Chapter 10 Selected Diseases and Disorders of the Digestive System
Chapter 10 Digestive System Diseases and Disorders – Darrek
Zoë Soon and Darrek Kniffen
Creative Commons – Simple Pictures, Images, Video Clips, and/or Gifs that help illustrate any of the following:
*For diseases we discuss:
a) Basic Risk Factors
b) Most Common signs and symptoms
c) Basic Pathology, with basic diagnostic tools (e.g. imaging, blood tests) and basic treatment
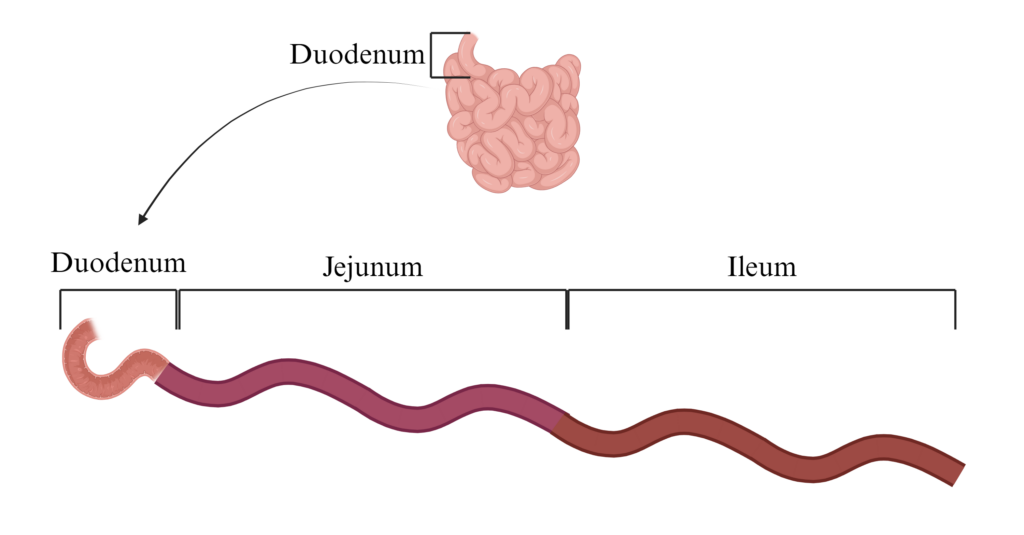
Basics (anatomy and physiology of the GI tract)
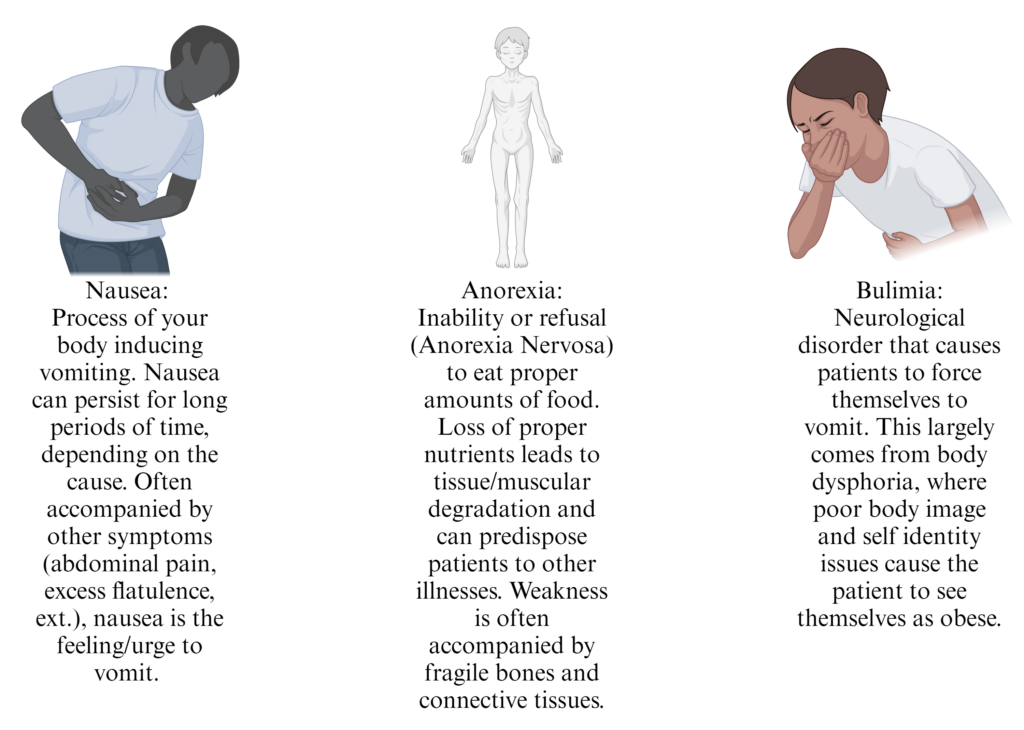
- Definitions – Nausea, Vomiting (emesis), Anorexia (loss of appetite), Anorexia Nervosa, Bulimia
- Vomiting/Emetic Reflex Center – medulla oblongata
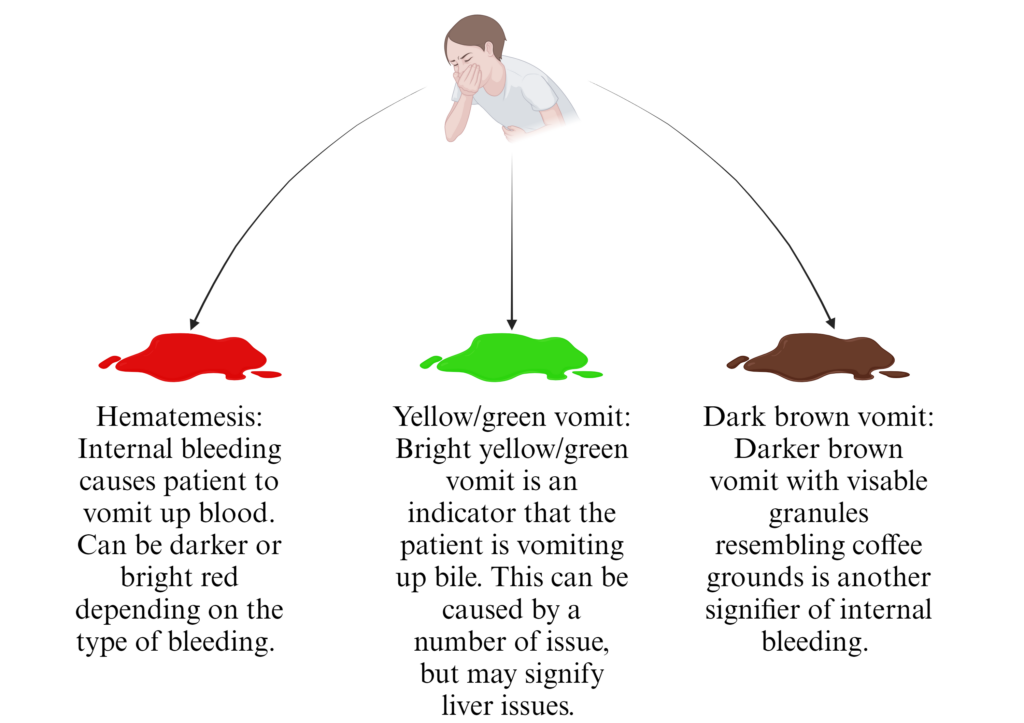
- Vomit Chararcteristics: hematemesis, yellow/green vomitus, deep brown vomitus, recurrent vomiting
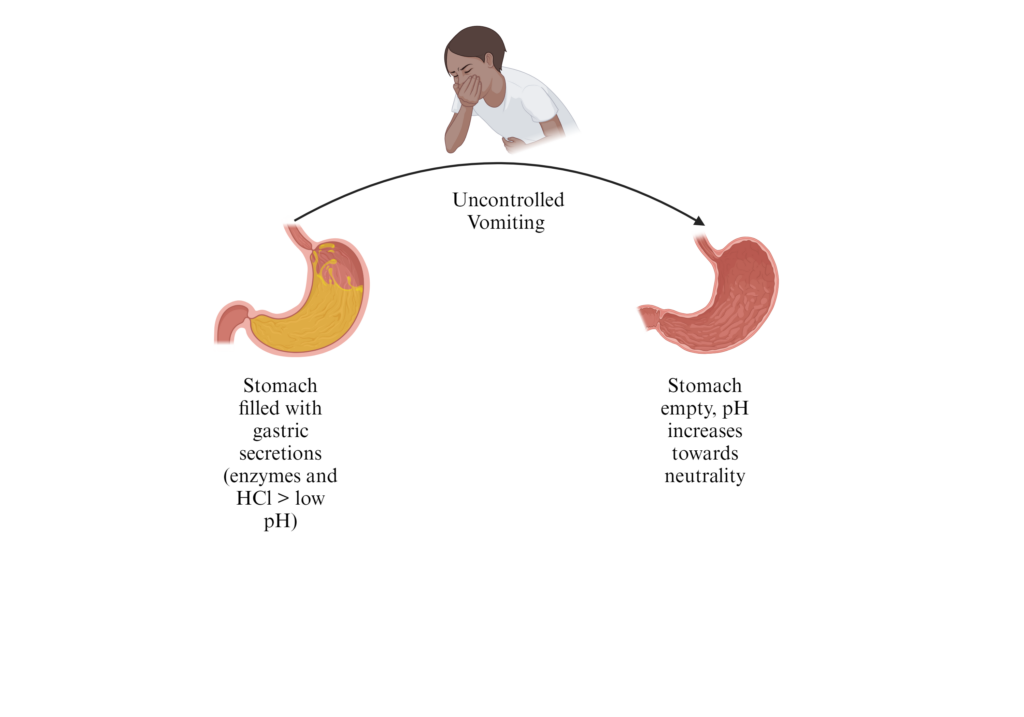
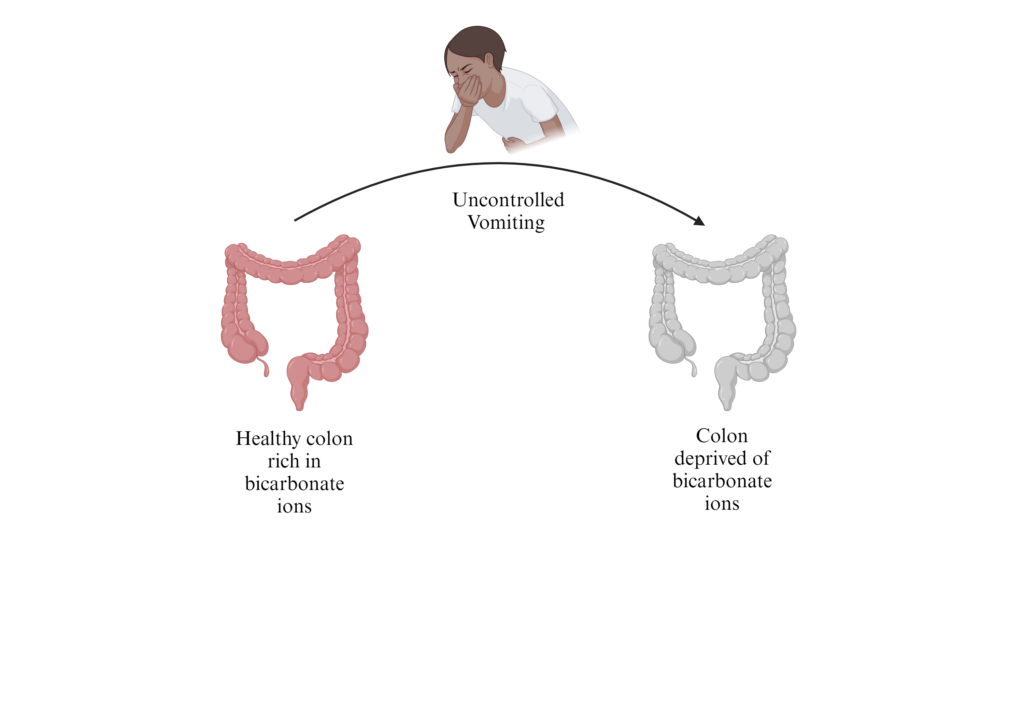
- Vomiting can cause metabolic alkalosis due to loss of gastric HCl
Risk factors for severe HCl depletion that can lead to metabolic acidosis include infection/disease(cancer), mental illness (Bulimia), toxin ingestion, narcotic withdrawal, and pregnancy. Metabolic acidosis can lead to degradation of muscle