leukocytes, such as tumor-associated macrophages (TAMs), activate steroidogenesis and may increase glucocorticoid concentrations within the tumor. Elevated glucocorticoids inhibit anti-tumor immune responses and are linked to increased tumor cell survival. -
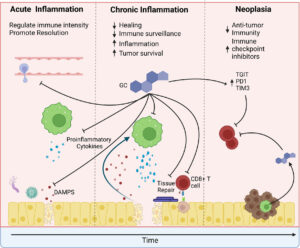
The effects of glucocorticoids change over the course of tumor development. In the pre-tumor microenvironment, glucocorticoids may protect from cancer by limiting the intensity of inflammation. Glucocorticoids suppress immune cell recruitment to sites of damage or infection and suppress proinflammatory cytokine production. However, during chronic inflammation, glucocorticoids may promote tumor development. Prolonged glucocorticoid signaling inhibits wound healing, thereby causing a feedforward loop of increased release of damage-associated molecular patterns (DAMPs), which increase inflammation and further promote tissue damage. Simultaneously, glucocorticoids suppress anti-tumor surveillance by CD8 T cells. Similarly, glucocorticoids suppress anti-tumor immunity within the tumor microenvironment and promote the expression of immune checkpoint proteins. However, their effects are compounded by increased psychological stress, exogenous steroid treatment, and local steroidogenesis by tumor-infiltrating immune cells. Furthermore, glucocorticoids may directly promote tumor cell survival by suppressing apoptosis and promoting tumor cell growth.
-
- Sex hormones
-
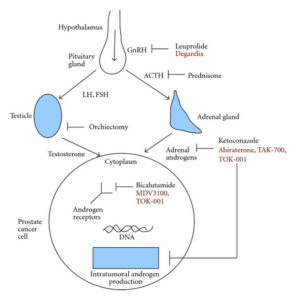
Hormonal therapy in prostate cancer. Physiologically relevant androgens for prostate cancer originate from three sources: the testicle, adrenal glands, and via intratumoral production. The sites of activity of clinically relevant hormonal therapies are illustrated here, with new and investigational treatments indicated in red. -
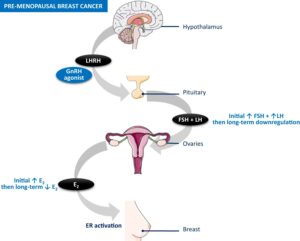
Upon initiation of GnRH agonist therapy, it mimics endogenous LHRH and stimulates the production of FSH and LH from the pituitary, resulting in an initial surge of E2 from the ovaries. With long-term administration of GnRH agonists, the LHRH receptors are downregulated and desensitized, resulting in reduced ovarian hormone production. Abbreviations: GnRH gonadotropin-releasing hormone, LHRH luteinizing hormone-releasing hormone, FSH follicle-stimulating hormone, LH luteinizing hormone, E2 estradiol, ER estrogen receptor. - `
-
- Glucocorticoid (prednisone)
- Antibodies – why and how? (simplistically)
- Radiolabelled antibodies
-
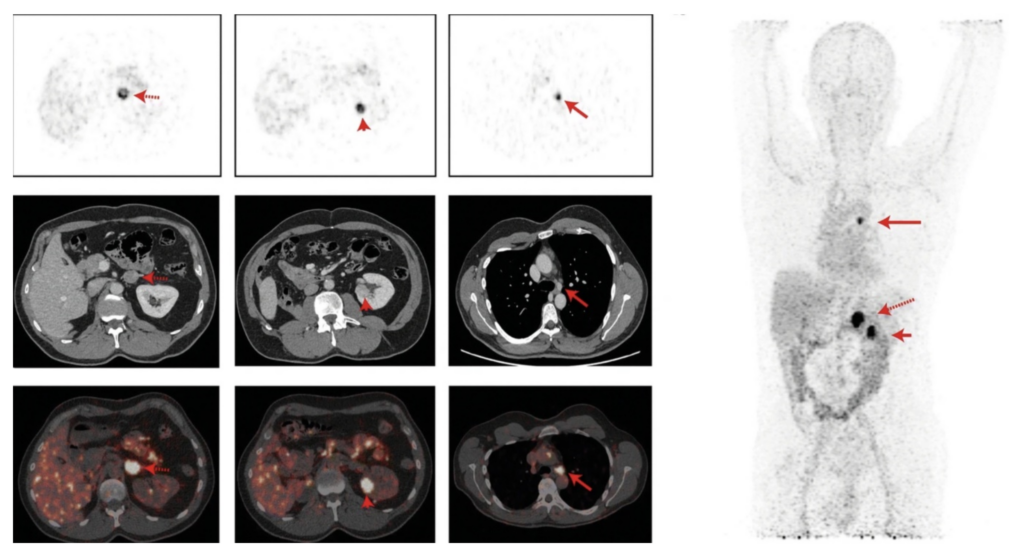
89Zr-girentuximab in renal cancer patient.
