Chapter 7 Selected Diseases and Disorders of the Cardiovascular System
Chapter 7 Cardiovascular Diseases and Disorders – Shirley
Zoë Soon and Sijie (Shirley) Yang
Creative Commons – Simple Pictures, Images, Video Clips, and/or Gifs that help illustrate any of the following:
*For diseases we discuss:
a) Basic Risk Factors
b) Most Common signs and symptoms
c) Basic Pathology, with basic diagnostic tools (e.g. imaging, blood tests) and basic treatment
- Review of Cardiovascular System Anatomy
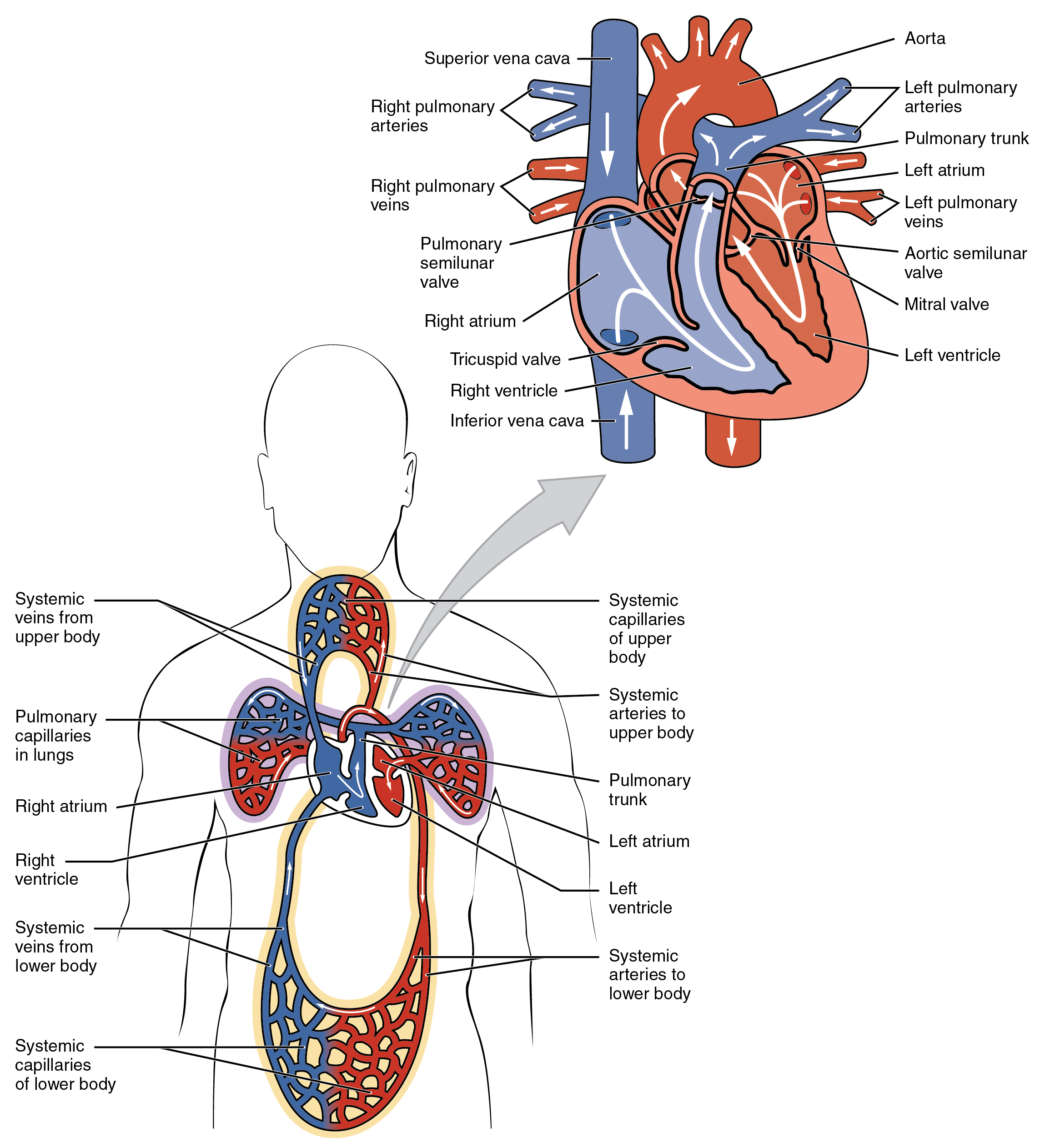
- (1) Dual System of Human Circulation: Pulmonary Circulation and Systemic Circulation
- (2) Systemic Blood Flow During Rest, Mild Exercise, and Maximal Exercise in a Healthy Young Individual
Organ Resting
(mL/min)Mild exercise
(mL/min)Maximal exercise
(mL/min)Skeletal muscle 1200 4500 12,500 Heart 250 350 750 Brain 750 750 750 Integument 500 1500 1900 Kidney 1100 900 600 Gastrointestinal 1400 1100 600 Others
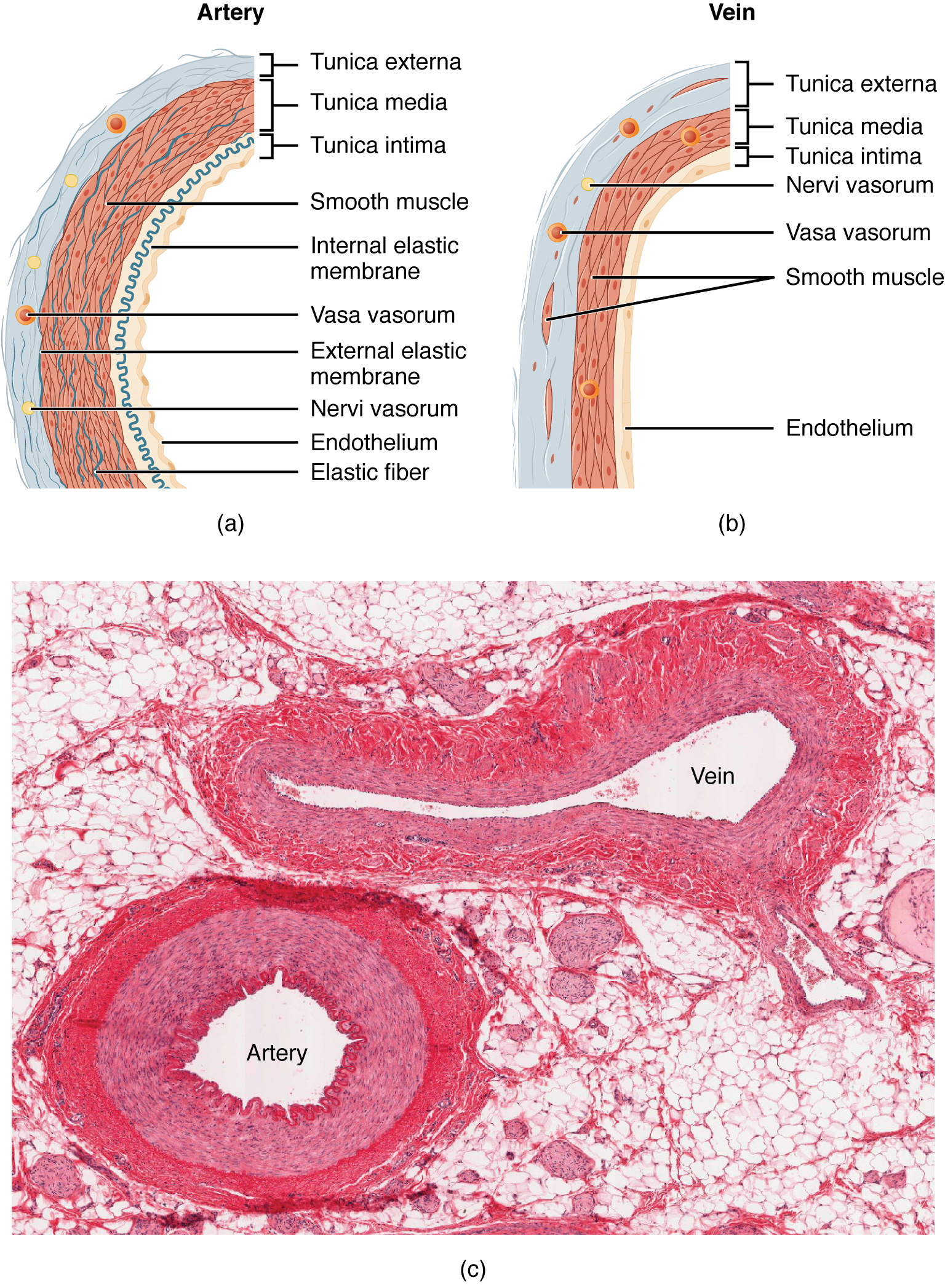
(i.e., liver, spleen)600 400 400 Total 5800 9500 17,500 - (3) Structure of Blood Vessels: (a) Arteries and (b) veins share the same general features, but the walls of arteries are much thicker because of the higher pressure of the blood that flows through them.
- (4) Types of Arteries and Arterioles
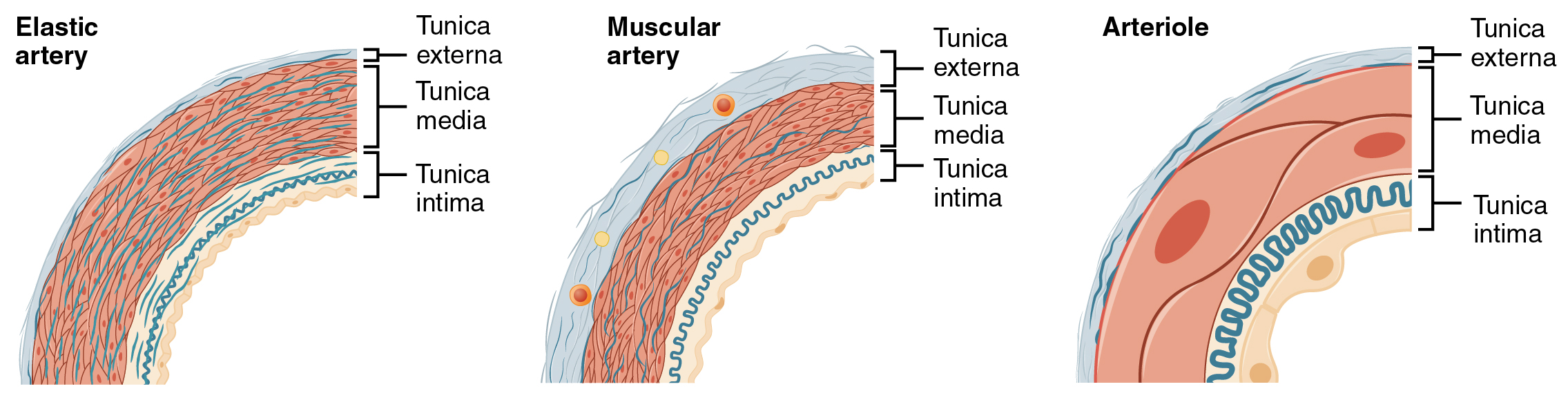
Arterioles Comparison of the walls of an elastic artery, a muscular artery, and an arteriole is shown. In terms of scale, the diameter of an arteriole is measured in micrometers compared to millimeters for elastic and muscular arteries. - (5) Types of Veins and Venules
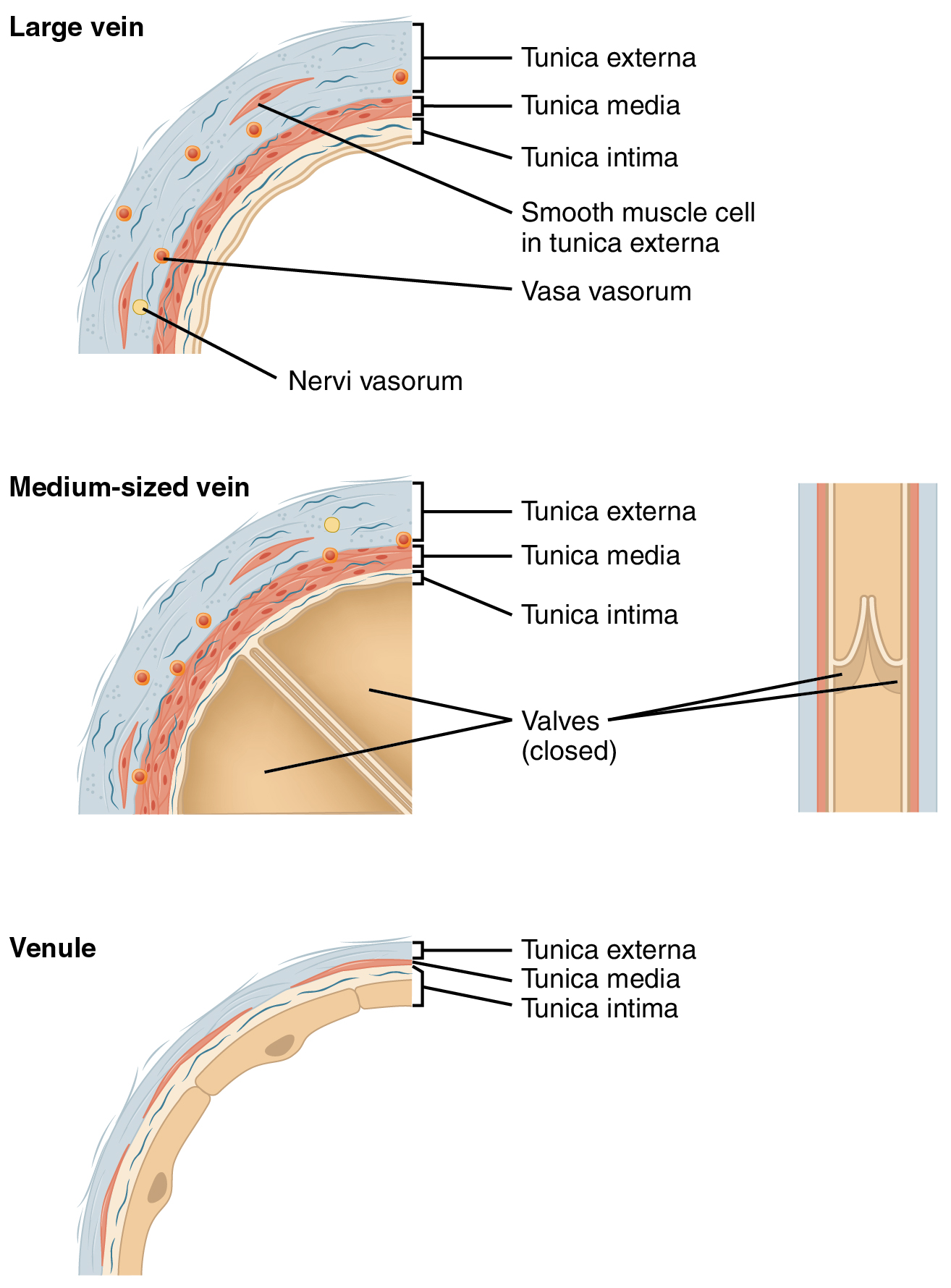
Many veins have valves to prevent back flow of blood, whereas venules do not. In terms of scale, the diameter of a venule is measured in micrometers compared to millimeters for veins. 
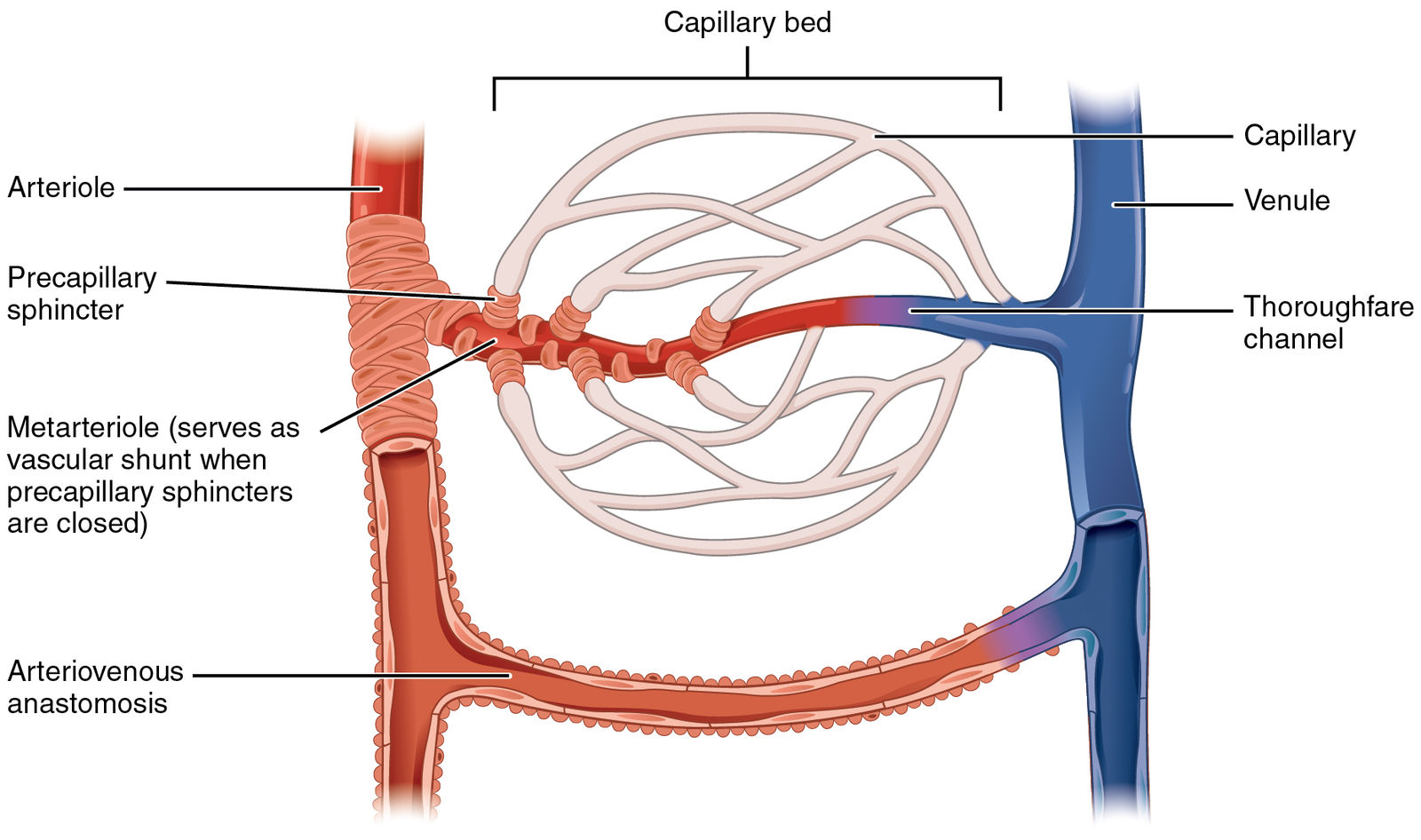
Varicose veins are commonly found in the lower limbs. (credit: Thomas Kriese) - (6) Capillary Bed
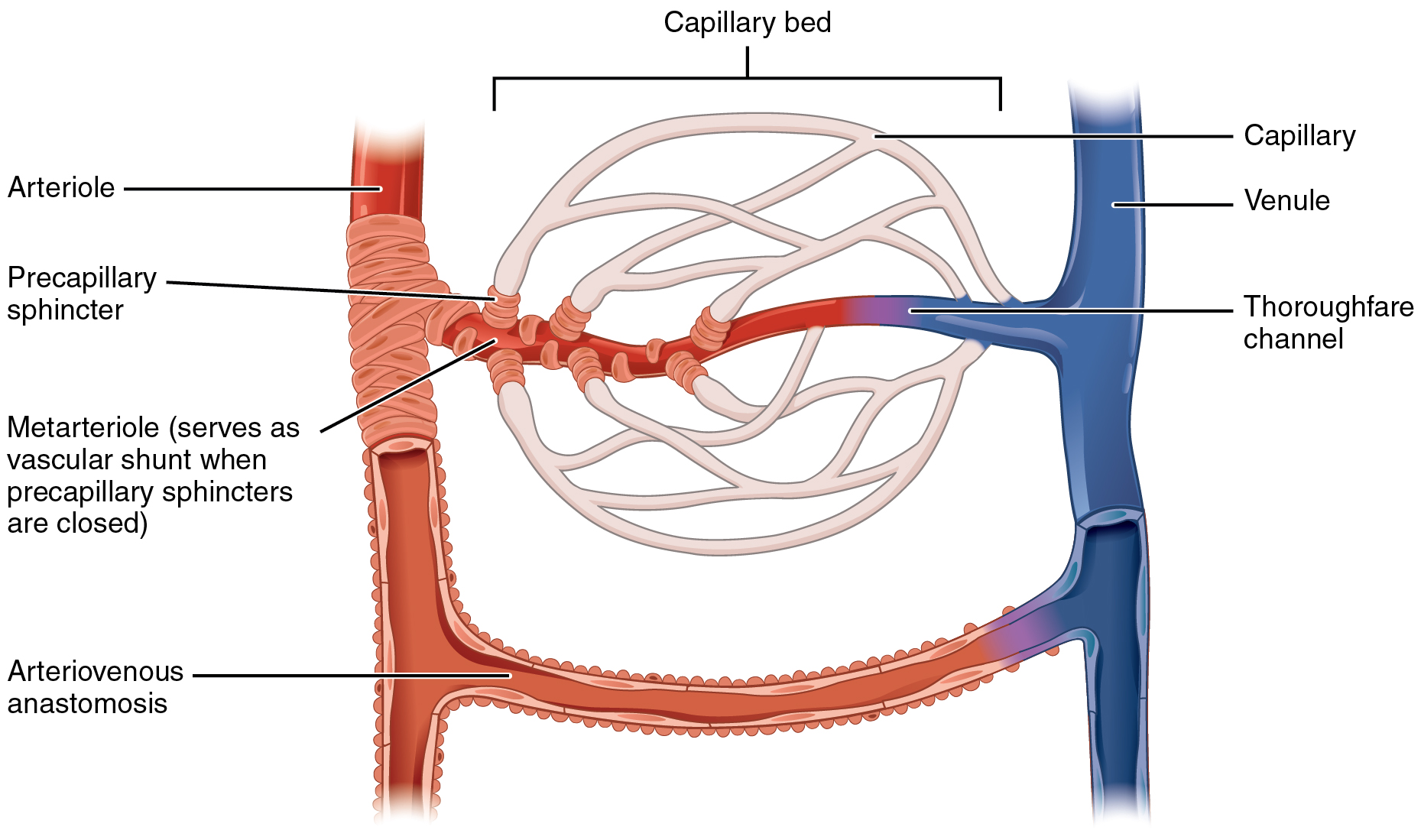
In a capillary bed, arterioles give rise to metarterioles. Precapillary sphincters located at the junction of a metarteriole with a capillary regulate blood flow. A thoroughfare channel connects the metarteriole to a venule. An arteriovenous anastomosis, which directly connects the arteriole with the venule, is shown at the bottom. - (7) Types of Capillaries
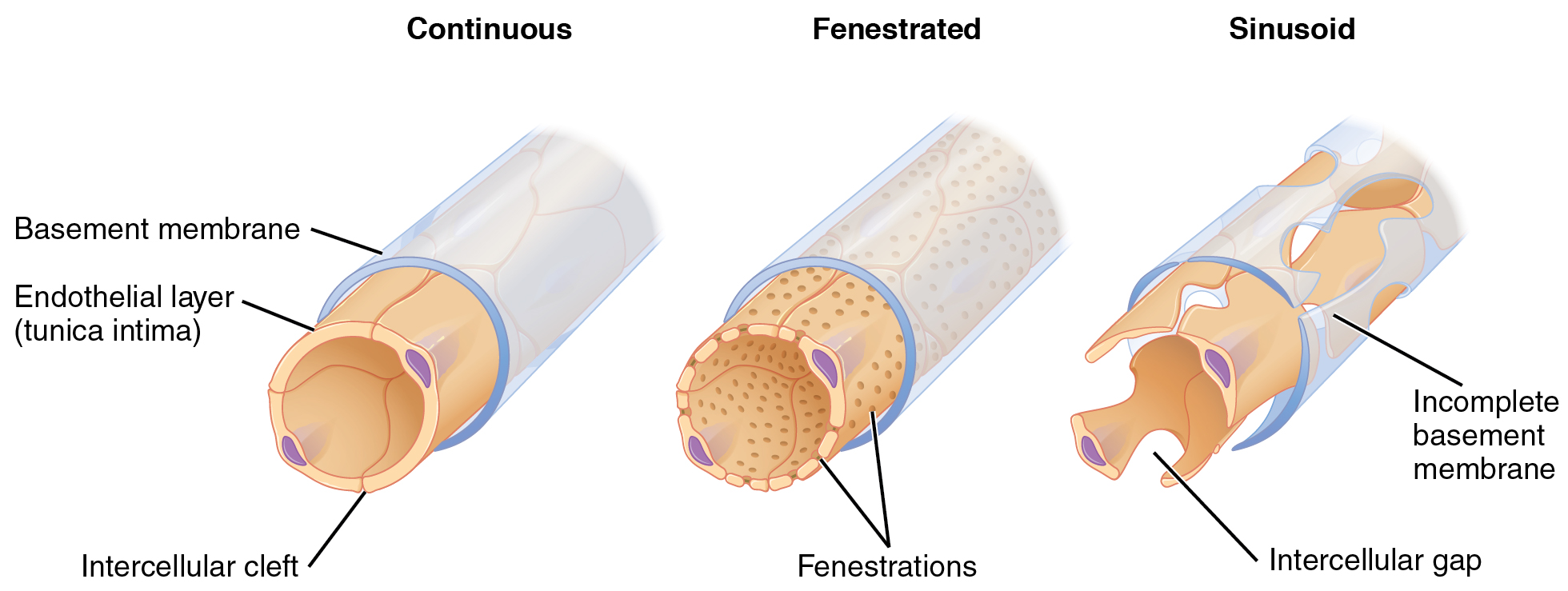
The three major types of capillaries: continuous, fenestrated, and sinusoid. - `
- Review of Heart Anatomy
- (1) External Anatomy of Human Heart

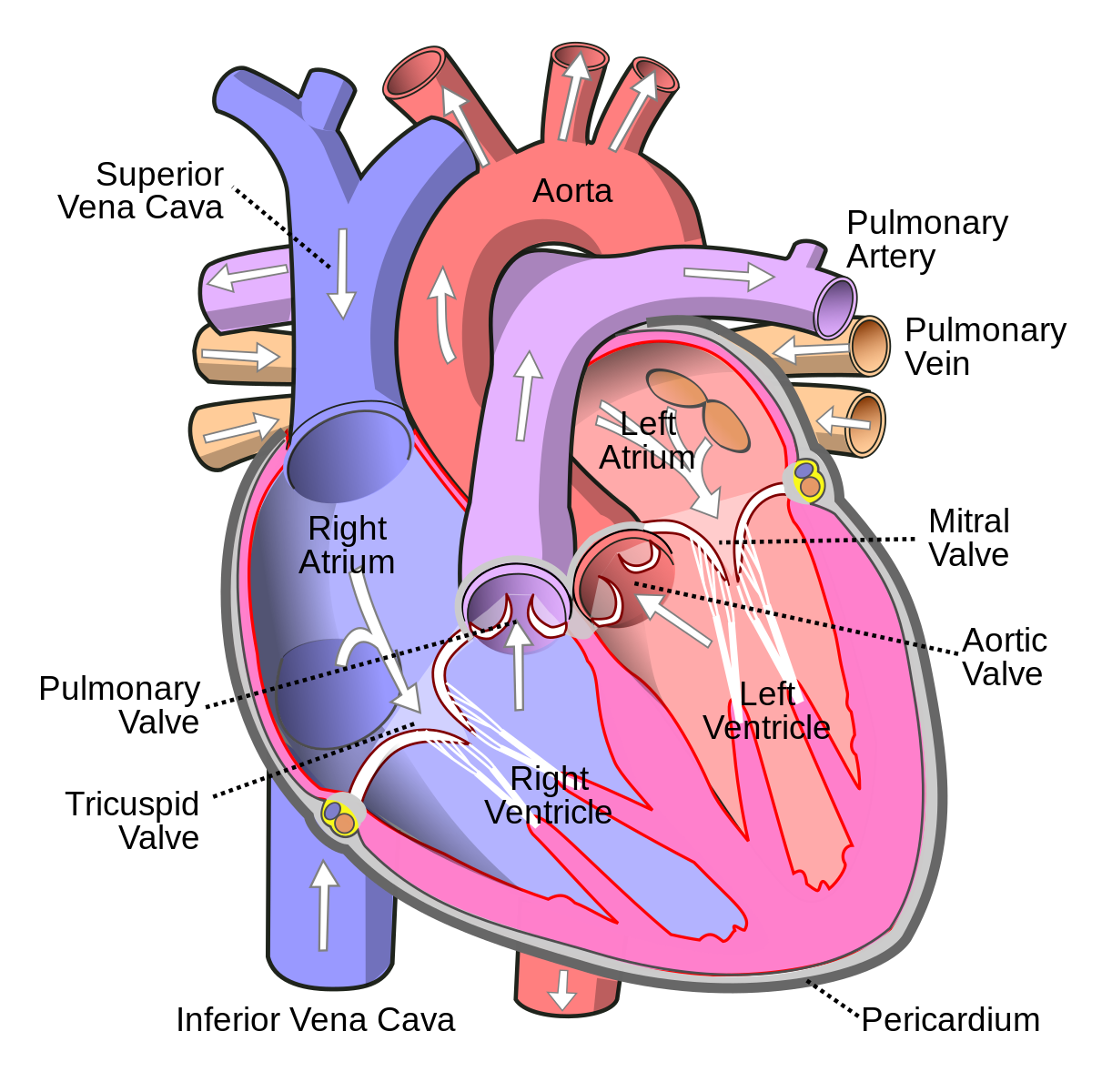
Inside the pericardium, the surface features of the heart are visible. - (2) Internal Structures of the Heart
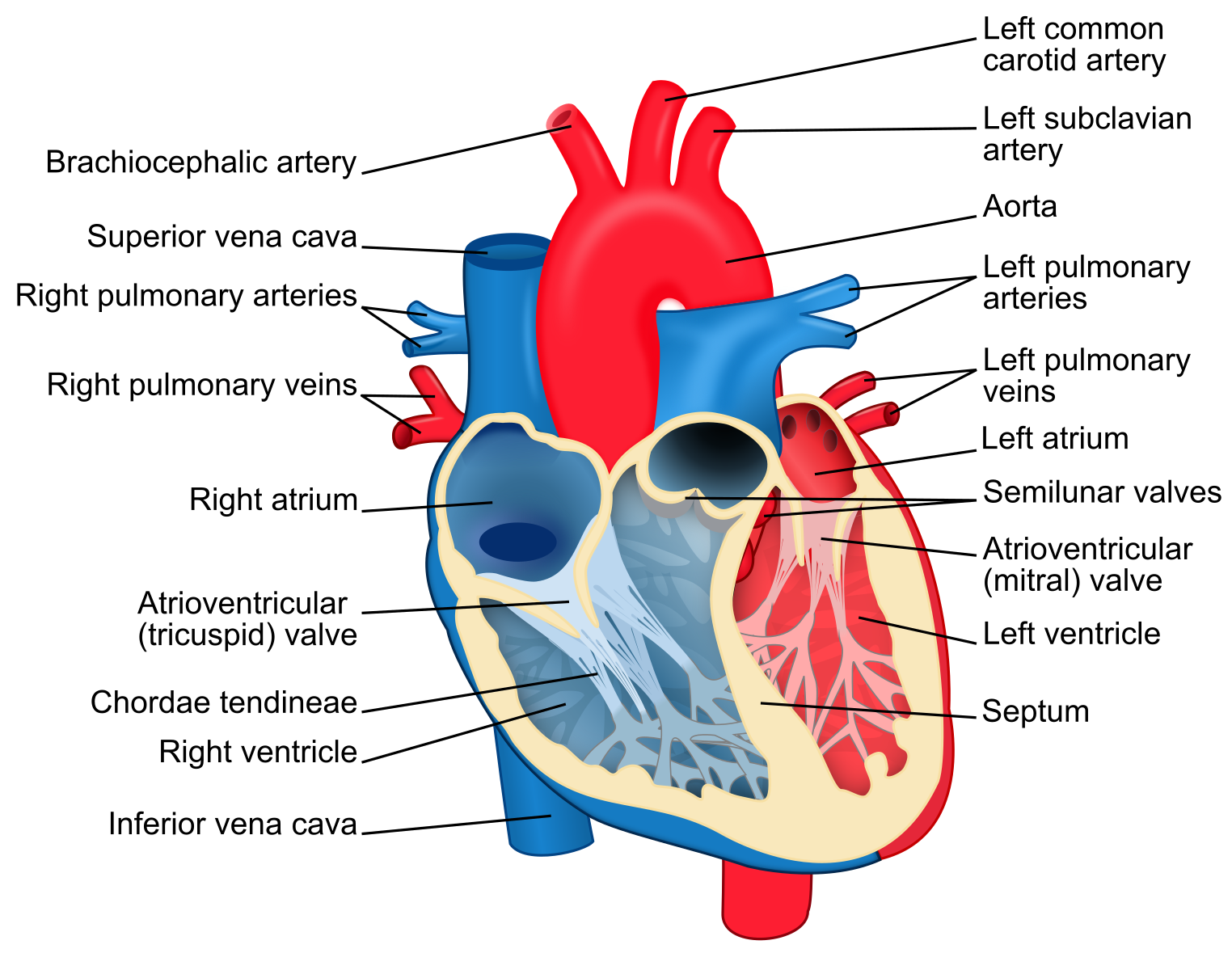
The anterior view of the heart: four chambers, major arteries and veins, and valves. Blue components indicate de-oxygenated blood pathways and red components indicate oxygenated blood pathways. - (3) Pericardial Membranes and Layers of the Heart Wall
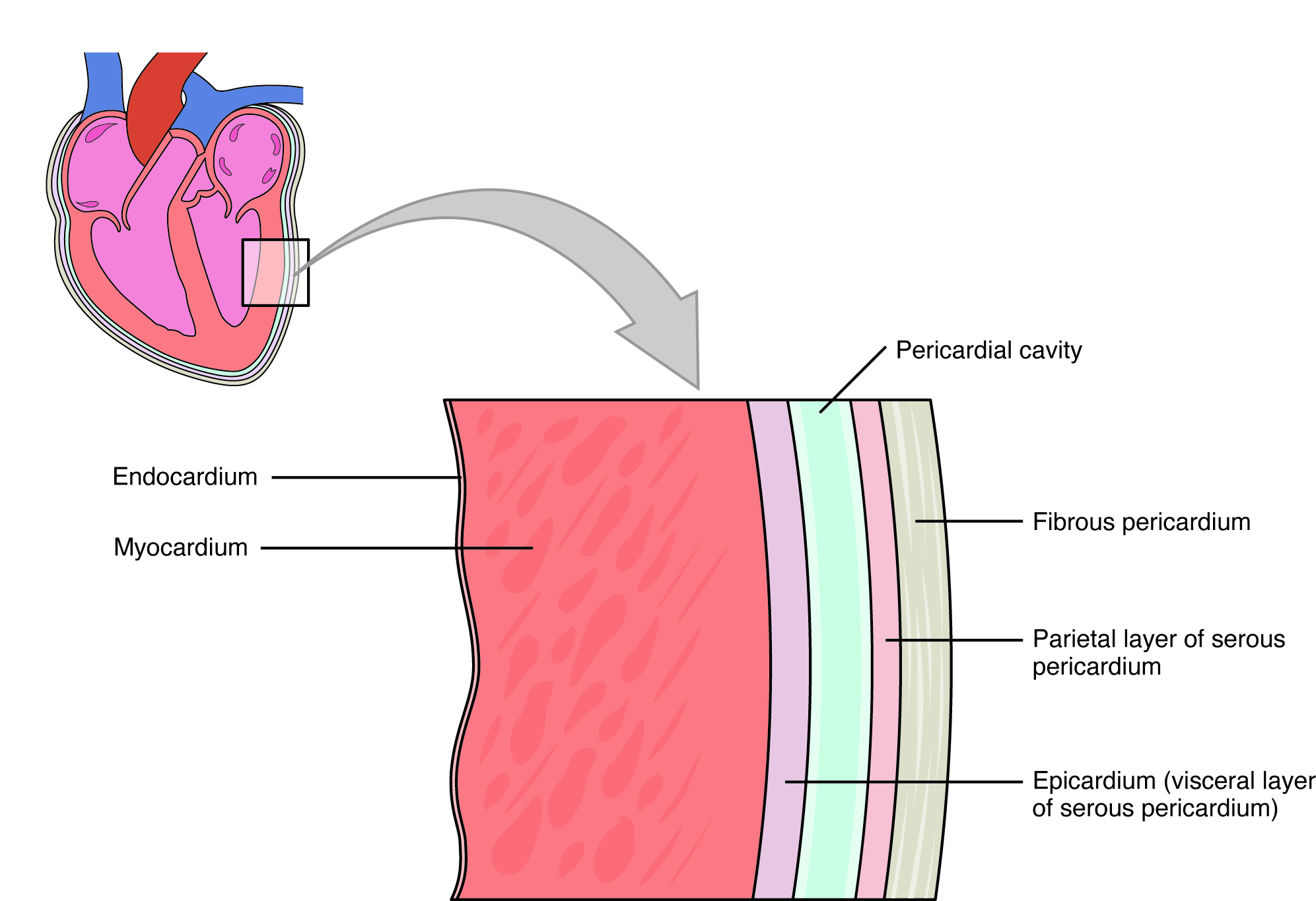
The pericardial membrane that surrounds the heart consists of three layers and the pericardial cavity. The heart wall also consists of three layers. The pericardial membrane and the heart wall share the epicardium. - (4) Heart Valves