tissue which, in extreme cases, can lead to blockages of the kidney and multi-organ failure in the patient. - Severe vomiting can cause metabolic acidosis due to loss of intestinal bicarbonate
Possible damage caused by Bulimia – damage to oral mucosa, teeth, esophagus, contipation, diarrhea, electrolyte/nutritional imbalances - Diarrhea Characteristics: Small volume associated with inflammatory bowel disease; Large volume associated with intestinal infection (e.g. Cholera) or lactose intolerance; Steatorrhea associated with celiac disease and cystic fibrosis – characteristic of malabsorption syndromes
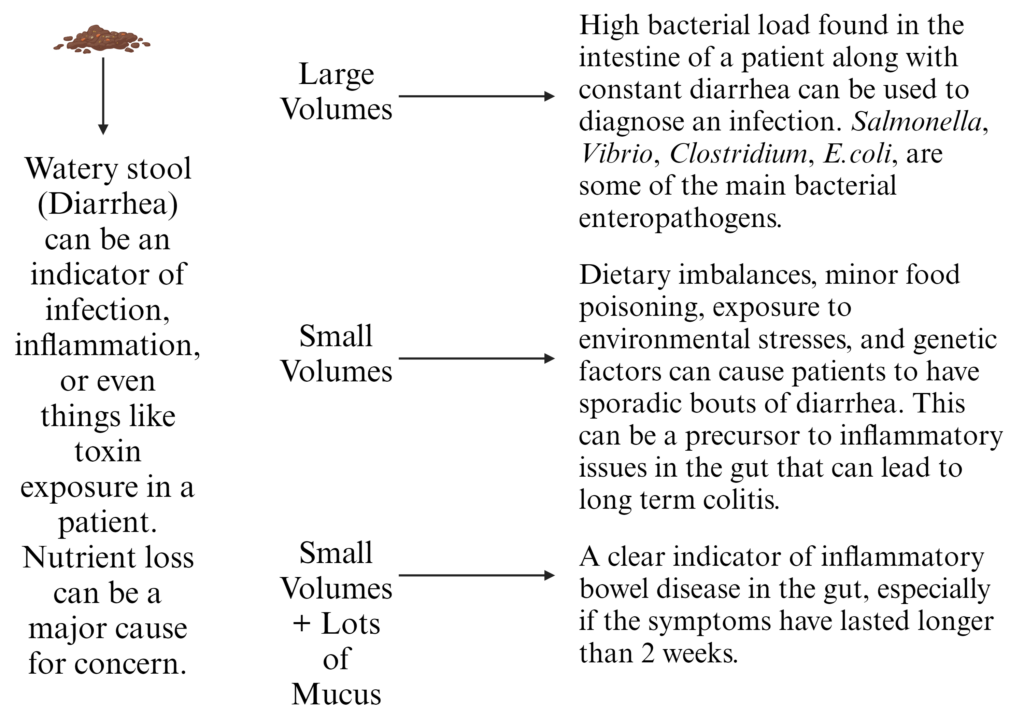
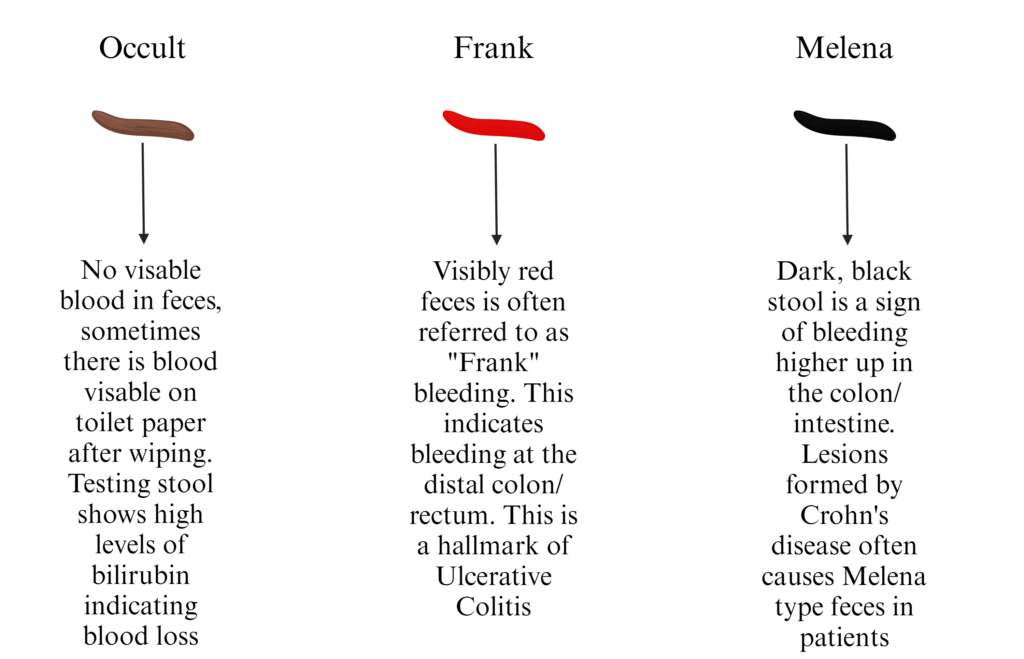
Can be caused by diet disturbances (new foods can cause shifts in the function and diversity of our microbiota), drugs (antibiotics, antacids, laxatives, ext.), toxin exposure, disease (IBS/IBD, cancer, ext.), infection (Salmonella, Cholera, Clostridium) - Feces Blood: Frank, Occult or Melena – associated with lesions in the GI tract
The “type” of blood found in fecal samples from patients can indicate where and what type of bleeding is occurring. This can be crucial in aiding physicians in positively diagnosing a patient with a gastrointestinal illness.