-
- Interferons
-
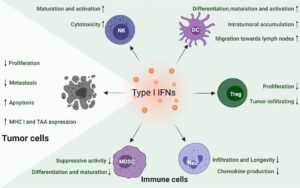
The effects of type I IFNs in the tumor microenvironment. Type I IFNs induce tumor cell apoptosis and inhibit tumor cell proliferation and metastasis. In addition, type I IFNs upregulate TAA and MHC I expression in tumor cells. Type I IFNs are essential for NK cell maturation and activation. Moreover, type I IFNs increase NK cell cytotoxicity. Type I IFNs promote DC differentiation, maturation, and migration into lymph nodes to activate CD8+ T cells. Moreover, type I IFNs increase DC intratumoral accumulation. Type I IFNs reduce Treg infiltration into tumor and Treg proliferation. Type I IFNs inhibit neutrophil infiltration, longevity, and chemokine production. In addition, type I IFNs decrease differentiation and maturation of MDSCs, and block their suppressive activity on CD8+ T cells. - `
-
- BCG Vaccine
-
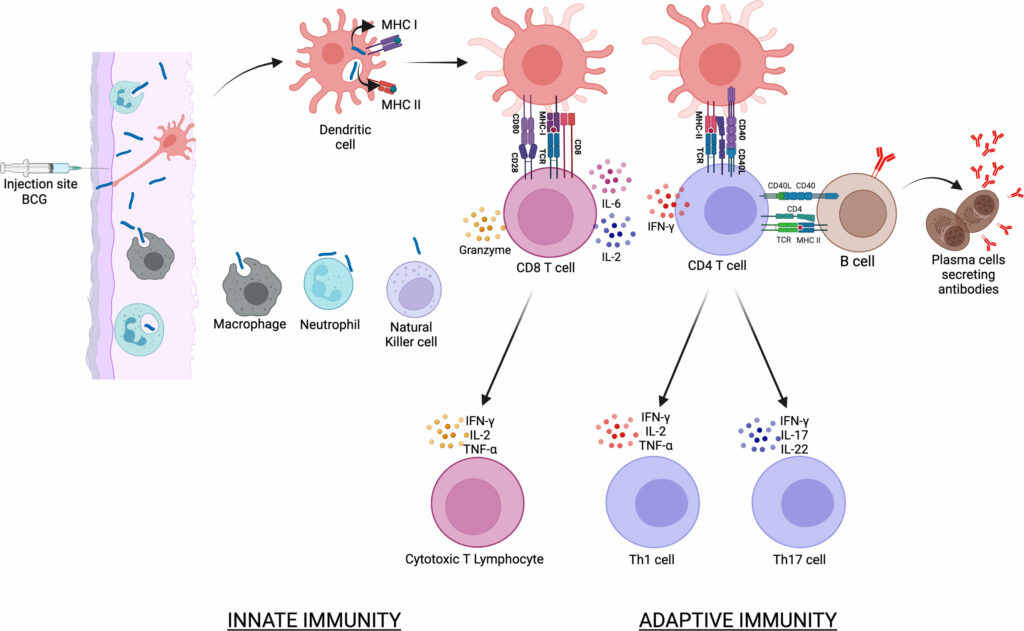
This figure illustrates the events that follow the intradermal injection of BCG. BCG is phagocytosed by various cells of the innate immune response that includes dendritic cells, macrophages and neutrophils. Dendritic cells are the main antigen presenting cells and BCG antigens are presented to CD4 via the MHC class II molecules and to CD8 T cells via the MHC class I molecules. This is followed by the activation of B cells, cytotoxic T lymphocytes and Th17 cells that collectively constitute the adaptive immune response to BCG vaccination. -