With the atria and major vessels removed, all four valves are clearly visible, although it is difficult to distinguish the three separate cusps of the tricuspid valve.
- (1) External Anatomy of Human Heart
- Review of Cardiac Conduction System
-
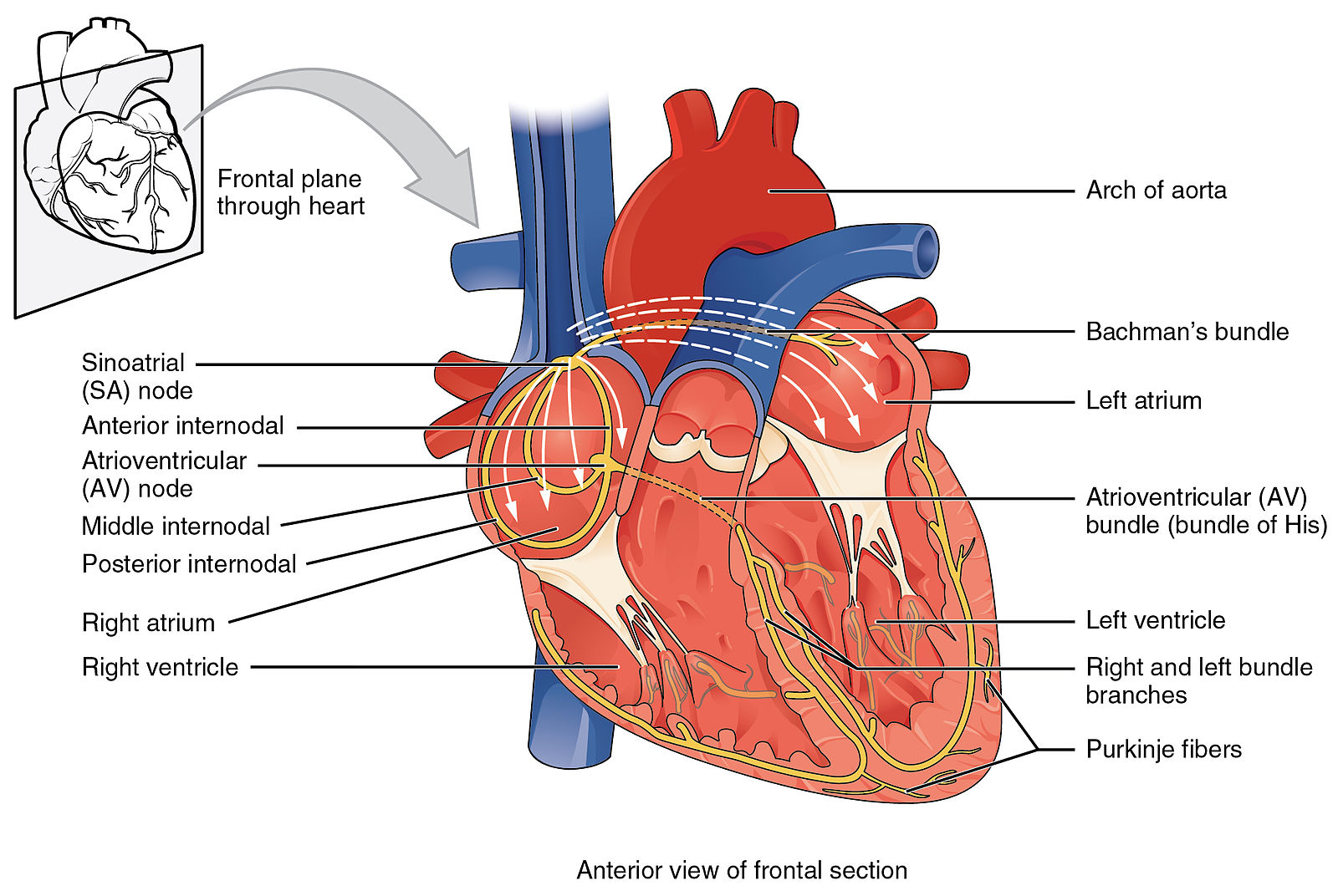
Conduction System of Heart: sinoatrial (SA) node, atrioventricular (VA) node, atrioventricular (AV) bundle, and Purkinje fibers. -
P wave: Depolarization of atria; QRS wave: Depolarization of ventricles; T wave: Repolarization of ventricles.
-
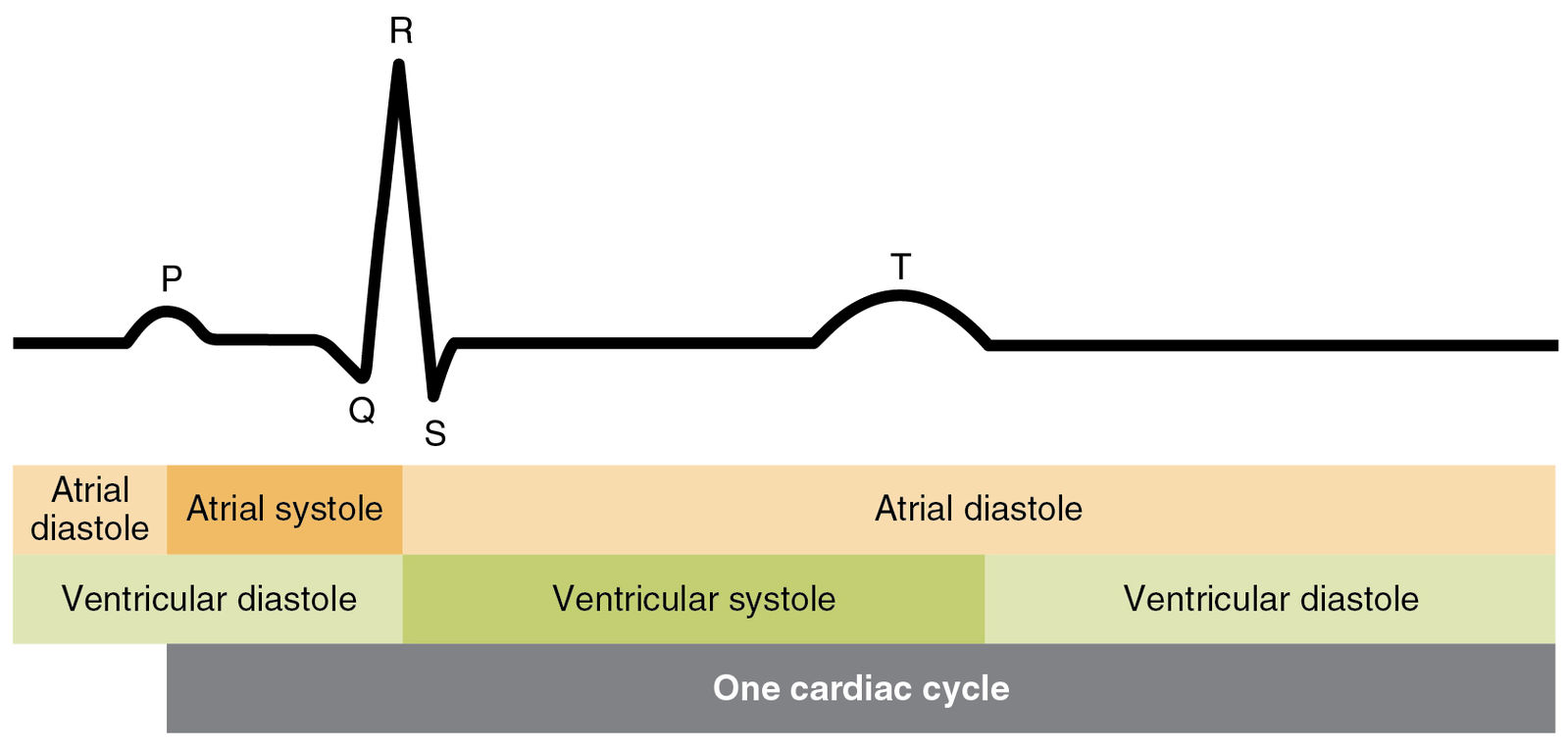
- Review of Cardiac Cycle
- Cardiac cycle: the period of time that begins with contraction of the atria and ends with ventricular relaxation. Systole: the period of contraction that the heart undergoes while it pumps blood into circulation. Diastole: the period of relaxation that occurs as the chambers fill with blood.
-
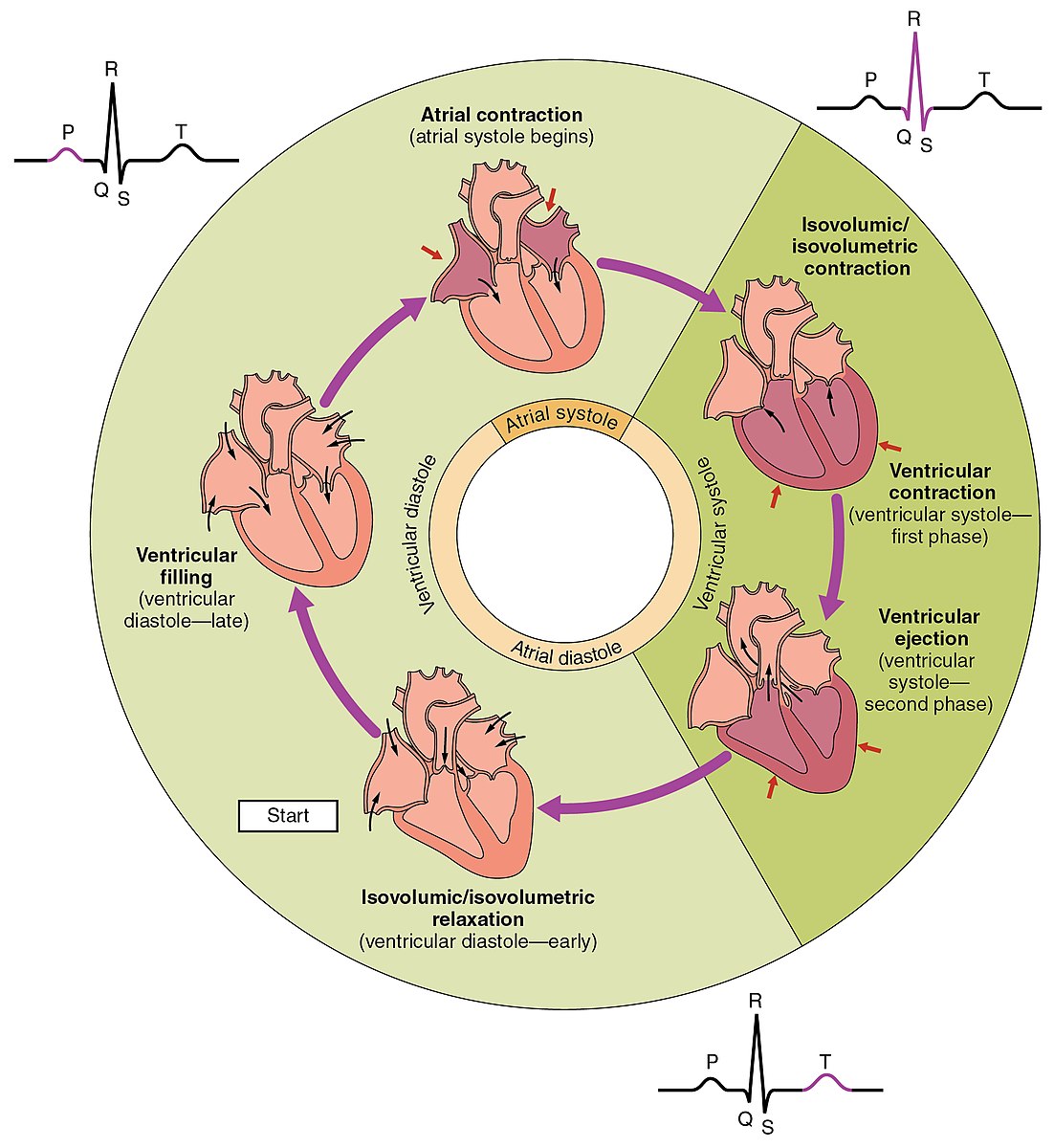
The cardiac cycle begins with atrial systole and progresses to ventricular systole, atrial diastole, and ventricular diastole, when the cycle begins again. Correlations to the ECG are highlighted. -
`
-
Abnormal ECG = arrhythmias/dysrhythmias
- Abnormal ECG is due to infarct (ischemia) or systemic problem (e.g. K+deficiency), etc.
- If heart rate too high = tachycardia (>100bpm) & not able to fill enough & cardiac output is too low to support life.
- If heart rate too low = bradycardia (<60bpm) & cardiac output is too low.
-
- `
- Review of Medulla Oblongata Control of Heart Rate and Contractility (Stroke Volume)
- Factors that stimulate increase in HR and SV
-
Major Factors Increasing Heart Rate and Force of Contraction Factor Effect Cardioaccelerator nerves Release of norepinephrine by cardioaccelerator nerves Proprioreceptors Increased firing rates of proprioreceptors (e.g. during exercise) Chemoreceptors Chemoreceptors sensing decreased levels of O2 or increased levels of H+, CO2 and lactic acid Baroreceptors Decreased firing rates of baroreceptors (indicating falling blood volume/pressure) Limbic system Anticipation of physical exercise or strong emotions by the limbic system Catecholamines Decreased epinephrine and norepinephrine release by the adrenal glands Thyroid hormones Increased T3 and T4 in the blood (released by thyroid) Calcium Increase in calcium ions in the blood Potassium Decrease in potassium ions in the blood Sodium Decrease in sodium ions in the blood Body temperature Increase in body temperature Nicotine and caffeine Presence of nicotine, caffeine or other stimulants
-
- Factors that decrease HR and SV
-
Factors Decreasing Heart Rate and Force of Contraction Factor Effect Cardioinhibitor nerves (vagus) Release of acetylcholine by cardioinhibitor nerves Proprioreceptors Decreased firing rates of proprioreceptors (e.g. during rest) Chemoreceptors Chemoreceptors sensing increased levels of O2 or decreased levels of H+, CO2 and lactic acid Baroreceptors Increased firing rates of baroreceptors (indicating rising blood volume/pressure) Limbic system Anticipation of relaxation by the limbic system Catecholamines Decreased epinephrine and norepinephrine release by the adrenal glands Thyroid hormones Decreased T3 and T4 in the blood (released by thyroid) Calcium Decrease in calcium ions in the blood Potassium Increase in potassium ions in the blood Sodium Increase in sodium ions in the blood Body temperature Decrease in body temperature Opiates and tranquilizers Presence of opiates (heroin), tranquilizers or other depressants 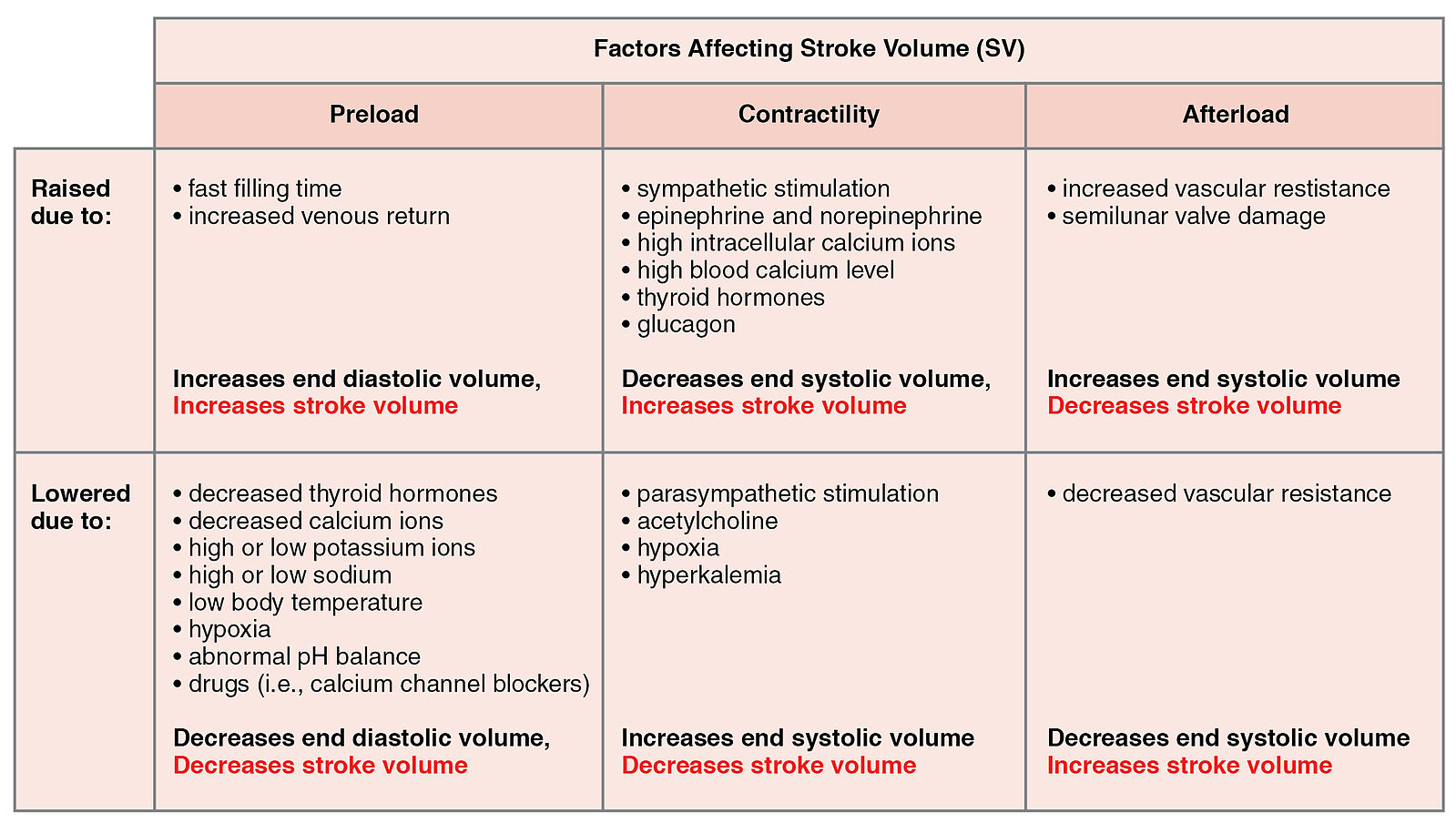
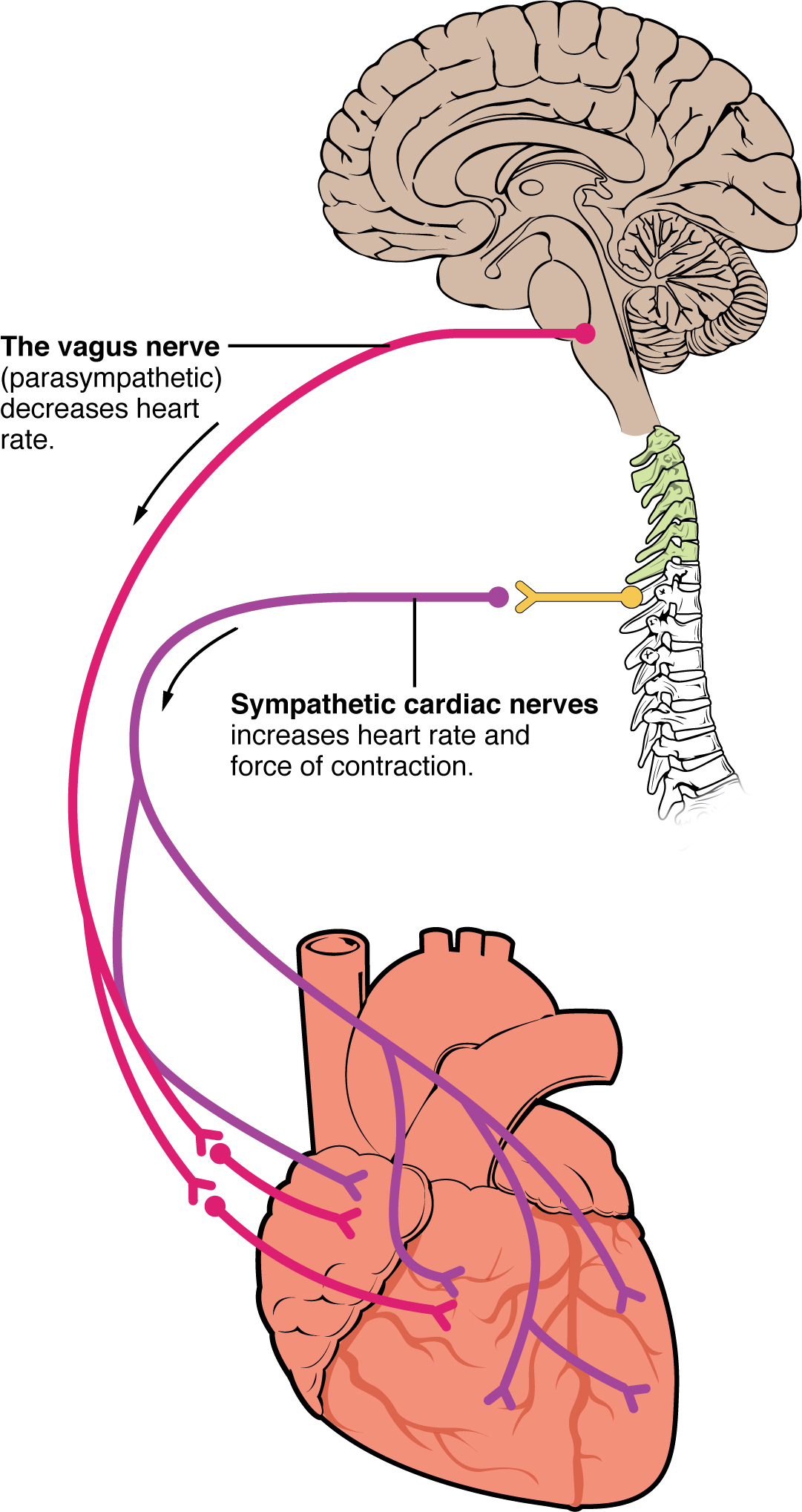
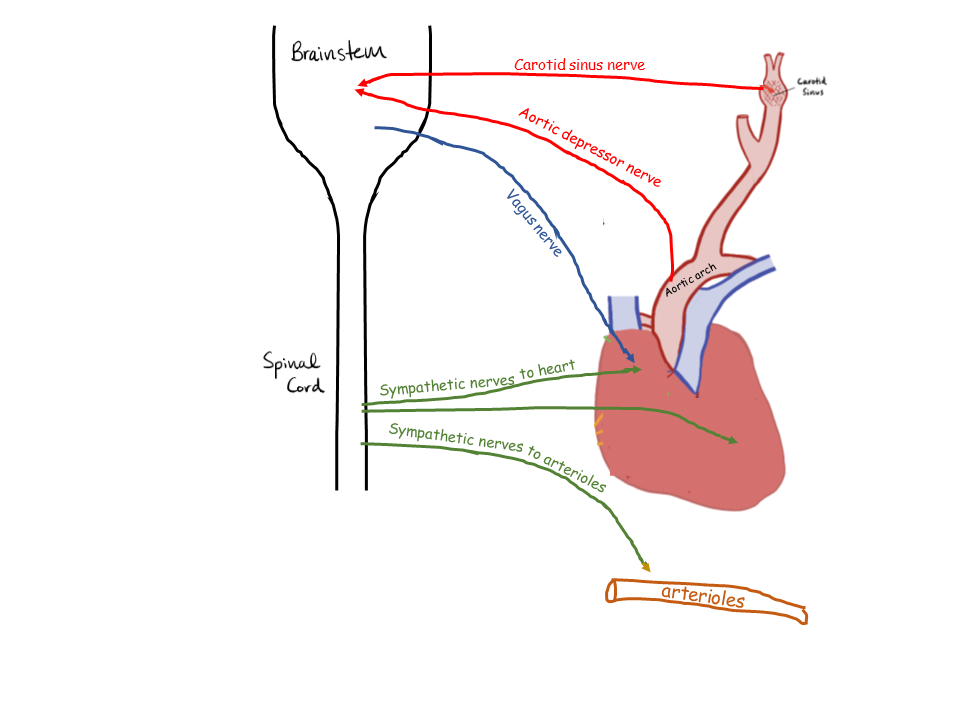
Autonomic Innervation of the Heart: Cardioaccelerator and cardioinhibitory areas are components of the paired cardiac centers located in the medulla oblongata of the brain. They innervate the heart via sympathetic cardiac nerves that increase cardiac activity and vagus (parasympathetic) nerves that slow cardiac activity.
-
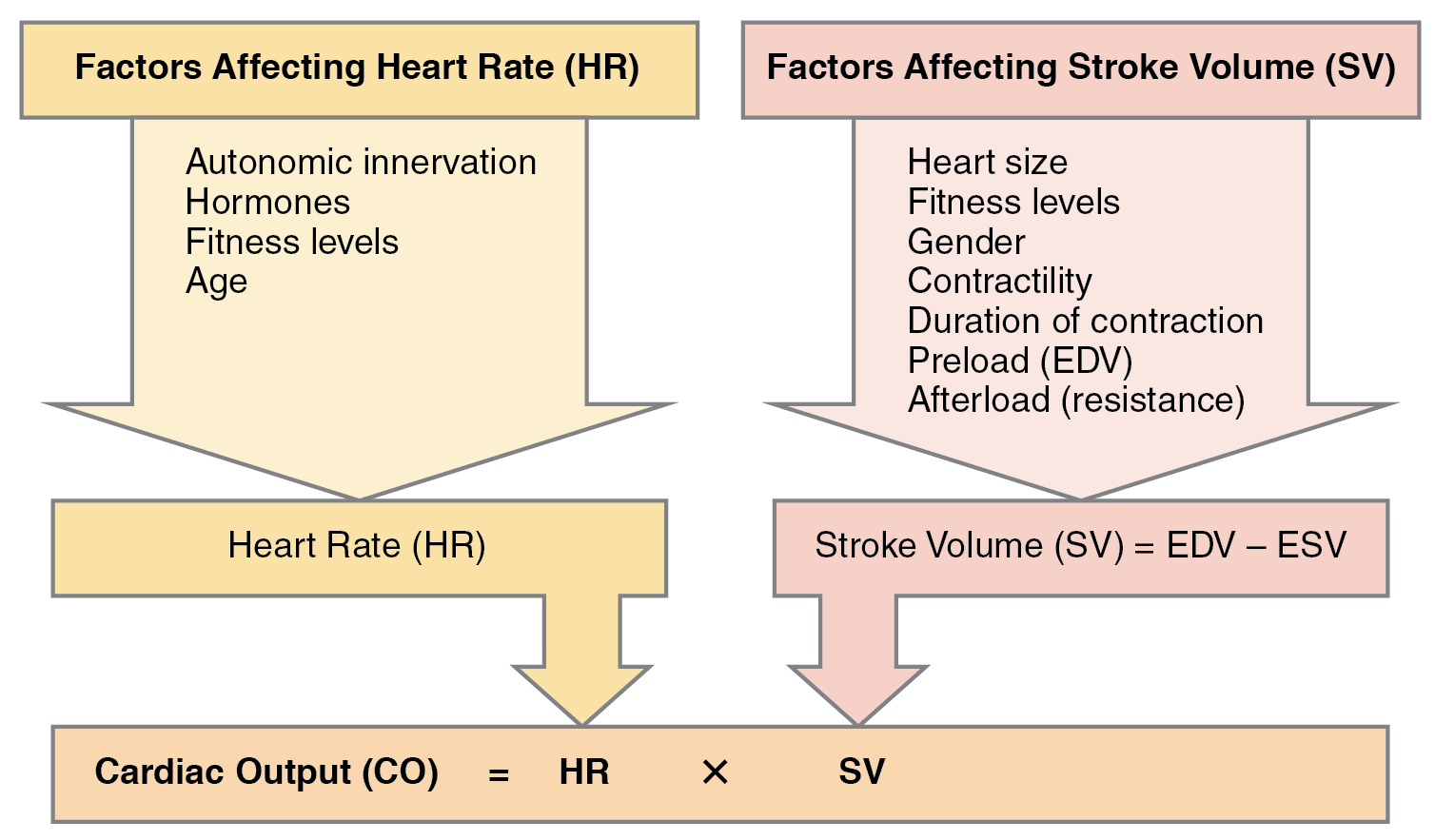
- CO = HR x SV
-
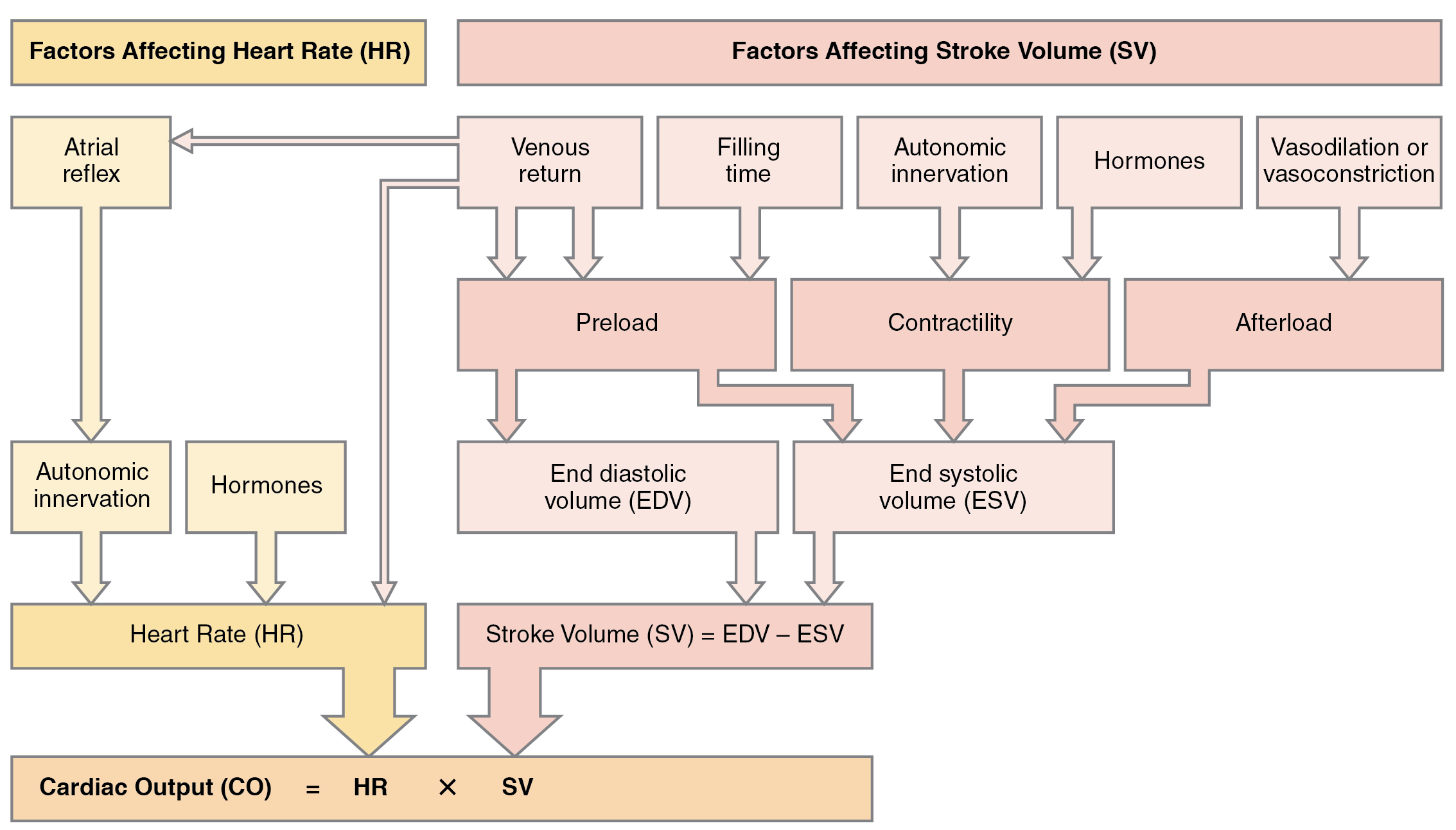
Summary of Major Factors Influencing Cardiac Output: The primary factors influencing HR include autonomic innervation plus endocrine control. Not shown are environmental factors, such as electrolytes, metabolic products, and temperature. The primary factors controlling SV include preload, contractility, and afterload. Other factors such as electrolytes may be classified as either positive or negative inotropic agents.
-
- Review of Starling’s Law
- Summary
-
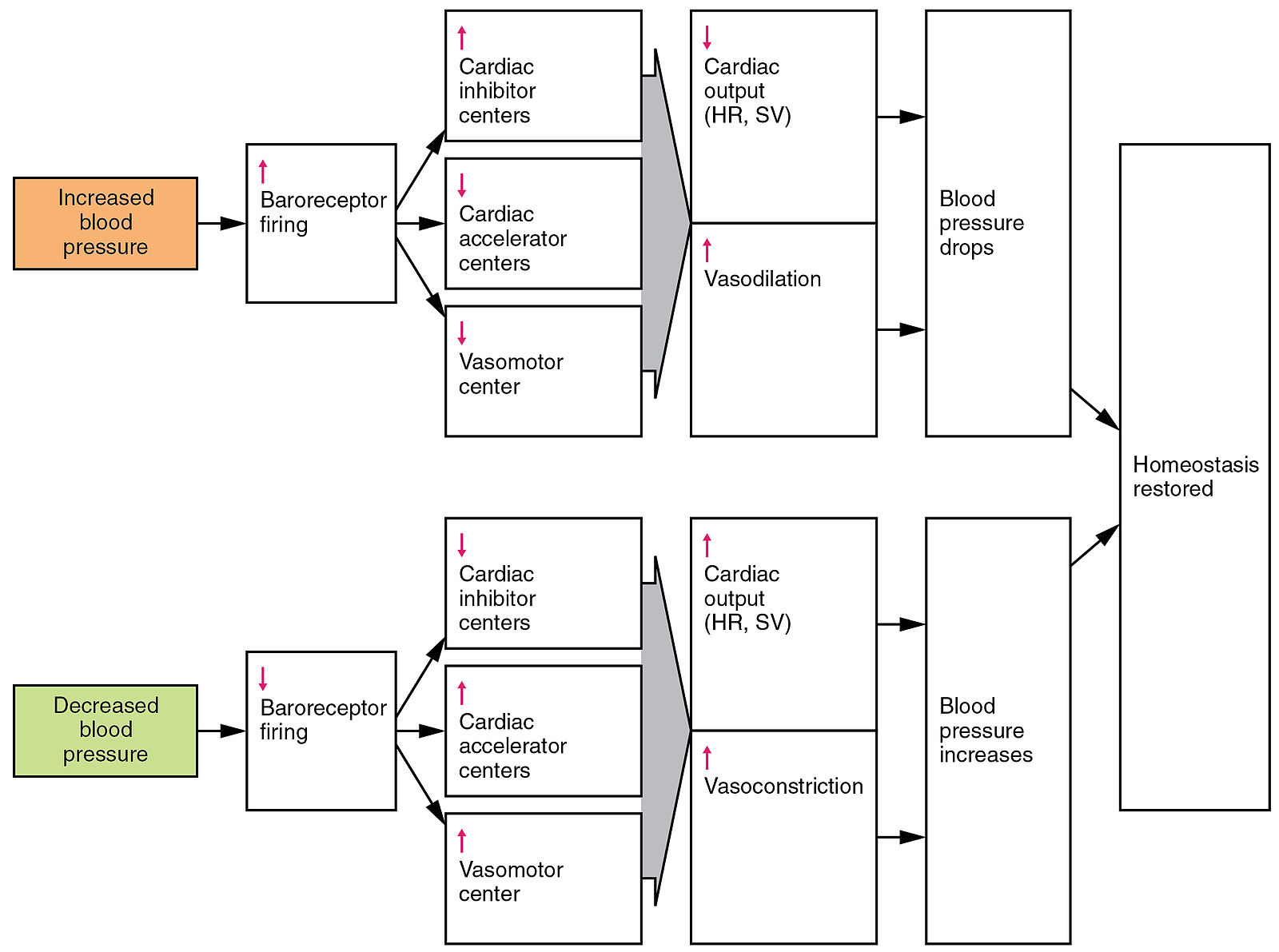
Cardiac Response to Decreasing Blood Flow and Pressure Due to Decreasing Cardiac Output Baroreceptors (aorta, carotid arteries, venae cavae, and atria) Chemoreceptors (both central nervous system and in proximity to baroreceptors) Sensitive to Decreasing stretch Decreasing O2 and increasing CO2, H+, and lactic acid Target Parasympathetic stimulation suppressed Sympathetic stimulation increased Response of heart Increasing heart rate and increasing stroke volume Increasing heart rate and increasing stroke volume Overall effect Increasing blood flow and pressure due to increasing cardiac output; homeostasis restored Increasing blood flow and pressure due to increasing cardiac output; homeostasis restored -
Cardiac Response to Increasing Blood Flow and Pressure Due to Increasing Cardiac Output Baroreceptors (aorta, carotid arteries, venae cavae, and atria) Chemoreceptors (both central nervous system and in proximity to baroreceptors) Sensitive to Increasing stretch Increasing O2 and decreasing CO2, H+, and lactic acid Target Parasympathetic stimulation increased Sympathetic stimulation suppressed Response of heart Decreasing heart rate and decreasing stroke volume Decreasing heart rate and decreasing stroke volume Overall effect Decreasing blood flow and pressure due to decreasing cardiac output; homeostasis restored Decreasing blood flow and pressure due to decreasing cardiac output; homeostasis restored