- Definitions: Eructation (burp); Borborygmus (rumbling) – associated with excess gas
- Acute/Chronic Constipation – associated with lack of dietary fiber, inadequate fluid intake, GI muscle or neural issues, obstructions (tumors/strictures) – can cause hemorrhoids, anal fissures, diverticulosis
- Excessive loss of fluid from vomiting/diarrhea – can cause hypovolemia, intracellular dehydration, organ failure
-
Achalasia – Failure of LES to relax because of missing or damaged esophageal nerves.
causes ↓ esophageal muscle activity (peristalsis); harder to swallow fluids
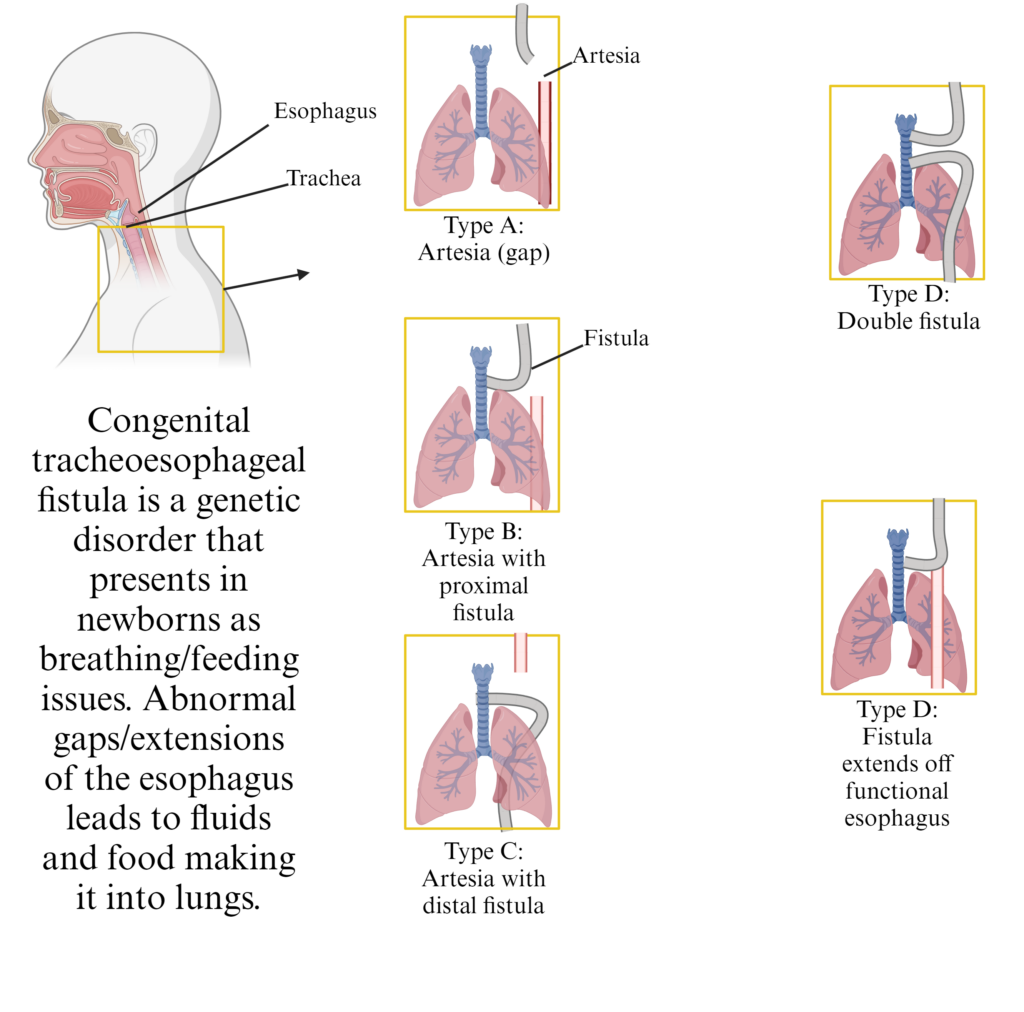
- Congenital Esophageal Atresia and Congenital tacheoesophageal fistula
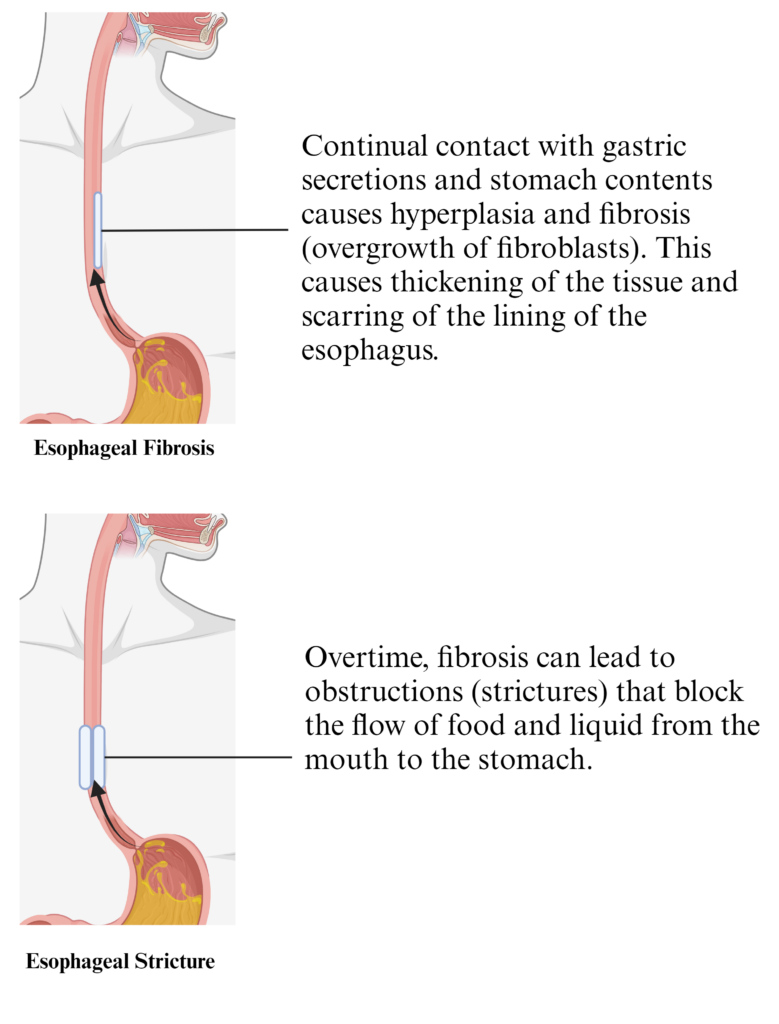
- Esophageal fibrosis and strictures
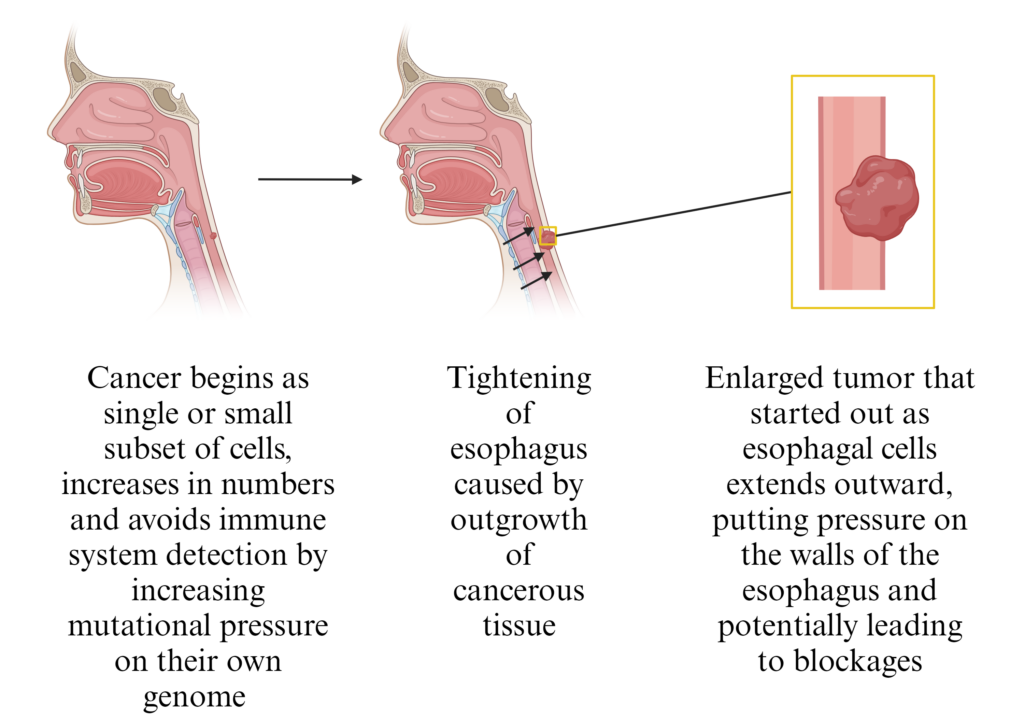
- Tumor causing esophageal narrowing
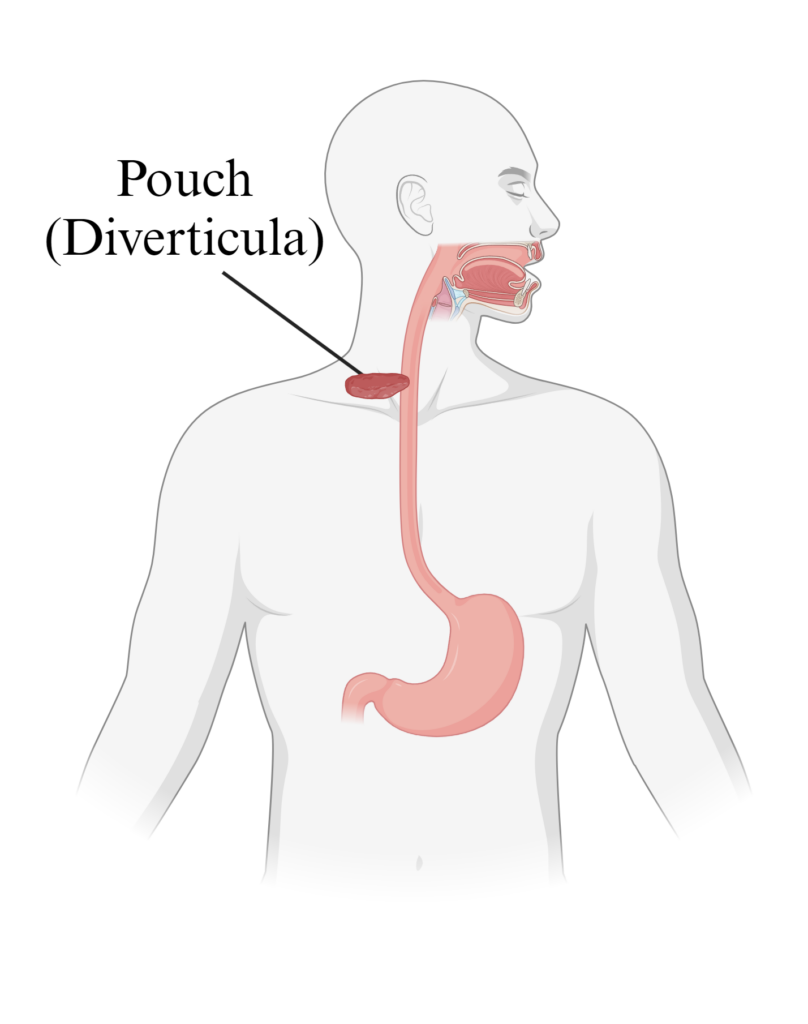
- Esophageal Diverticulum
- Sliding Hiatal Hernia
- Rolling/Paraesophageal Hernia
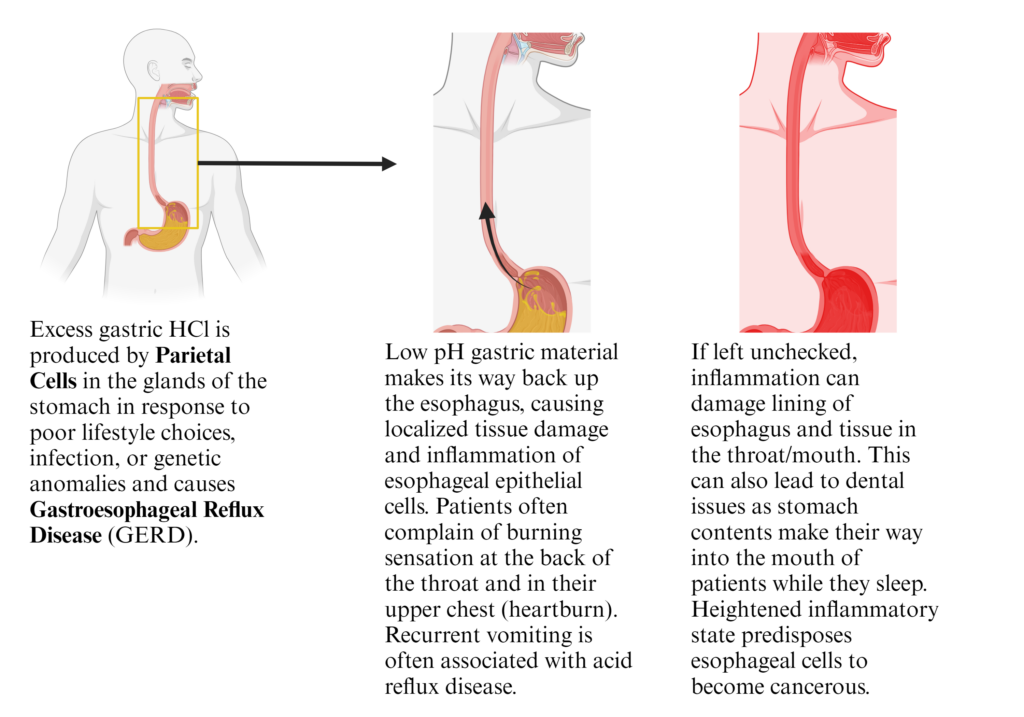
- Gastroesophageal Reflux Disease (GERD)
- Esophageal manometer
- Esophageal Catheter monitoring pH
- Barrett’s Esophagus