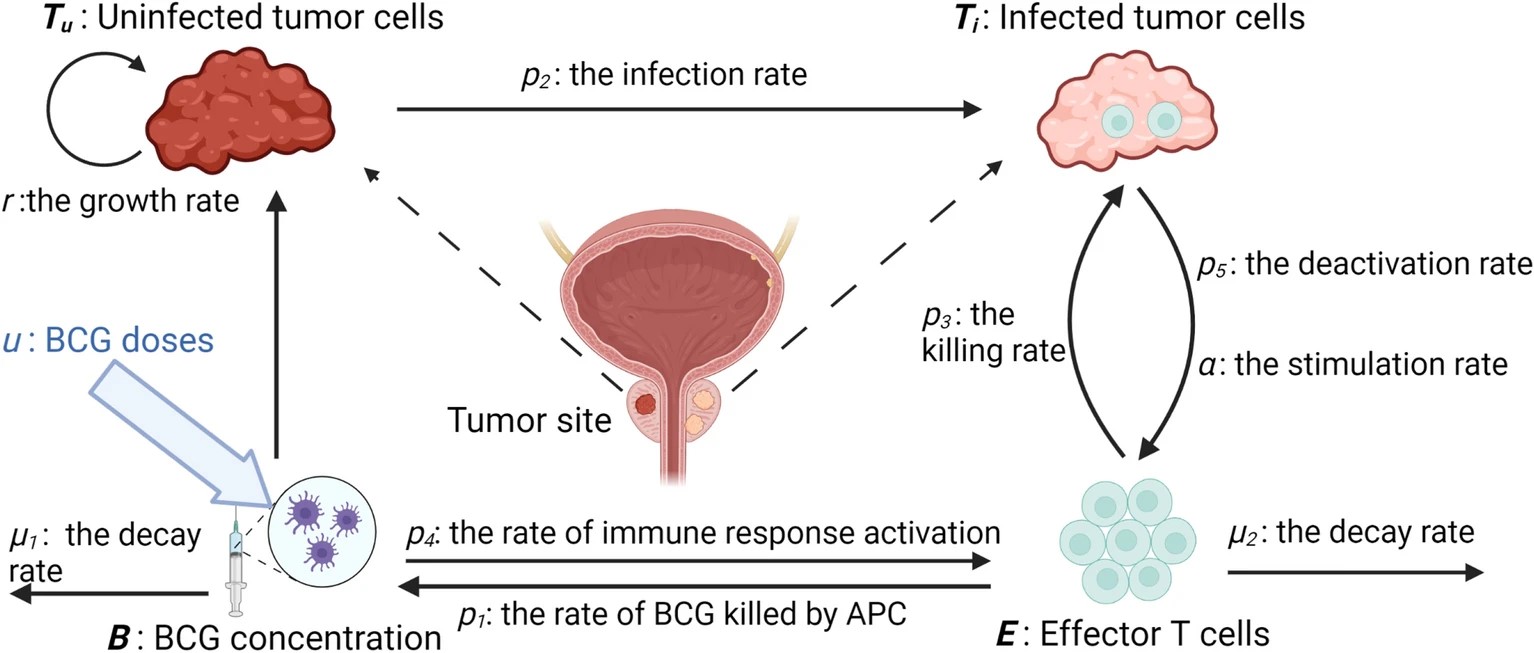
BCG treatment model for bladder cancer. BCG is instilled into tumor sites to bring uninfected tumor cells
to infected tumor cells
that will be eliminated by effector T cells E. -
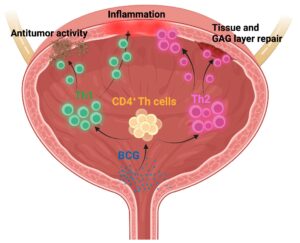
T helper (Th) cells in BCG-induced antitumor effects and bladder inflammation and repair. Intravesical application of BCG induces recruitment of CD4+ Th cells into the urothelium. A Th1-dominant bladder microenvironment is needed for an effective antitumor response. However, BCG-induced Th1-type inflammation also promotes cystitis. In contrast, Th2 T cells are required to repair the bladder wall and to restore the glycosaminglycan (GAG) layer
-
- Angiogenesis inhibitors
- Analgesics – not curative
-
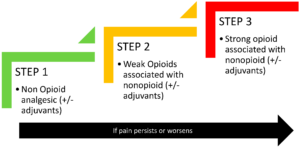
The WHO analgesic ladder for treating cancer pain.
-
- Surgery: laparoscopic, radiofrequency ablation,
- Adverse effects of Radiation
- Adverse effects of Chemotherapy
- Adverse effects of Surgery – scarring, possible permanent damage to surrounding lymph vessels (impeding lymph drainage -particularly with breast cancer) and surrounding tissue removal
- Skin Cancers
- Lung Cancer
- – Coughing that gets worse or doesn’t go away.
– Chest pain.
– Shortness of breath.
– Wheezing.
– Coughing up blood.
– Feeling very tired all the time.
– Weight loss with no known cause.
- – Coughing that gets worse or doesn’t go away.