-
- Factors that stimulate increase in HR and SV
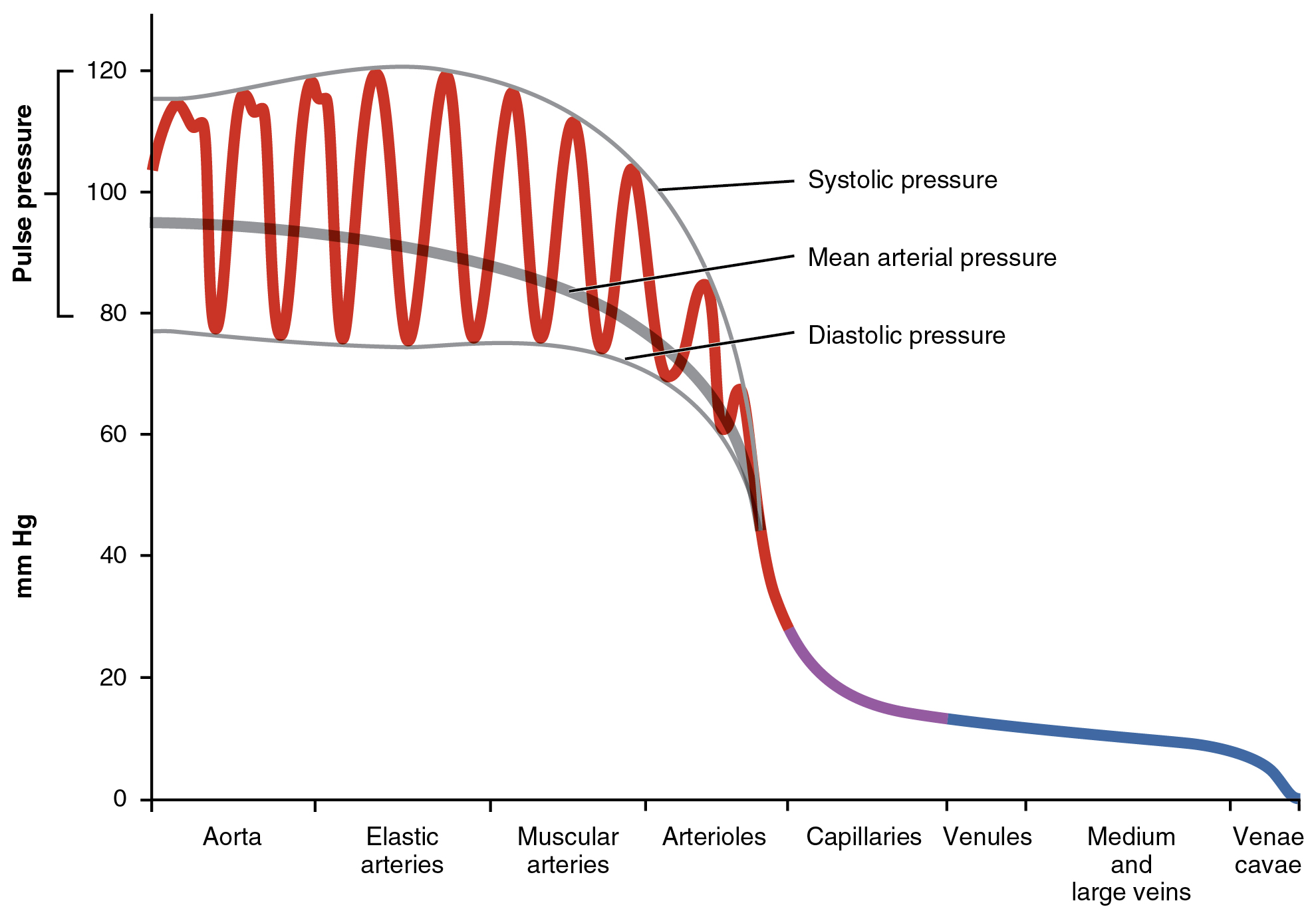
- Systolic pressure and Diastolic Pressure in aorta
- Systemic Blood Pressure
- Blood Pressure Measurement
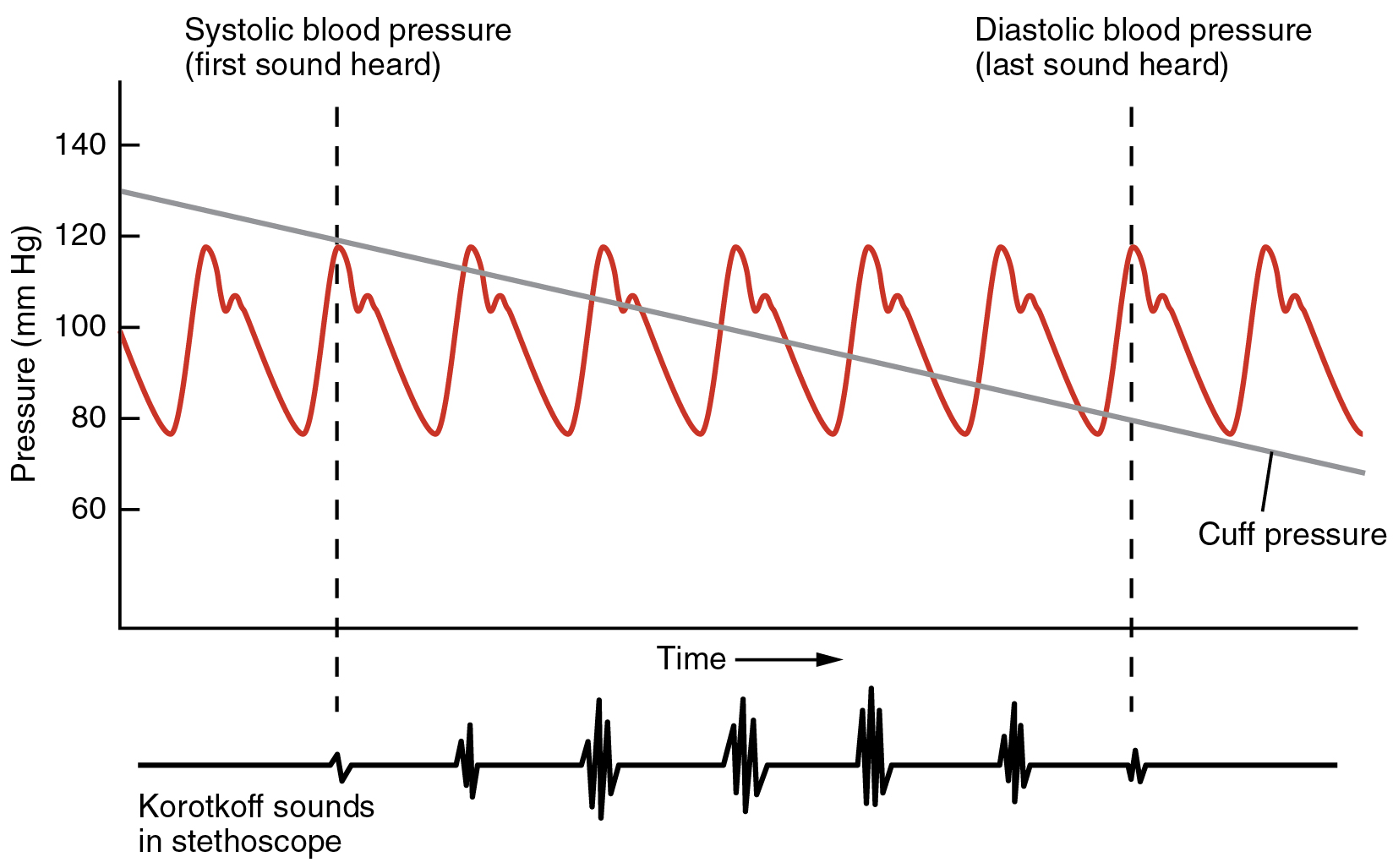
When pressure in a sphygmomanometer cuff is released, a clinician can hear the Korotkoff sounds. In this graph, a blood pressure tracing is aligned to a measurement of systolic and diastolic pressures.
- Systemic Blood Pressure
- Review of pressure generated by left ventricle and pressure generated by right ventricle
- The pressure generated by the left ventricle will be significantly higher than that generated by the right ventricle due to the much higher pressure in the aorta.
- Review of Blood Pressure, Mean Arterial Pressure and Blood Pressure Numbers through Systemic Circuit and Pulmonary Circuit
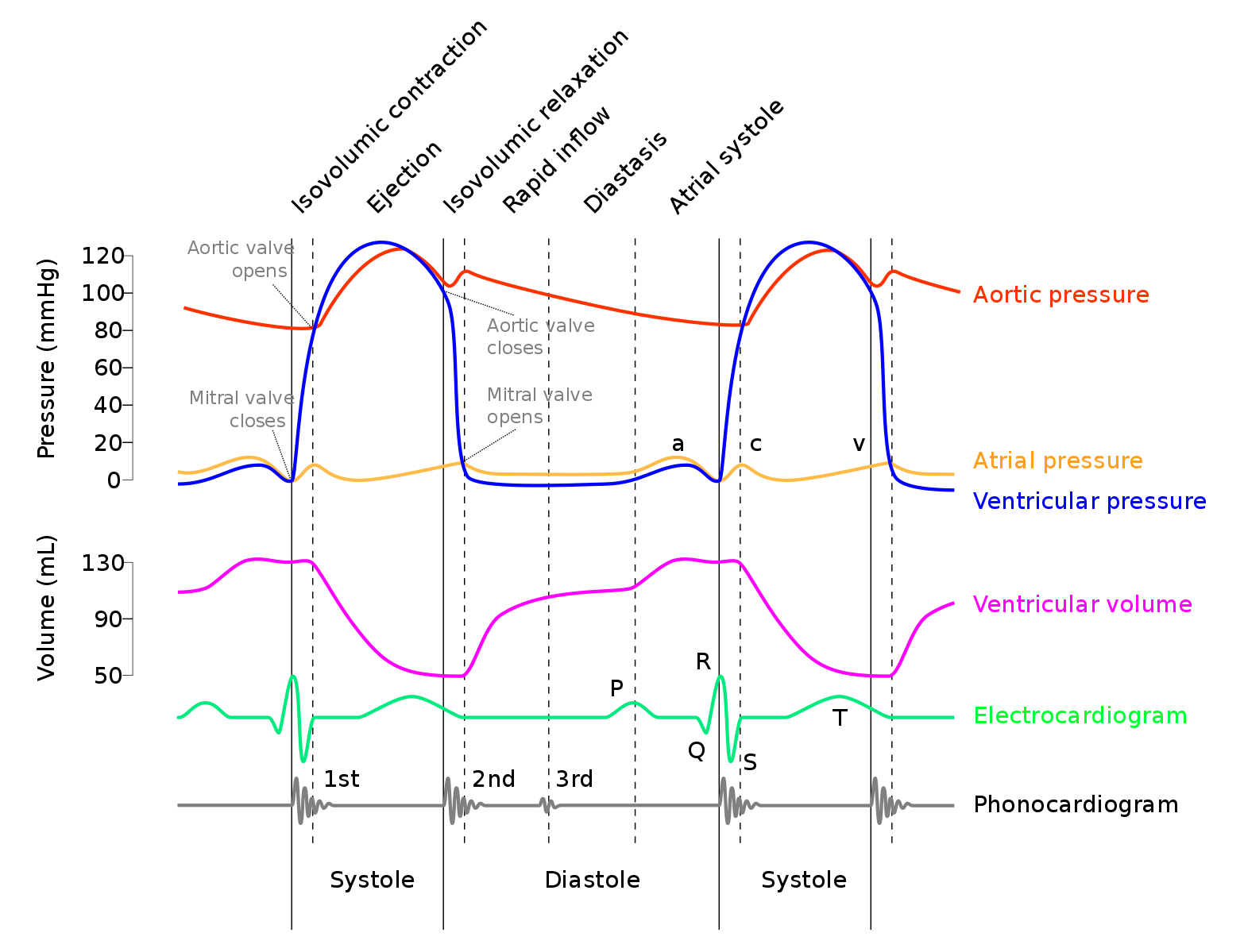
The Wiggers diagram shows the cardiac cycle events occurring in the left ventricle.
In the atrial pressure plot: wave “a” corresponds to atrial contraction, wave “c” corresponds to an increase in pressure from the mitral valve bulging into the atrium after closure, and wave “v” corresponds to passive atrial filling.
In the electrocardiogram: wave “P” corresponds to atrial depolarization, waves “QRS” correspond to ventricular depolarization, and wave “T” corresponds to ventricular repolarization.
In the phonocardiogram: The sound labeled 1st contributes to the S1 heart sound and is the reverberation of blood from the sudden closure of the mitral valve (left A-V valve) and the sound labeled “2nd” contributes to the S2 heart sound and is the reverberation of blood from the sudden closure of the aortic valve.- Mean Arterial Pressure (MAP)
- MAP = diastolic BP + (systolic BP diastolic BP)/3 𝐨𝐫 MAP = diastolic BP + (pulse pressure)/3
- Mean Arterial Pressure (MAP)
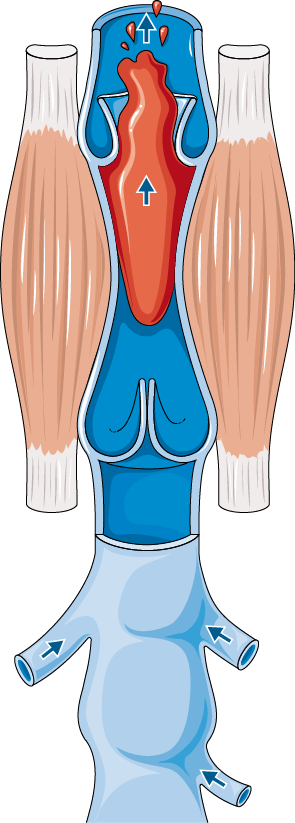
- Venous Return – Respiratory Pump, Venous valves, Skeletal Muscle Pump
- (1) Respiratory pump
- The respiratory pump facilitates blood flow through the thoracic and abdominal veins.
- Inhalation increases thoracic volume as the diaphragm contracts, moving downward and compressing the abdominal cavity. Simultaneously, the external intercostal muscles contract, elevating the chest and further expanding thoracic volume. This volume expansion reduces air pressure within the thorax, enabling inhalation. Consequently, thoracic vein pressure decreases, causing blood to flow from higher-pressure veins outside the thorax to the lower-pressure thoracic region, facilitating blood return to the heart.
- During exhalation, thoracic cavity pressure rises, increasing thoracic vein pressure and accelerating blood flow into the heart, aided by vein valves preventing backward blood flow.
- (2) Venous valves
- (3) Skeletal muscle pump
-
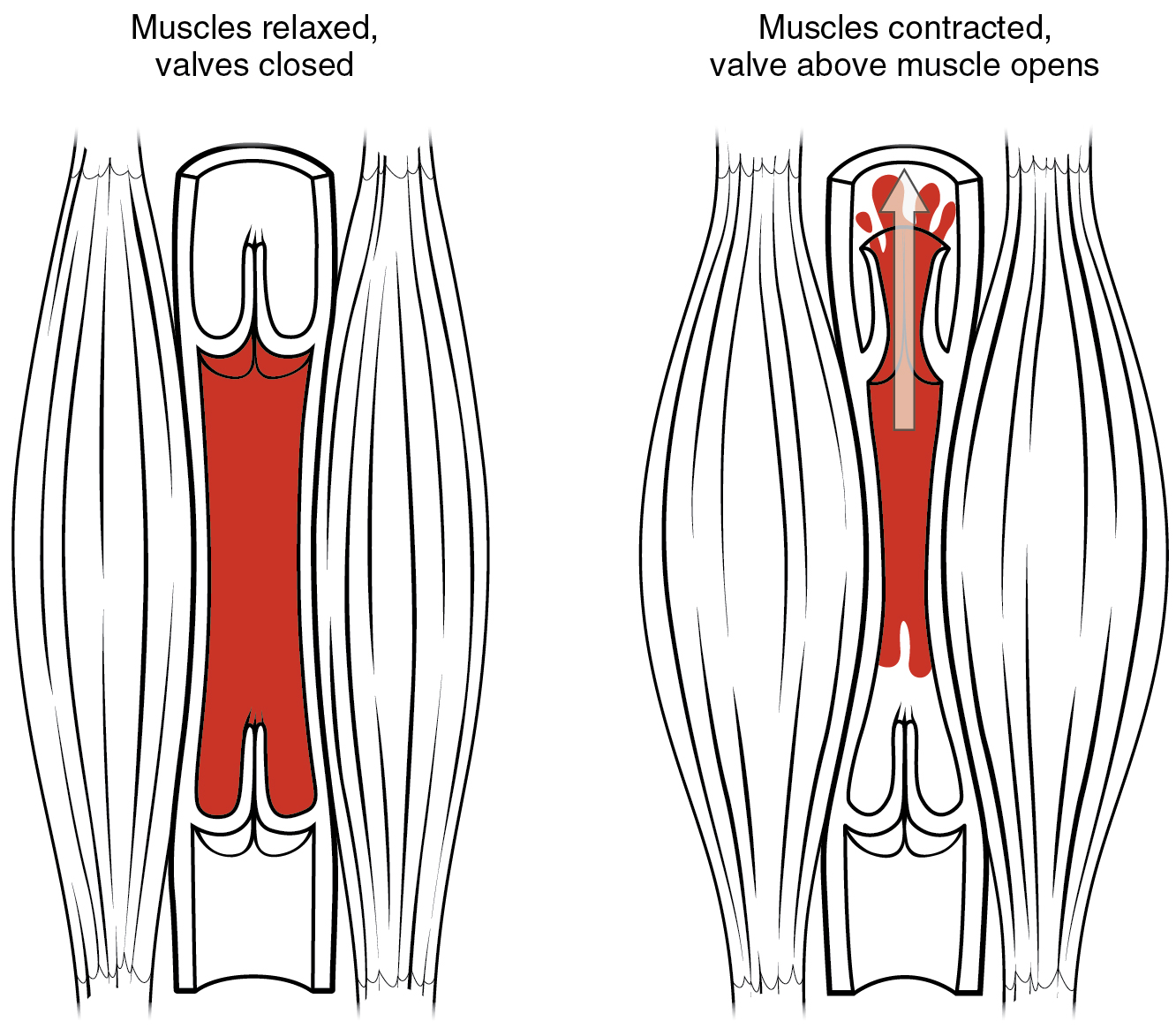
The contraction of skeletal muscles surrounding a vein compresses the blood and increases the pressure in that area. This action forces blood closer to the heart where venous pressure is lower. Note the importance of the one-way valves to assure that blood flows only in the proper direction.
-
- (1) Respiratory pump
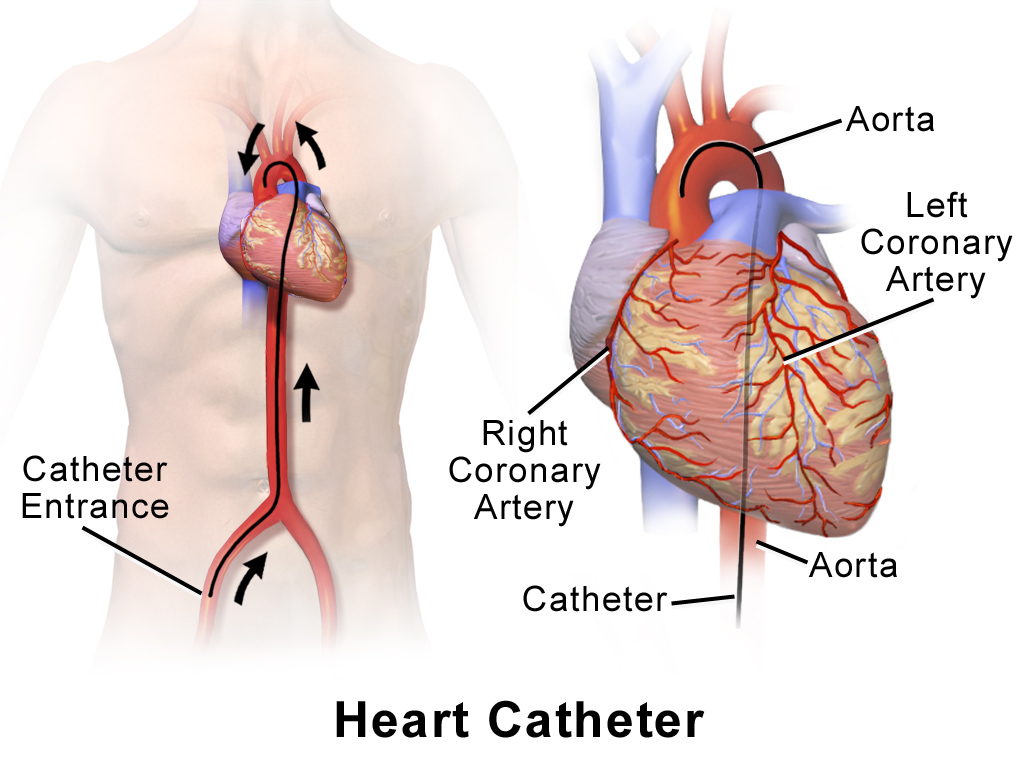
- Right and Left Coronary Artery, Cardiac Sinus
- Coronary arteries supply blood to the myocardium and other components of the heart. The left coronary artery distributes blood to the left side of the heart, the left atrium and ventricle, and the interventricular septum. The right coronary artery proceeds along the coronary sulcus and distributes blood to the right atrium, portions of both ventricles, and the heart conduction system.
-
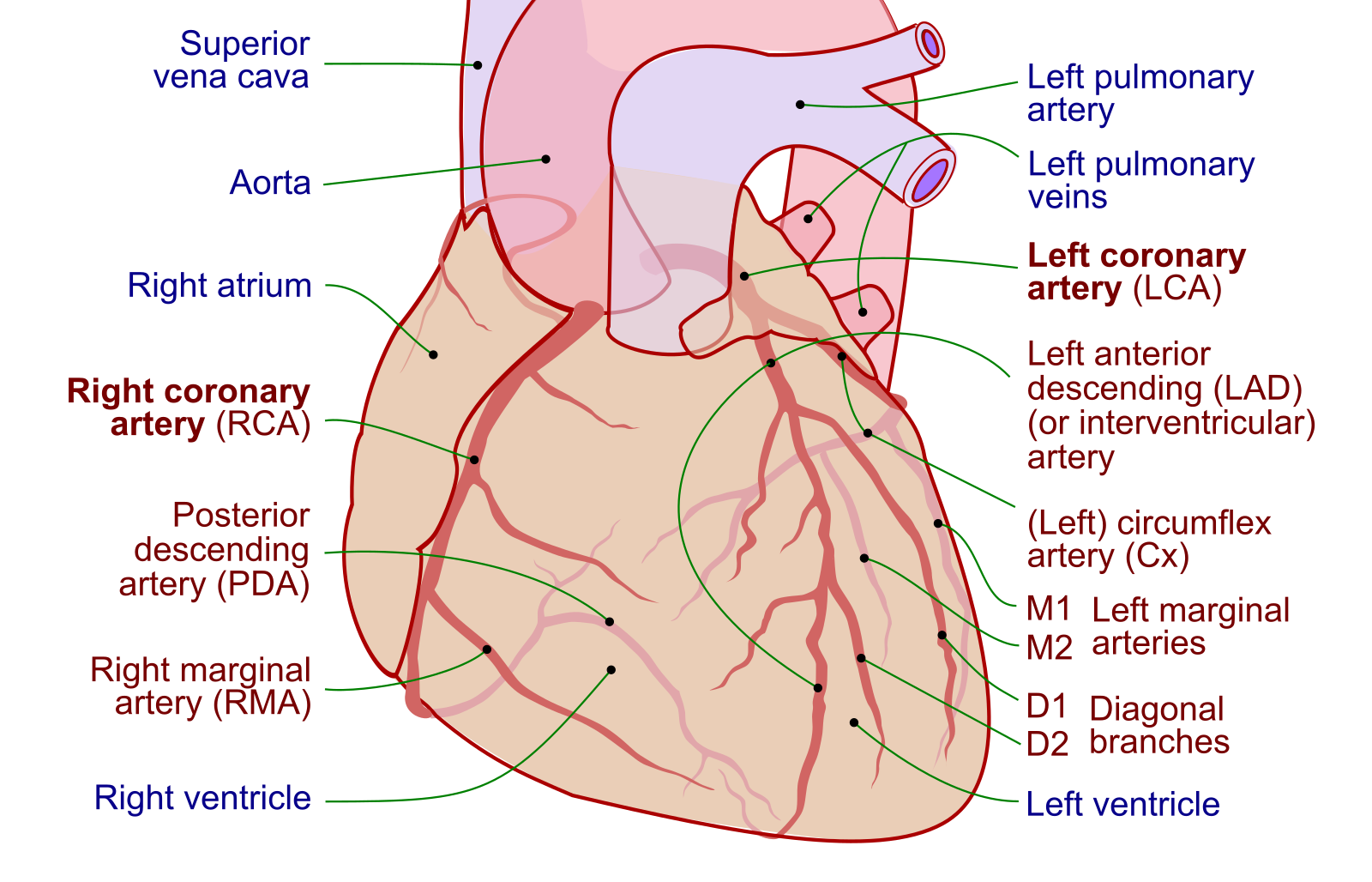
The right and left coronary arteries branch off from the aorta immediately distal to the aortic valve, contributing to systemic circulation, which supplies oxygenated blood to the heart muscle. -
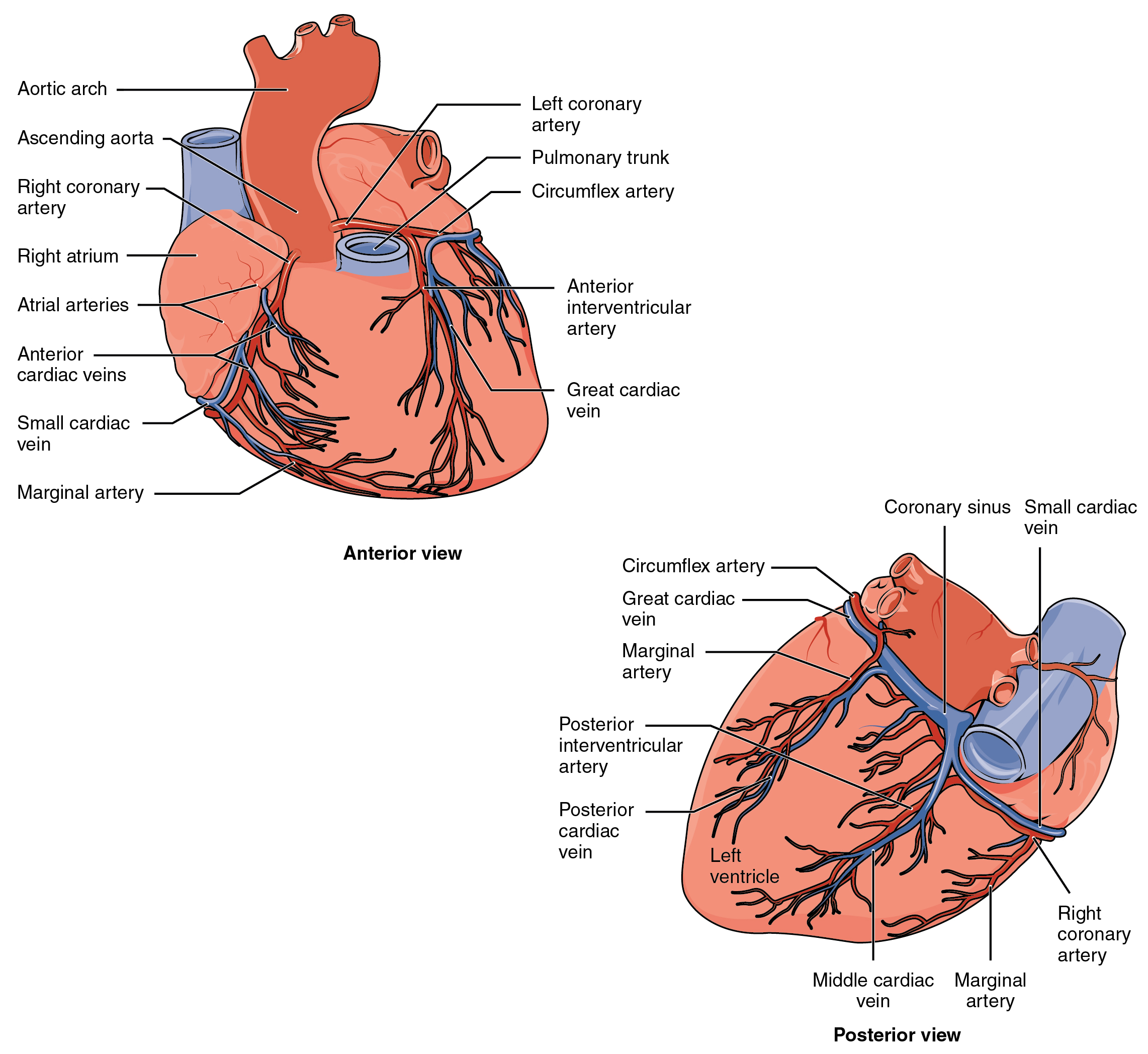
Coronary Circulation: The anterior view of the heart shows the prominent coronary surface vessels. The posterior view of the heart shows the prominent coronary surface vessels. - Cardiac Sinus
- Cardiac sinus
- Coronary sinus: The coronary sinus is a large, thin-walled vein on the posterior surface of the heart lying within the atrioventricular sulcus and emptying directly into the right atrium.
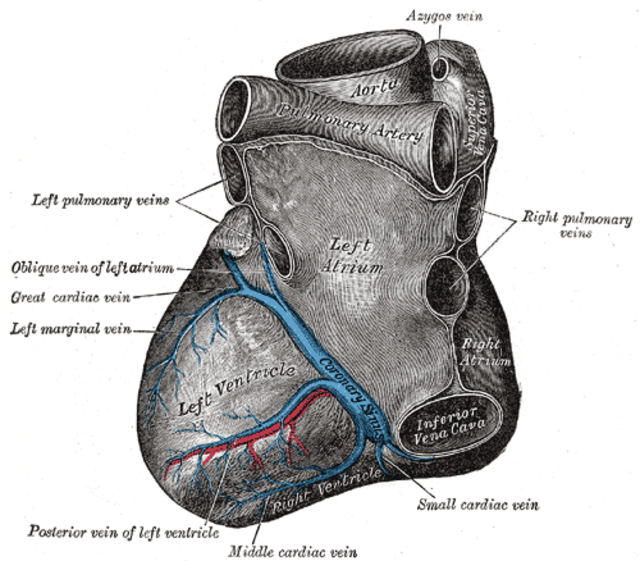
Back (posterior) side of the heart, with coronary sinus (blue) labeled - Pericardial sinus.
- Anastomosis in apex
-
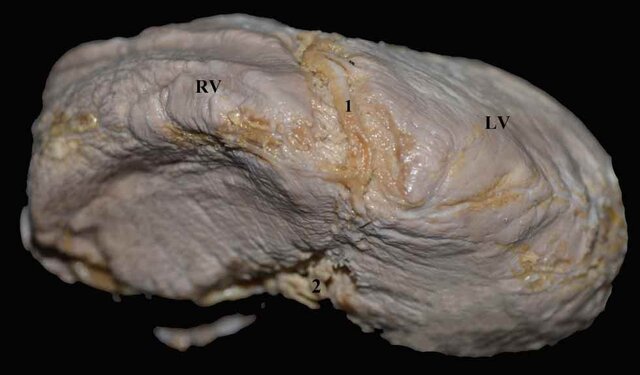
Apex of the heart. Anastomosis between the anterior interventricular artery (1) and the posterior interventricular artery (2). -
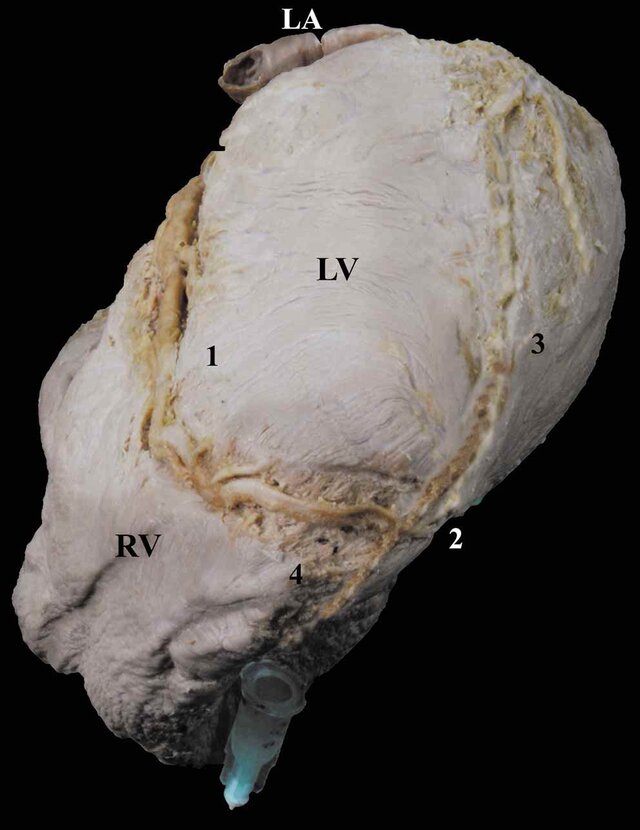
Apex of the heart. 2nd stage of the dissection process. An anastomotic network takes place in the apex between the anterior interventricular artery (1), the posterior interventricular artery (2) and small branches originated in the left marginal artery (3) and right marginal artery (4). - `
-
- SNS and PSNS affect on SA node
- SNS: sympathetic nervous system; PSNS: parasympathetic nervous system
-
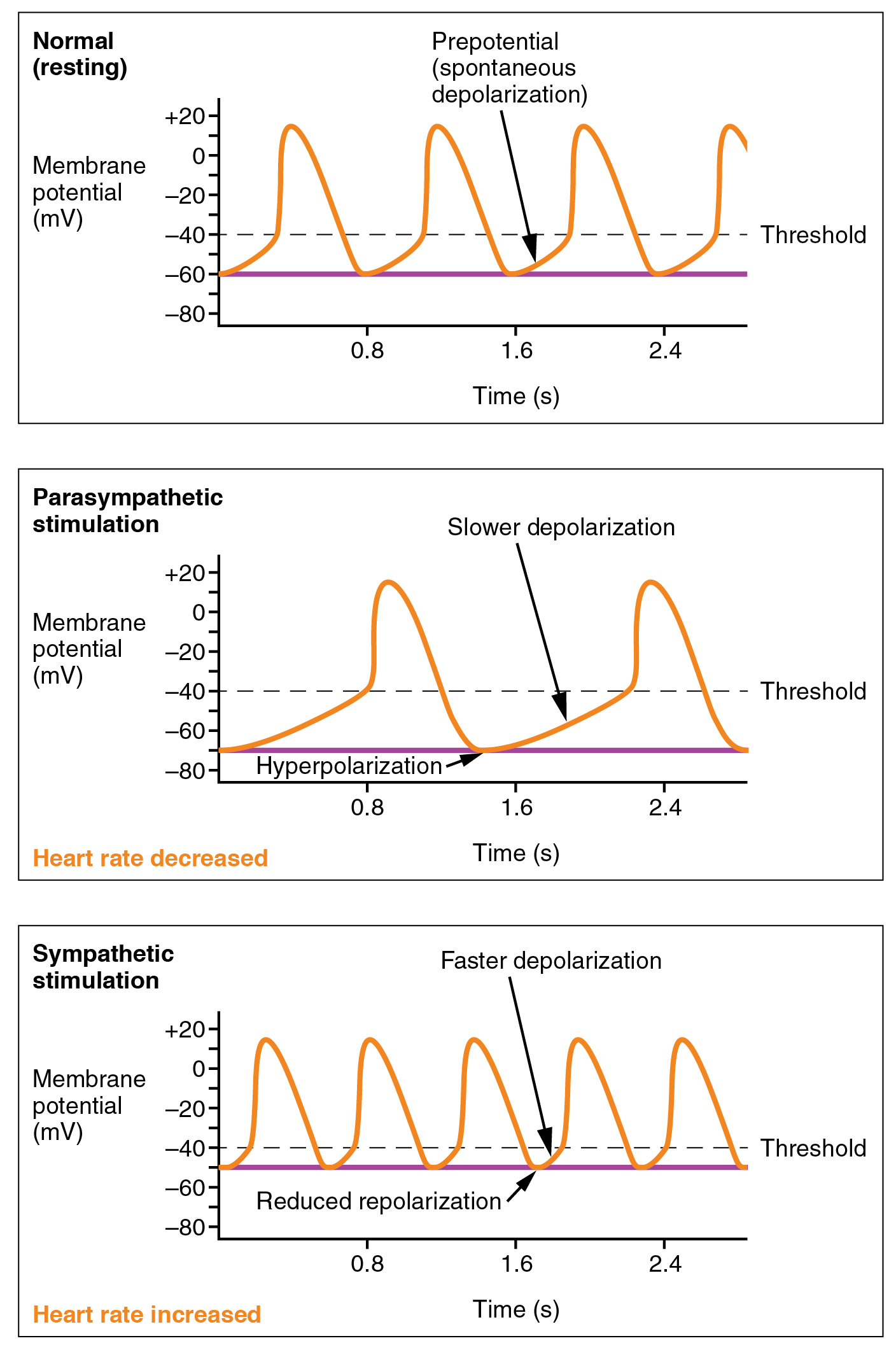
Effects of Parasympathetic and Sympathetic Stimulation on Normal Sinus Rhythm: The wave of depolarization in a normal sinus rhythm shows a stable resting HR. Following parasympathetic stimulation, HR slows. Following sympathetic stimulation, HR increases.
- Hypotension, Hypertension
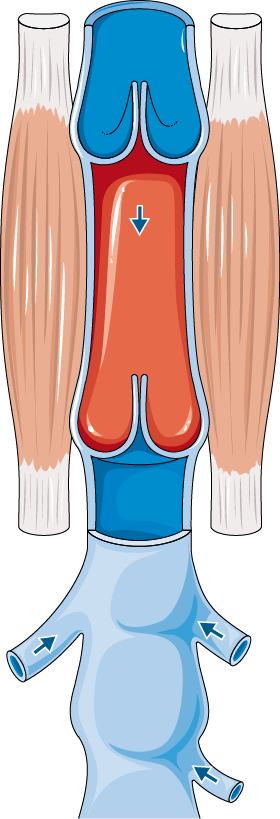
- Vasoconstriction, Vasodilation
- Local Regulation of blood flow – precapillary sphincters, vasoconstriction/dilation
-