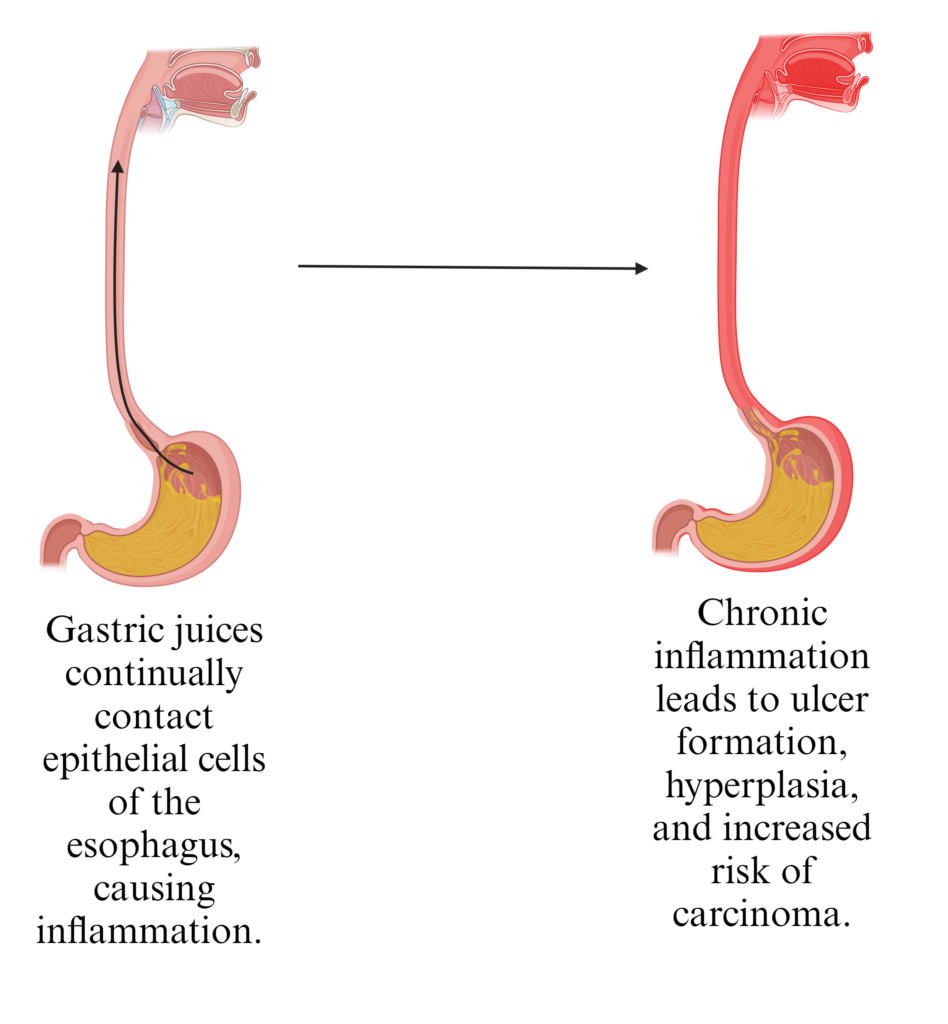
Caused by long-term exposure of the esophagus to low pH of the stomach contents from acid reflux. Endoscopy presents reddening of the tissue lining the throat. This puts patients at an increased risk of developing cancer. - Peptic Ulcers, H. Pylori bacterium
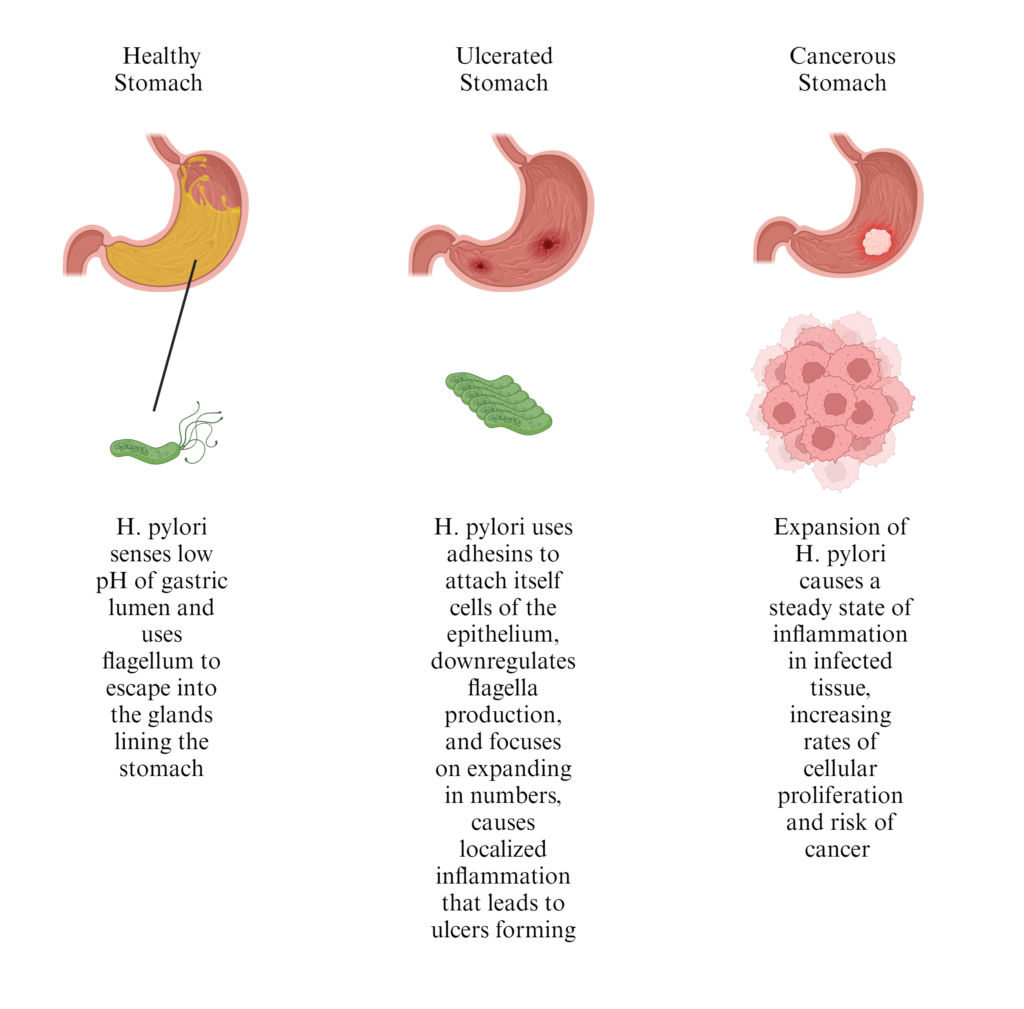
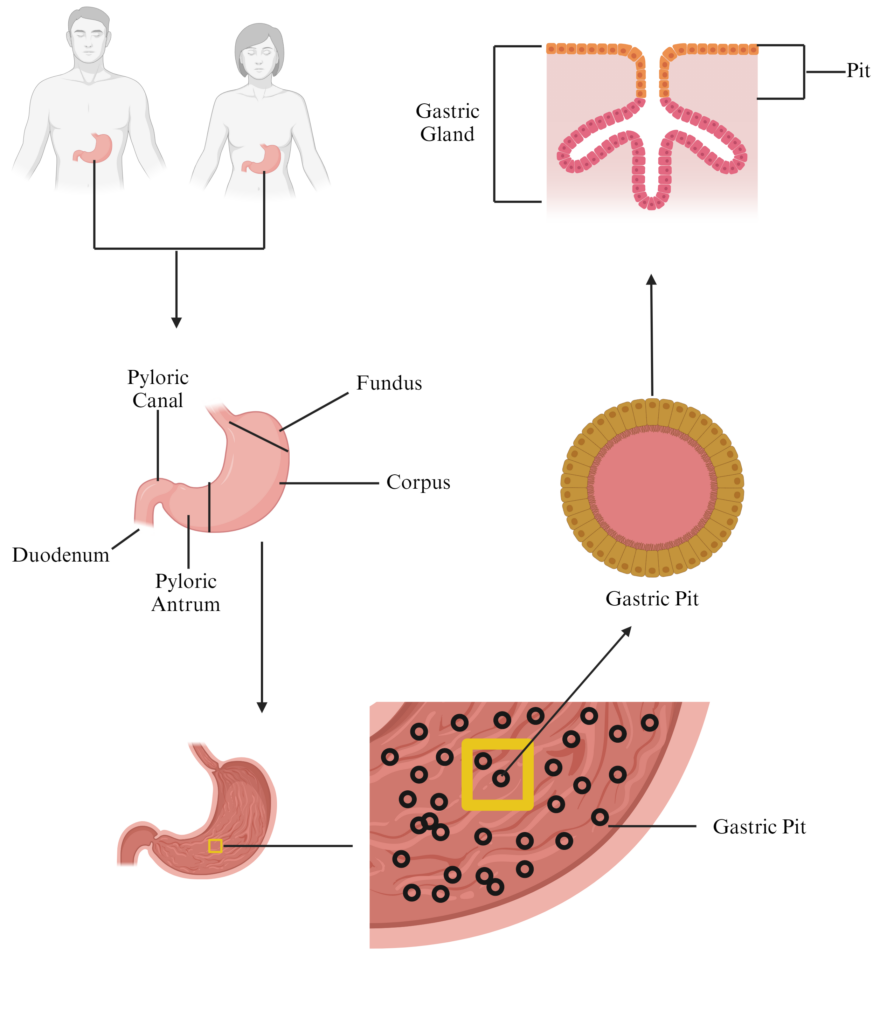
Peptic ulcers were long thought to be solely caused by lifestyle and diet. Alcohol and consumption of spicy, salty foods where continually sourced as the root cause of stomach ulcers. These painful sores can lead to bleeding in the stomach which causes vomiting and nausea. In severe cases, peptic ulcers can cause degradation of the stomach lining and allow acid/lumenal contents to leak out of the stomach. Peptic ulcers can also lead to cancer due to the tumorigenic potential of ulcers (cells residing in and around the ulcer are in a constant state of inflammation). Barry Marshall is a clinical researcher and physician who started to notice a common factor in biopsies taken from patients with peptic ulcers, a bacteria known as Helicobacter pylori. Because the common thinking was that no bacteria could survive and much less colonize the harsh environment of the human stomach, it was hard to get acceptance from his colleagues. This lead him to do something that no ethics board would be happy with seeing, infecting himself with the bacteria and assessing its ability to cause gastric ulcers. He made sure to eat a healthy diet before and during the experiment to help prove his idea. Endoscopy of his stomach before he drank an overgrown liquid broth of H. pylori showed he had no ulcers whatsoever. Following his ingestion of the bacteria, he developed ulcers and was able to cure them by taking antibiotics that targeted the bacteria. Cultures grown from scrapings of his stomach lining were positive for H. pylori. This proved the hypothesis, that peptic ulcers in humans can be caused by H. pylori; he also revolutionized our understanding of the stomach as a reservoir for bacterial colonization. We now know there is a diverse community that inhabits the human stomach and it is, in part, thanks to the sacrifices of Dr. Marshall.