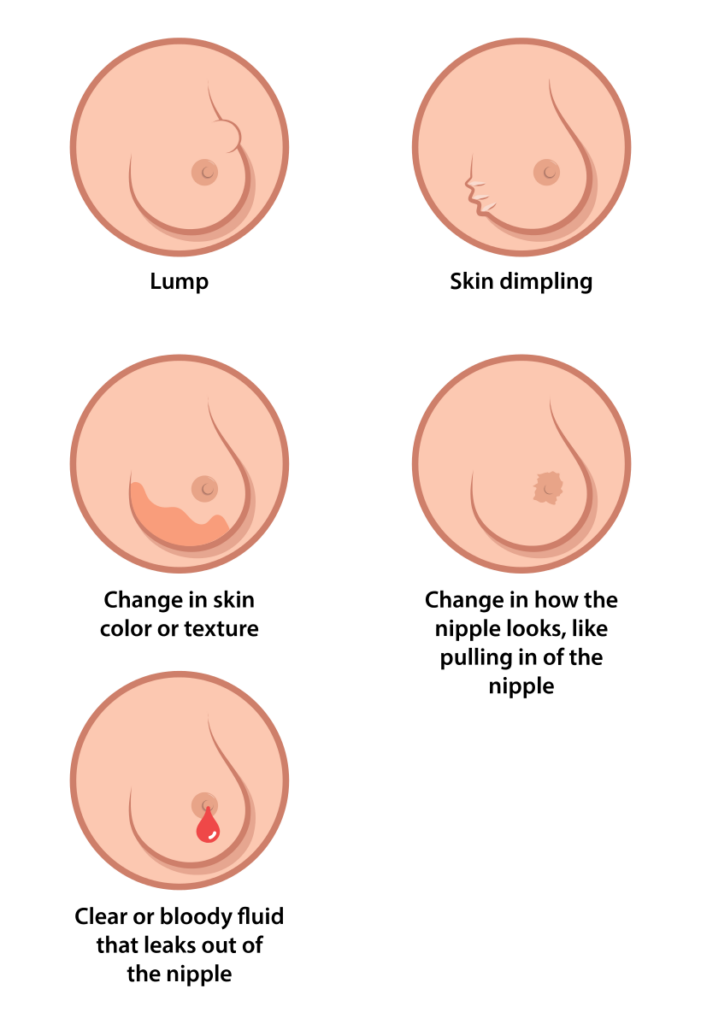
- Breast Cancer
- – New lump in the breast or underarm (armpit).
– Thickening or swelling of part of the breast.
– Irritation or dimpling of breast skin.
– Redness or flaky skin in the nipple area or the breast.
– Pulling in of the nipple or pain in the nipple area.
– Nipple discharge other than breast milk, including blood.
– Any change in the size or the shape of the breast.
– Pain in any area of the breast. - `
- – New lump in the breast or underarm (armpit).
- Cervical Cancer
- Ovarian Cancer
- – Vaginal bleeding (particularly if you are past menopause), or discharge from your vagina that is not normal for you.
– Pain or pressure in the pelvic area.
– Abdominal or back pain.
– Bloating.
– Feeling full too quickly, or difficulty eating.
– A change in your bathroom habits, such as more frequent or urgent need to urinate and/or constipation.
- – Vaginal bleeding (particularly if you are past menopause), or discharge from your vagina that is not normal for you.
- Benign Prostatic Hypertrophy
- Prostate Cancer
- – Difficulty starting urination.
– Weak or interrupted flow of urine.
– Frequent urination, especially at night.
– Difficulty emptying the bladder completely.
– Pain or burning during urination.
– Blood in the urine or semen.
– Pain in the back, hips, or pelvis that doesn’t go away.
– Painful ejaculation. - `
- `
- – Difficulty starting urination.