Net filtration occurs near the arterial end of the capillary since capillary hydrostatic pressure (CHP) is greater than blood colloidal osmotic pressure (BCOP). There is no net movement of fluid near the midpoint since CHP = BCOP. Net reabsorption occurs near the venous end since BCOP is greater than CHP.
- Systemic Regulation of Blood Flow – neural and hormonal
- Summary of Factors Maintaining Vascular Homeostasis: Adequate blood flow, blood pressure, distribution, and perfusion involve autoregulatory, neural, and endocrine mechanisms.

- Summary of Factors Maintaining Vascular Homeostasis: Adequate blood flow, blood pressure, distribution, and perfusion involve autoregulatory, neural, and endocrine mechanisms.
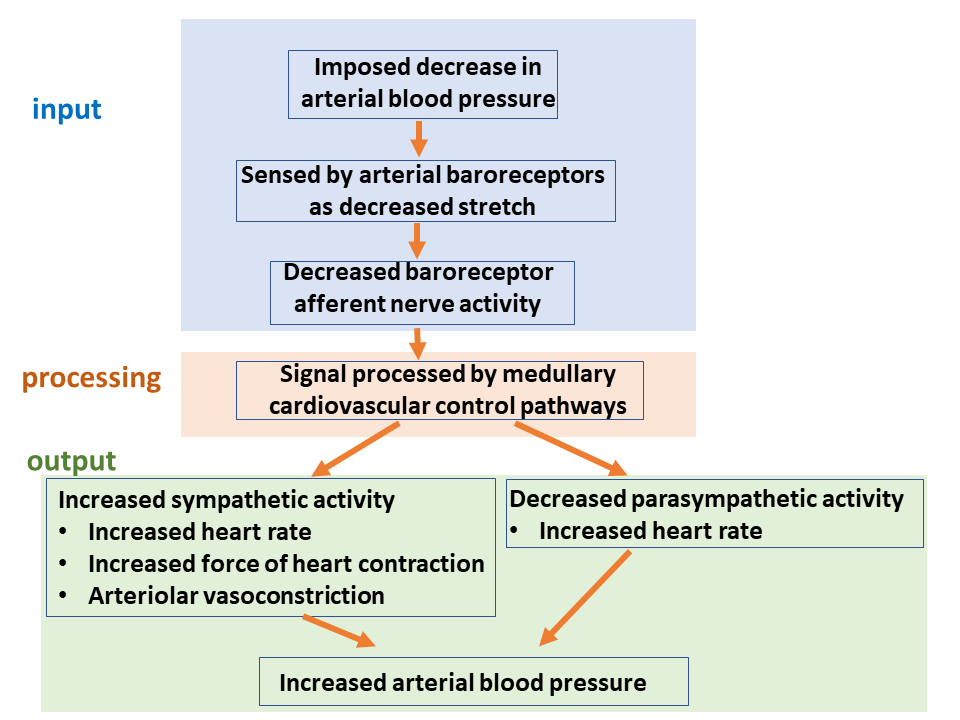
- Baroreceptor Reflex to maintain blood pressure homeostasis
- Baroreceptors, situated in blood vessels and heart chambers, are specialized stretch receptors sensitive to blood presence-induced stretching. They relay impulses to the cardiovascular center, contributing to blood pressure regulation.
-
- When blood pressure increases, the baroreceptors are stretched more tightly and initiate action potentials at a higher rate. At lower blood pressures, the degree of stretch is lower and the rate of firing is slower. When the cardiovascular center in the medulla oblongata receives this input, it triggers a reflex that maintains homeostasis
- Chemoreceptor Reflex to maintain blood oxygenation and pH homeostasis
- Chemoreceptors regulate oxygen, carbon dioxide, and pH levels, vital for vascular homeostasis. Positioned near baroreceptors in the aortic and carotid sinuses, they relay signals to the cardiovascular and respiratory centers in the medulla oblongata.
-
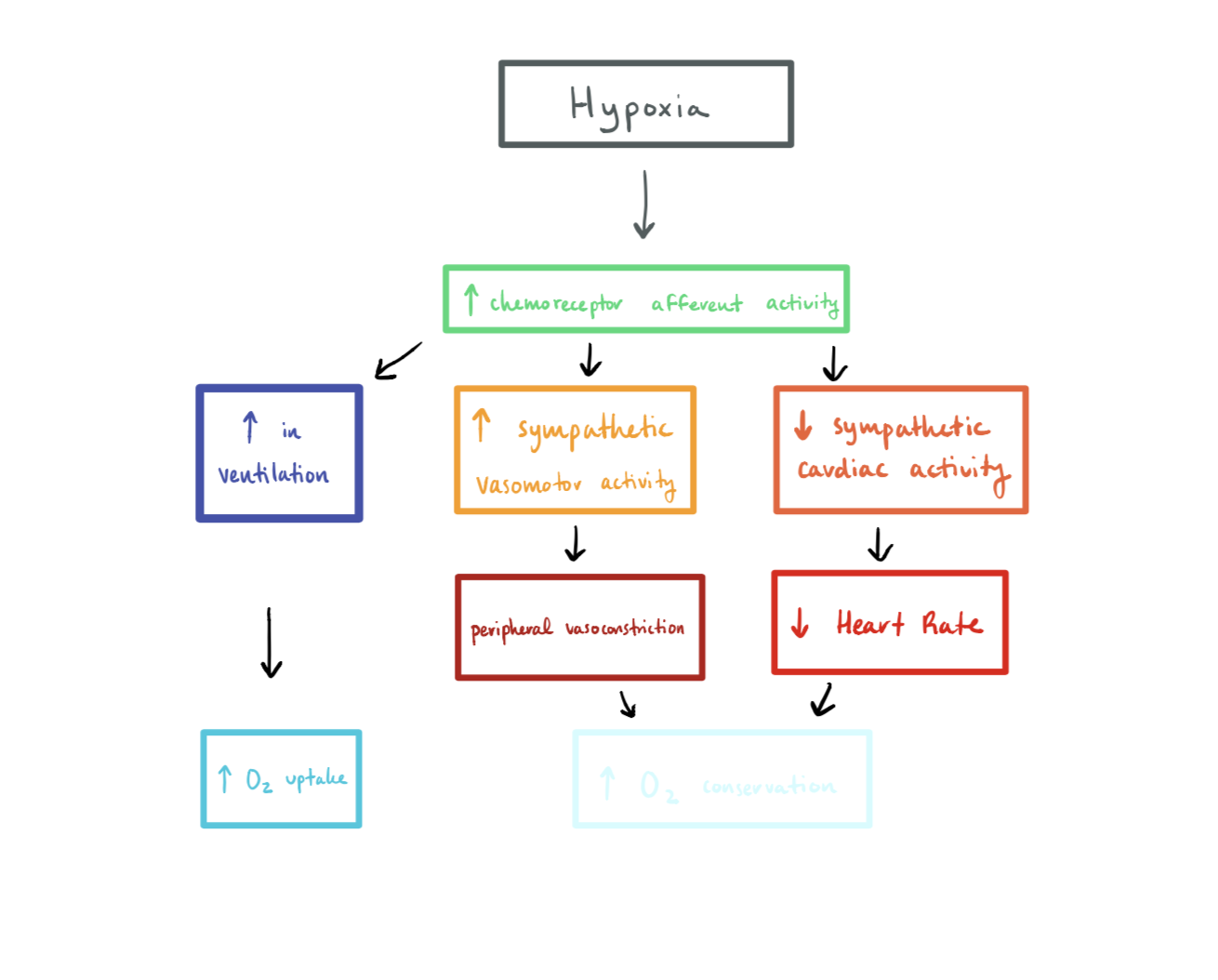
Chemoreceptor reflex response to hypoxia.
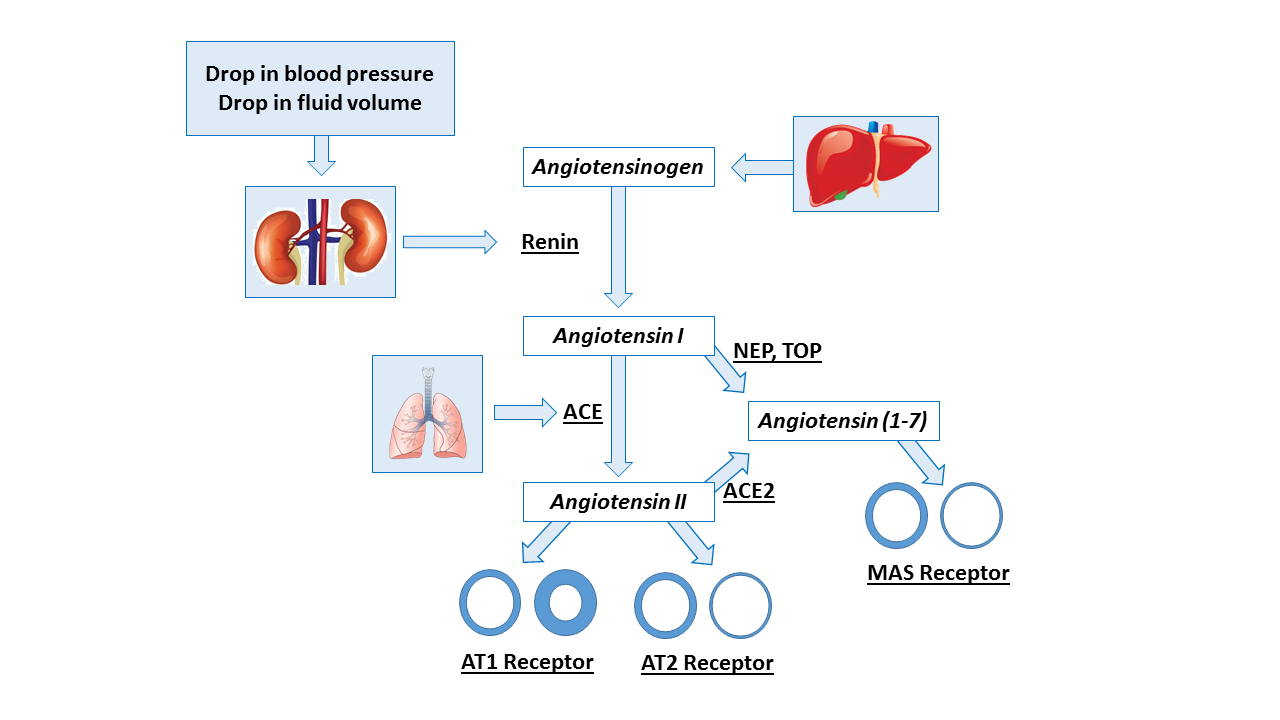
- Endocrine Regulation to increase blood pressure and volume using Renin, Angiotensinogen → Angiotensin I → Angiotensin II, ACE, ADH, Aldosterone, EPO, and thirst
-
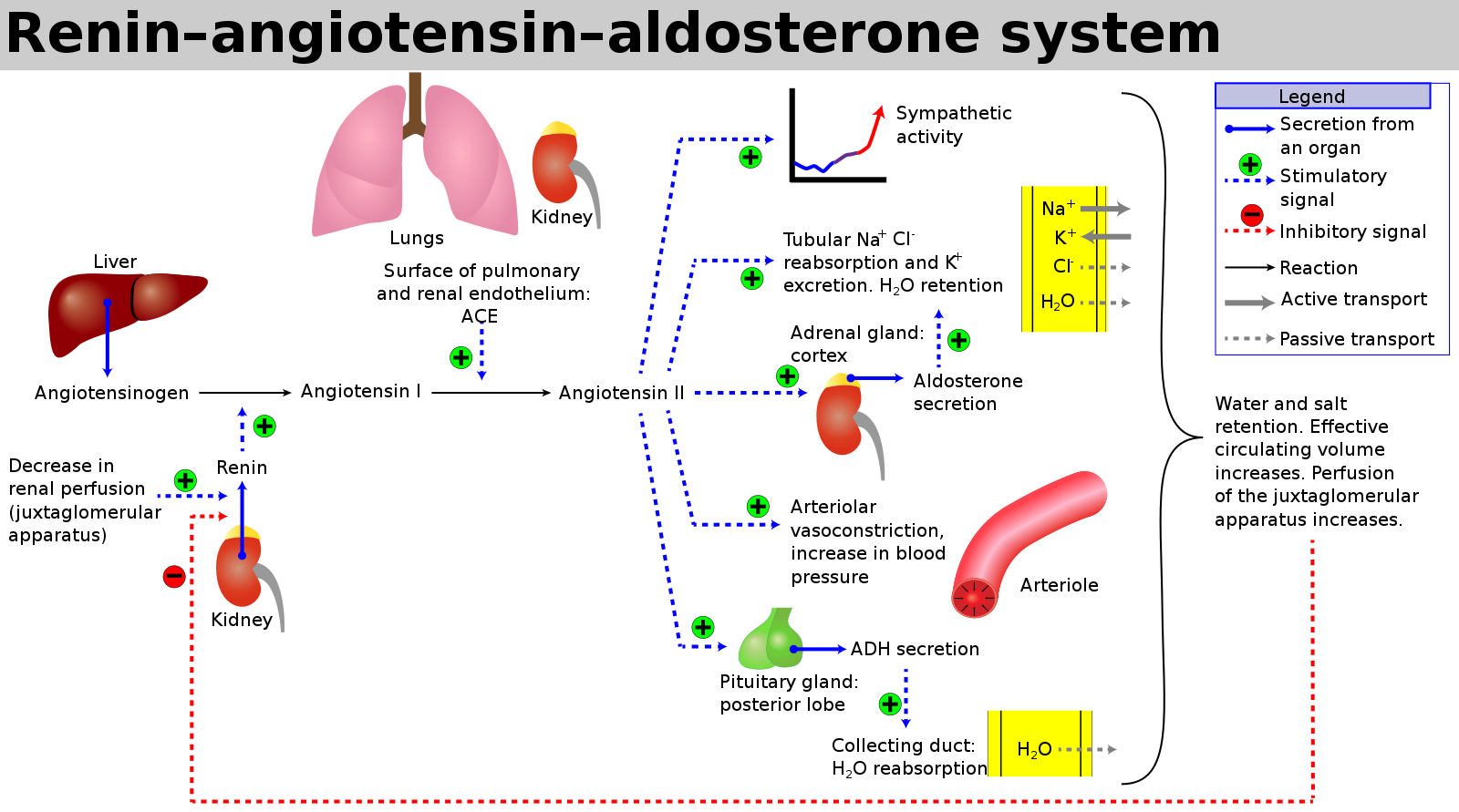
The renin–angiotensin system (RAS) or the renin–angiotensin–aldosterone system (RAAS). Start reading this schematic from the left, where it says “Decrease in renal perfusion (juxtaglomerular apparatus)”. Alternatively, the RAAS can also be activated by a low NaCl concentration in the macula densa or by sympathetic activation.
Legend info: Blue and red dashed arrows indicate stimulatory or inhibitory signals, which is also indicated by the +/-. In the tubule and collecting duct graphics, the grey dashed arrows indicate passive transport processes, contrary to the active transport processes which are indicated by the solid grey arrows. The other solid arrows either indicate a secretion from an organ (blue, with a starting spot) or a reaction (black). These 2 processes can be stimulated or inhibited by other factors.
- Endocrine Regulation to increase blood pressure and volume using ANP, BNP
- Diagnostic Tools – ECG, Ausculatation, 3D and 4D Echocardiography, Exercise Stress Tests, Electrocardiogram, X-rays, Angiography, CT scan, SPECT, Doppler Ultrasound, Central Venous Pressure, Pulmonary Wedge Capillary Pressure, Pulse Oximeter, Arterial blood gas monitor,
- Electrocardiogram (ECG)
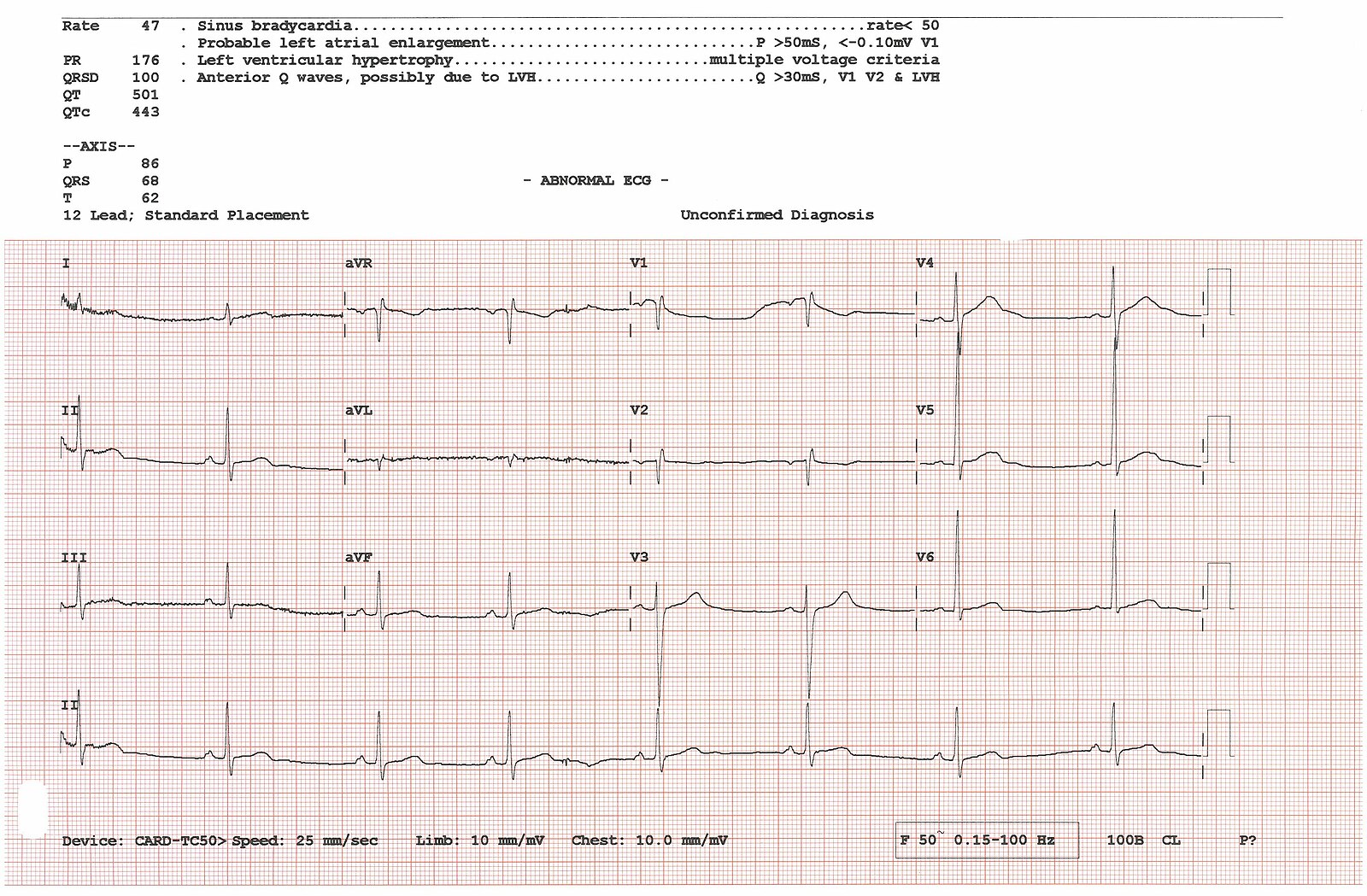
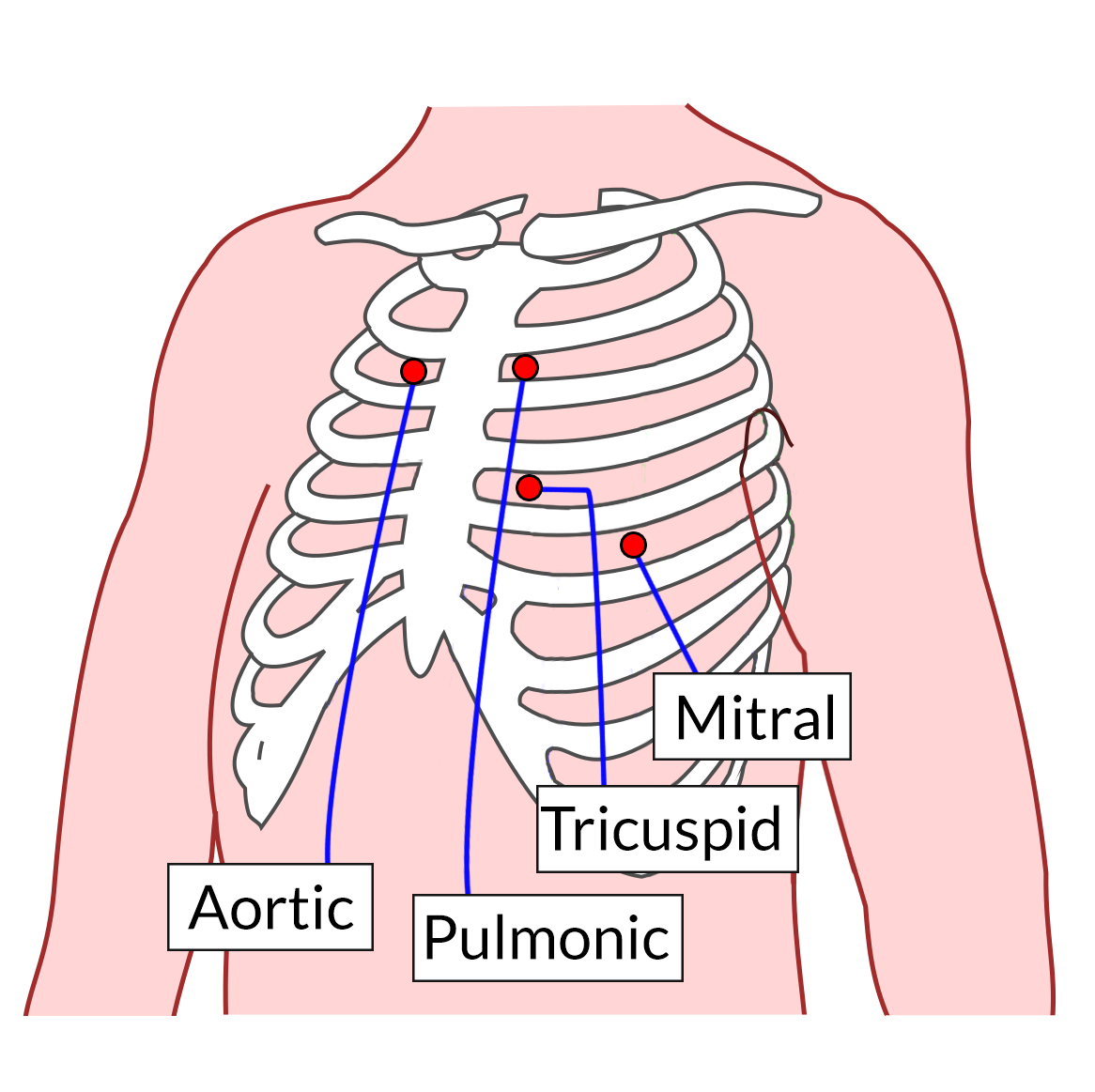
A 12-lead electrocardiogram (ECG) that was measured in clinical practice. - Ausculatation: During auscultation, it is common practice for the clinician to ask the patient to breathe deeply. This procedure not only allows for listening to airflow, but it may also amplify heart murmurs.
-
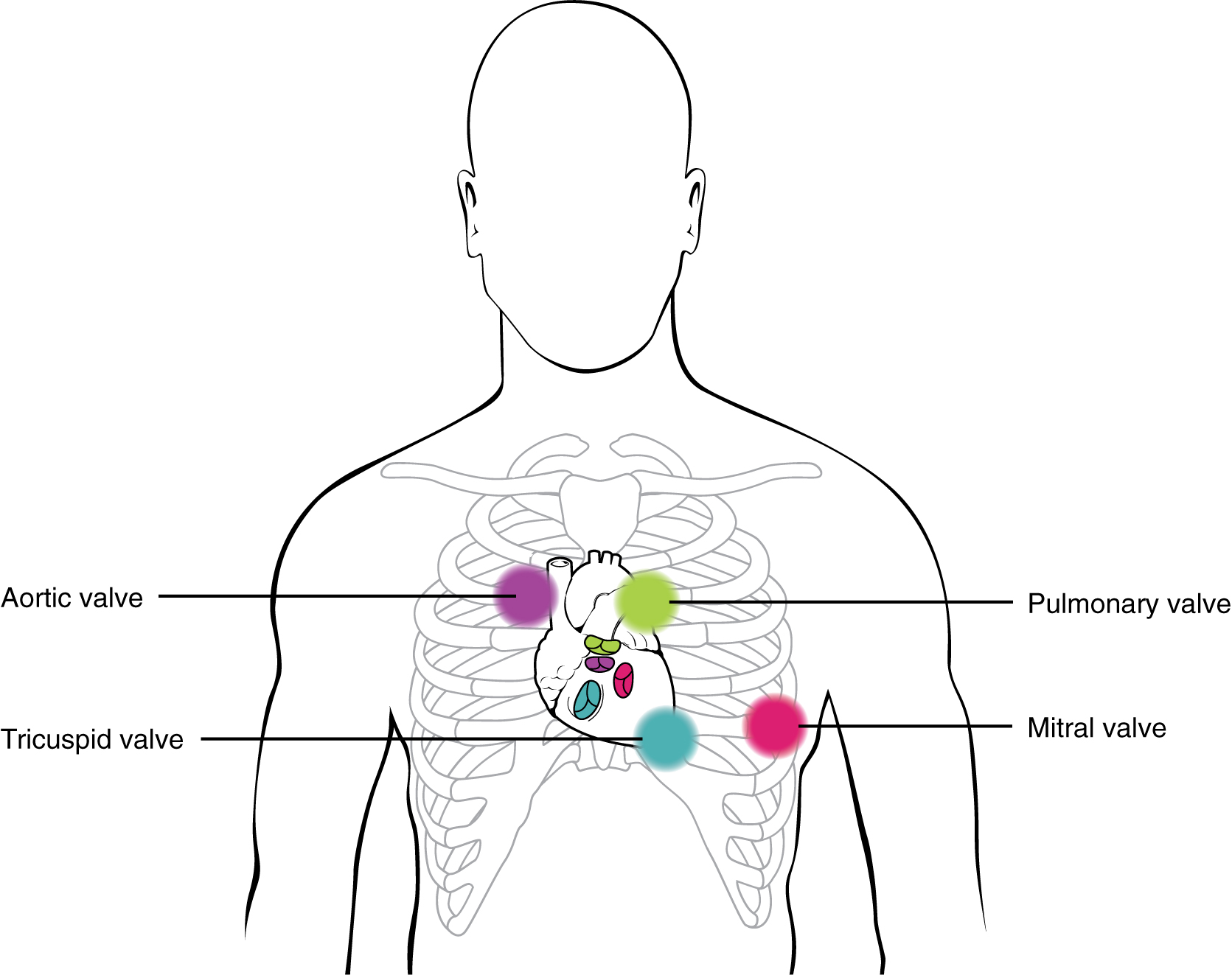
Stethoscope Placement for Auscultation: Proper placement of the bell of the stethoscope facilitates auscultation. At each of the four locations on the chest, a different valve can be heard.
- 3D and 4D Echocardiography
-
3D and 4D Echocardiography: a 3D-loop of a heart viewed from the apex, with the apical part of the ventricles removed and the mitral valve clearly visible. Due to missing data the leaflet of the tricuspid and aortic valve is not clearly visible, but the openings are. To the left are two standard two-dimensional views taken from the 3D dataset.
-
- Exercise Stress Tests
- X-rays
-

Chest X-ray (Normal). -
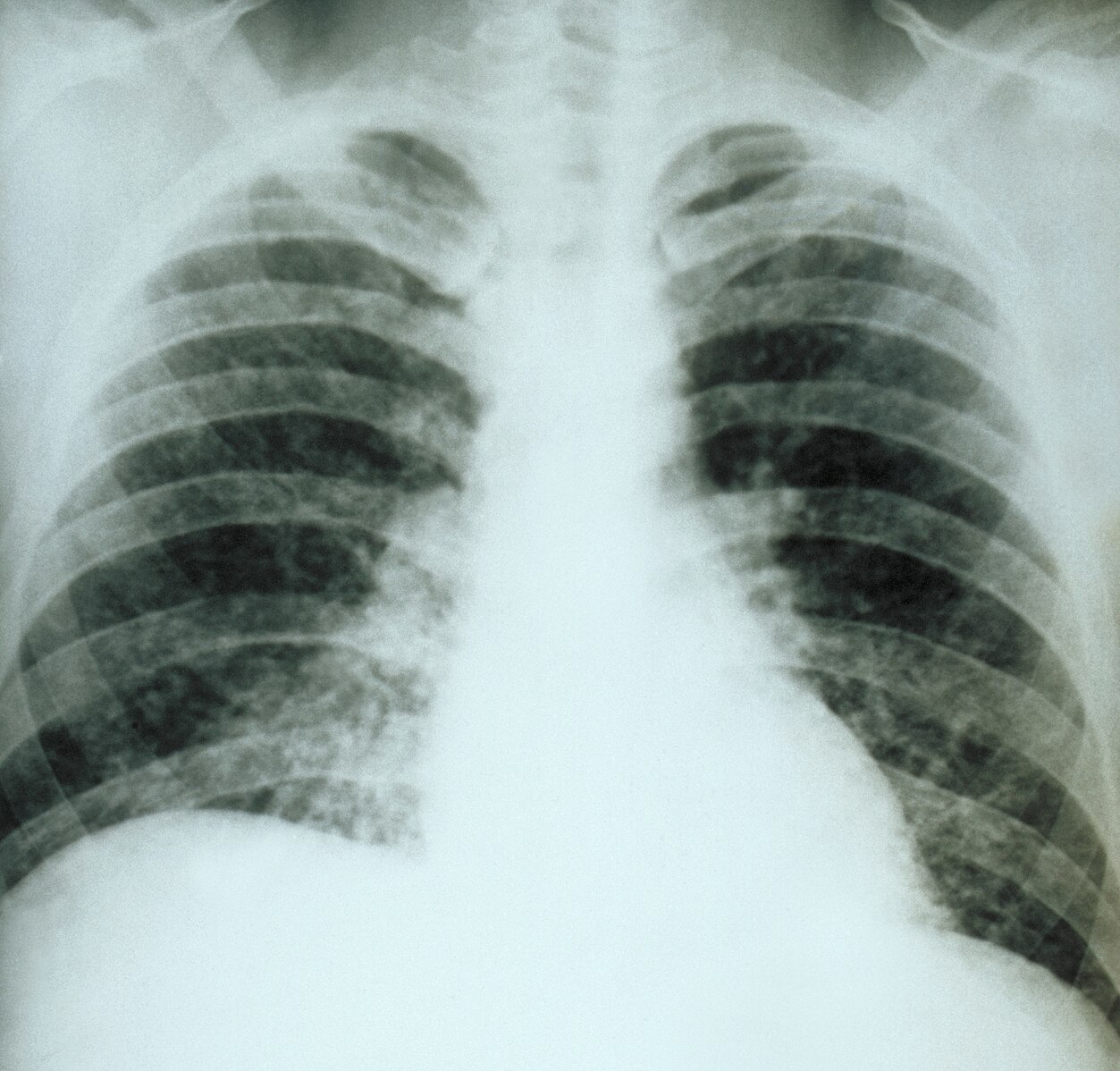
Chest X-ray (Acute Pulmonary Histoplasmosis).
-
- Angiography, CT scan, SPECT, Doppler Ultrasound, Central Venous Pressure, Pulmonary Wedge Capillary Pressure, Pulse Oximeter, Arterial blood gas monitor
-
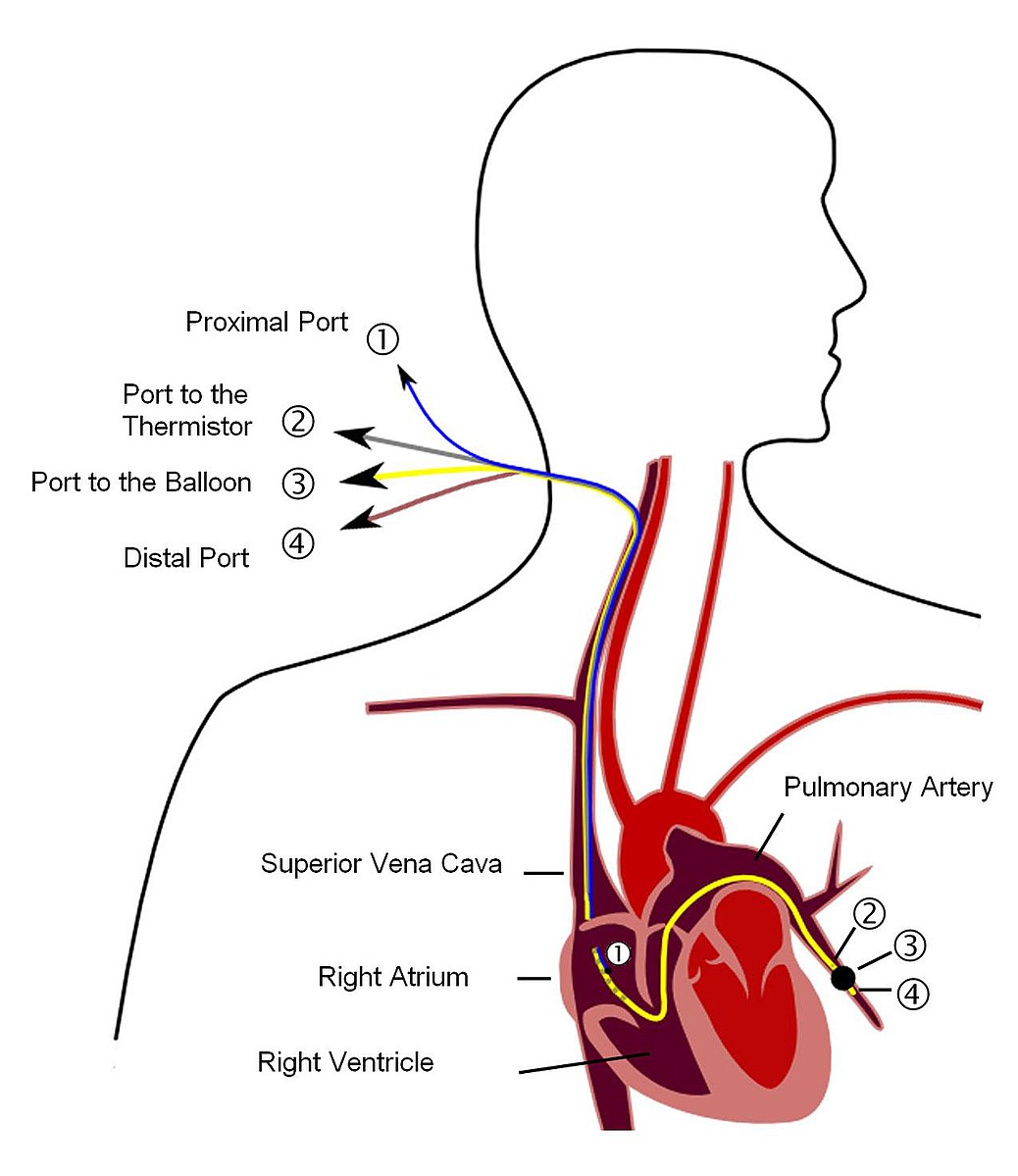
“The pulmonary capillary wedge pressure or PCWP is the pressure measured by wedging a pulmonary catheter with an inflated balloon into a small pulmonary arterial branch”: direct measure of pressure in pulmonary circuit & indirect measure of Left Atrial Pressure.
-
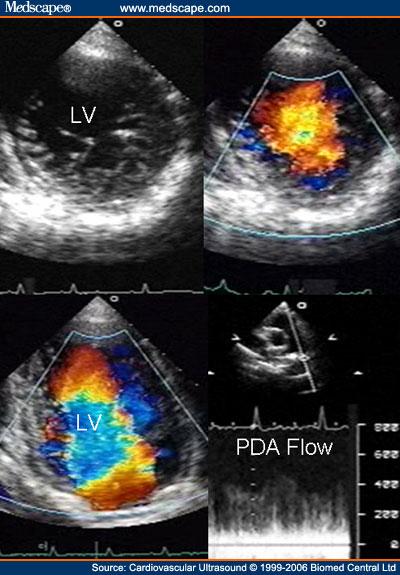
Transthoracic two-dimensional study with color and continuous wave Doppler shows left ventricular noncompaction associated with patent ductus arteriosus (PDA). Trabeculae and deep recesses with penetration of color can be observed in the left ventricle. Continuous wave Doppler from a suprasternal approach at the level of the great vessels registers systolic-diastolic flow through the ductus arteriosus. - SPECT
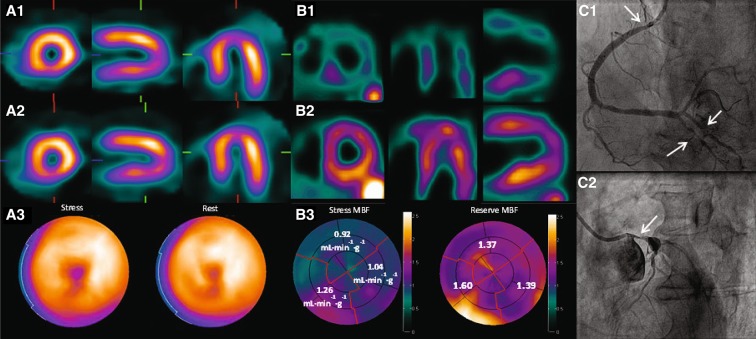
Tetrafosmin SPECT (A) and water-labeled PET (B) images of a patient with chest pain. Only the PET examination revealed balanced ischemia, confirmed by coronary angiography (C). - Pulse Oximeter
- Arterial blood gas monitor
- Electrocardiogram (ECG)
- General Treatment for Cardiac Disorders
- Summary of general treatment:
- Diet – cut fat (saturated and trans fat) and NaCl
- Exercise – decrease in serum lipids, pulse rate, and blood pressure; Increase in high-density lipoproteins (HDLs).
- Stop smoking – reduces vasoconstriction, heart rate, serum lipids, platelet adhesion, and risk of thrombus.
- Medication: vasodilators, beta blockers, alpha blockers, calcium channel blockers, digoxin, ACE inhibitors, diuretics, potassium sparing diuretics, anticoagualants, cholesterol/lipid lowering drugs.
- Vasodilators
- Vasodilators such as nitroglycerin are employed to prevent angina, heart attacks, and manage congestive heart failure (CHF).
- Mechanisms:
- Decrease peripheral resistance, thereby reducing the workload of the heart
- Increase oxygen supply to the heart by acting as coronary and systemic vasodilators and venodilators (decreasing preload and afterload, which leads to increased cardiac output).
- Decrease in blood pressure (BP), if excessively low, may result in dizziness.
- Beta-blockers
- Beta-blockers such as metoprolol and atenolol are prescribed for hypertension, dysrhythmias, and congestive heart failure (CHF).
- They work by blocking β1-adrenergic receptors, thereby helping to regulate heart rate and blood pressure.
- Alpha blockers
- Alpha blockers function by blocking α1-adrenergic receptors in arteries, resulting in vasodilation.
-
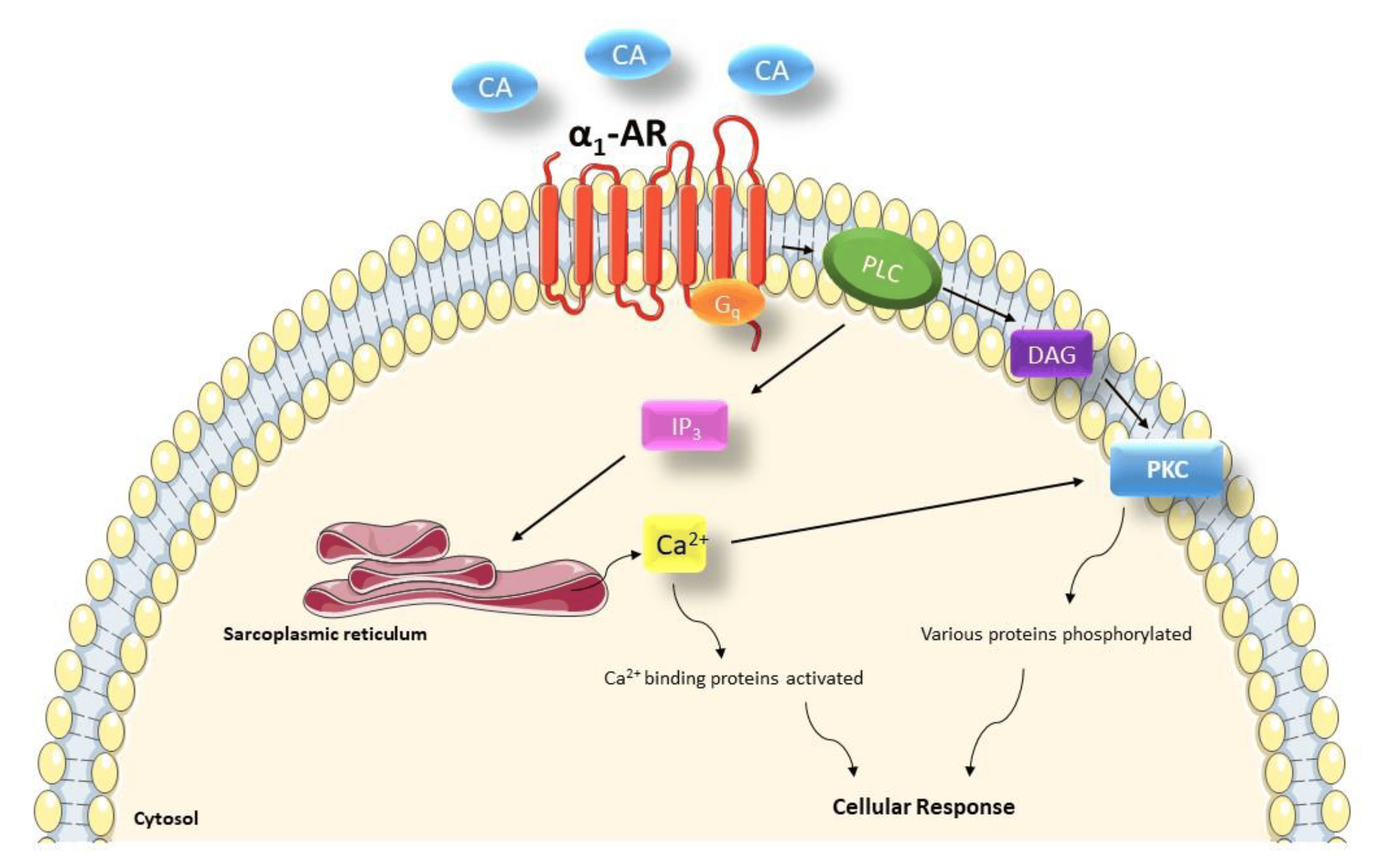
Alpha blocker: block α1-adrenergic R in arteries = vasodilation.
The prototypical signaling pathway of α1-ARs. CA: catecholamines, DAG: diacylglycerol, IP3: inositol triphosphate, PKC: protein kinase C, PLC: phospholipase C.
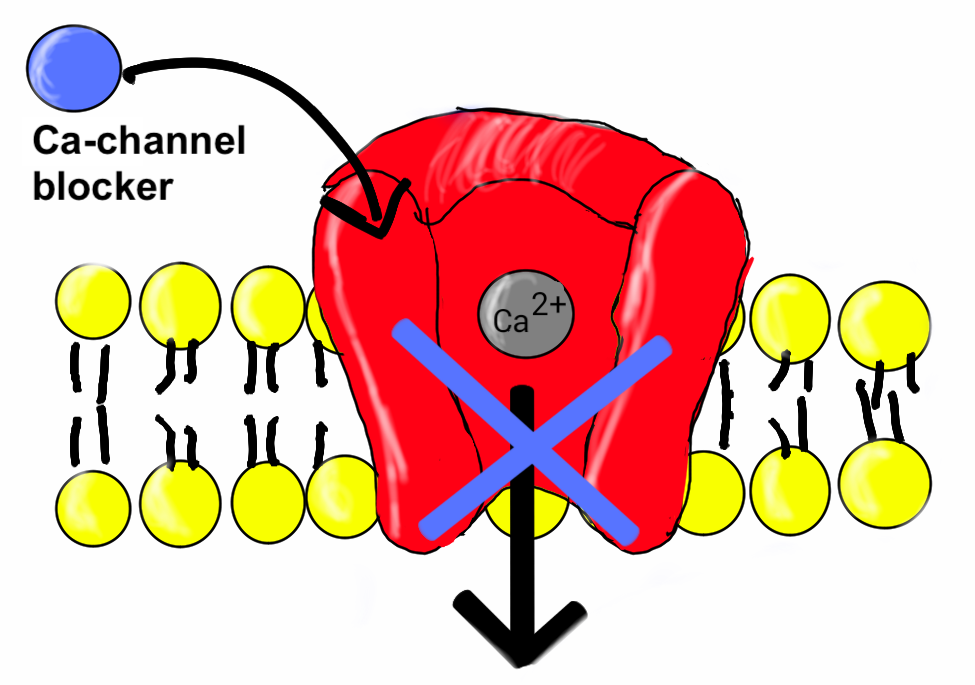
- Ca-channel blockers
- Calcium channel blockers function by blocking calcium from entering the heart and smooth muscle cells. This action decreases heart contractility and causes vasodilation, making them useful for antihypertensive and angina prophylaxis. There are different types of calcium channel blockers:
- Type 2 blockers (e.g., Diltiazem) are more specific for the heart, reducing conduction (heart rate) and contractility.
- Type 3 blockers (e.g., Verapamil) reduce heart rate, preventing tachycardia and fibrillation.
- Type 4 blockers (e.g., Nifedipine, Amlodipine/Norvasc) act as peripheral vasodilators, reducing blood pressure by decreasing large vessel stiffness, particularly in the elderly.
- Calcium channel blockers cause vasodilation.
- Calcium channel blockers function by blocking calcium from entering the heart and smooth muscle cells. This action decreases heart contractility and causes vasodilation, making them useful for antihypertensive and angina prophylaxis. There are different types of calcium channel blockers:
- Digoxin
- Digoxin, a cardiac glycoside, is utilized to manage dysrhythmias such as atrial fibrillation (uncoordinated) and atrial flutter (250-350 bpm), along with cardiac failure.
- It works by inhibiting the Na+/K+ pump, leading to a buildup of Na+. Consequently, the Na+/Ca++ exchanger brings in more Ca++, accumulating in the sarcoplasmic reticulum (SR) for release with each contraction. This action reduces conduction and heart rate (HR), resulting in fewer but stronger contractions.
- Caution: toxicity.
-
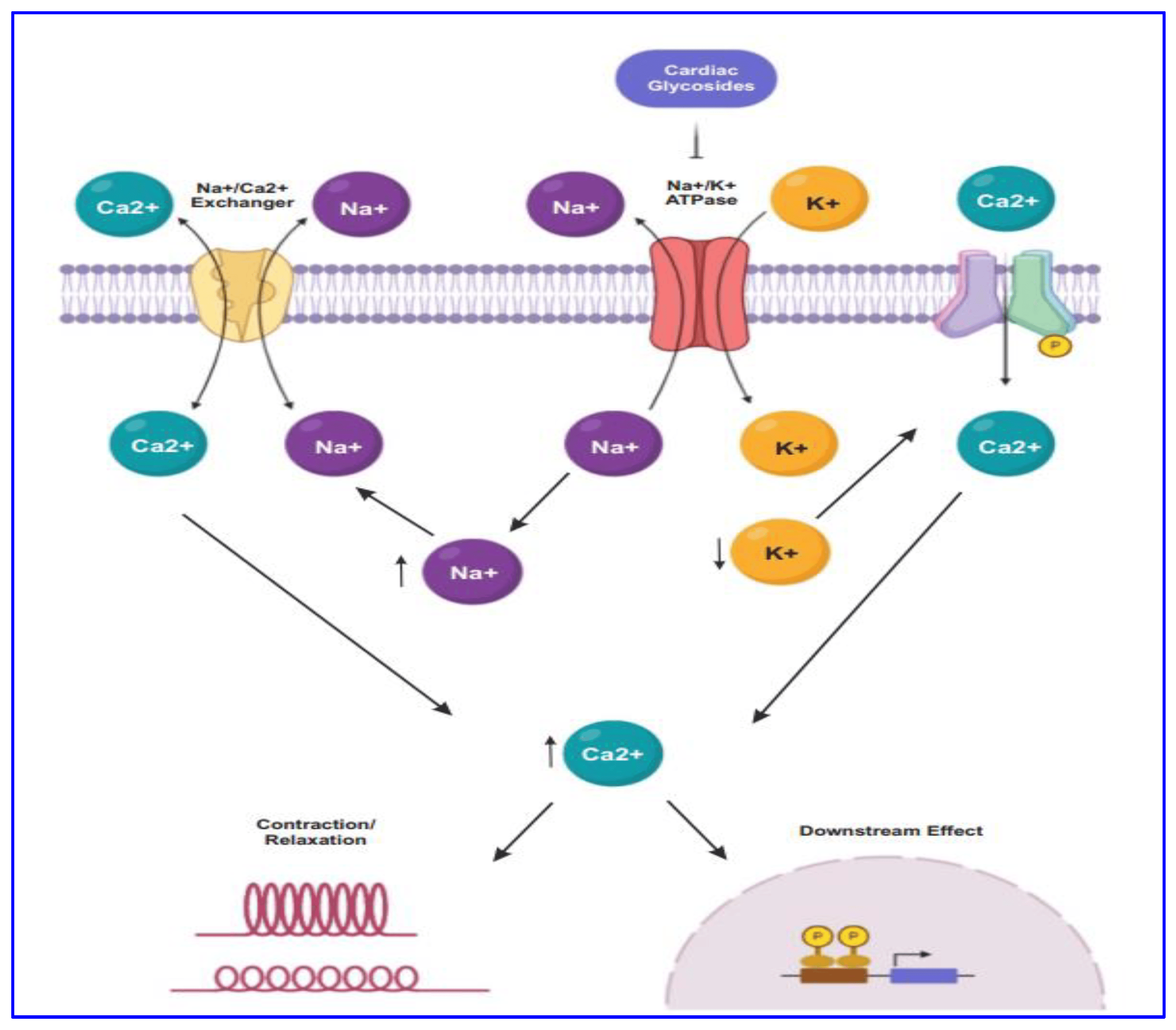
Digoxin – Cardiac glycoside: The mode of action of cardiac glycoside through targeting Na+/K+-ATPase by maintaining the concentration of sodium-potassium gradient across the plasma membrane. Cardiac glycoside binds to the Na+/K+-ATPase pump, thus inhibiting it, resulting in intracellular retention of Na+ and increasing the concentration of Ca2+. Subsequently, lower expression of Na+/K+-ATPase. – Inhibit Na+/K+ pump; – Na+ builds up so Na+/Ca++ exchanger brings in more Ca++ which builds up in SR (for release with each contraction). – ↓conduction so ↓HR = Less frequent rate but stronger contractions – caution: toxicity
- Anti-hypertensive drugs: to lower BP back to normal
- Beta blockers (adrenergic blockers): reduce heart rate and contractility
- Ca2+ channel blockers: vasodilation
- Alpha blockers: block α1-adrenergic R in arteries leading to vasodilation
- Angiotension-converting enzyme inhibitors (ACE inhibitors):
- Block the conversion of angiotensin I to angiotensin II
- Reduce vasoconstriction and secretion of aldosterone and ADH
- Decrease sodium and water retention, thereby reducing blood volume.
- Advantage: Lowers preload and afterload, contributing to improved cardiac function.
- Diuretics:
- “Water pills” block sodium and water reabsorption.
-
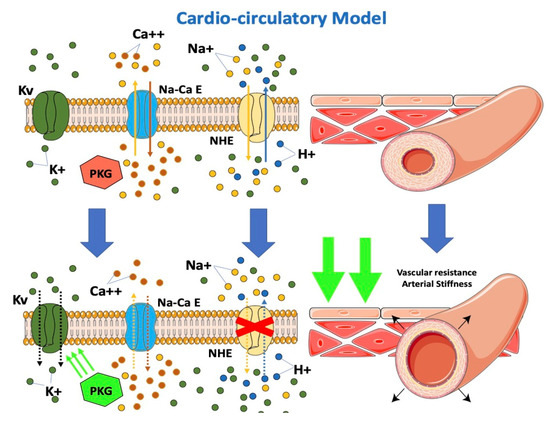
From the cardio-circulatory model’s point of view, diuretics would be effective in reducing afterload by reducing cardiovascular resistances. -
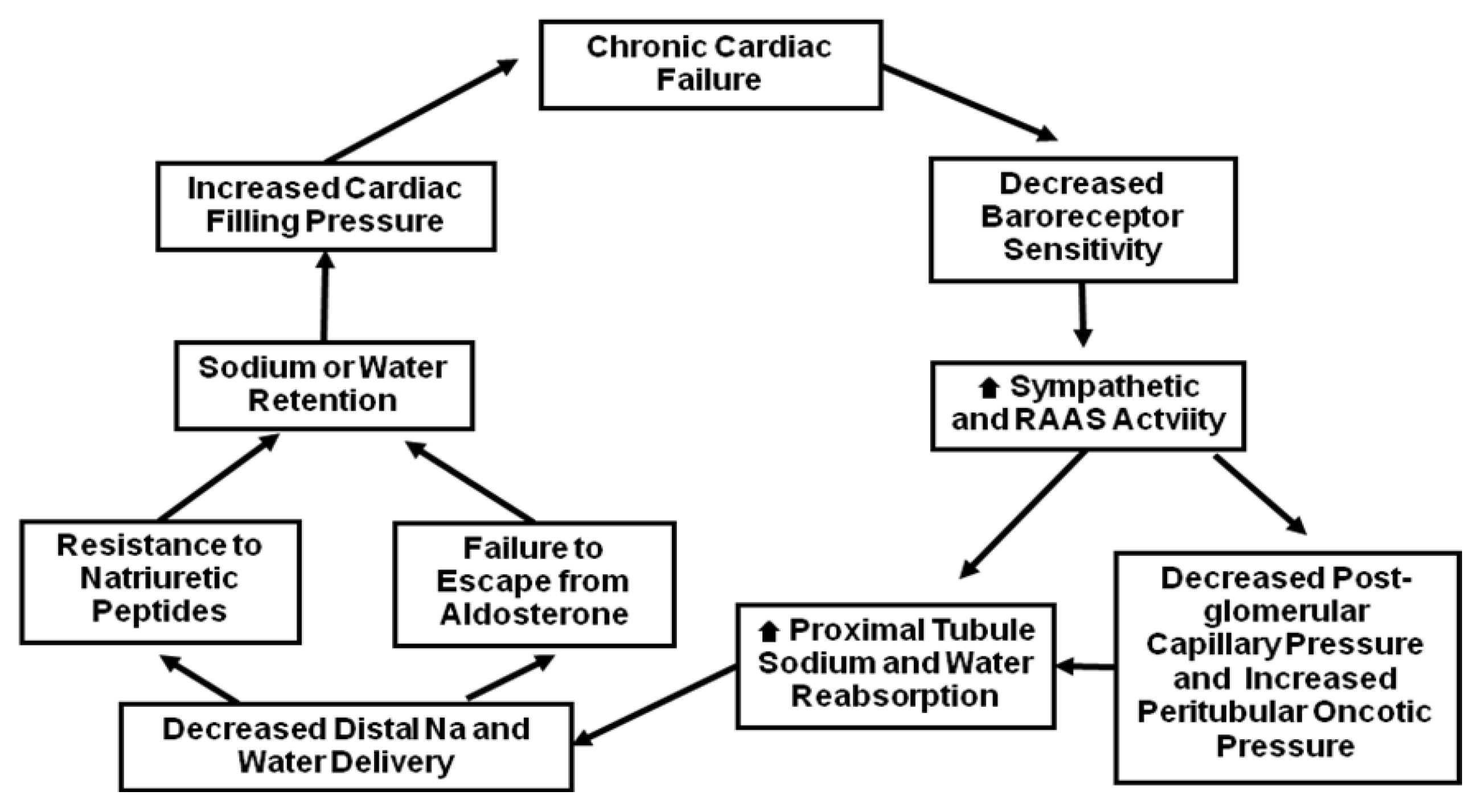
Vicious cycle of sodium and water retention in chronic heart failure.
- Anticoagulants “blood thinners”
- Examples: heparin, warfarin, streptokinase, urokinase, TPA, and ASA
- Reduce the risk of blood clot formation
- Prevent platelet aggregation (blood clotting)
- Small daily doses of aspirin (ASA) are commonly used
- However, their use carries a risk of increased bleeding tendencies
- Cholesterol/lipid-lowering drugs
- Commonly referred to as “statins” (such as Zocor and Lipitor)
- Block the synthesis of LDL and cholesterol in the liver
- Aim to prevent the buildup of atheromas (atherosclerosis)
- Selected cardiovascular drugs
Name Use Action Adverse Effects Nitroglycerin Angina attacks and prophylaxis Reduces cardiac workload, peripheral and coronary vasodilator Dizziness, headache Metroprolol (Lopressor) Hypertension, angina, antiarrhythmic Blocks beta-adrenergic receptors, slows heart rate Dizziness, fatigue Nifedipine (Adalat) Angina, hypertension, peripheral vasodilator, antiarrhythmic Calcium blockers, vasodilator Dizziness, fainting, headache Digoxin (Lanoxin) Congestive heart failure and atrial arrhythmias Slows conduction through AV node and increases force of contraction (cardiotonic) to increase efficiency Nausea, fatigue, headache, weakness Enalapril (Vasotec) Hypertension ACE inhibitor — blocks formation of angiotensin II and aldosterone Headache, dizziness, hypotension Furosemide (Lasix) hypetension Edema with CHF, hypertension Diuretic — increases excretion of water and sodium Nausea, diarrhea, dizziness Simvastatin (Zocor) Hypercholesterolemia (CHD) Decreases cholesterol and LDL Digestive discomfort Warfarin (Coumadin) Prophylaxis and treatment of thromboemboli Anticoagulant — interferes with vitamin K in synthesis of clotting Excessive bleeding (antidote: vitamin K) ASA (aspirin) Prophylaxis of thromboemboli Prevents platelet adhesion, anti-inflammatory Gastric irritation, allergy
- Summary of general treatment:
- Arteriosclerosis
- Atherosclerosis
-
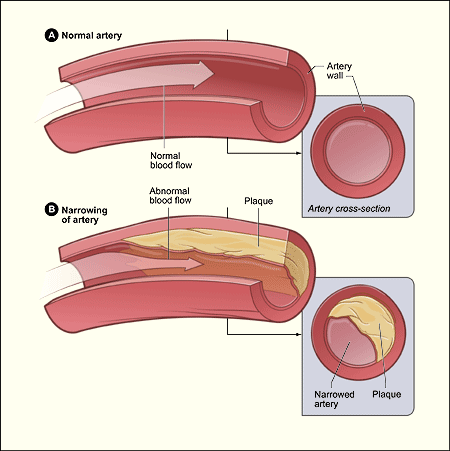
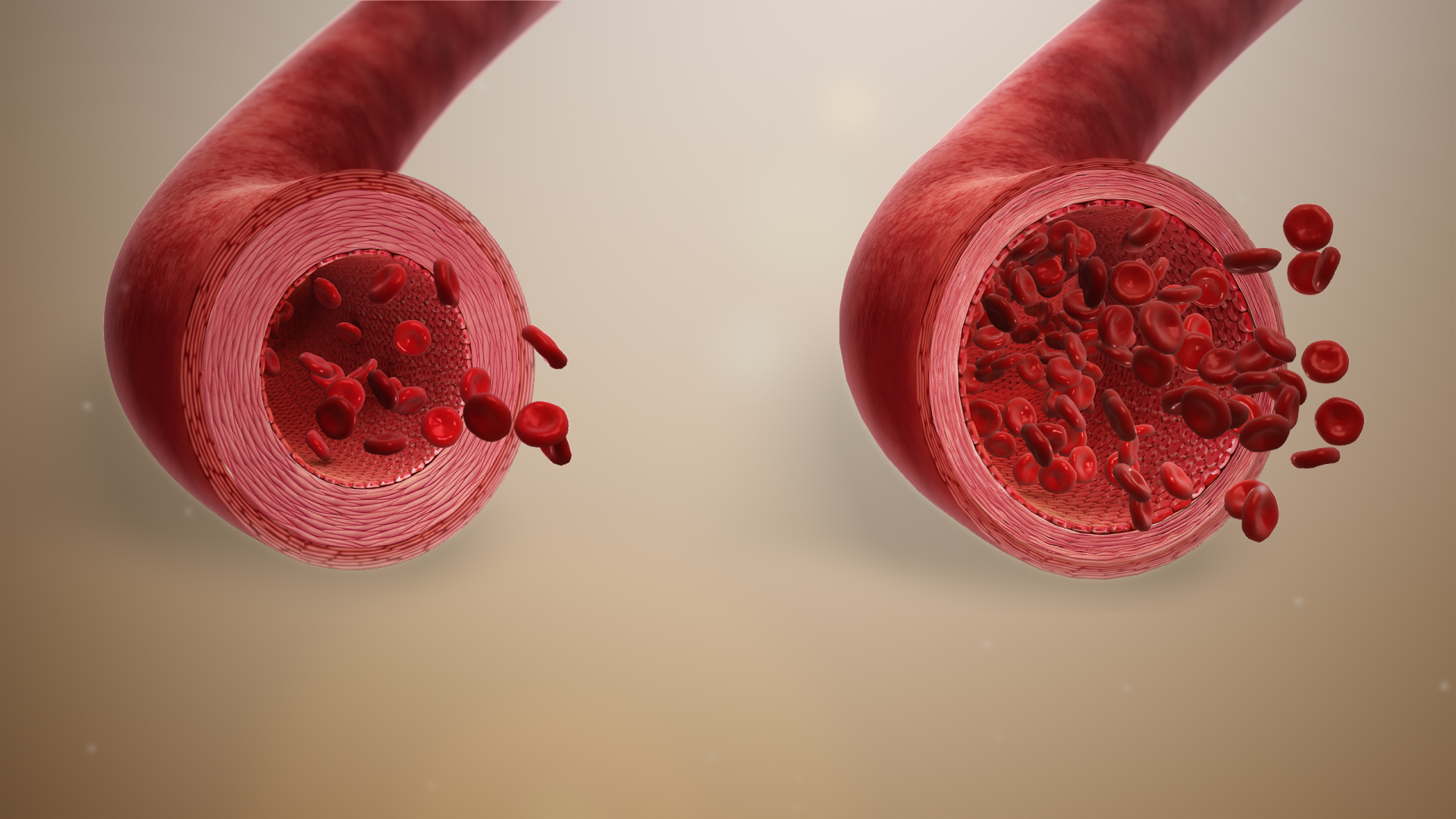
The illustration shows a normal artery with normal blood flow (figure A) and an artery containing plaque buildup (figure B). -
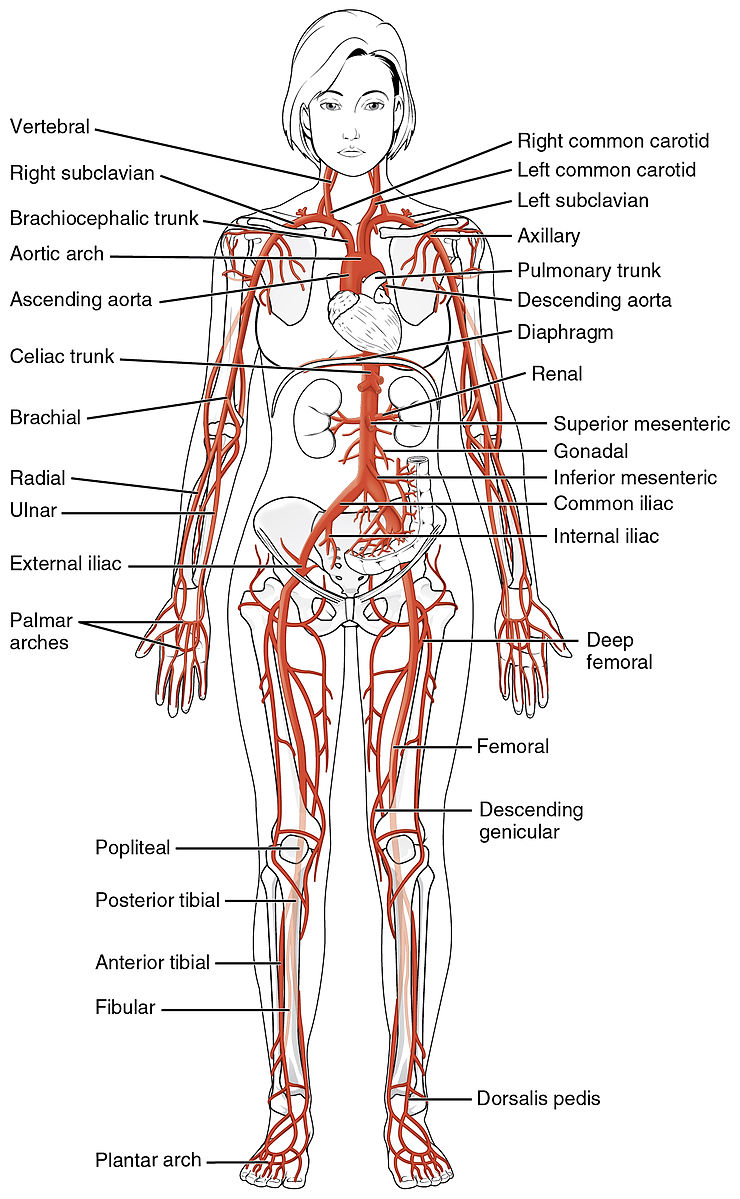
Major Systemic Artery. Atherosclerosis is the presence of atheromas in large arteries. It commonly forms in large arteries, including the aorta, iliac arteries, coronary arteries, carotid arteries, and points of bifurcation. -