H. pylori as a pathogen:
It is now approximated that roughly half the global population may be infected with a strain of H. pylori. The bacteria is able to utilize the glands of the human antrum as a niche for its survival and expansion due to the protective nature of the gastric mucin that is secreted by foveolar (mucus producing) cells. By utilizing chemosensing pathways the bacteria is able to move from areas of higher pH (lumen of the stomach, pH ~3.5) to areas of lower pH (gastric glands, pH ~7.4) Adhesins allow the bacteria to firmly attach to cells lining the glands and they can then secrete effector proteins capable of modulating numerous host cell factors including the production of mucus and inflammatory compounds such as interleukins. Interestingly, a specific sugar residue (glycan) on gastric mucus seems to be extremely bactericidal towards H. pylori. Glycoproteins containing a terminal alpha 1,4 N-Acetylglucosamine residue inhibit an essential pathway for H. pylori growth and can infer tolerance or even total resistance towards infection with the bacteria. - Bile Stones
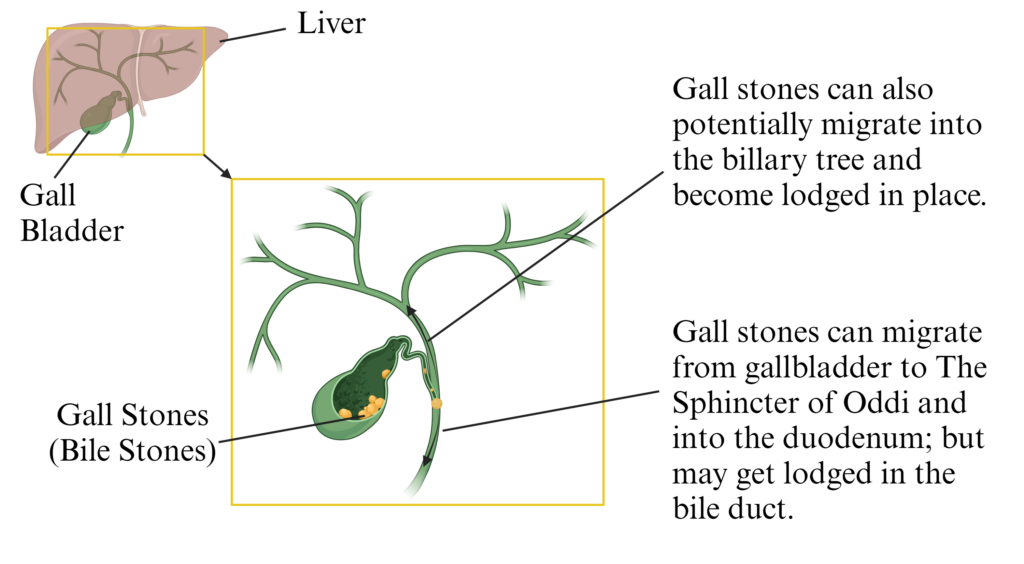
- Prehepatic Juandice – caused by hemolytic anemias (e.g. Sickle Cell Anemia) or transfusion reactions
- Intrahepatic Jaundice – causes by Hepatitis virus infection or Alcohol damage (cirrhosis)
- Posthepatic Jaundice – caused by gallstone blockages or tumors
- Types of cirrhosis (irreversible liver damage) – alcohol, gallstones, toxins, genetic metabolic disorders
- 3 Stages of Liver Disease/Damage – Fatty Liver, Hepatitis, End-Stage Cirrhosis
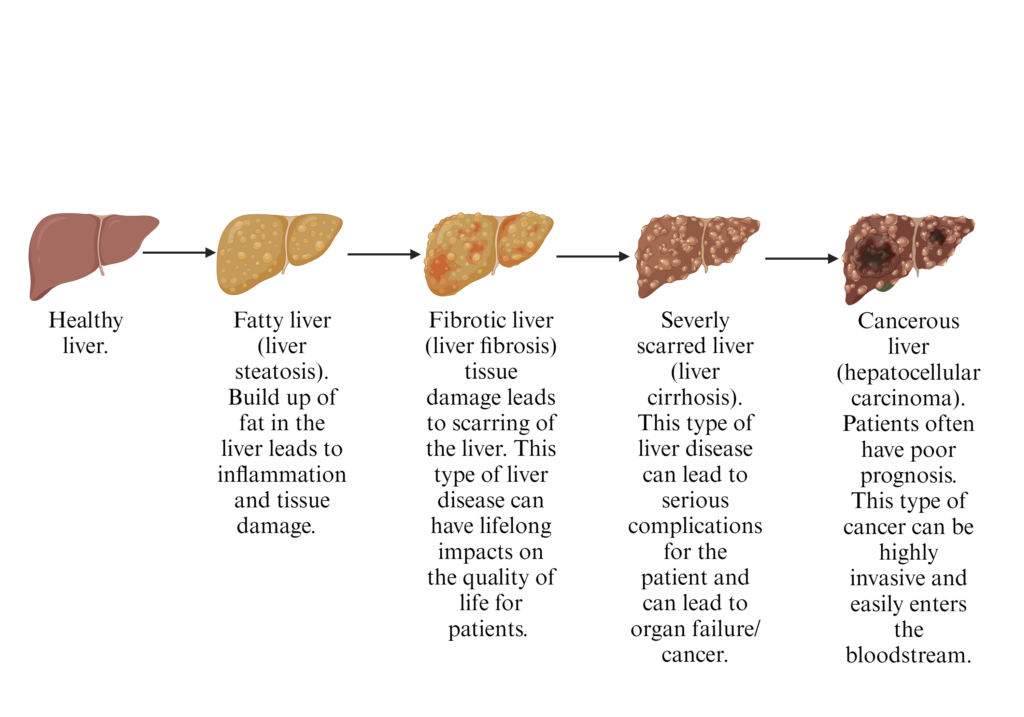
- Signs & Symptoms of Cirrhosis – ascites, portal hypertension, splenomegaly, esophageal varices, jaundice, encephalopathy, reduced healing, spider nevi, increased bruising, edema, ammenorrhea (in adult pre-menopausal females), anroexia, nausae, gynecomastia (in males)
- Portocaval shunts
- Celiac Disease
-
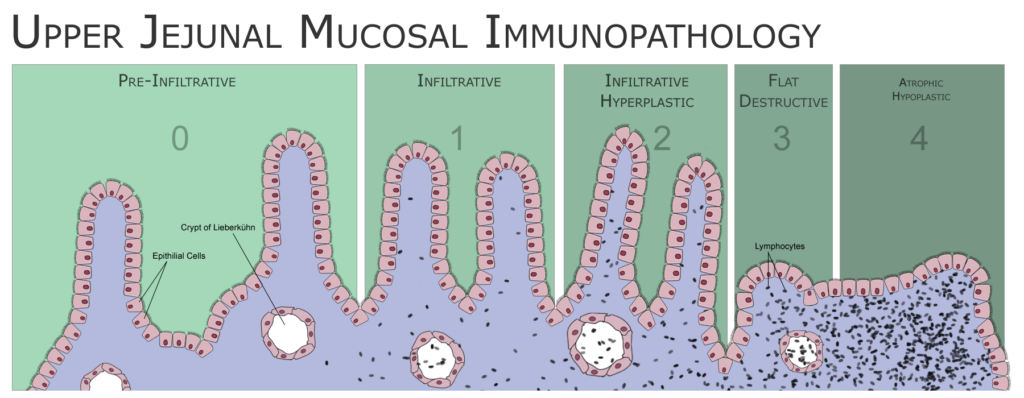
Diagram to show the different stages of Coeliac Disease - Irritable Bowel Syndrome (IBS)
IBS presents itself as a mild to severe illness that can be chronic or acute. Antibiotic use has been closely tied to incidences of IBS due to the negative impacts it can have on the resident microbiota. Patients usually present with lose watery stools, difficulty passing bowel movements, cramping in the lower abdomen, and other symptoms likely tied to loss of proper absorptive properties in the ileum and colon. Neurological symptoms, such as disruption to sleep patterns and increased anxiety have also been linked to IBS due to the loss of important electrolytes. Treatments normally focus on restoring a healthy resident microbiota and fecal transplants from healthy donors have proven very successful in providing a long-term treatment. - Inflammatory Bowel Disease (IBD)
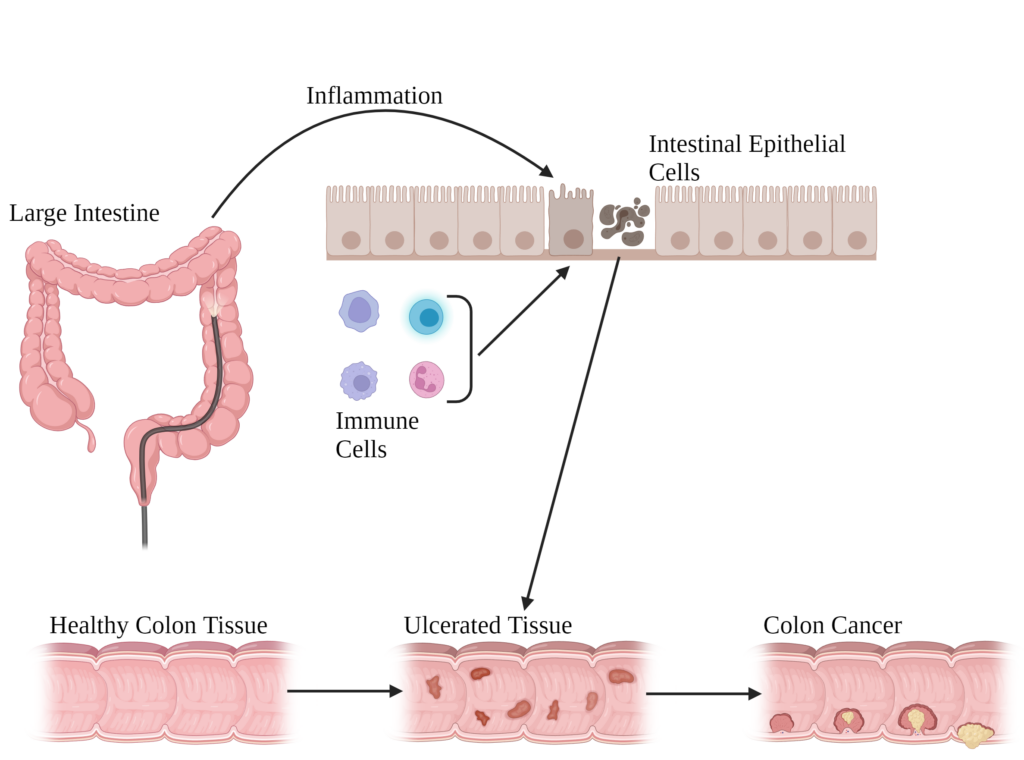