- Testicular Cancer
- – A lump or enlargement in either testicle
– A feeling of heaviness in the scrotum
– A dull ache in the abdomen or groin
– A sudden collection of fluid in the scrotum
– Pain or discomfort in a testicle or the scrotum
– Enlargement or tenderness of the breasts
– Back pain
- – A lump or enlargement in either testicle
*For diseases we discuss:
a) Basic Risk Factors
b) Most Common signs and symptoms
c) Basic Pathology, with basic diagnostic tools (e.g. imaging, blood tests) and basic treatment
Media Attributions
- Different cell types & differentiation © OpenStax is licensed under a CC BY (Attribution) license
- Outcome of S phase © Christinelmiller adapted by Tom Michaels; Matt Clark; Emily Hoover; Laura Irish; Alan Smith; and Emily Tepe is licensed under a CC BY-SA (Attribution ShareAlike) license
- A Schematic Diagram of DNA Replication © LibreTexts libraries is licensed under a CC BY-NC-SA (Attribution NonCommercial ShareAlike) license
- Relevance of telomere dysfunction to cellular aging hallmarks Telomere dysfunction can drive the hallmarks of cellular aging. © Deepavali Chakravarti, Kyle A. LaBella, Ronald A. DePinho is licensed under a CC BY (Attribution) license
- DNA damage © Alessandro Torgovnick, Björn Schumacher is licensed under a CC BY (Attribution) license
- The diagram displays the responses to reduced oxygenation within the tumor microenvironment. © Emami Nejad, A., Najafgholian, S., Rostami, A. et al. is licensed under a CC BY (Attribution) license
- An outline of the different causes of pain in patients surviving cancer © M. Brown and P. Farquhar-Smith is licensed under a CC BY (Attribution) license
- Signs of breast cancer including pains © Nazanin Derakshan, Joanne Taylor, Bethany Chapman and Bethany Chapman
- Breast cancer illustration © Raphseck is licensed under a CC BY (Attribution) license
- Integrative Physiology of Cancer Cachexia © Kenneth C.H. Fearon, David J. Glass, Denis C. Guttridge is licensed under a CC BY (Attribution) license
- Intratumoural morphological heterogeneity of breast cancer as a model for studying the mechanisms of tumour cell invasion. © Novikov, N.M., Zolotaryova, S.Y., Gautreau, A.M. is licensed under a CC BY (Attribution) license
- Lymphoma macro © Emmanuelm is licensed under a CC BY (Attribution) license
- Illustration of Laparoscopy © BruceBlaushttps://commons.wikimedia.org/wiki/User:BruceBlaus is licensed under a CC BY (Attribution) license
- Radiofrequency ablation © https://www.scientificanimations.com/ is licensed under a CC BY-SA (Attribution ShareAlike) license
- Development and Elimination of Cancer Cells as Chemotherapy is Applied © IdkItsKatieB is licensed under a CC BY-SA (Attribution ShareAlike) license
- Diagram showing how you have chemotherapy into the abdomen © Cancer Research UK is licensed under a CC BY-SA (Attribution ShareAlike) license
- Side Effects of Chemotherapy © Halycon is licensed under a CC0 (Creative Commons Zero) license
- Effects of the TNBC secretome. Protein factors secreted by TNBC cells and tumors regulate cancer-promoting processes © Helen H.W. Chen and Macus Tien Kuo is licensed under a CC BY-SA (Attribution ShareAlike) license
- By placing the radioactive source inside the body, brachytherapy can target tumors more directly than external beam radiotherapy © Cancer Research UK is licensed under a CC BY-SA (Attribution ShareAlike) license
- cobalt-60 machine © Petrucci et al. is licensed under a CC BY-NC-SA (Attribution NonCommercial ShareAlike) license
- The HPA axis integrates internal and external cues to modulate glucocorticoid production. © Khadka S, Druffner SR, Duncan BC and Busada JT is licensed under a CC BY (Attribution) license
- The effects of glucocorticoids change over the course of tumor development. © Khadka S, Druffner SR, Duncan BC and Busada JT is licensed under a CC BY (Attribution) license
- Hormonal therapy in prostate cancer. © Xiaoyu Hou, Thomas W. Flaig is licensed under a CC BY (Attribution) license
- GnRH Agonist Mode of Action in Pre-Menopausal Breast Cancer. is licensed under a CC BY (Attribution) license
- 89Zr-girentuximab in renal cancer patient. © Parakh S, Lee ST, Gan HK, Scott AM. is licensed under a CC BY (Attribution) license
- The effects of type I IFNs in the tumor microenvironment. © Yu, R., Zhu, B. & Chen, D. is licensed under a CC BY (Attribution) license
- Events that follow the intradermal injection of BCG © Singh S, Saavedra-Avila NA, Tiwari S and Porcelli SA is licensed under a CC BY (Attribution) license
- T helper (Th) cells in BCG-induced antitumor effects and bladder inflammation and repair. © Pichler R, Stäblein J, Mari A, Afferi L, D’Andrea D, Marcq G, del Giudice F, Soria F, Caño-Velasco J, Subiela JD, et al. is licensed under a CC BY (Attribution) license
- The WHO analgesic ladder for treating cancer pain. © Mestdagh F, Steyaert A, Lavand’homme P. is licensed under a CC BY (Attribution) license

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}