(a) Normal thoracic aorta in a child; (b) Severe atherosclerosis of the aorta in an old man.
-
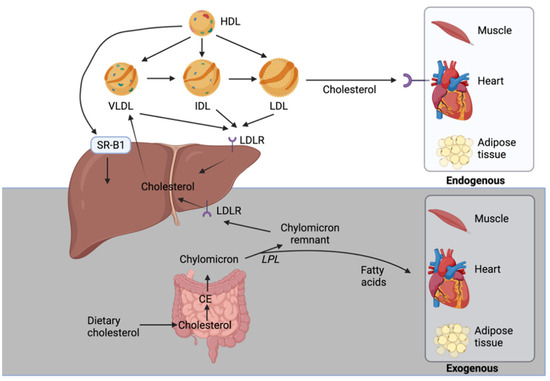
- HDLs, LDLs,
- Atheroma formation, thrombi, emboli
-
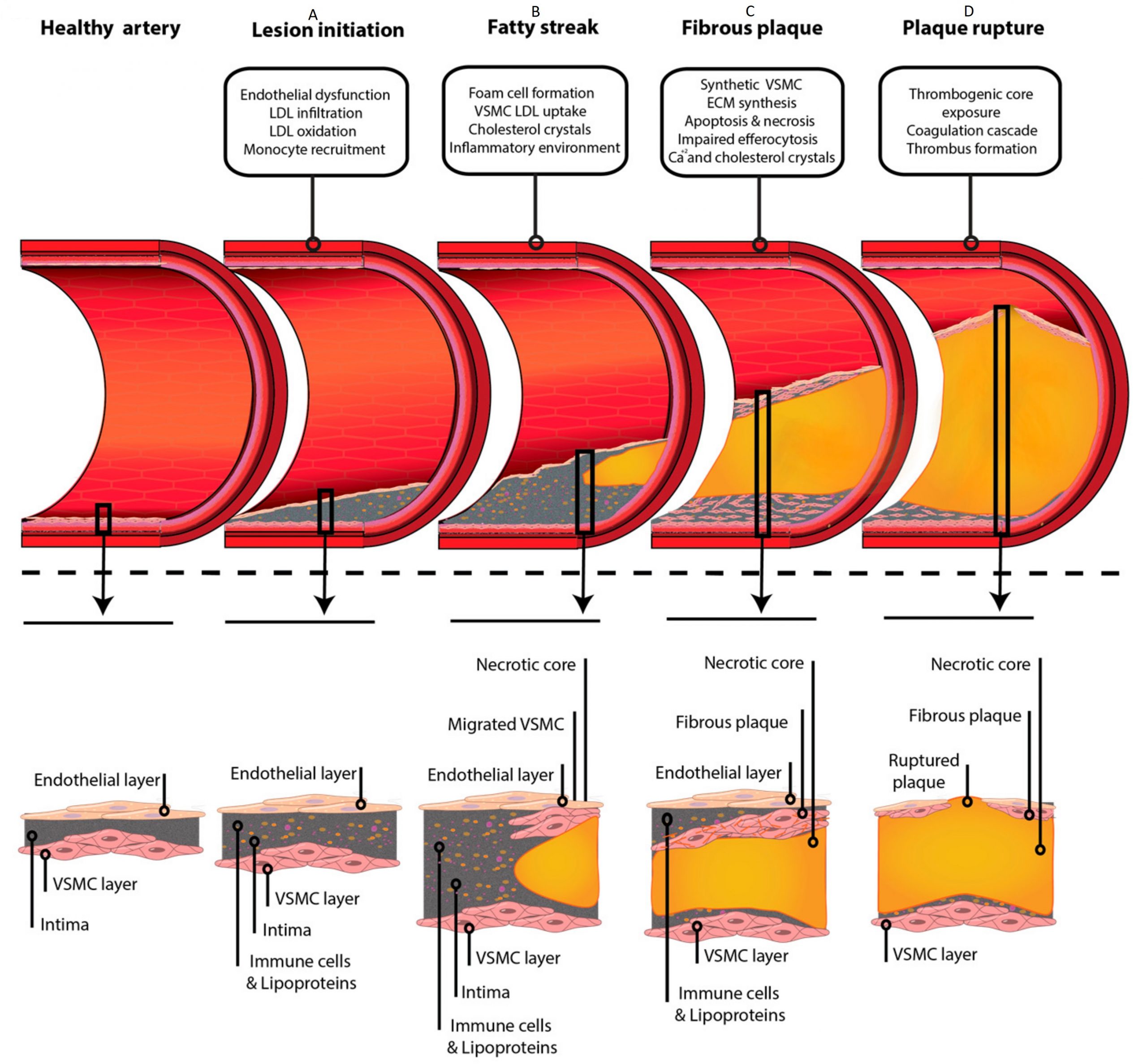
Schematic representation of atheroma plaque formation from a healthy artery to plaque rupture underlying the most important events that contribute to its development in each stage. -
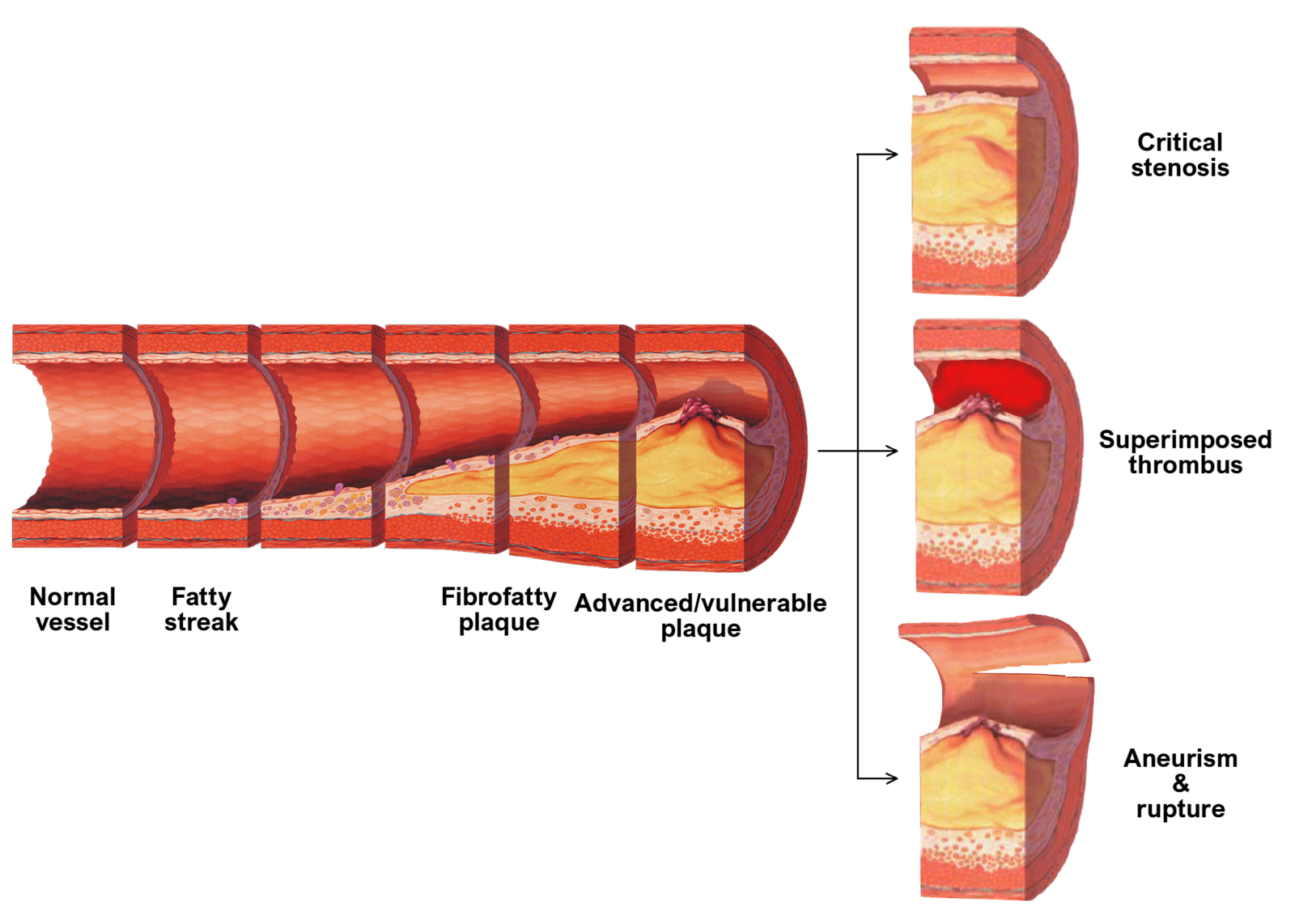
Late complications of atherosclerosis. -
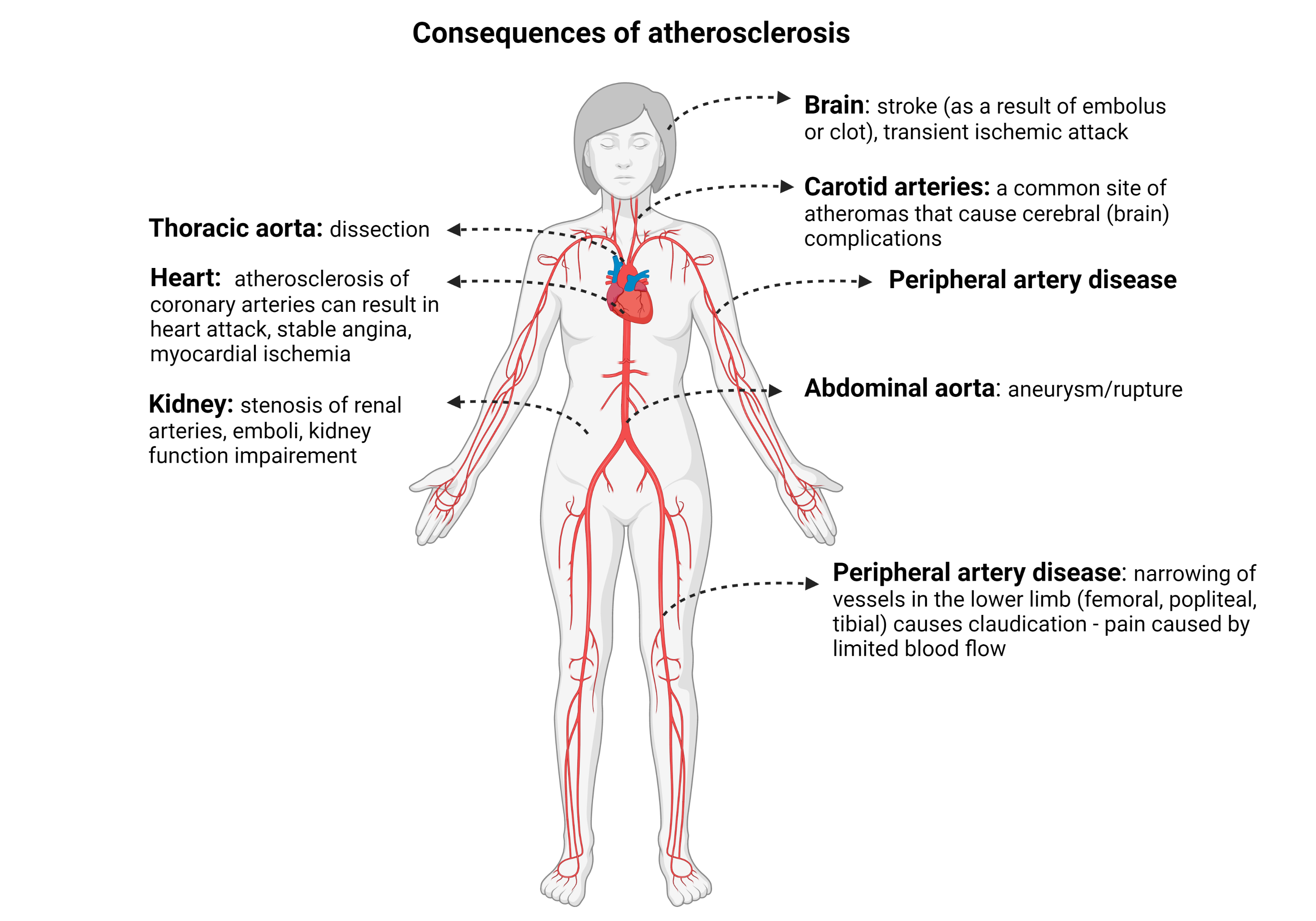
Clinical consequences of atherosclerosis. Created by Tetiana Povshedna with Biorender.com, under its creative commons license
-
- Coronary Bypass Graft
-
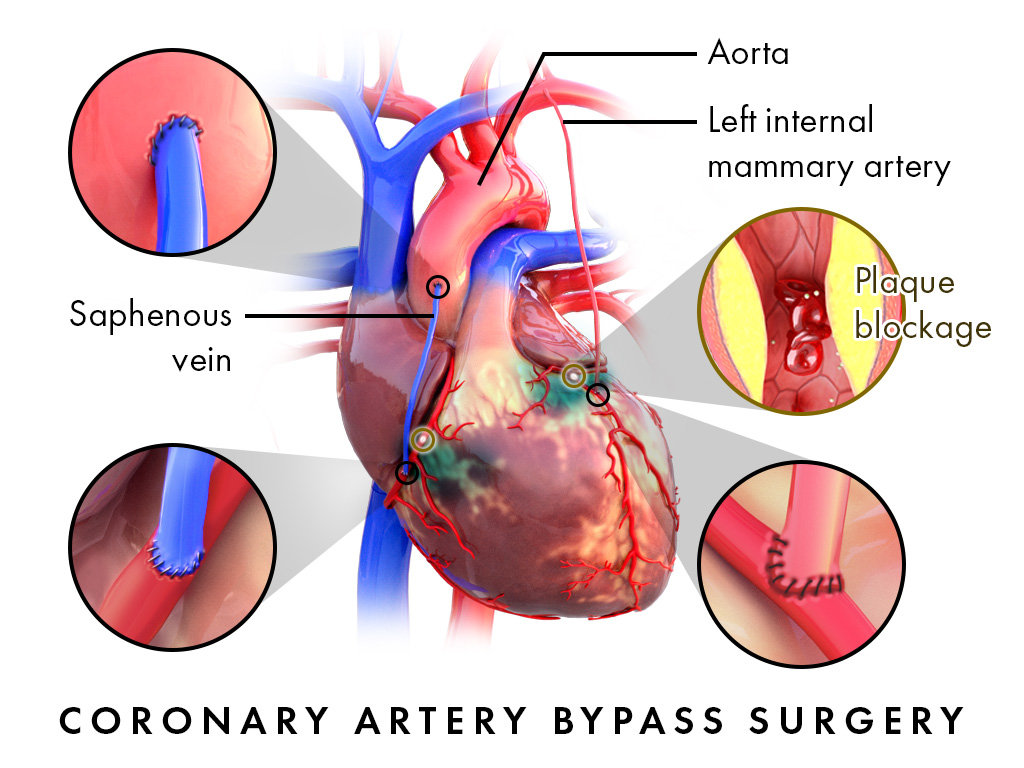
Coronary Artery Bypass Graft.
-
- Angina Pectoris
-
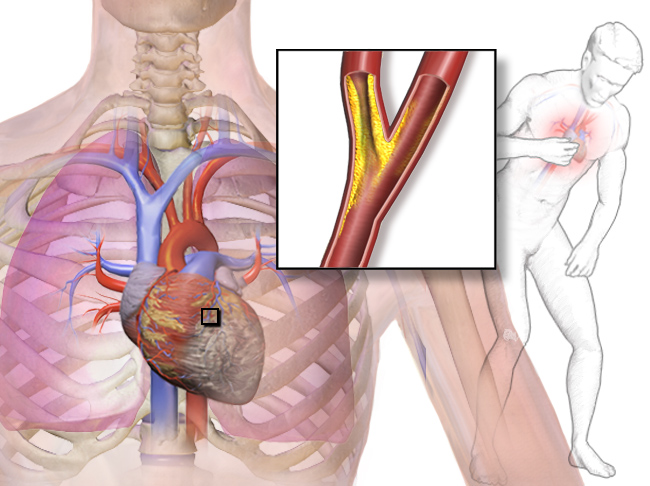
Angina. - `
-
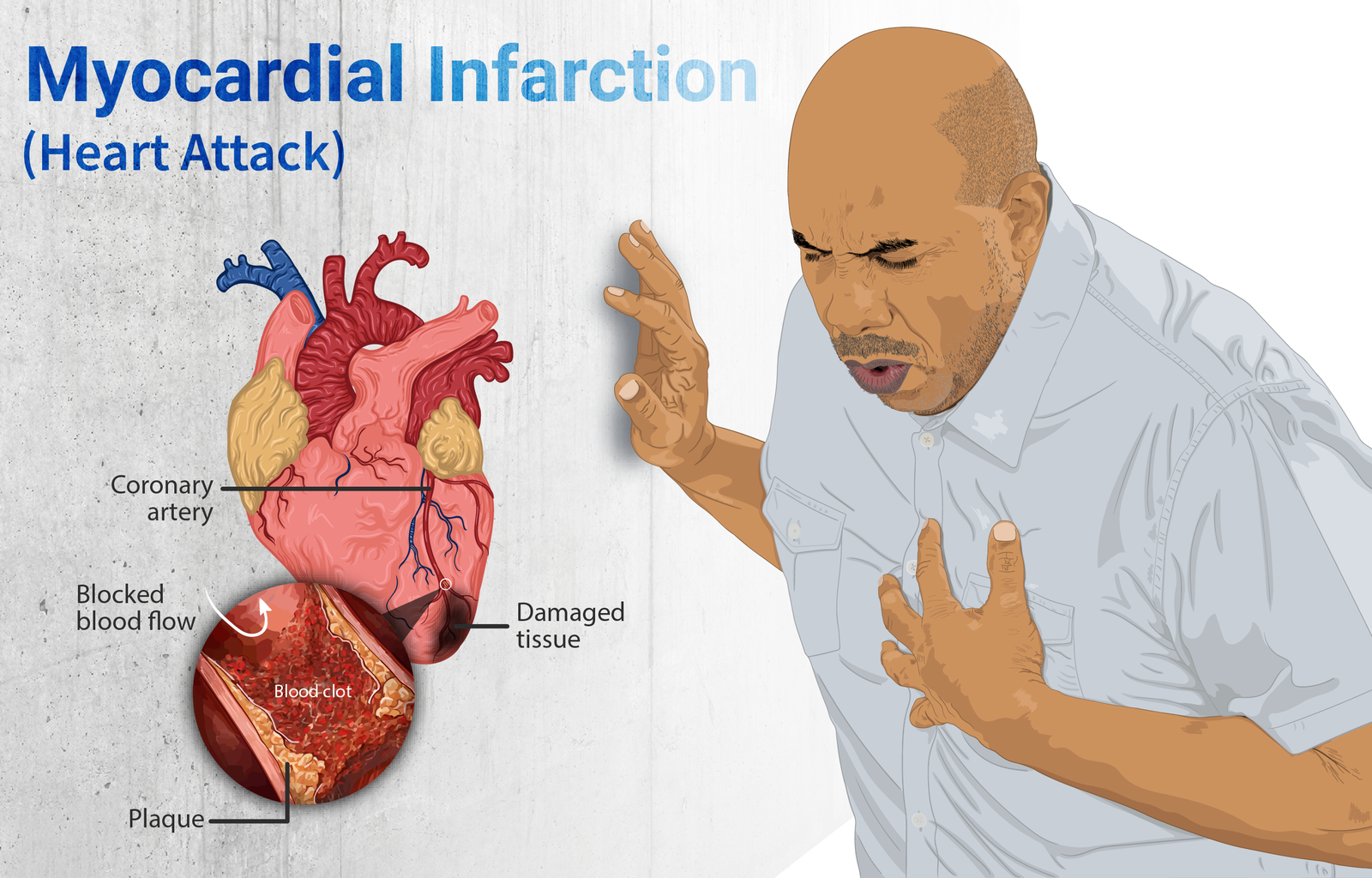
- Myocardial Infarction
-
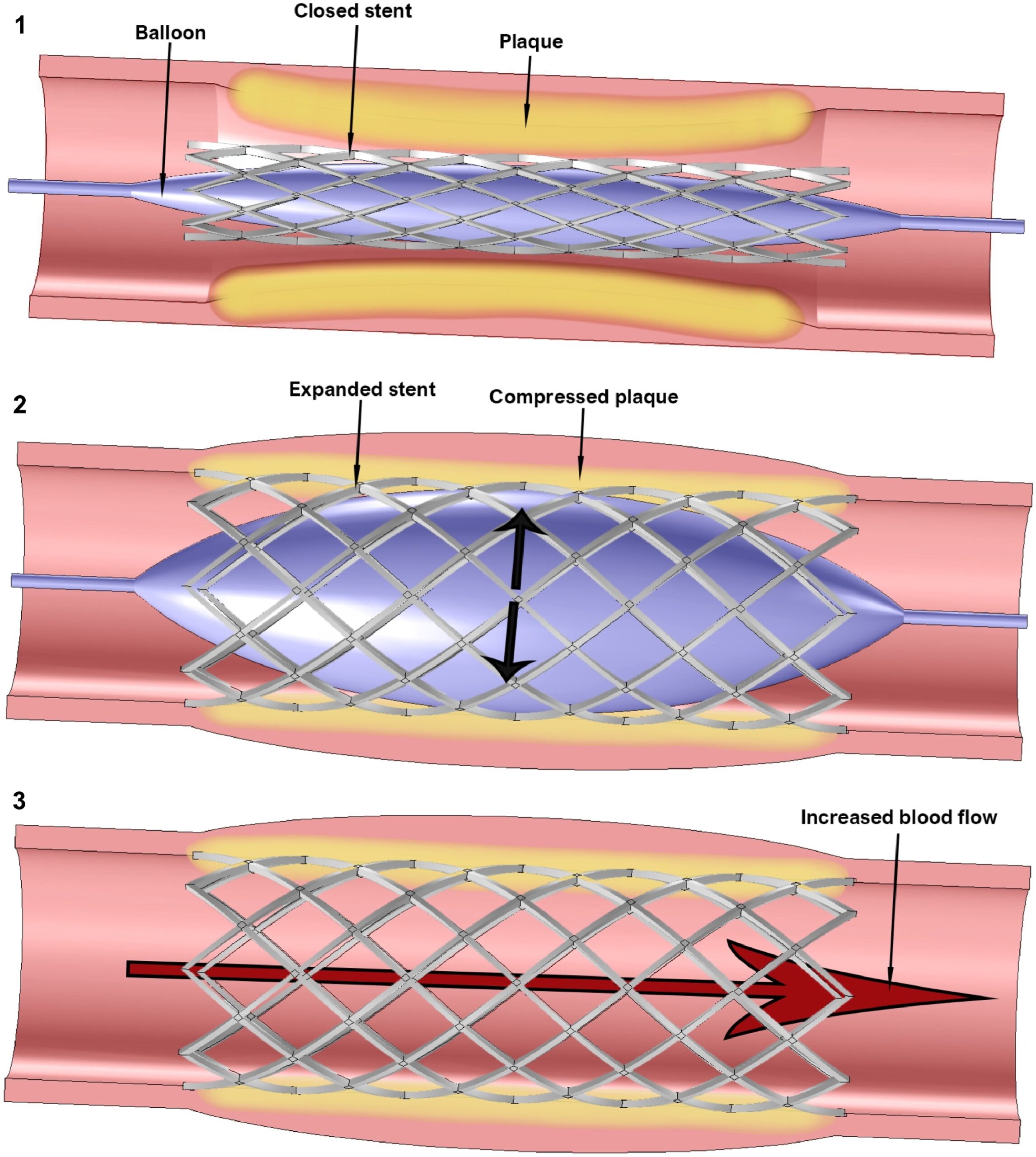
Stent placement
- Peripheral Vascular Disease
-
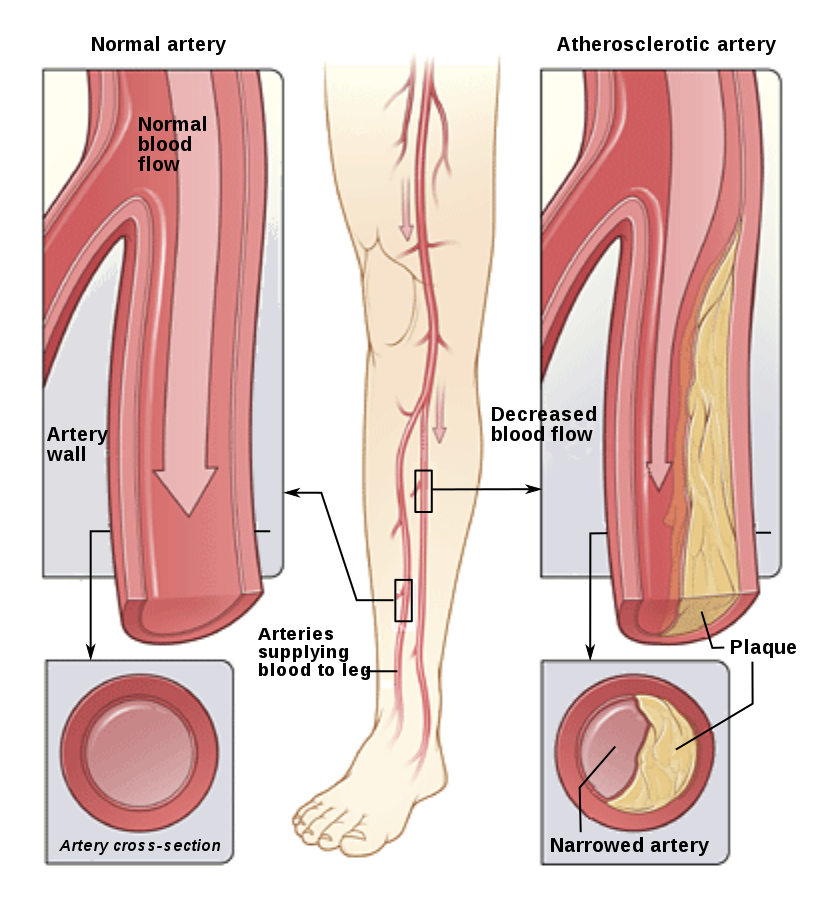
The illustration shows how P.A.D. can affect arteries in the legs. Left figure shows a normal artery with normal blood flow. The inset image shows a cross-section of the normal artery. Right figure shows an artery with plaque buildup that’s partially blocking blood flow. The inset image shows a cross-section of the narrowed artery.
-
- Left-sided Congestive Heart Failure, associated with hypertension and LV MI
-
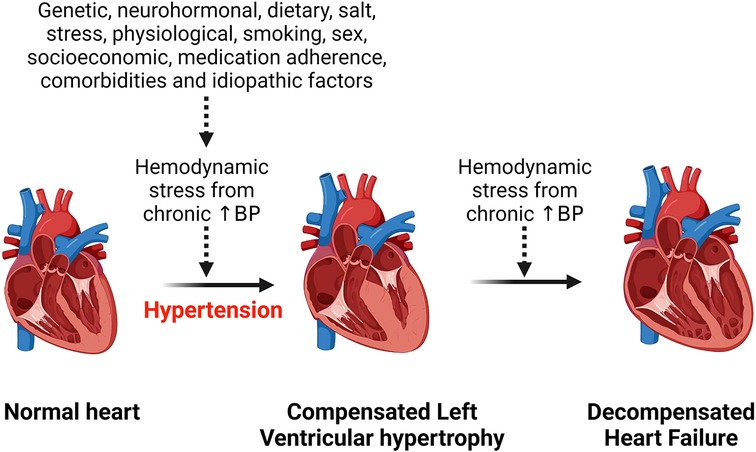
Hypertensioncauses left-sided CHF: Effect of chronic hemodynamic stress on the heart. Chronic hypertension resulting from various stimuli leads to left ventricular hypertrophy as a compensation for the hemodynamic stress and metabolic demand on the heart. However, heart failure results when the heart can no longer withstand the persistent hemodynamic stress. BP, blood pressure. -
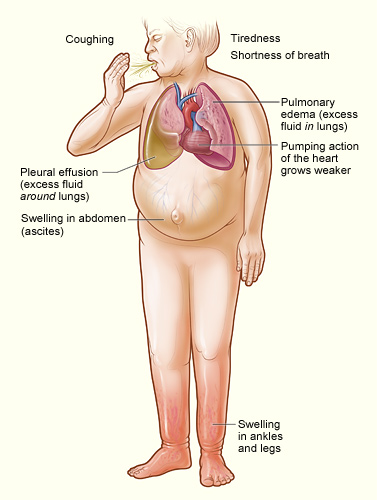
The major signs and symptoms of heart failure.
-
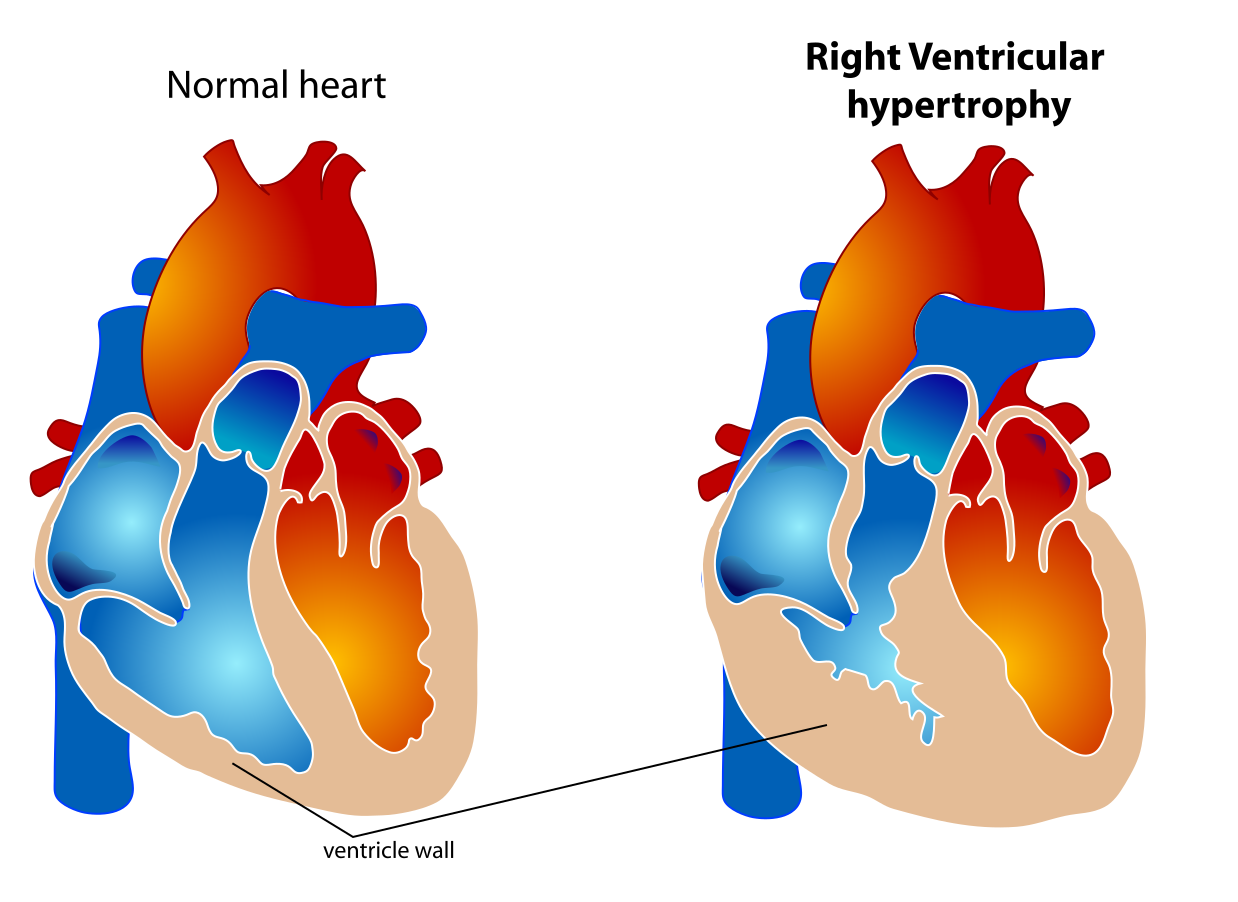
- Right-sided Congestive Heart Failure, associated with cor pulmonale (emphysema, cystic fibrosis, chronic bronchitis) or RV MI
- `
- `
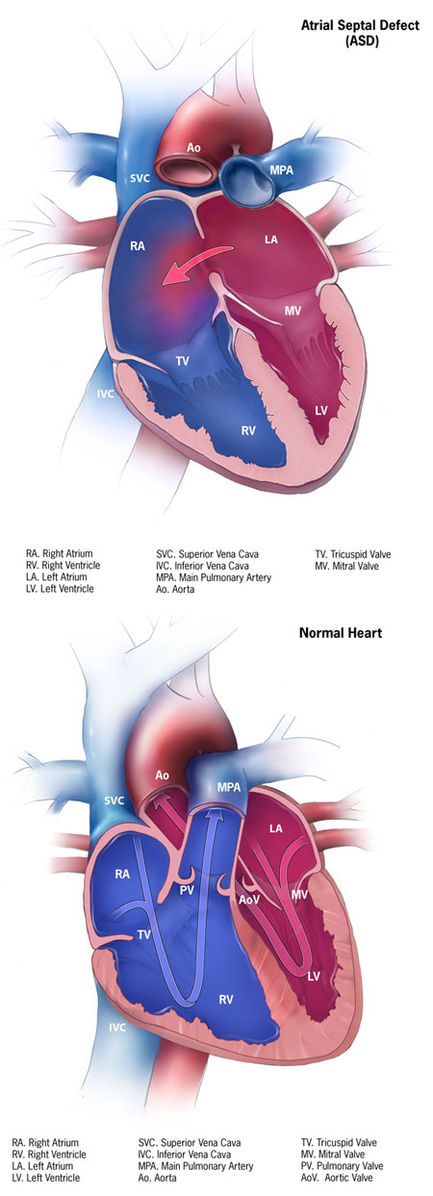
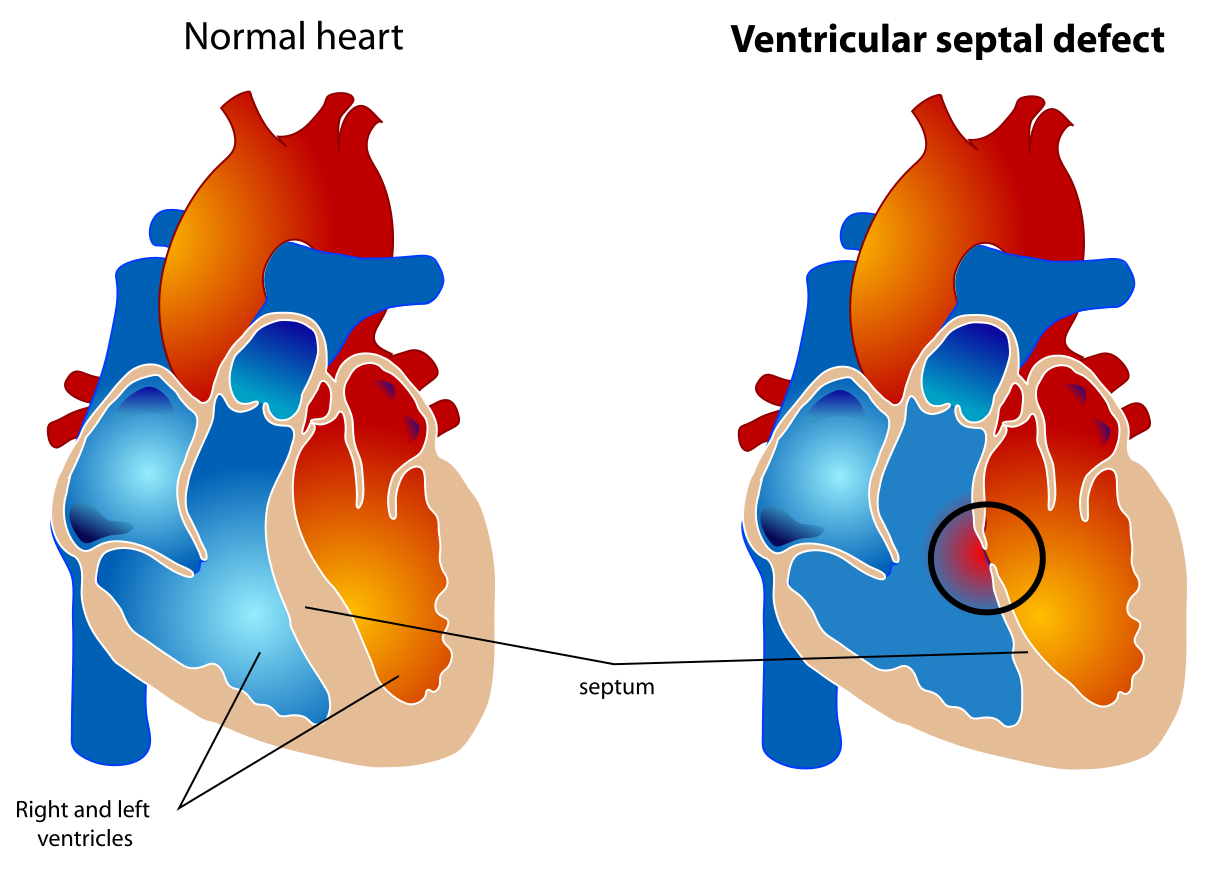
- Congenital Heart Defects – Atrial Septal, Ventricular Septal, Valvular Defects, Tetralogy of Fallot
-
This diagram shows the valves of the heart. The aortic and mitral valves are shown in the left heart, and the tricuspid and pulmonic valves are shown in the right heart. 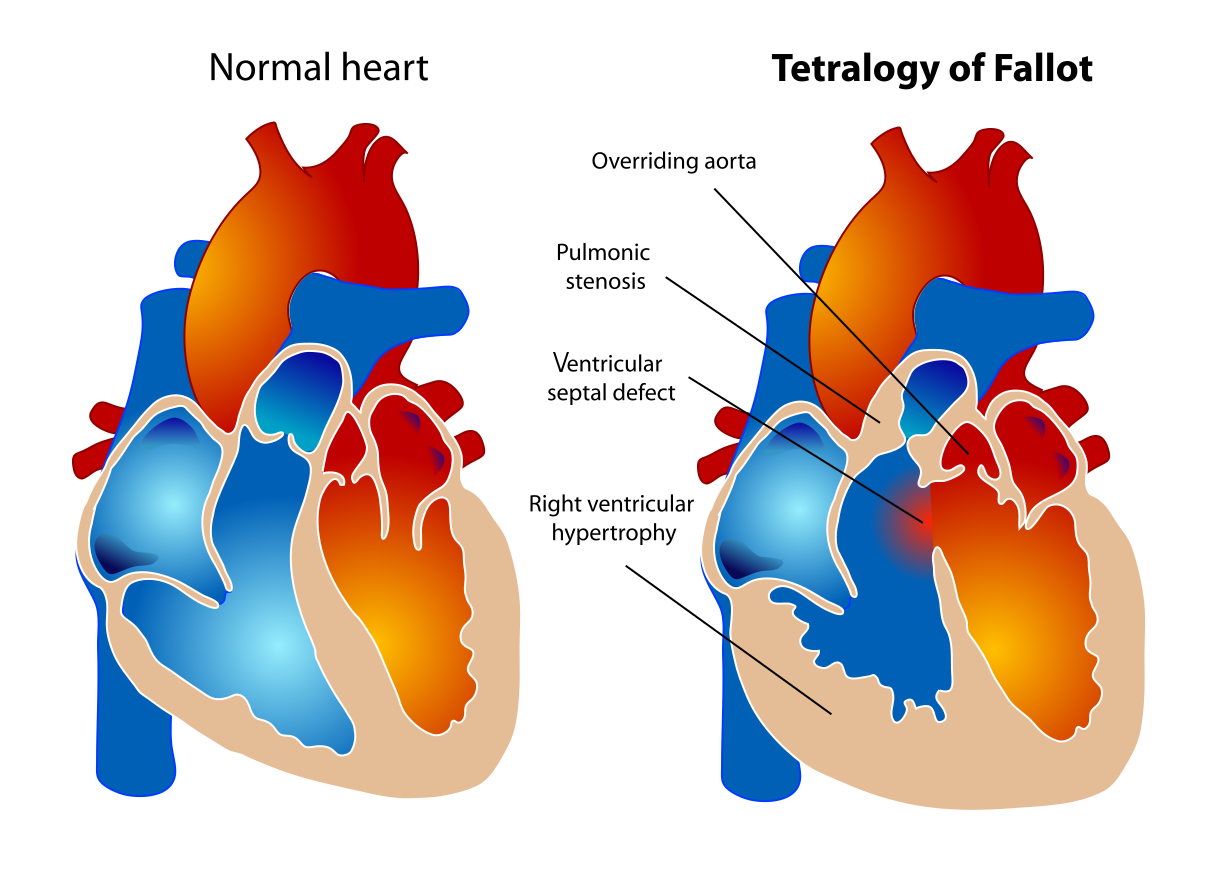
-
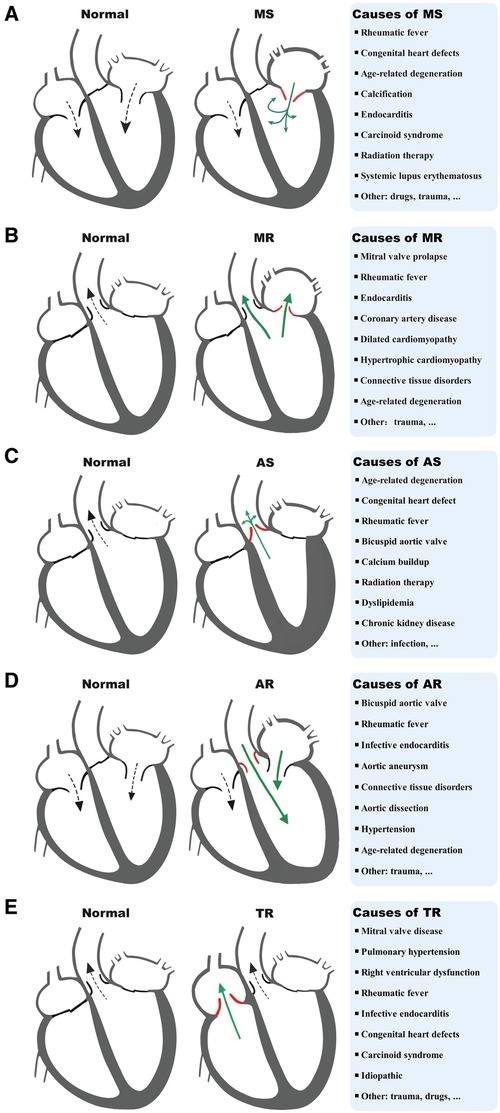
Diagram of a typical blood flow and causes of MS (A), MR (B), AS (C), AR (D), and TR (E). MS, mitral stenosis; MR, mitral regurgitation; AS, aortic stenosis; AR, aortic regurgitation; TR, tricuspid regurgitation.
- Infective Endocarditis
- Infective endocarditis (IE) is divided into acute and subacute forms, depending on the virulence of the causal pathogen.
- Acute IE is rapid in onset and involves highly destructive pathogens that cause necrosis and significant lesions that can lead to death in a matter of days.
- Streptococcus viridans (FYI)
- Subacute IE, alternatively, can deform the valves over weeks to months and generally involves a much less destructive pathogen
- Staphylococcus aureus(more virulent)
- Acute IE is rapid in onset and involves highly destructive pathogens that cause necrosis and significant lesions that can lead to death in a matter of days.
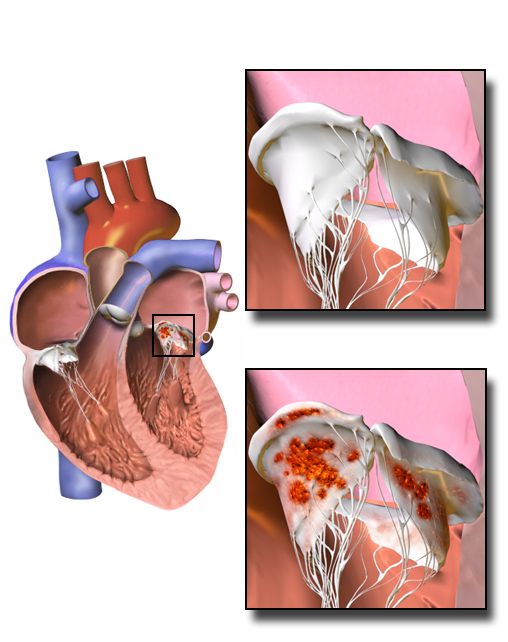
- Basic effects:
- Same regardless of organism
- Microorganisms invade endocardium & valves causing inflammation& formation of vegetation on cusps -can be seen with transesophageal echocardiogram (large, fragile masses of fibrin, platelets, blood cells, & microbes)
- Factors that predispose infection
- Presence of abnormal valves in heart (congenital defects, rheumatic fever, mitral prolapse, artificial/replacement valves)
- Bacteremia–can occur during scaling of teeth & facial piercings
- Reduced host defenses
- Intravenous drug users (dirty needles)
-
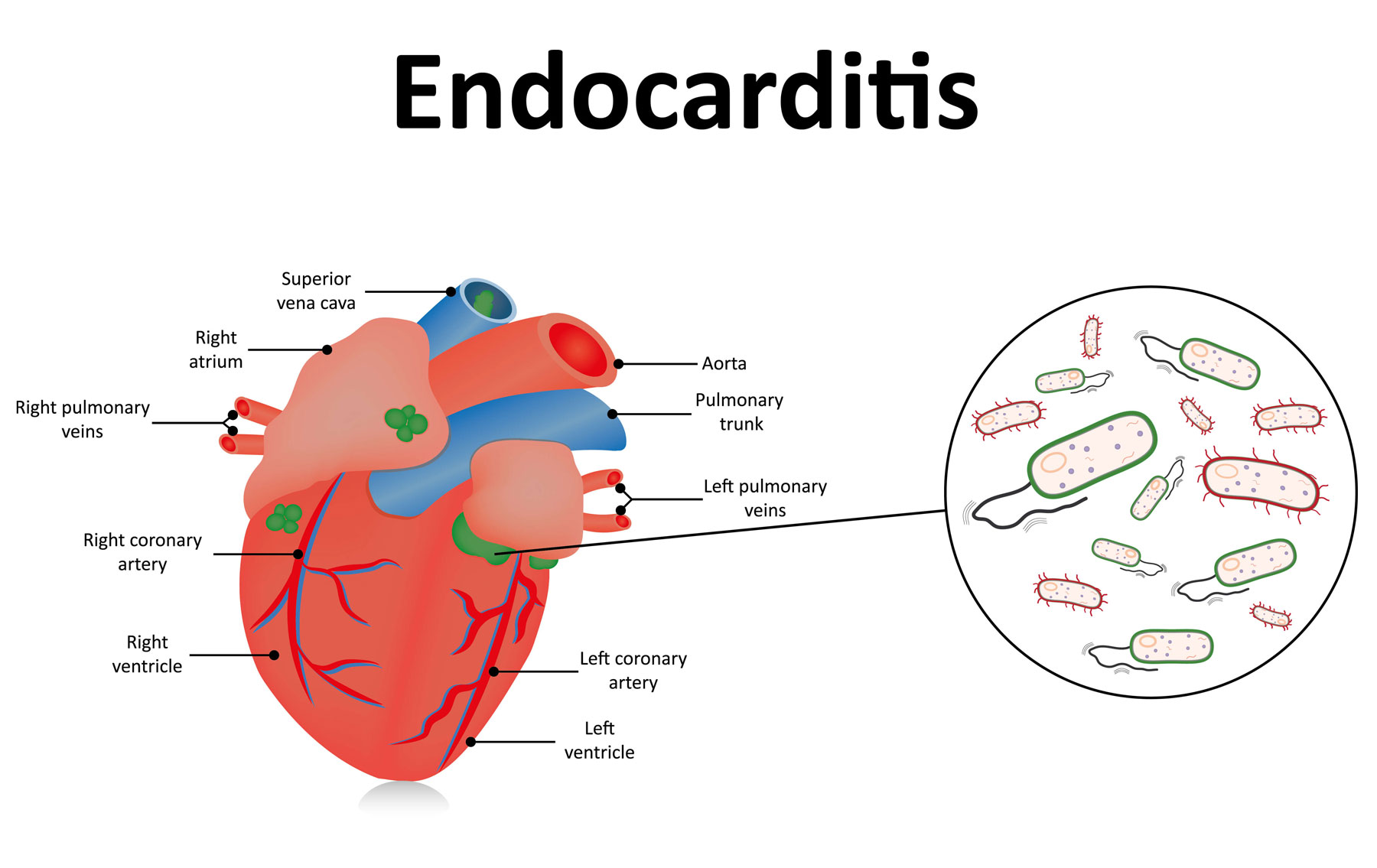
The endocardium is the inner lining of the heart muscle and covering of the heart valves. If the endocardium is damaged, such as from mitral regurgitation, bacteria or other germs can infect the damaged area. As the microorganisms multiply, they cause more damage to the endocardium and may travel through the bloodstream to other parts of the body. The microorganisms can form infected blood clots that can lodge in small arteries and block blood flow. Gradually, the multiplying microorganisms cause severe damage to the heart valves, resulting in heart failure. -
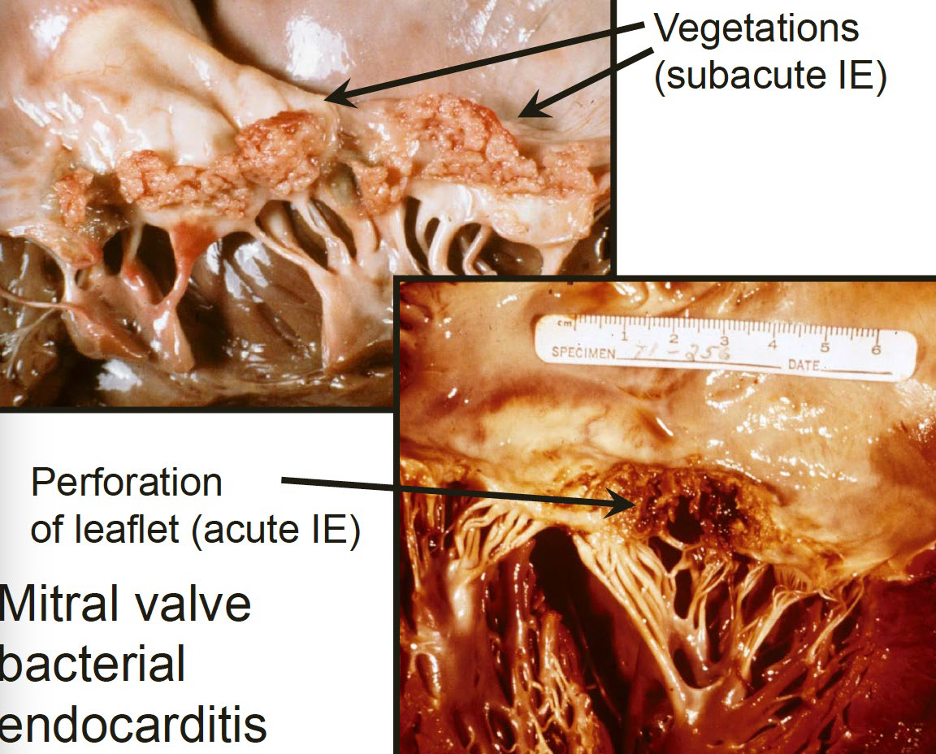
Endocarditis - Most incidence of IE start with fever, but it can also manifest as nonspecific fatigue, weight loss, or flu-like symptoms in older adults. The infection leads to vegetations on the valve that are the hallmark of IE (figure belows). These lesions contain fibrin, inflammatory cells, and bacteria.
-
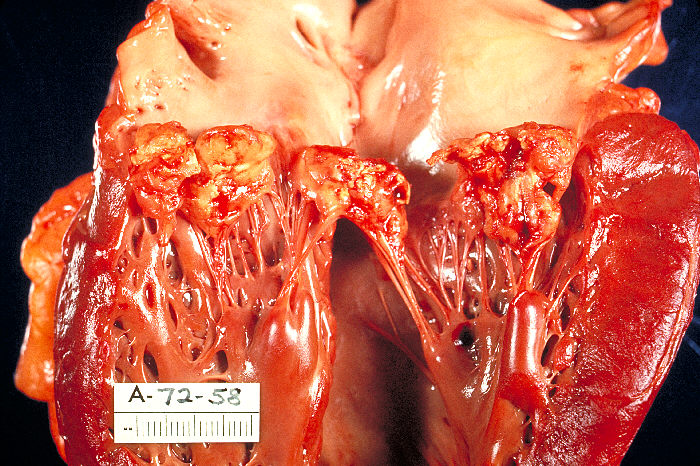
Vegetative lesions (in white box) associated with Infective endocarditis: Gross pathology of subacute bacterial endocarditis involving mitral valve. - The risk is twofold as the vegetations can:
- Disrupt valve function and form abscesses into the underlying myocardium, and
- Embolize and carry the pathogens to a new septic infarcts or obstruct vasculature.
-
- Signs & Symptoms:
- New heart murmurs
- Low-grade fever or fatigue
- Anorexia, splenomegaly, tender Osler’s nodes, CHF in severe cases
-
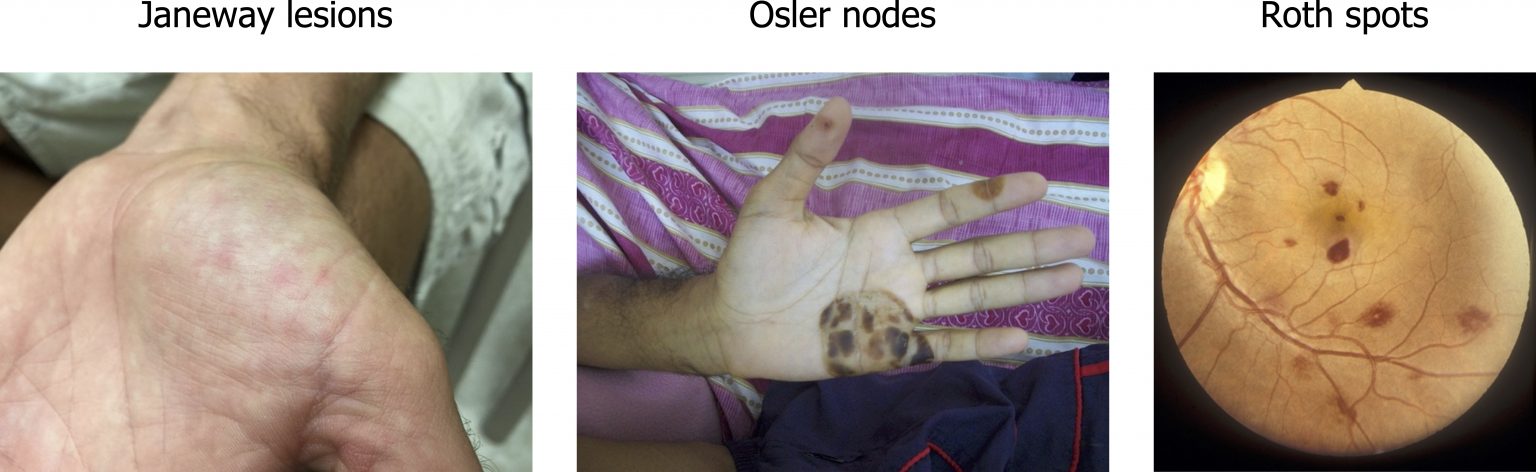
Signs of IE include Janeway lesions (left), Osler nodes (middle), and Roth spots (right).
-
- Septic emboli from vegetation can cause:
- vascular occlusion or infection in other areas of the body (e.g. toes & fingers dermis & disappear in hrsto days) –biopsy to rule out other causes (e.g. DIC, insect bites) & identify bacteria.
- Acute endocarditis
- Sudden, marked onset –spiking fever, chills, drowsiness
- Subacute endocarditis
- Insidious onset –increasing fatigue, anorexia, cough, and dyspnea
- Treatment
- Blood culture to identify causative agent
- Administration of antimicrobial drugs for several weeks
- Medications for congestive heart failure (CHF).
- Blood culture to identify causative agent
- Infectious endocarditis is the inflammation of the endocardium, the inner lining of the heart, as well as the valves that separate each of the four chambers within the heart.
-
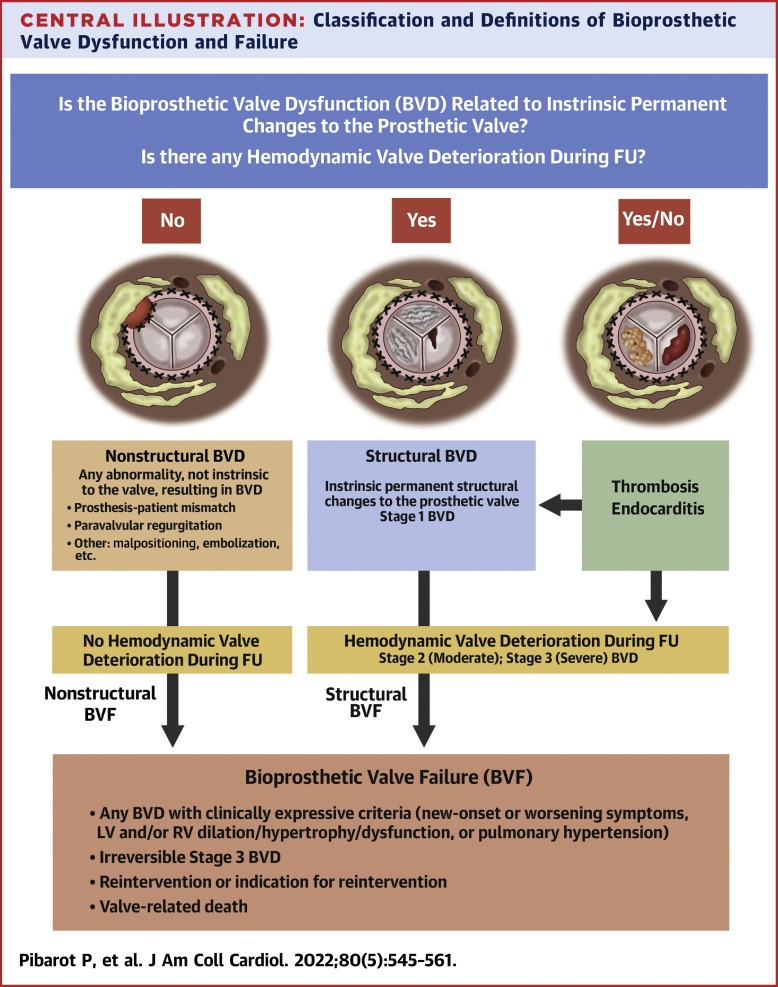
Classification and Definitions of Bioprosthetic Valve Dysfunction and Failure
This figure presents the classification and main criteria for definition of (aortic or mitral) bioprosthetic valve dysfunction and failure. BVD = bioprosthetic valve dysfunction; BVF = bioprosthetic valve failure; FU = follow-up.
-
- Infective endocarditis (IE) is divided into acute and subacute forms, depending on the virulence of the causal pathogen.
- Rheumatic Heart Failure
- Rheumatic heart disease (RHD) is virtually the only cause of mitral valve stenosis. It arises after a group A streptococcal infection that often originates in the upper airway and leads to rheumatic fever (a multisystem, immune-mediated disease).
- Acute stage –inflammation of the heart may involve
- Pericarditis – inflammation of pericardium puts pressure on heart and impairs filling
- Myocarditis – localized lesions called Aschoffbodies, may interfere with conduction
-
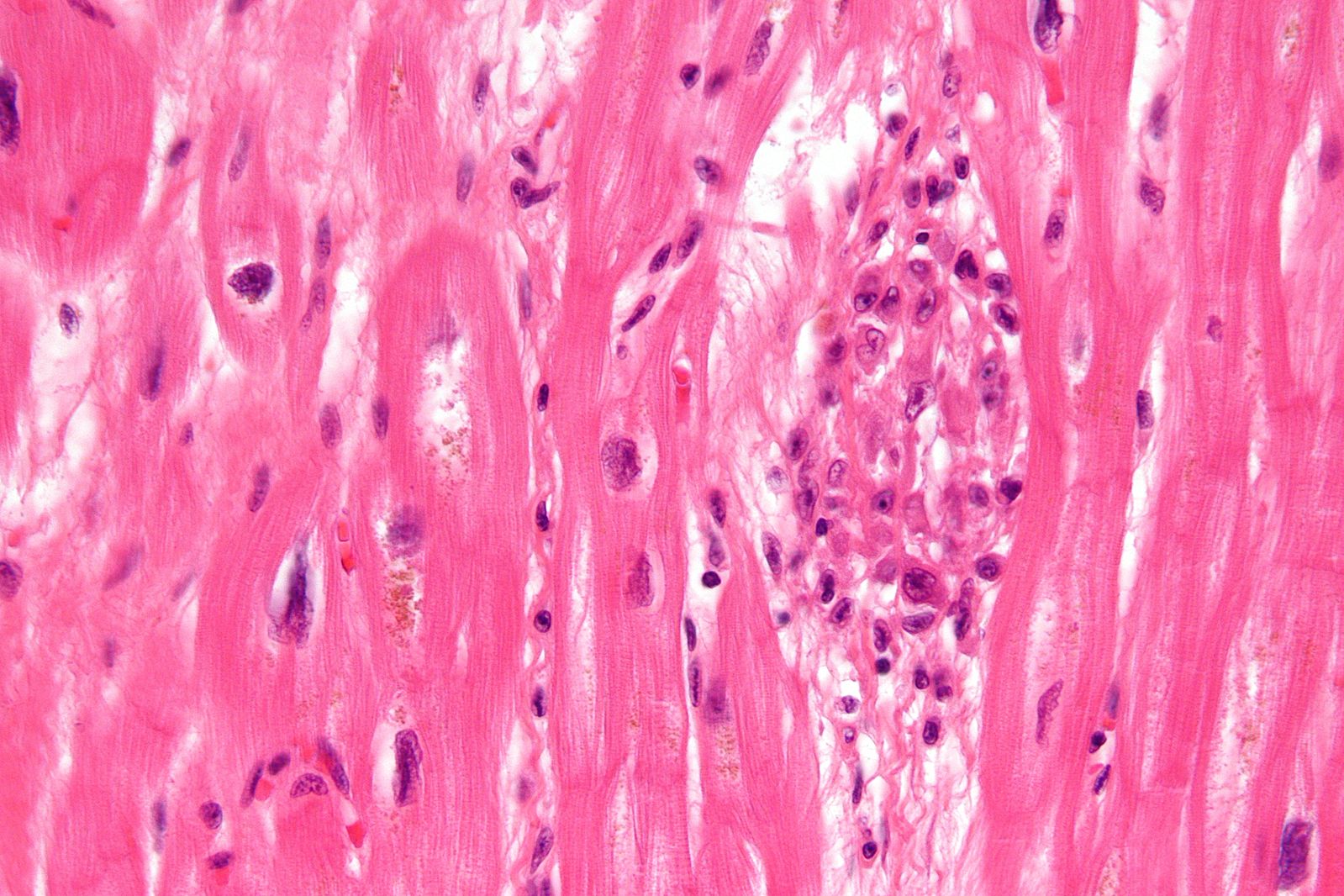
Micrograph of rheumatic heart disease.
-
- Endocarditis and incompetent heart valves – most common problem (mitral valve verrucae =“warts”)
- Leads to stenosis or valvular incompetence
- Other sites of inflammation
- Large joints – synovitis
- Erythema marginatum, non-pruritic skin rash (<5% patients)
-