Broad diagnosis that encompasses multiple diseases in the lower GI tract of humans. Characterized by increased and dysbiotic inflammation that leads to cell necrosis and uncontrolled rates of proliferation (mitosis). Clinical symptoms can range from loss of apatite, nausea, diarrhea, bloody stool, and fecal bacterial presence in the blood. A fecal protein concentration of 40ug/g of Calprotectin (neutrophil granule) is often used as a positive diagnosis of IBD, standard practice is to also conduct a colonoscopy and collect biopsies for further analysis. Uncontrolled cell proliferation is also a hall-mark of cancer, which puts patients who have been positively diagnosed with IBD at an increased rate of developing carcinomas. Colonoscopy of patients in active disease status present increased granulation and hyperplasia of the intestinal walls. Two of the main forms of IBD are Crohn’s Disease and Ulcerative Colitis. Recent evidence suggests that loss of the mucus barrier layer, alterations to host immune response, and activity of bacterial commensal microbes play harmonious roles in driving disease pathology. Risk factors include lifestyle, diet, geographic area, environmental toxin/microbe exposure, and genetics. Some taxa of bacteria and fungi may play key roles in development of disease in patients by altering the composition and diversity of microbes in the gut. - Crohn’s Disease (CD)
Patchy inflammation, can be impact tissue anywhere on body but most commonly associated with small intestine (ileum) and colon. Lesions form in the walls of the gut, extending past the surface of the mucosa (mucus associated tissue, includes the lamina propria) and penetrating into the serosa (muscle tissue) surrounding the small/large intestine. Creeping fat (remodeling of the mesentery to form a “band aid” around tissue) is a hall-mark of CD and is likely driven by the activity of M2 macrophages which express Fibroblast Growth Factor (FGF). Mesenteric adipose tissue contains many lymphoid follicles (enriched for T-cells and B-cells) which increases the amount of immune cell infiltration in the tissue. CD is a chronic progressive illness that can impact people at any point in their lives. Critically, CD can lead to leaking of lumenal contents into the peritoneal cavity, causing life threatening sepsis as bacteria translocate into the bloodstream and infect other organs/tissues. Stricturing disease, where overgrowth of fibroblasts leads to twisting and tightening of the intestine lumen, can lead to blockages that require surgery. Patients often go through phases of active disease status and remission, due to this heterogeneity treatments have remained elusive. Many patients with CD can control their symptoms by carefully regulating their diet and lifestyle. - Ulcerative Colitis (UC)
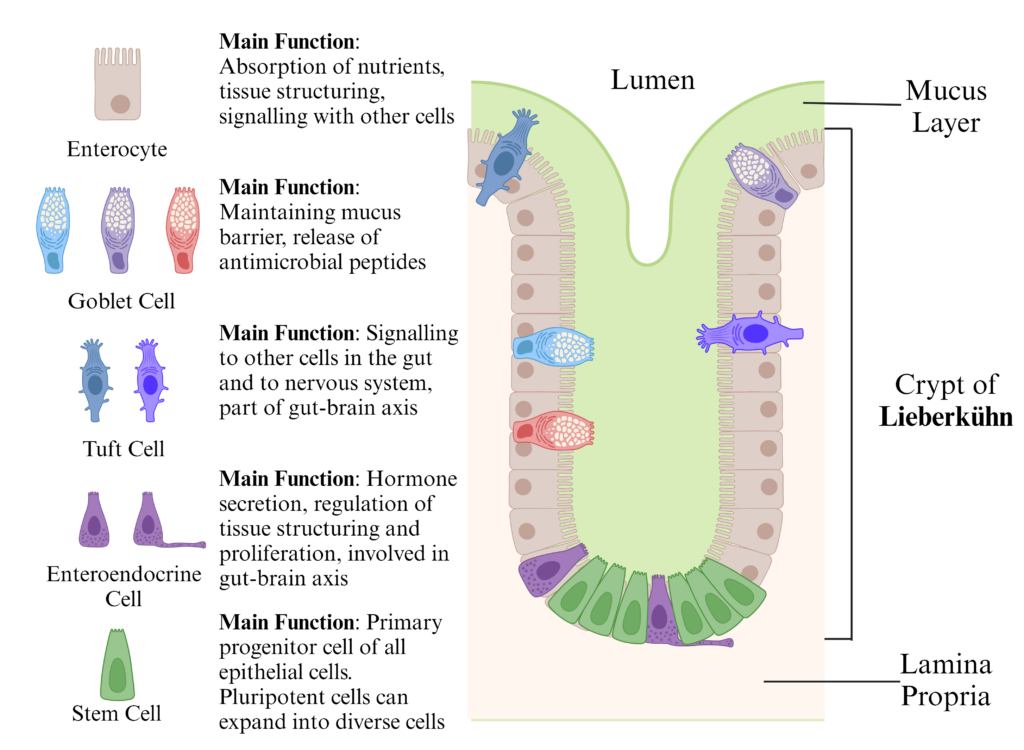
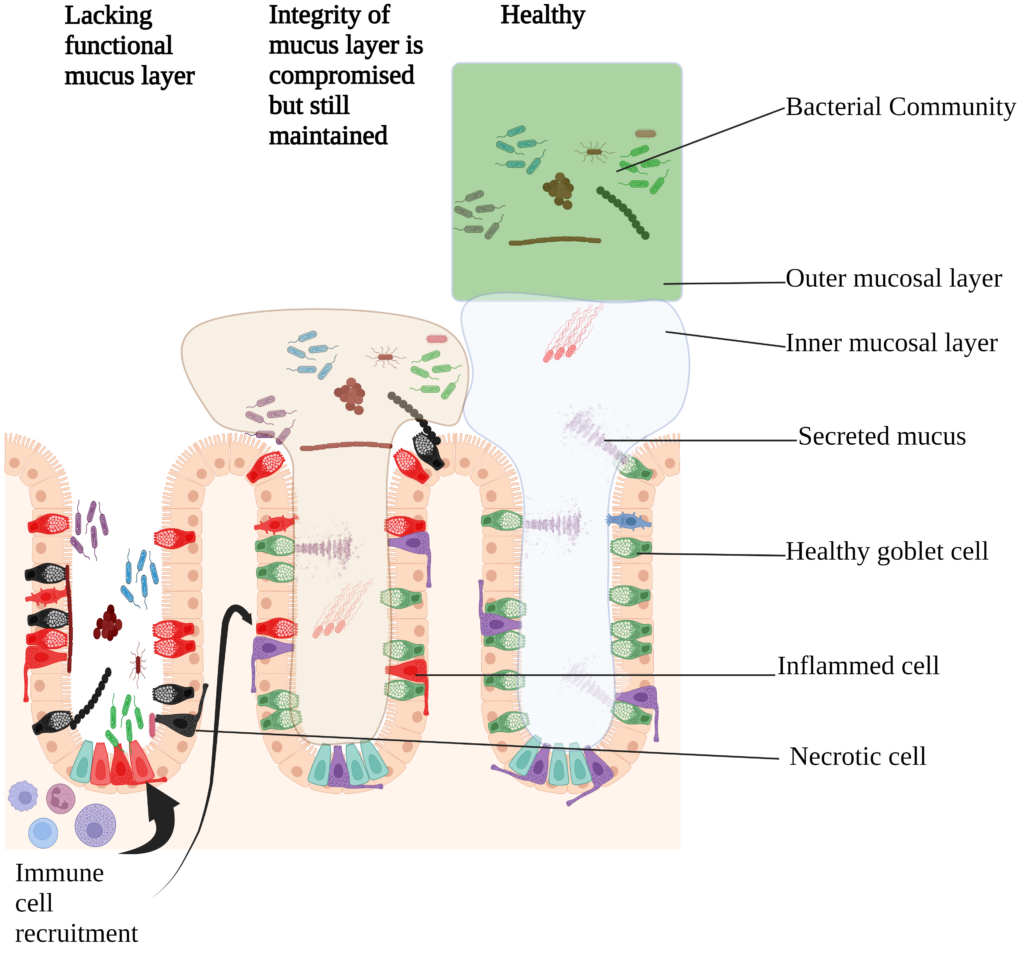
Continuous inflammation, normally starts at distal end (sigmoid) of colon/rectum. Inflammation does not extend past mucosa and largely impacts epithelium, causes bleeding and loss of proper absorption in affected tissue which can lead to malnourishment. Blood samples of UC patients show increased levels of C-reactive protein. Loss of goblet cells and increased rates of cell proliferation leads to a loss of the barrier layer that protect host cells from their microbiota. Direct contact with bacteria and other microbes causes inflammatory signals to be created in the form of cytokines, which recruit immune cells to the site of inflammation. Pro-inflammatory immune cells damage the cells of the epithelium and recruit more immune cells in the process which creates a positive feedback loop. Continual damage of the epithelium leads to genetic alterations in the cells and eventually cancer. The only cure with a 100% success rate is to fully remove the colon before cancer begins to develop. Unfortunately there is a disease known as pouchitis that can develop in people who had their colon removed which shares many similarities to UC and can lead to removal of the ileum as well as the colon. - Discontinuous Colitis (DC)