Erythema marginatum
-
- Non-tender subcutaneous nodules – wrists, elbows, knees, ankles
- Involuntary jerky movement of the face, arms, legs involving basal nuclei; “Sydenham’s chorea” -more common in girls
- Signs and symptoms
- Low-grade fever, leukocytosis, malaise, anemia, anorexia, fatigue, tachycardia
-
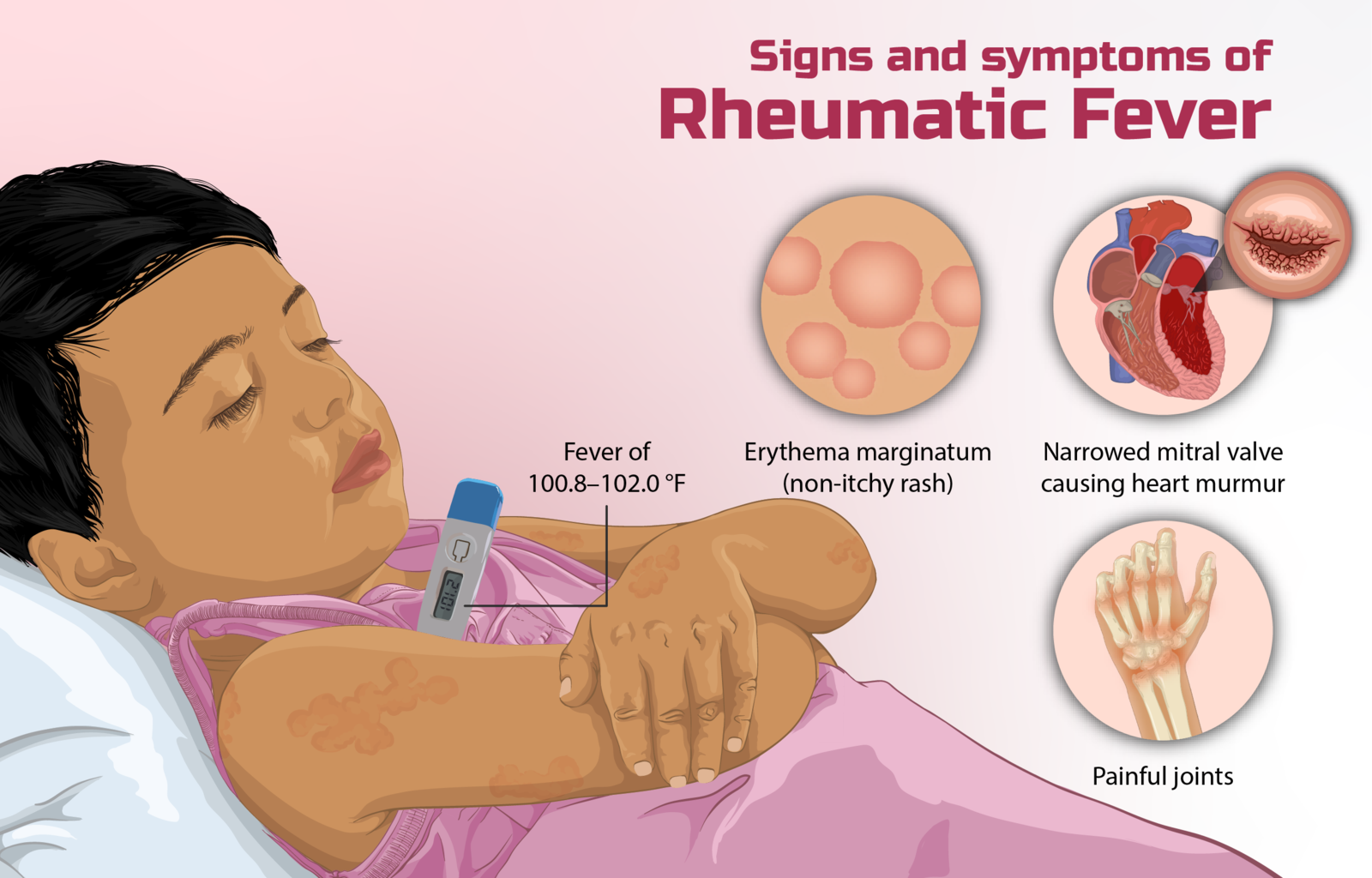
The typical symptoms of Rheumatic Fever.
- Diagnostic tests
- Heart function test (& heart murmur)
- ECG (dysrhythmias)
- ASO (anti-streptolysin O)antibody titer
- Treatment
- Prophylactic antibacterial agents
- Anti-inflammatory agents
- `
- Pericarditis
- Pericarditis: inflammation of pericardium puts pressure on heart and impairs filling
- Acute pericarditis
- Usually secondary to another condition
-
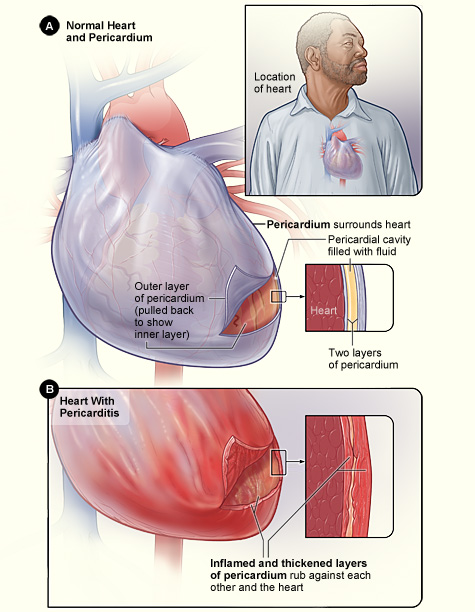
An enlarged cross-section that shows the inflamed and thickened layers of the pericardium.
-
- Classified by cause or type of exudate
- May involve simple inflammation of the pericardium
- Rough, swollen surfaces cause chest pain & friction rub (hear grating sound-stethoscope)
- May be secondary to
- Open heart surgery, myocardial infarction, rheumatic fever, systemic lupus erythematosus, cancer, renal failure, trauma, viral infection
- May involve simple inflammation of the pericardium
- Effusion may develop -fluid accumulating in pericardial sac & fluid may be:
- Serous
- Fibrinous& purulent with infection
- Blood (hemopericardium) with trauma or cancer
- Effects of Pericardial Effusion
- Fluid around heart compresses heart wall
- Heart cannot expand to fill
- Superior vena cava: backup into the systemic circulation
- Aorta: decreased output to body
- Pulmonary artery: decreased blood flow to lungs
- Usually secondary to another condition
- Chronic pericarditis
-
- Results in formation of adhesions between the pericardial membranes
- Fibrous tissue often results from TB or radiation of mediastinum
- Limiting movement of the heart during diastole and systole →↓CO
- Inflammation or infection may develop from adjacent structures
- Signs & symptoms
- Chest pain, friction rub, dyspnea, tachycardia, fatigue, weakness, abdominal discomfort
- Due to systemic venous congestion
- Chest pain, friction rub, dyspnea, tachycardia, fatigue, weakness, abdominal discomfort
- Treatment:
- Treat primary problem
- Aspirate fluid = paracentesis–analyze
- `
- Results in formation of adhesions between the pericardial membranes
-
- Pericarditis: inflammation of pericardium puts pressure on heart and impairs filling
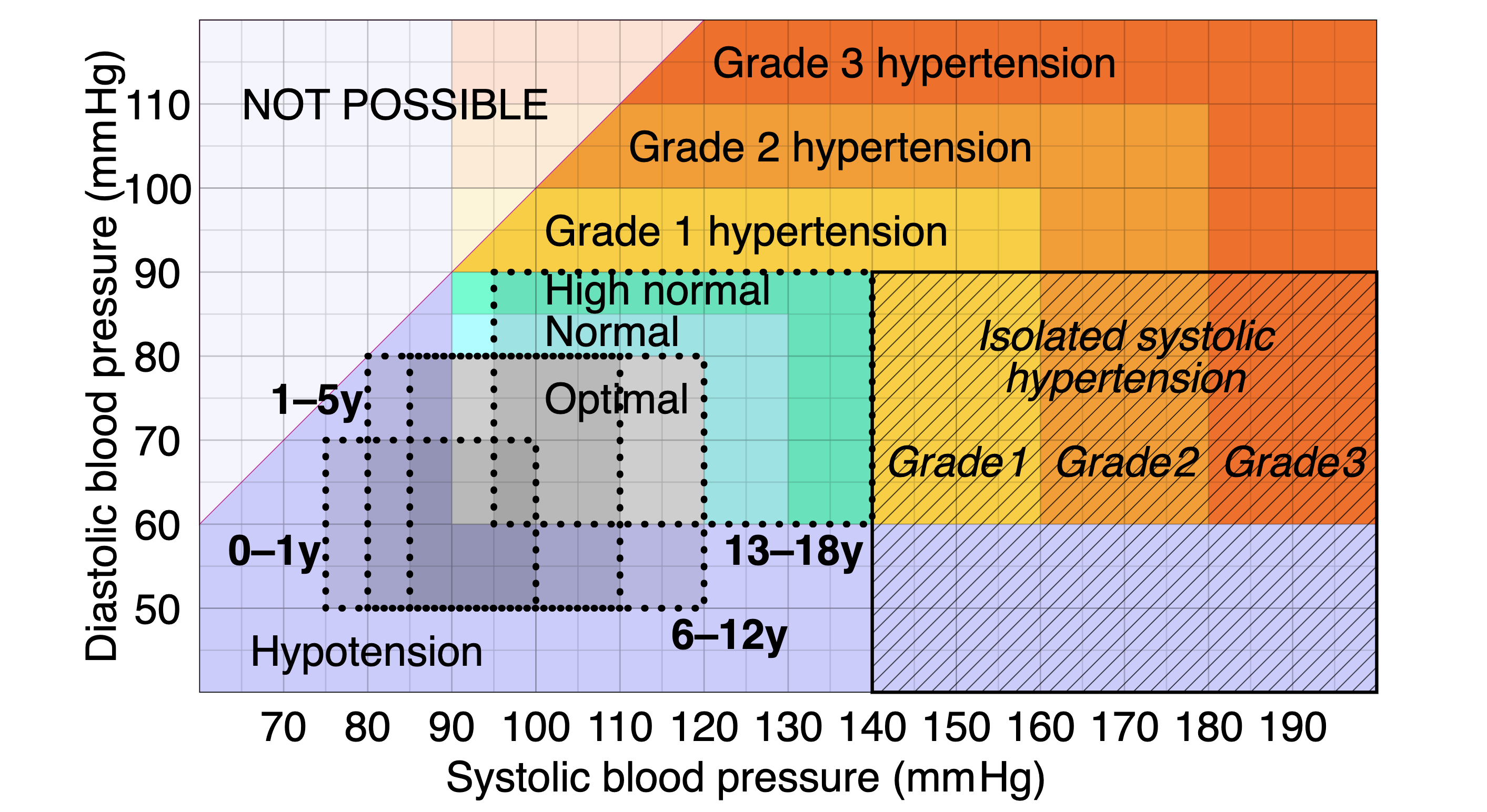
- Hypertension
- Hypertension: high blood pressure
- Sometimes classified as systolic (>140) or diastolic (>90)
-
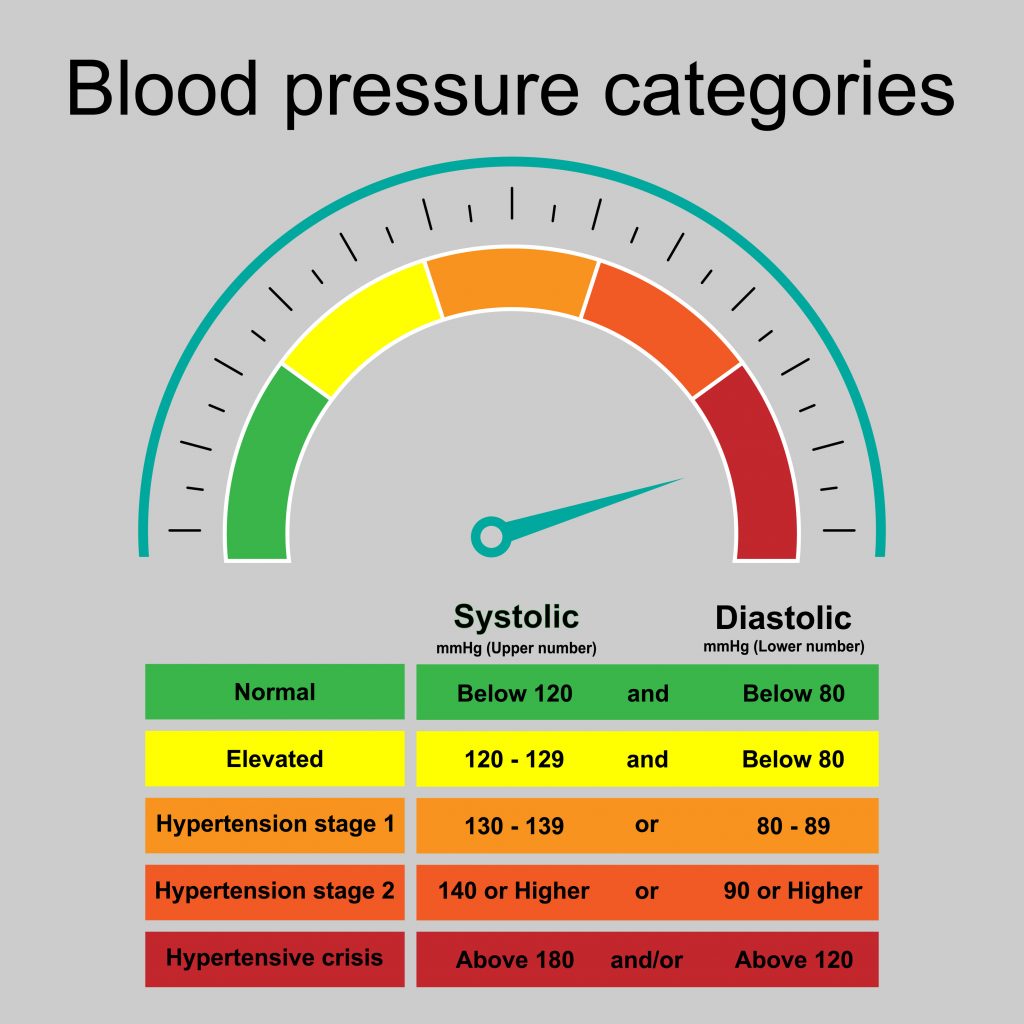
Blood Pressure Ranges
-
- Pre-hypertensive: 120-139 (systolic) or 80-89 (diastolic)
-
Hypertension chart
- Sometimes classified as systolic (>140) or diastolic (>90)
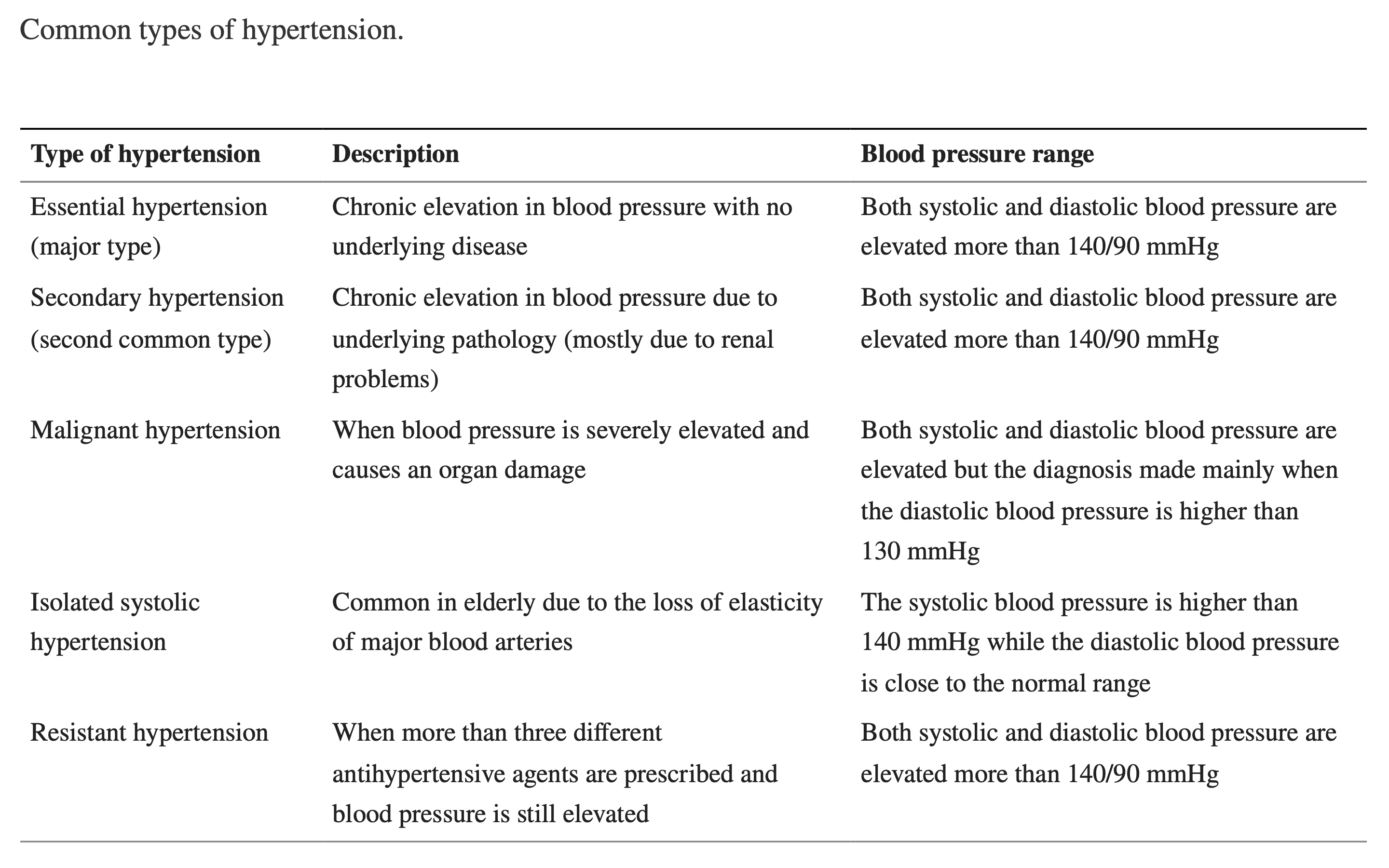
- Three types of hypertension: primary/essential, secondary, malignant/resistant
- Hypertension: high blood pressure
- Essential Hypertension
- Essential hypertension, also called primary hypertension, accounts for 90-95% of all cases and is idiopathic in nature. It is defined by consistently elevated blood pressure readings above 140/90, with adjustments sometimes made for age-related arteriosclerosis.
- This condition is characterized by increased arteriolar vasoconstriction, leading to reduced blood flow to the kidneys and triggering the renin-angiotensin-aldosterone response. Consequently, there is heightened vasoconstriction and blood volume, resulting in elevated blood pressure levels.
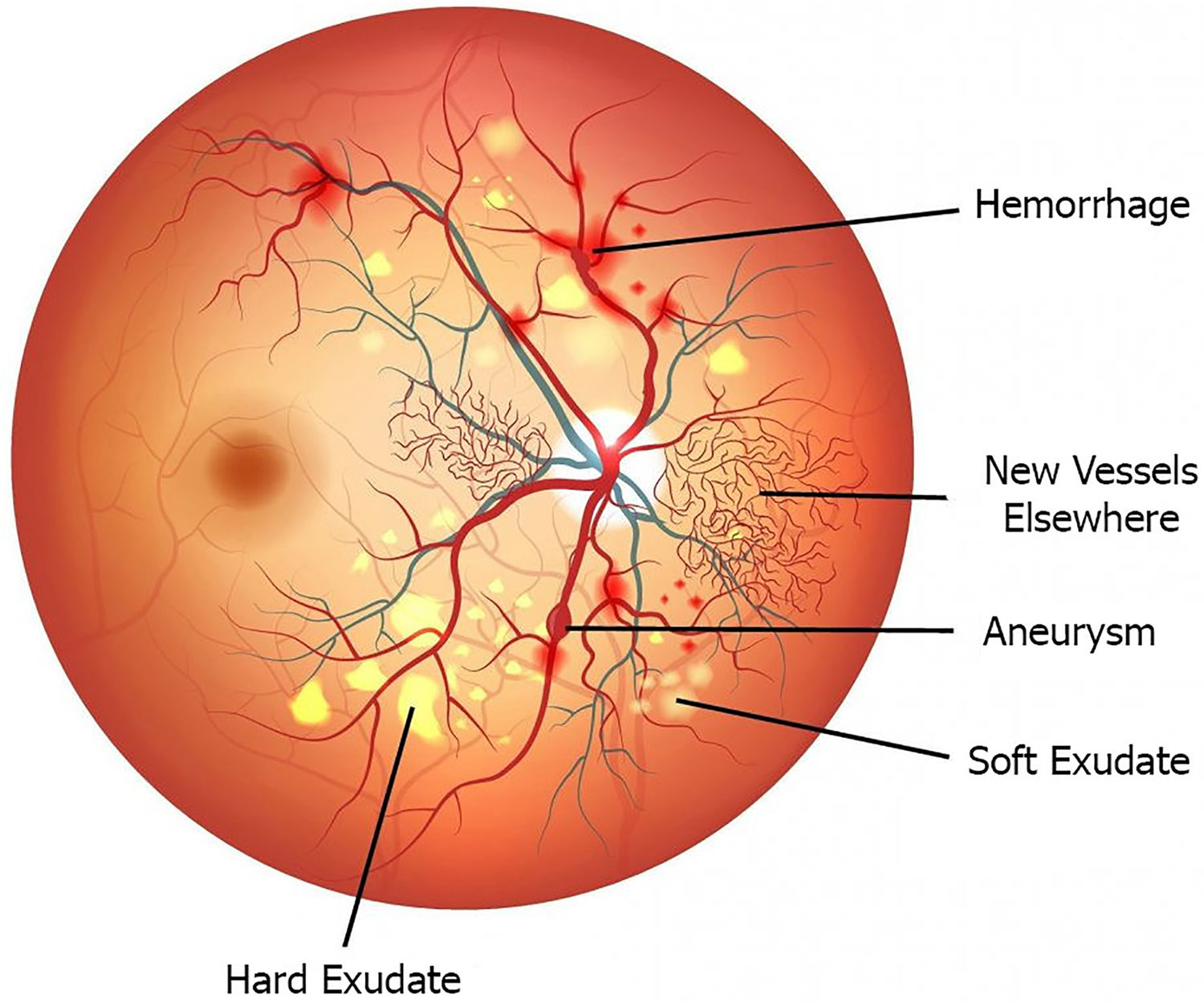
- Prolonged hypertension can lead to arterial wall damage and the formation of atheromas, causing arterial walls to harden and become sclerotic. This can lead to wall tearing or the development of aneurysms. Retinal examination can detect these changes, which can contribute to left-sided congestive heart failure. Additionally, reduced blood supply to vital organs such as the brain, kidneys, and retina can lead to ischemia and tissue necrosis, ultimately resulting in loss of function.
-
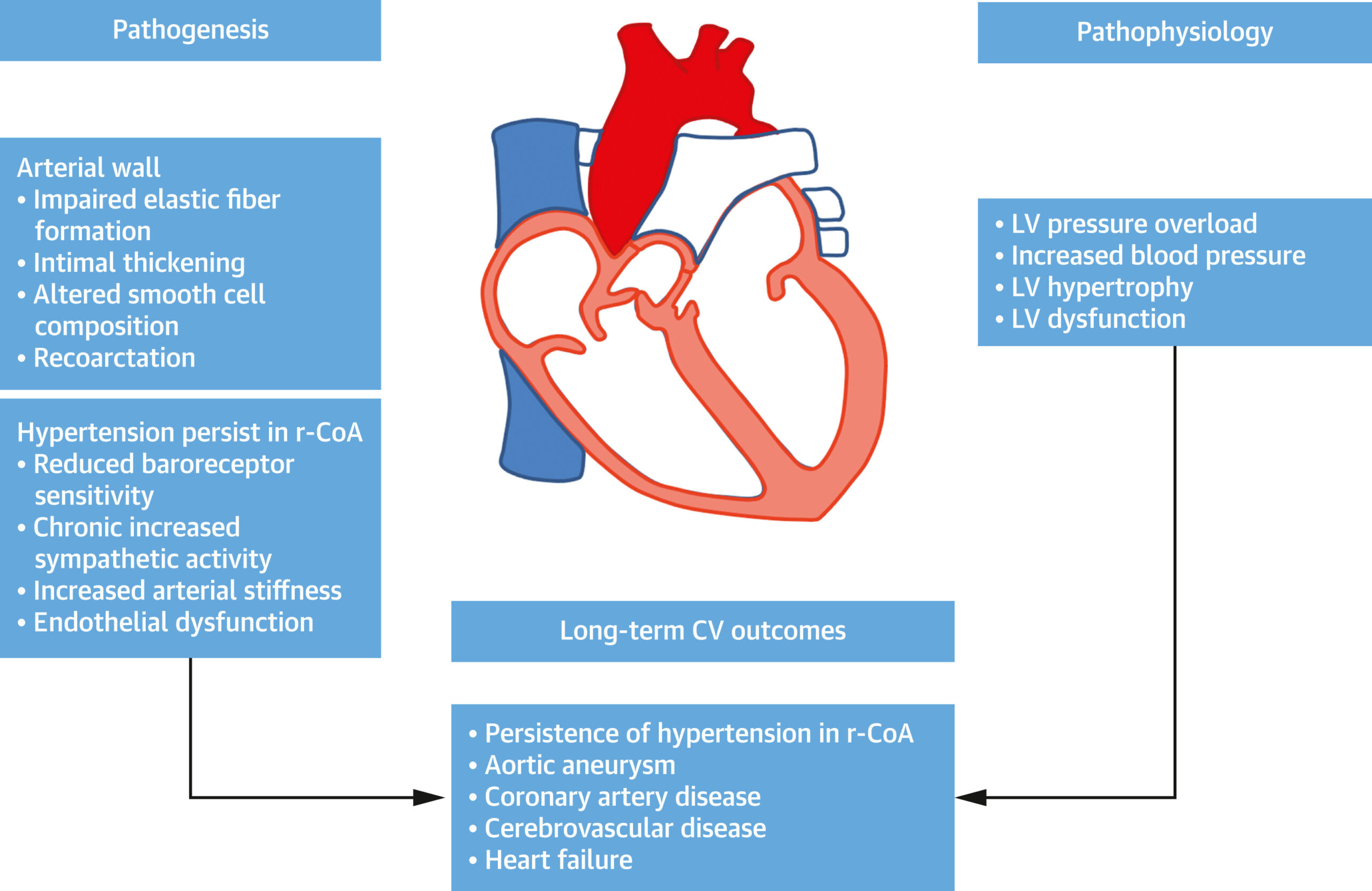
Impact of the Coarctation of Aorta on the CV System: Long-term left ventricular (LV) pressure overload and remodeling as a consequence of persistent or de novo diagnosed hypertension as well as restenosis of aortic isthmus are common in adult patients with repaired coarctation of the aorta (r-CoA) and account for the increased cardiovascular (CV) morbidity and mortality. The cardiac long-term complications of the coarctation of aorta include concentric cardiac remodeling and hypertrophy, diastolic dysfunction, left atrial dilation, and—in more advanced stages—systolic LV dysfunction.
- Secondary Hypertension – due to Renal Disease, or Endocrine Dysfunction, Drugs, Alcohol
-
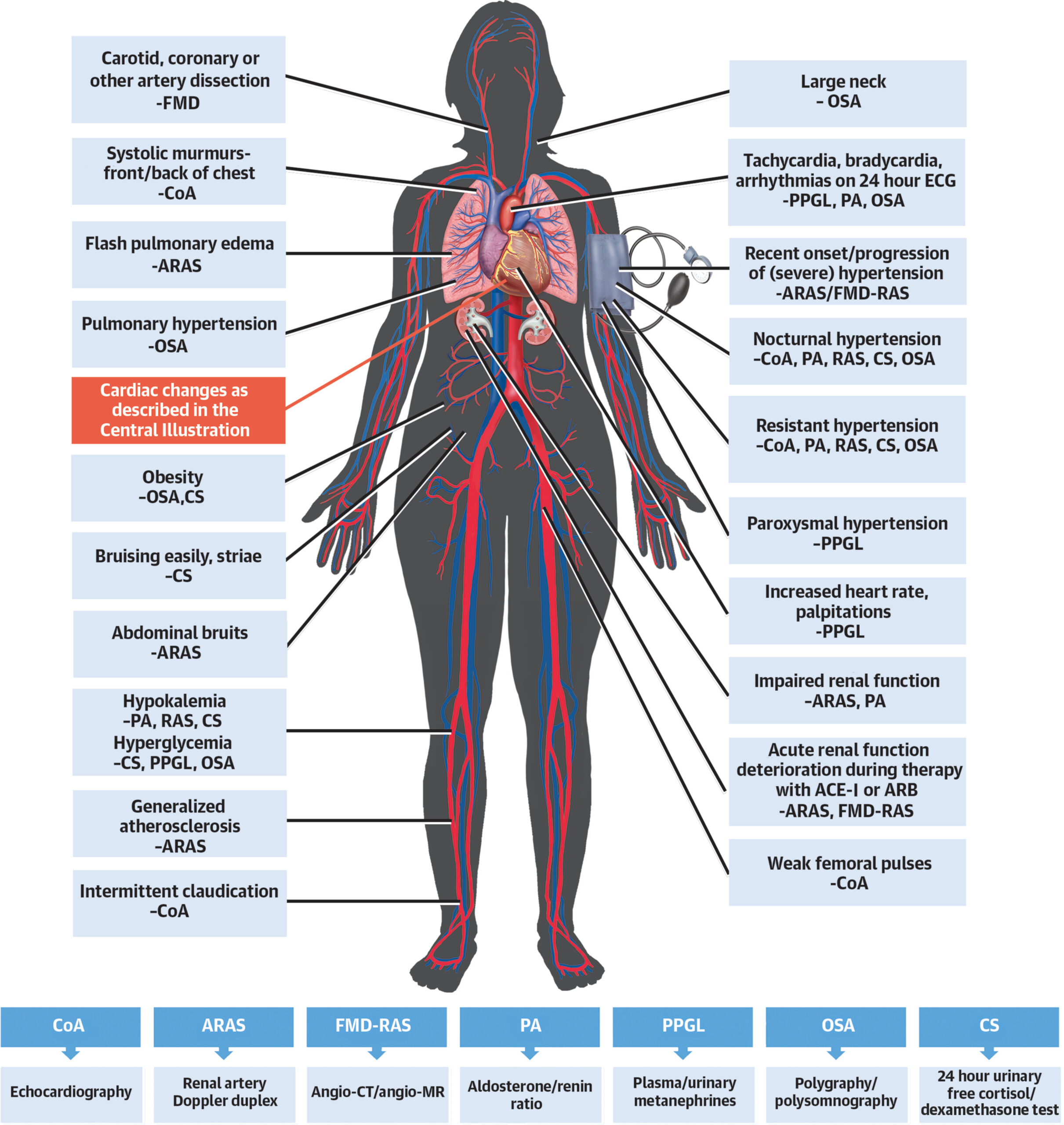
Signs, Symptoms, and Screening of Secondary Hypertension: Screening of secondary forms of hypertension in patients at risk or with specific biochemical/clinical phenotypes of these conditions. Although in some cases the symptoms of secondary forms of hypertension may be mild, the coincidence of cardiac changes (Central Illustration) with the symptoms shown in the figure should make discerning clinicians suspect secondary forms of hypertension. ACE-I = angiotensin-converting enzyme inhibitor; AF = atrial fibrillation; ARB = angiotensin receptor blocker; ARAS = atherosclerotic renal artery stenosis; CAD = coronary artery disease; CoA = coarctation of the aorta; CMR = cardiac magnetic resonance; CS = Cushing syndrome; ECG = electrocardiography; FMD = fibromuscular dysplasia; OSA = obstructive sleep apnea; PA = primary aldosteronism; PPGL = pheochromocytoma/paraganglioma; RAS = renal artery stenosis. - Areas most frequently damaged by hypertension: kidneys, heart, brain, retina.
-

Secondary damage induced by hypertension.
-
-
- Malignant or resistant hypertension
- Develops in 1% of people with essential hypertension
- Emergencies! Uncontrollable, severe, and rapidly progressive form with many complications (damaging organs); idiopathic; other causes include drug or alcohol overdose/withdrawal
- Diastolic pressure is extremely high.
- Retinopathy with papilledema, headache, and encephalopathy can occur due to hypoperfusion causing cerebral edema, angina, MI, CHF, and pulmonary edema.
- Aortic Aneurysms
- An aortic aneurysm is a localized dilation and weakening of the arterial wall, often found in the abdominal or thoracic aorta. It typically develops due to a defect in the medial layer associated with turbulent blood flow.
-
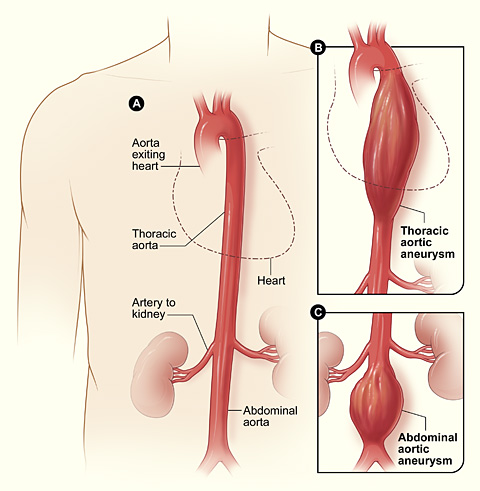
Common location: abdominal or thoracic aorta -
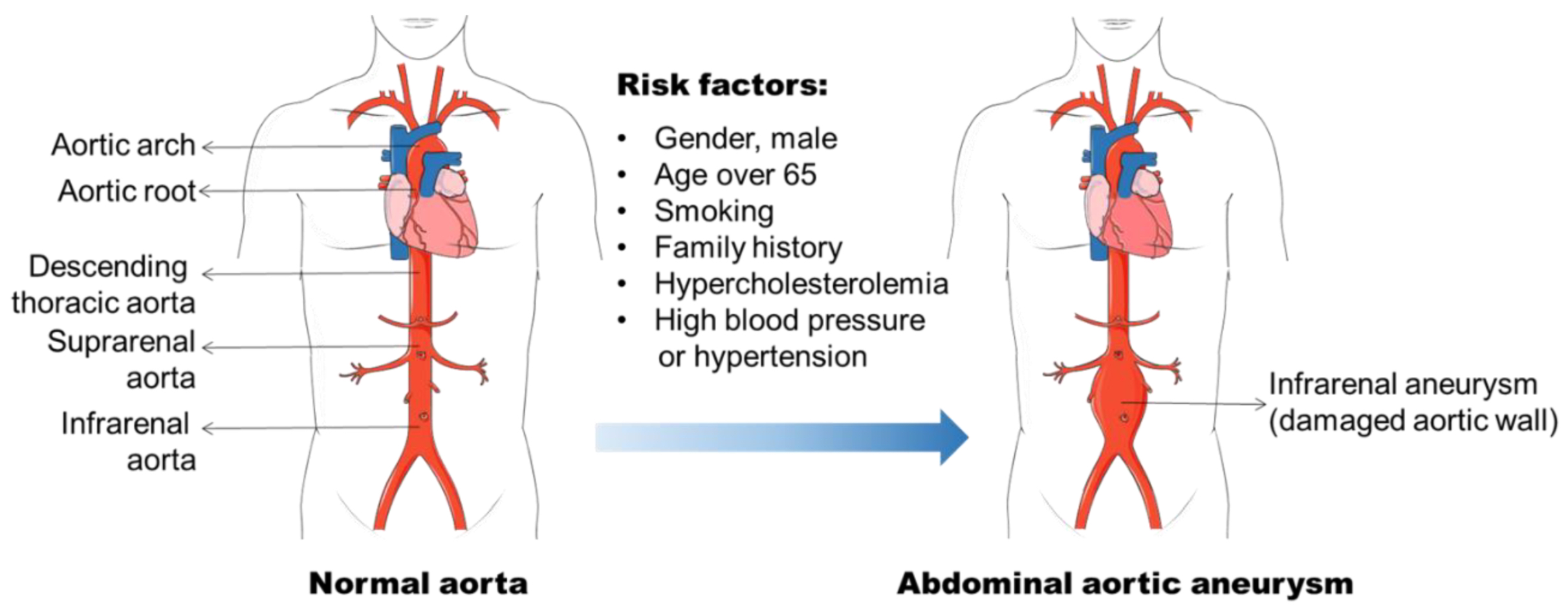
Abdominal aortic aneurysm formation and its risk factors. -
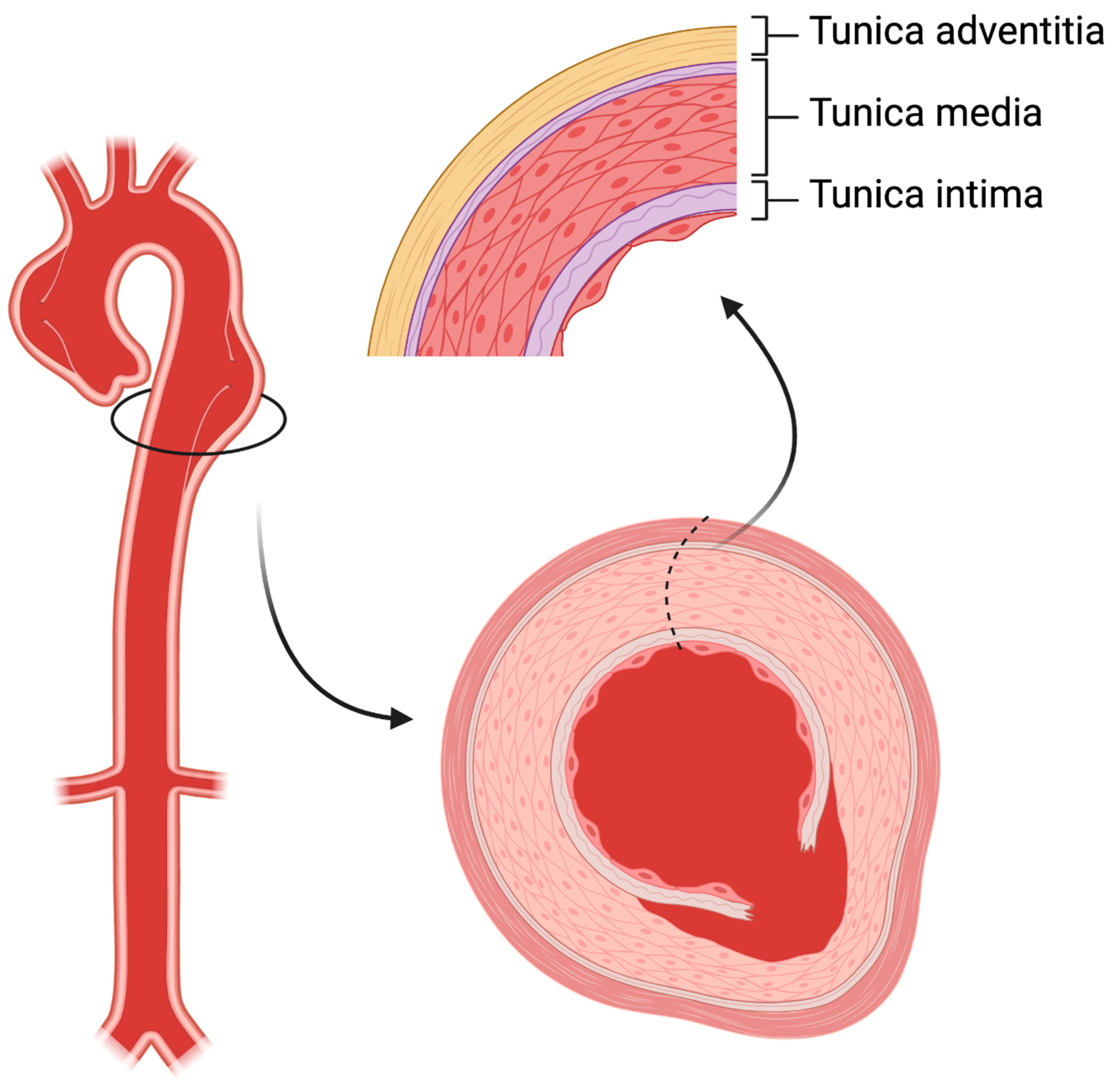
The structure of aortic wall.
-
- Aortic Aneurysm causes include atherosclerosis, trauma, infections like syphilis, and congenital defects. Symptoms may include the presence of a bruit upon auscultation, feeling a pulse upon palpating the abdomen, dysphagia if there’s pressure on the esophagus, and occasionally chest or back pain. Aneurysms are often asymptomatic until they grow large or rupture, which can lead to severe hemorrhage, shock, loss of pulse, organ dysfunction, and even death.
- Three types of Aortic Aneurysms (classified by shapes)
-

3 Types of Aortic Aneurysms: (A) Saccular: Bulging wall on the side. (B) Fusiform: Circumferential dilation along a section of artery. (Brown: thrombus). (C) Dissecting aneurysms: Develops when there is a tear in the intima of the wall and blood continues to dissect or separate tissues (Pink dashed line: tear in intima; blood flows between layers of wall.
-
- An aortic aneurysm is a localized dilation and weakening of the arterial wall, often found in the abdominal or thoracic aorta. It typically develops due to a defect in the medial layer associated with turbulent blood flow.
- Venous disorders – Varicose Veins
- Introduction
- Irregular, dilated, & tortuous areas of superficial veins in legs
- It has familial tendency
- Development
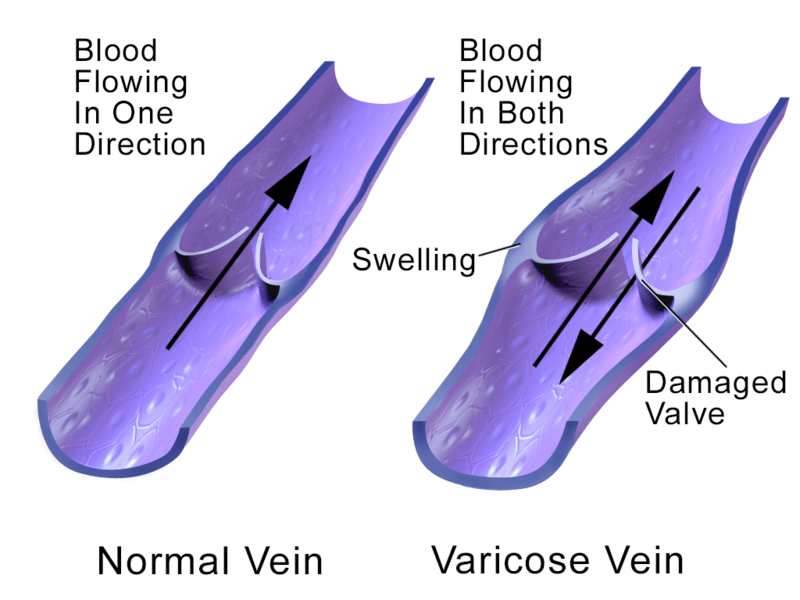
-
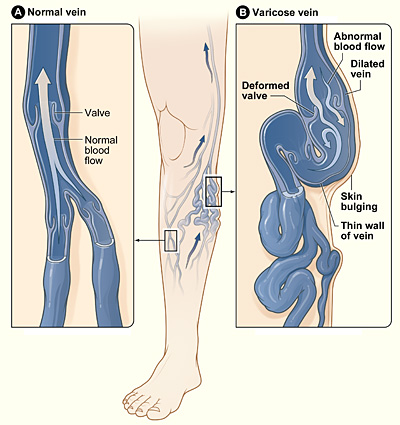
The illustration shows how a varicose vein forms in a leg. Figure A shows a normal vein with a working valve and normal blood flow. Figure B shows a varicose vein with a deformed valve, abnormal blood flow, and thin, stretched walls. The middle image shows where varicose veins might appear in a leg. -
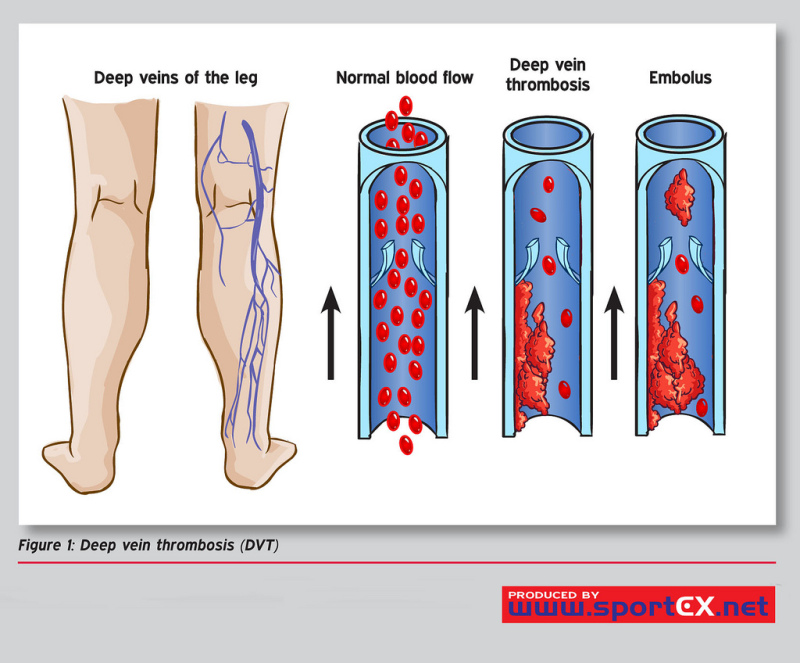
Deep Vein Thrombosis (DVT) - A multi-task convolutional neural network for classification and segmentation of chronic venous disorders
- Risk factors: Increased BMI, parity & weight lifting
- May develop from defect or weakness in vein walls or valves
- Standing for long periods of time, crossing legs, wearing tight clothing, pregnancy
- Appear as irregular, purplish, bulging structures
- Edema in feet
-
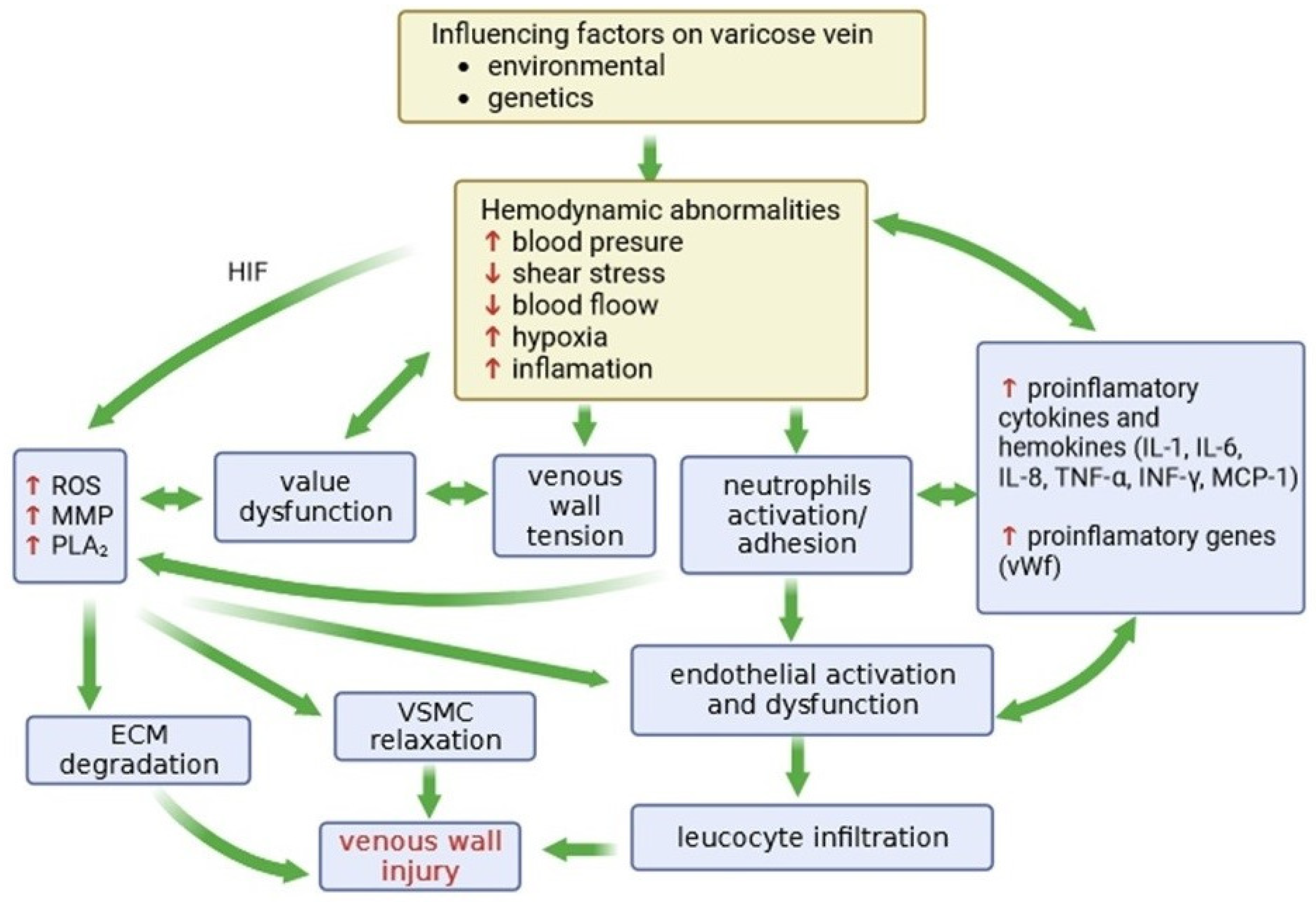
Factors influencing venous wall remodeling.
-
- Treatment
- Keep legs elevated, support stockings
- Restricted clothing and crossing legs should be avoided
- Irregular, dilated, & tortuous areas of superficial veins in legs
- Thrombophlebitis and phlebothrombosis
- Thrombophlebitis: Thrombus development in inflamed vein. e.g., IV site