Occurs in tissue that was left in patients after surgical removal of an upper portion of the GI tract. A common example is in patients who have undergone a full colectomy, often times the rectum is left intact but the top portion is closed off. The tissue in the rectum can become inflamed post-surgery and begin to pass blood and mucus. This can often be treated by re-connecting the rectum to the small intestine and allowing the passage of fecal material, which seems to have an anti-inflammatory affect. - Microscopic Colitis (MC)
Characterized by watery stools, nutrient deficiencies due to loss of proper colonic absorption function, and painful cramping in the lower abdomen. Patients with MC do not test positive for any known pathogens and often go through long periods of acute symptoms. Colonoscopy doesn’t reveal the normal patterns associated with IBD (hyperplasia, granulation, edema, hypervesiculation), it is only be taking a biopsy of colon tissue and examining it under a microscope that a positive diagnosis can be confirmed. - Colorectal Carcinoma
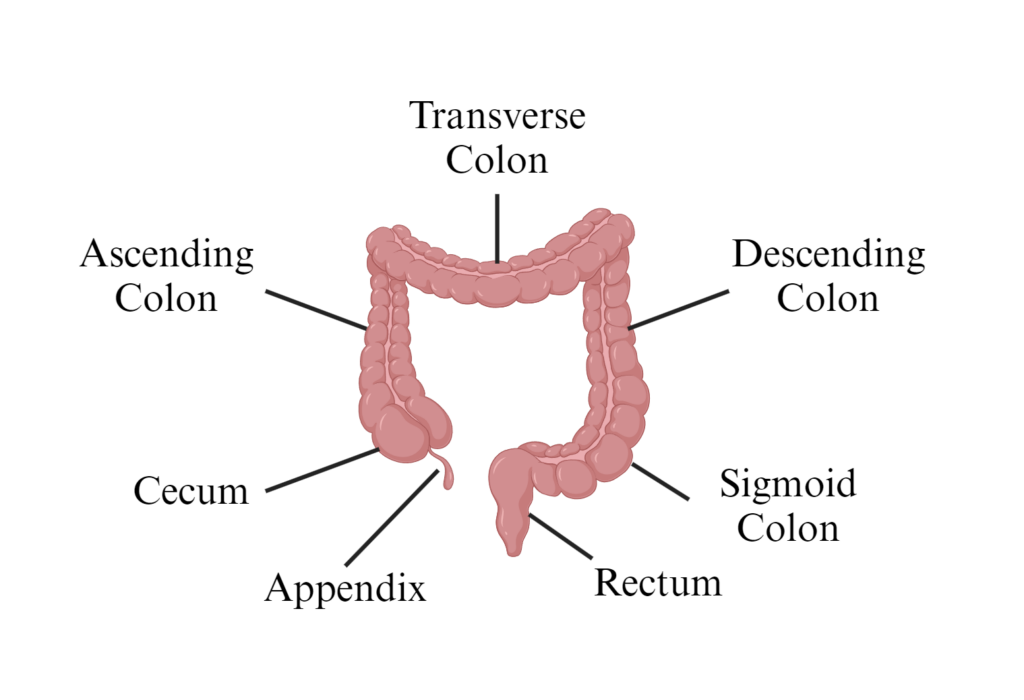
Cancer that has formed in the colon/rectum of a patient. Many different stimuli are thought to be potential instigators of carcinoma formation in the gut. Due to the nature of the colonic environment, epithelial cells are constantly in contact with a rich variety of compounds, toxins, and other organisms. Viruses, fungi, bacteria, parasites, these living things secrete and excrete compounds that can have direct or indirectly carcinogenic properties. Inflammation and the activity of stem cells can lead to cancer as well, this can be spontaneous and is often influenced by the genome/epigenome of the patient. Humans are also likely to come into contact with synthetic toxins in our food and workplaces that can make their way into our gut and cause cancerous tissues to form. - Appendicitis
Inflammation of the appendix (attached to the cecum), causes painful swelling and increased lymphatic infiltrate into the proximal colon and terminal ileum. Severe cases can lead to extreme localized edema and rupturing of the appendix which exposes the peritoneal cavity to bacterial sepsis. Diagnosis is often confirmed via ultrasound, antibiotics and steroids can be used to treat underlying infection and lower the inflammatory response. Uncontrolled inflammation of the appendix can lead to removal of the tissue from the patient.
Media Attributions
- DK-Stomach
- DK-glands and crypts2
- DK-Colon cell types
- DK-colon
- DK-Small intestine © Didn't not the author thatURL because there's a lot of authors there
- DK-Nausea and vomiting
- DK-Types of vomit (2)
- DK-Acid stomach
- DK-Bicarbonate
- DK-waterystool
- DK-Blood in feces types
- DK-CTF (2)
- DK-Esophagus fibrosis
- DK-esophageal cancer
- DK-Esophageal Diverticulum
- DK-Gastroesophageal Reflux Disease
- DK-Barrets
- Untitled (11)
- DK-Bilestones
- DK-Types of liver disease
- Celiac Disease © WikipedianProlific is licensed under a CC BY-SA (Attribution ShareAlike) license
- DK-Gut inflammation
- DK-Mucus and IBD

{kind=link}