-

Superficial thrombophlebitis (arrow) at the medial left groin with venous malformation, clearly visible as a newly appeared, bluish swelling that is tender on palpation. -

Classic circumscribed superficial thrombophlebitis just below the lateral malleolus with reddish discoloration and swelling in a patient with venous malformation.
- Phlebothrombosis: Thrombus forms spontaneously without prior inflammation; clot attached loosely
-

Phlebothrombosis of the right leg in a child with venous malformation. The right leg is somewhat swollen (clearly visible at the ankle) and slightly bluish-livid discolored. - `
-
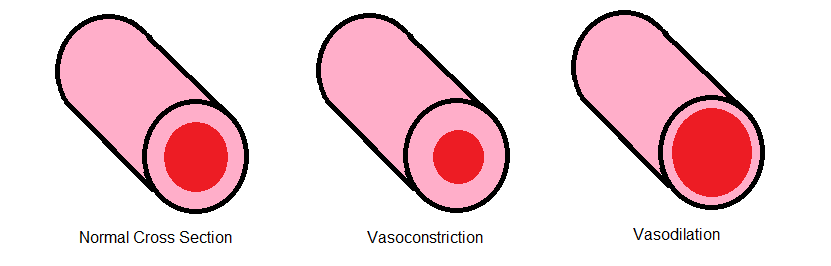
- Factors for thrombus development
- Stasis of blood or sluggish blood flow: due to immobility or restrictive clothing
- Endothelial injury: due to trauma
- Increased blood coagulability: due to dehydration, cancer, pregnancy, increased platelet adhesion
- Signs and symptoms
- Often unnoticed
- Aching, burning, tenderness in affected legs
- Systemic signs: fever, malaise, leukocytosis
- Complications: Pulmonary embolism

-
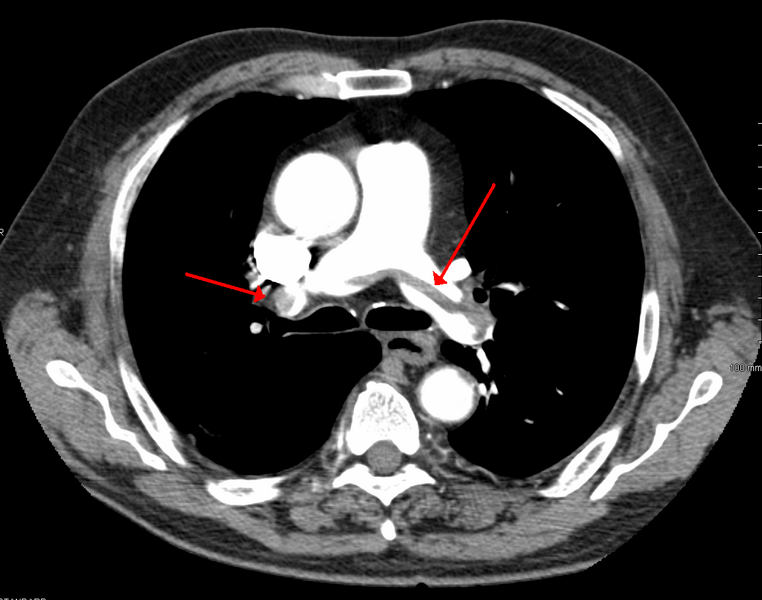
A large pulmonary embolism at the bifurcation of the pulmonary artery (saddle embolism).
- Treatment
- Preventive measures: Exercise, elevating legs, elastic stockings, reduce stress
- Anticoagulant therapy: heparin, fibrinolytic therapy
-

Catalytic effect of heparin on anticoagulant activity of heparin cofactor Ⅱ (HC Ⅱ). -
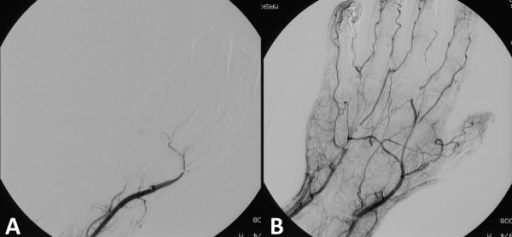
Angiograph before and after thrombolytic therapy in a case of thrombosis on the hand.
-
- Surgical intervention: thrombectomy
-
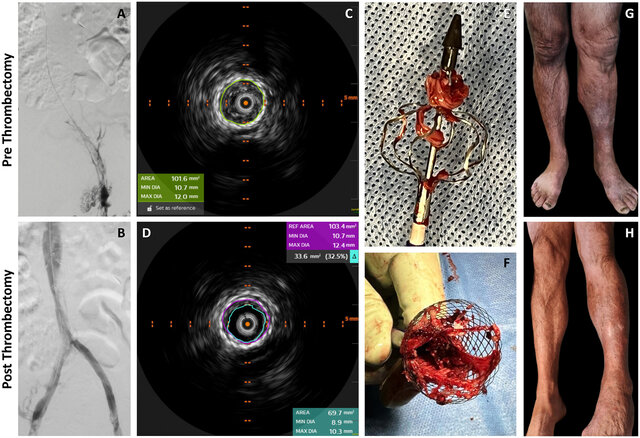
Pre and post-RevCore thrombectomy imaging and removed thrombus. -
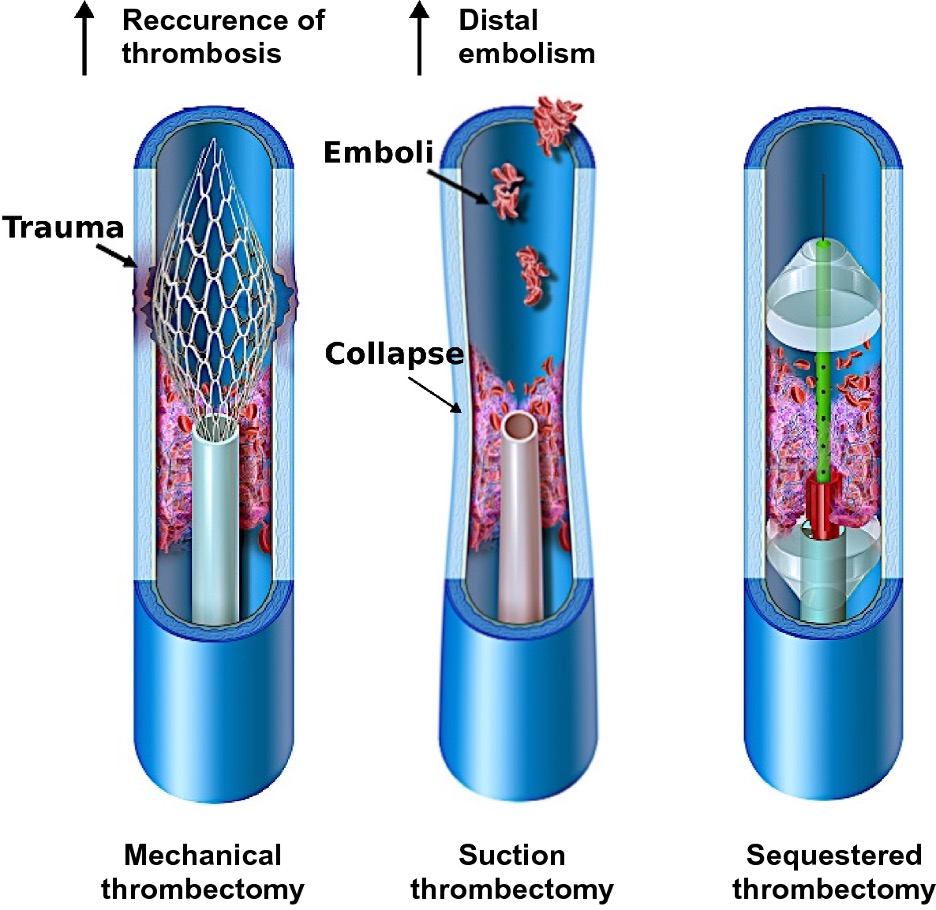
Multimodal thrombectomy device for treatment of acute deep venous thrombosis
-
- `
- Thrombophlebitis: Thrombus development in inflamed vein. e.g., IV site
- Introduction
- Types of Shock – hypovolemic, cardiogenic, obstructive, vasogenic, anaphylactic, septic
- Introduction
- Circulatory shock, commonly known simply as shock, is a life-threatening medical condition that occurs due to the provision of inadequate substrates for cellular respiration.Typical symptoms of shock include elevated but weak heart rate, low blood pressure, and poor organ function, typically observed as low urine output, confusion, or loss of consciousness.
-
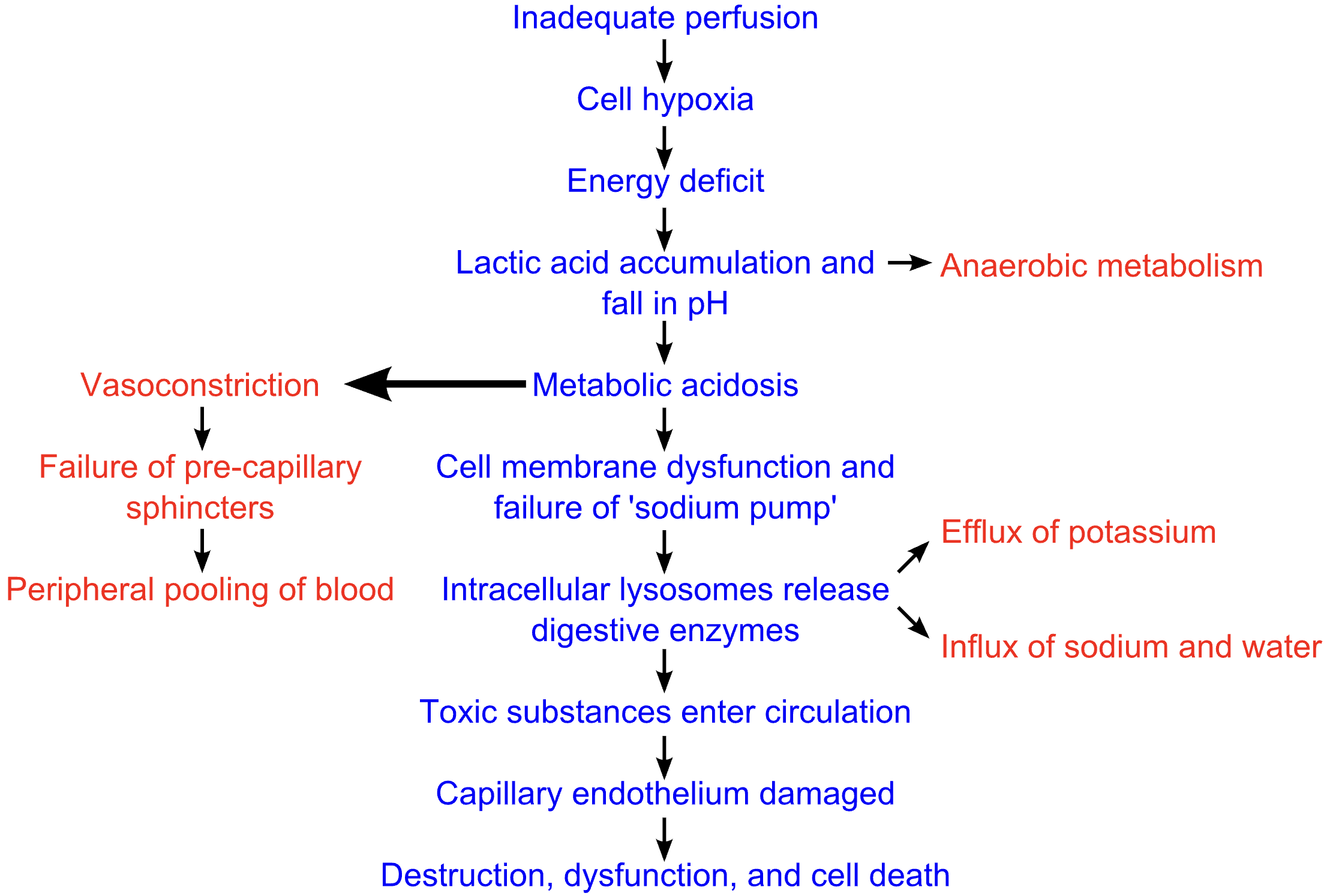
The scheme depicts the cell metabolic response as a result of inadequate blood delivery during circulatory shock.
- Summary
-
Type Mechanism Specific Cause Hypovolemic Loss of blood or plasma Hemorrhage, burns (fluid shift & edema), dehydration, peritonitis (fluid shift →third-spacing), pancreatitis Cardiogenic Decreased pumping capability of the heart Myocardial infarction of left ventricle, cardiac arrhythmia, pulmonary embolus, cardiac tamponade Obstructive Interference with blood flow through the heart Cardiac tamponade or pulmonary embolus Vasogenic (neurogenic or distributive) Vasodilation owing to loss of sympathetic & vasomotor tone Pain and fear, spinal cord injury (loss of SNS), hypoglycemia (insulin shock) Anaphylactic Systemic vasodilation & increased permeability owing to severe allergic reaction Insect stings, drugs, nuts, shellfish stimulating mast cells to release massive amounts of histamine Septic (endotoxic) Vasodilation owing to severe infection, often with gram-negative bacteria Virulent microorganisms (gram-negative bacteria) or multiple infections cause APCs to release massive cytokines→↑NO→↑ -
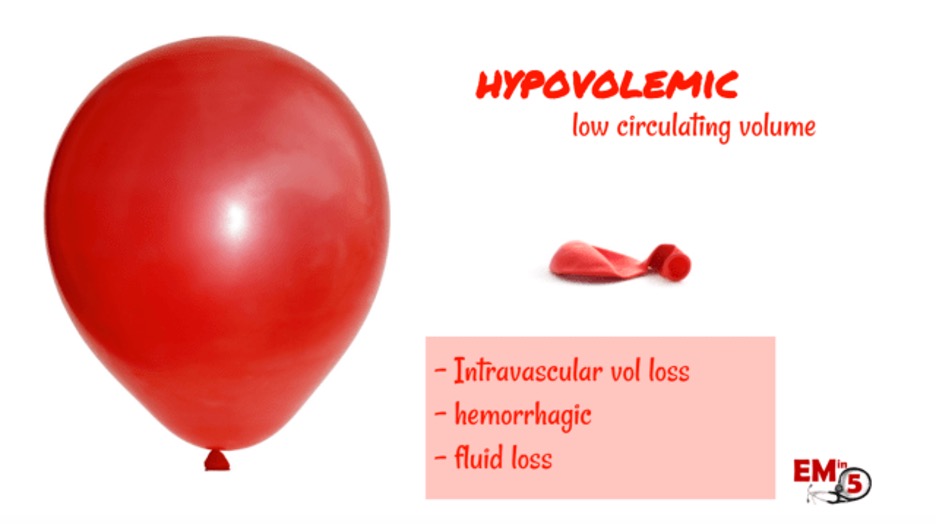
Hypovolemic shock: This is an issue with low circulating volume and includes patients who have been bleeding, vomiting, having diarrhea, or are generally volume down. -
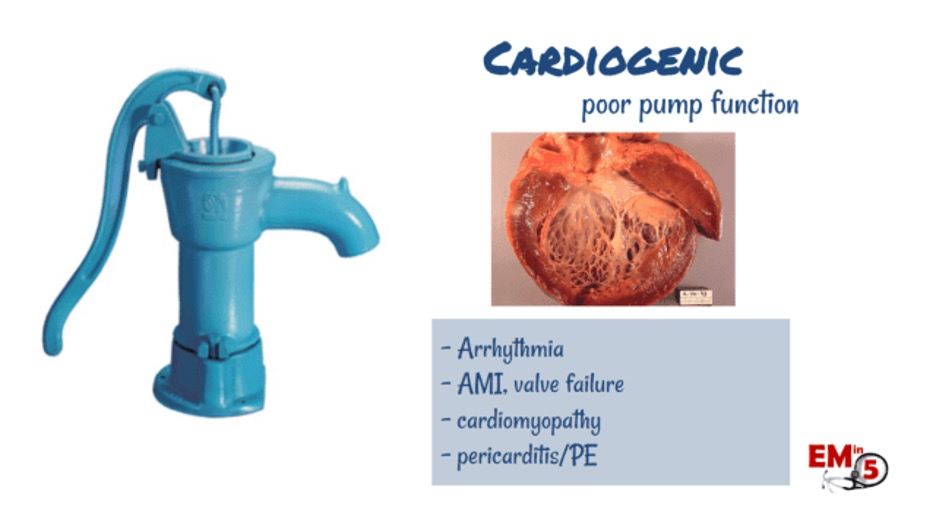
Cardiogenic shock: This is a problem with poor cardiac pump function, and can be caused by a number of different things including acute MI, valve failure, arrhythmias, cardiomyopathy, and pericarditis/myocarditis. -
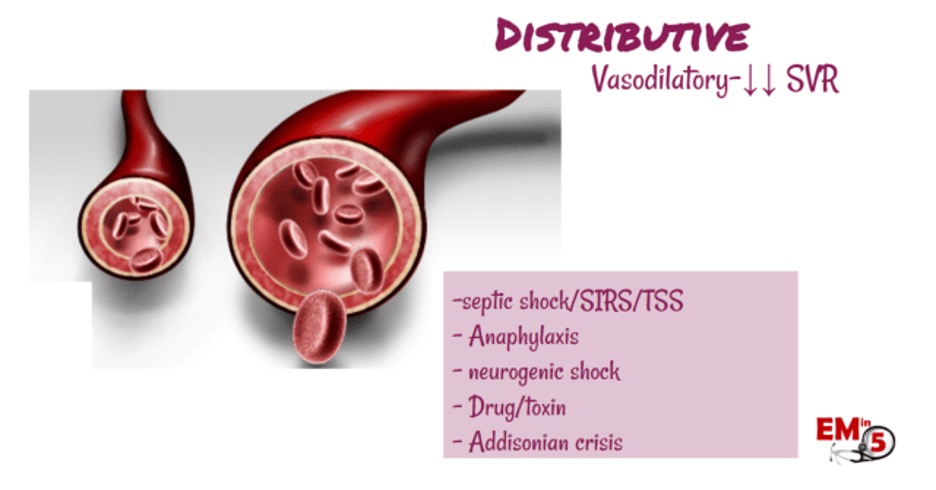
Distributive shock: This is the one that we probably think about most commonly, and includes a wide range of categories. But they all share something in common, and therefore are managed in a similar fashion – they all have a problem with severe peripheral vascular vasodilation. Examples include sepsis, anaphylaxis, neurogenic shock, and various drugs and toxins. -
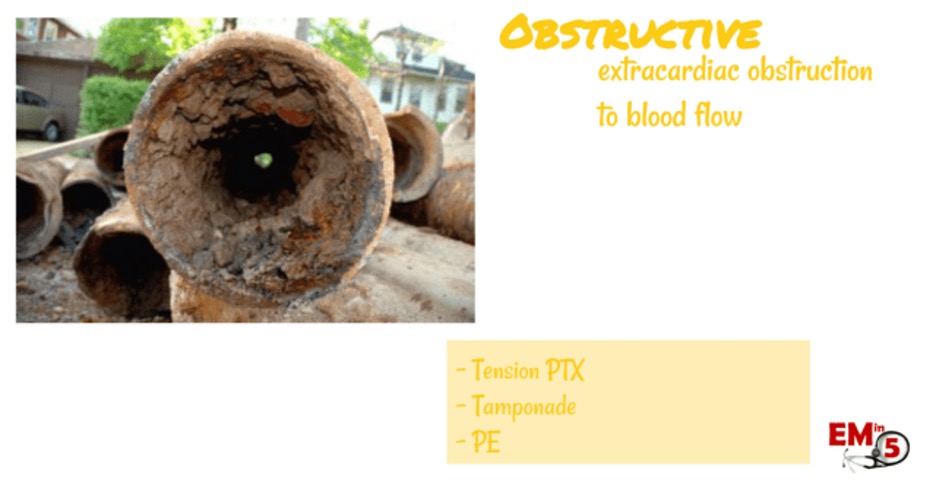
Obstructive shock: In this type of shock, there is no problem with the peripheral vasculature or the heart – it’s a problem with something obstructing the flow of blood. For example, a PE, tamponade, or a pneumothorax. -
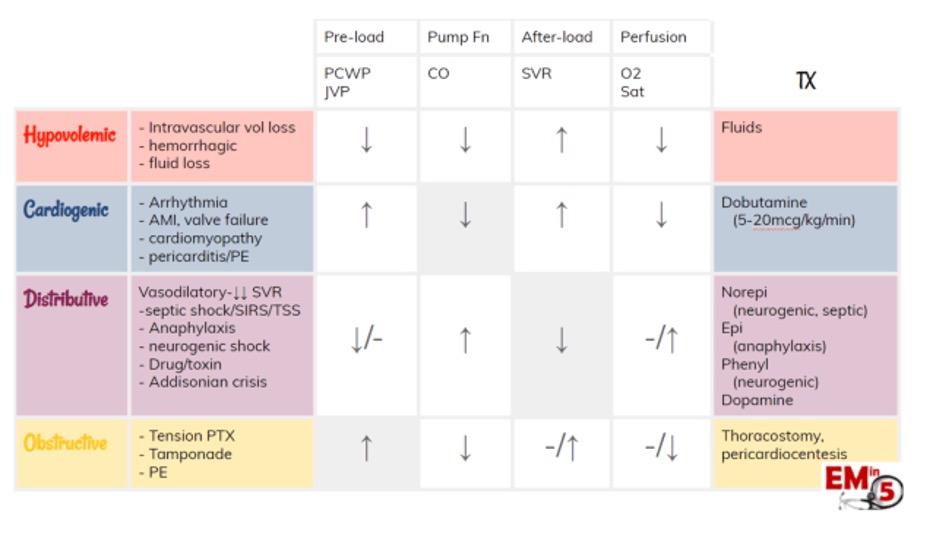
A summary of how these 4 types of shock affect the circulatory system. 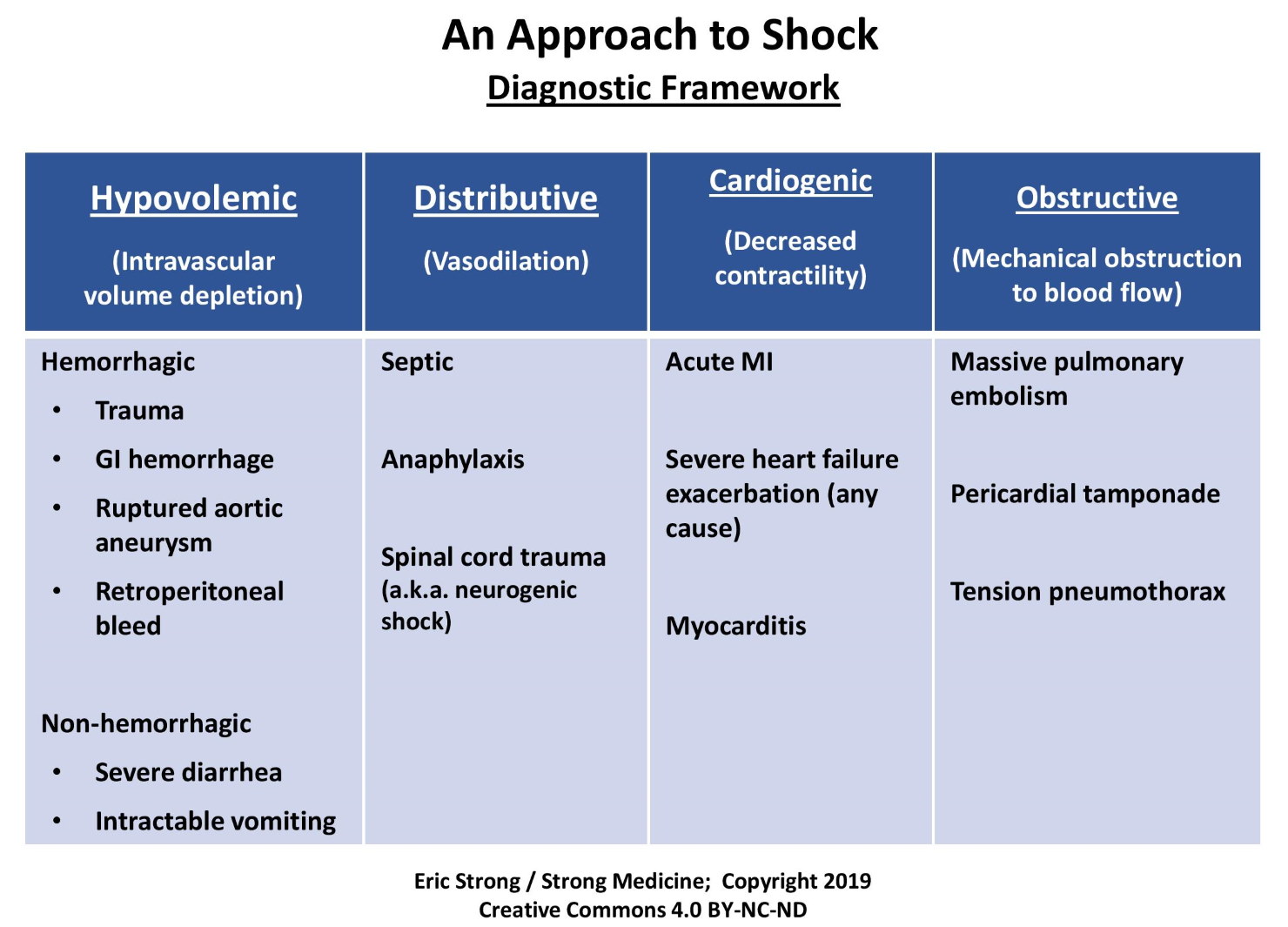
-
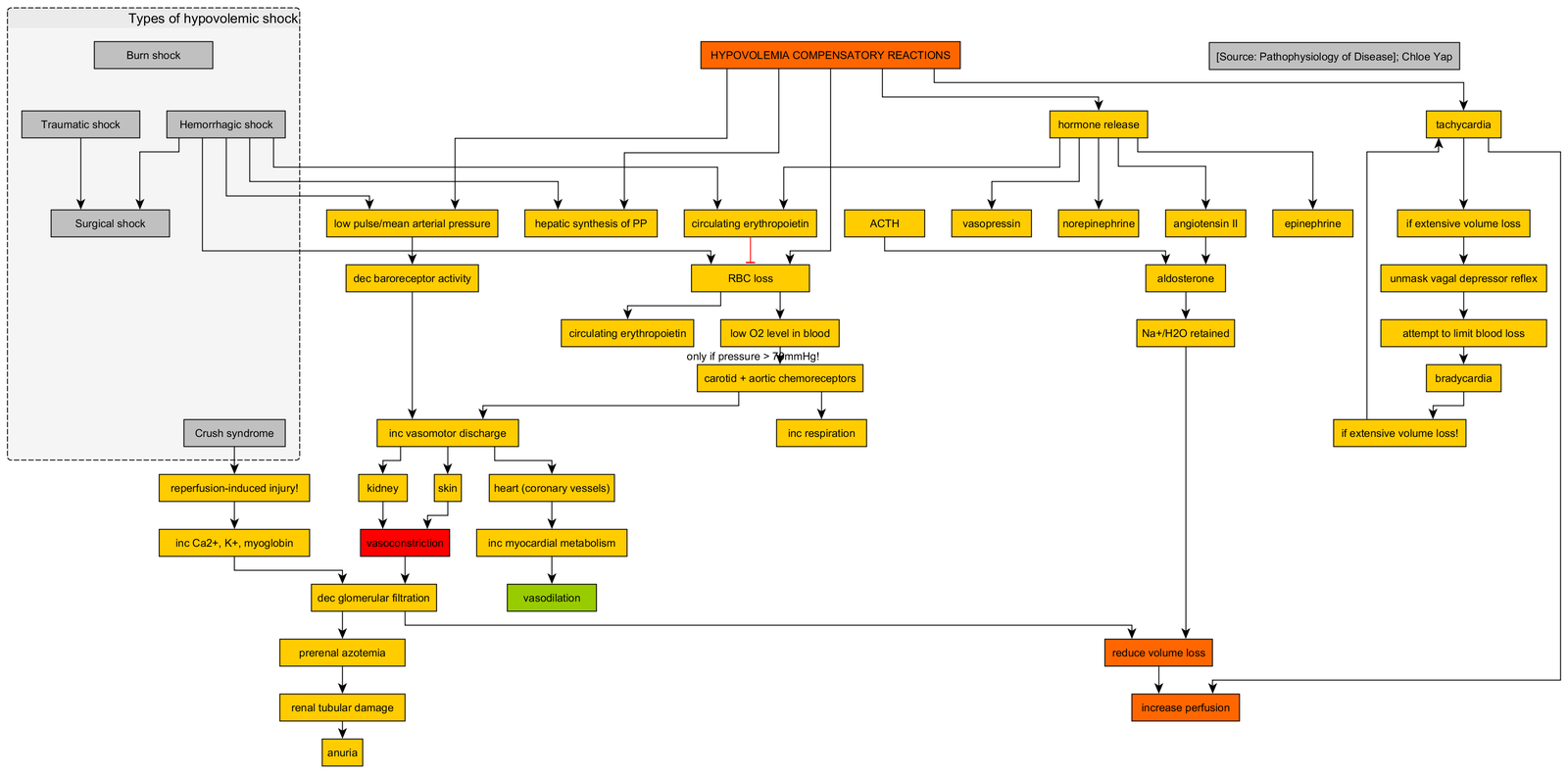
Hypovolemic Shock Pathophysiology of Disease - `
-
- Types of shock
- Hypovolemic shock, the most common type, is caused by insufficient circulating volume, typically from hemorrhage although severe vomiting and diarrhea are also potential causes. Hypovolemic shock is graded on a four-point scale depending on the severity of symptoms and level of blood loss. Typical symptoms include a rapid, weak pulse due to decreased blood flow combined with tachycardia, cool, clammy skin, and rapid and shallow breathing. Hypovolemic shock is characterized by loss of effective circulating blood volume, which leads to rapid pulse, cool skin, shallow breathing, hypothermia, thirst, and cold mottled skin.
- Cardiogenic shock is caused by a failure of the heart to pump correctly, either due to damage to the heart muscle through myocardial infarction or through cardiac valve problems, congestive heart failure, or dysrhythmia. Cardiogenic shock is characterized by distended jugular veins, weak or absent pulse, and arrhythmia.
- Obstructive shock is caused by an obstruction of blood flow outside of the heart. This typically occurs due to a reduction in venous return, but may also be caused by blockage of the aorta.
- Neurogenic shock arises due to damage to the central nervous system, which impairs cardiac function by reducing heart rate and loosening the blood vessel tone, resulting in severe hypotension.
- Distributive shock is caused by an abnormal distribution of blood to tissues and organs and includes septic, anaphylactic, and neurogenic causes. Distributive shock includes septic shock, characterized by fever or anaphylaxis, and neurogenic shock, characterized by a reduced heart rate and vasodilation of superficial vessels warming the skin.
- Anaphylactic shock is caused by a severe reaction to an allergen, leading to the release of histamine that causes widespread vasodilation and hypotension.
- Septic shock is the most common cause of distributive shock and is caused by an overwhelming systemic infection that cannot be cleared by the immune system, resulting in vasodilation and hypotension.
- Signs and symptoms
- Early: thirst, agitation, restlessness, anxiety due to early SNS stimulation by hypotension
- Then: cool, moist, pale skin; tachycardia; oliguria as vasoconstriction shunts blood from viscera & skin to vital areas. (Note: septic shock results in fever, warm, dry flushed skin with rapid, strong pulse & hyperventilation)
- Next: lethargy, weakness, dizziness; weak, thread pulse due to hypotension & decreased blood flow
- Increased respirations: due to hypoxia lead to respiratory alkalosis
- Metabolic acidosis occurs and is compensated for by increased respirations
- Due to low O2, anaerobic respiration takes over (glucose → lactic acid +ATP)
- Oxygen supplies dwindle & waste accumulates → ↓responsiveness
- Decompensated metabolic acidosis as pH drops below 7.35 leads to CNS depression and acute renal failure (due to tubular ischemia & necrosis)
- Increasing serum urea & creatinine (due to kidney failure)
- Compensation mechanisms
- Complications of Shock
-
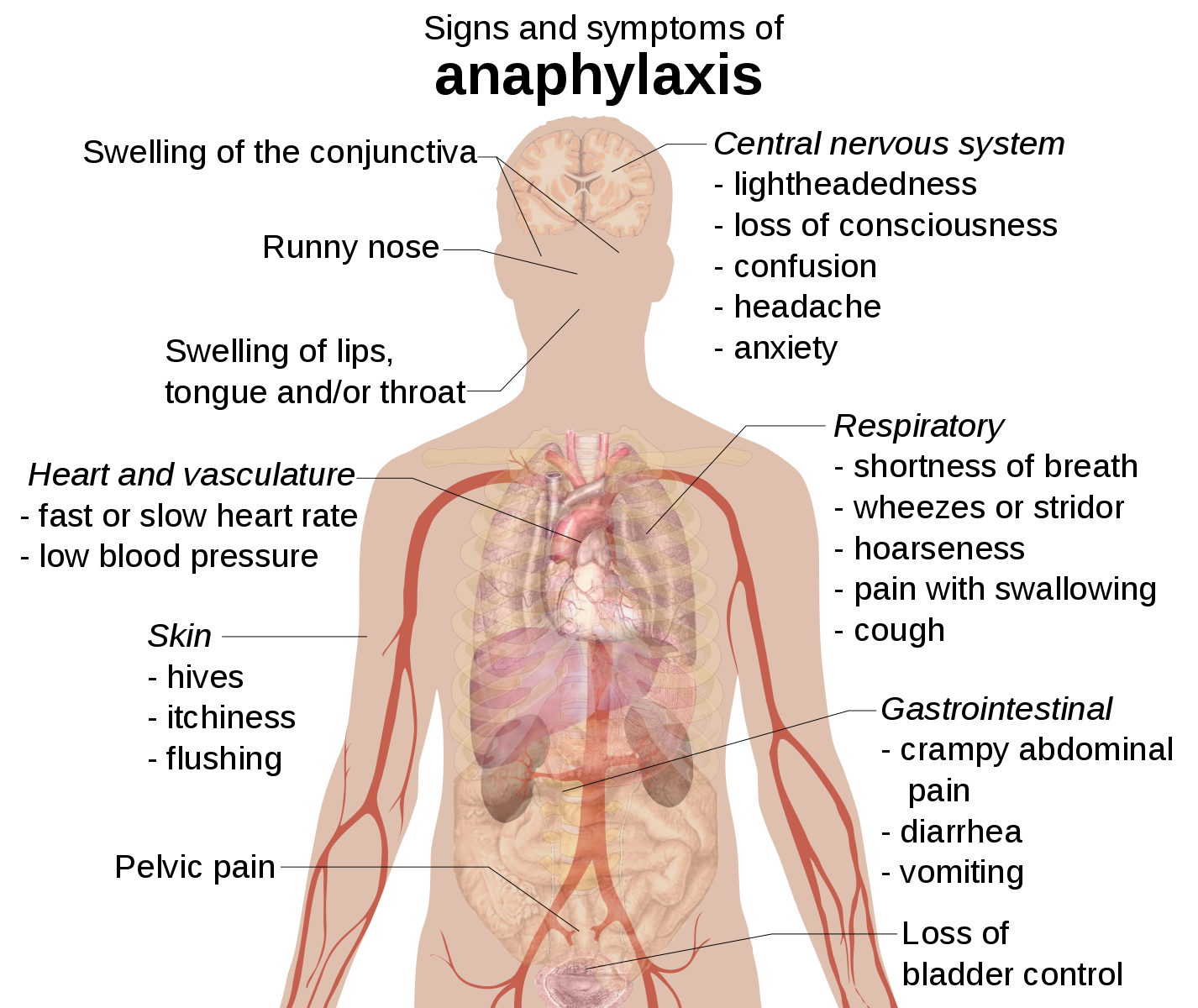
Signs and symptoms of anaphylaxis - Acute renal failure (tubular necrosis) = Acute Kidney Injury
- Shock lung, or adult respiratory distress syndrome (ARDS) due to pooling of blood (pulmonary congestion) & alveolar damage
- Hepatic failure (necrosis)
- Paralytic ileus (intestinal blockage due to malfunction of nerves & muscles); stress or hemorrhagic ulcers (↓gastric mucosa maintenance)
- Infection or septicemia (ischemia AND toxins depress myocardial function; high mortality rate) – if intestines become ischemic, bacteria may enter blood stream – complication of endotoxic shock
- Disseminated intravascular coagulation (thrombi form and obstruct microcirculation)
- Depression of cardiac function (due to hypoxia, acidosis & hyperkalemia)
- Multiple organ failure; Death
-
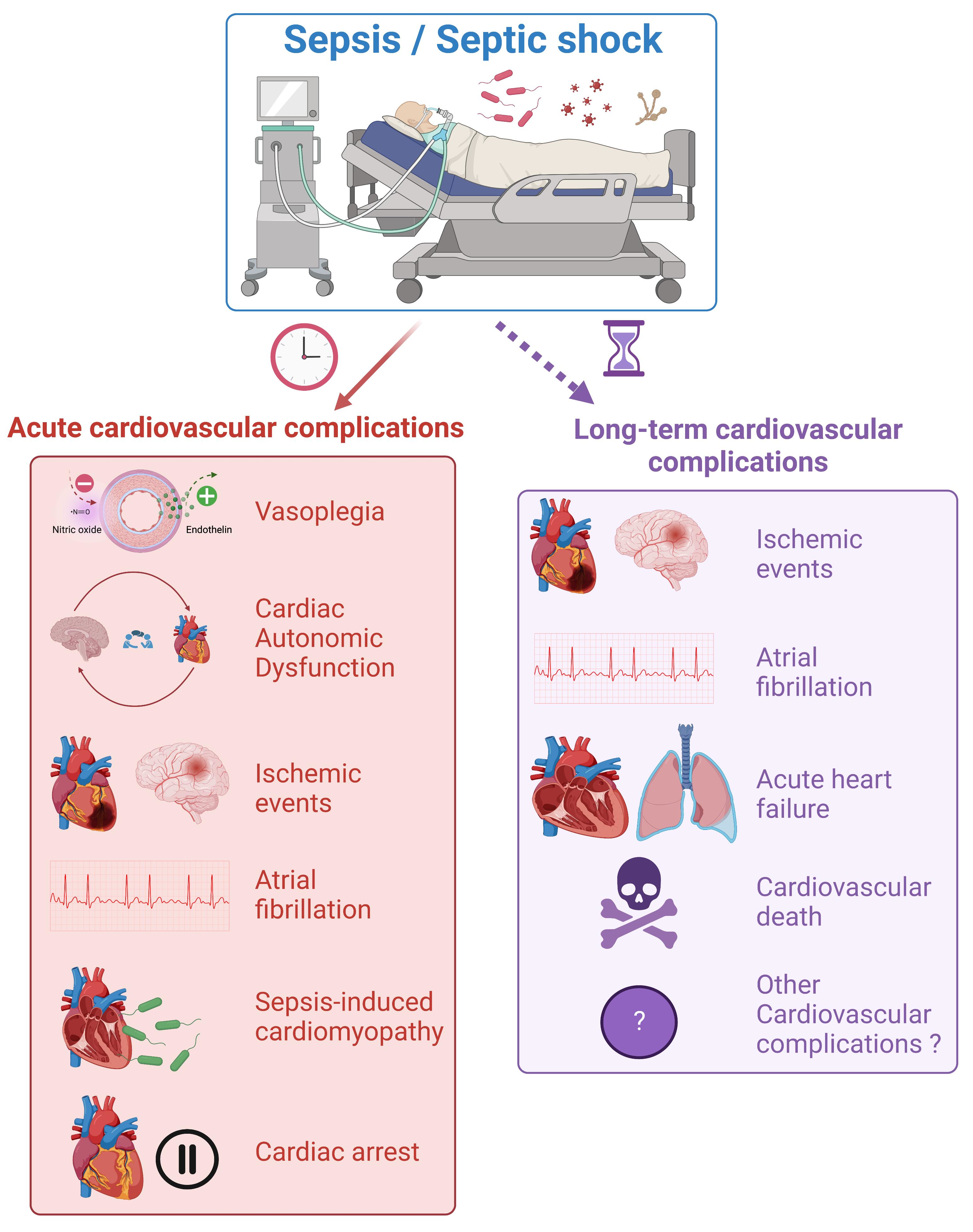
Acute and Long-Term Cardiovascular Complications among Patients with Sepsis and Septic Shock.
-
- Manifestations of Shock
- General Effects of Circulatory Shock
- Treatment
- Shock, in general:
- O2 therapy; vasoconstrictors/vasodilators (depending on type & cause of shock)
- Cover and keep warm; keep patient supine; treat underlying cause
- Hypovolemic shock:
- Apply pressure to stop bleeding
- Blood transfusion, IV fluid
- Anaphylactic shock:
- EpiPen
- Anti-histamines
- Corticosteroids
- EpiPen
- Septic shock:
- Anti-microbials
- Glucocorticoids
- Shock, in general:
- Introduction