Chapter 9 Selected Diseases and Disorders of the Endocrine System
Chapter 9 Endocrine System Diseases and Disorders – Mahdi
Zoë Soon
Creative Commons – Simple Pictures, Images, Video Clips, and/or Gifs that help illustrate any of the following:
*For diseases we discuss:
a) Basic Risk Factors
b) Most Common signs and symptoms
c) Basic Pathology, with basic diagnostic tools (e.g. imaging, blood tests) and basic treatment
- Endocrine System – Hypothalamus, Anterior and Posterior Pituitary Gland, Thyroid Gland, Adrenal Gland, Pancreatic Islets, Pineal Gland, Parathyroid Glands
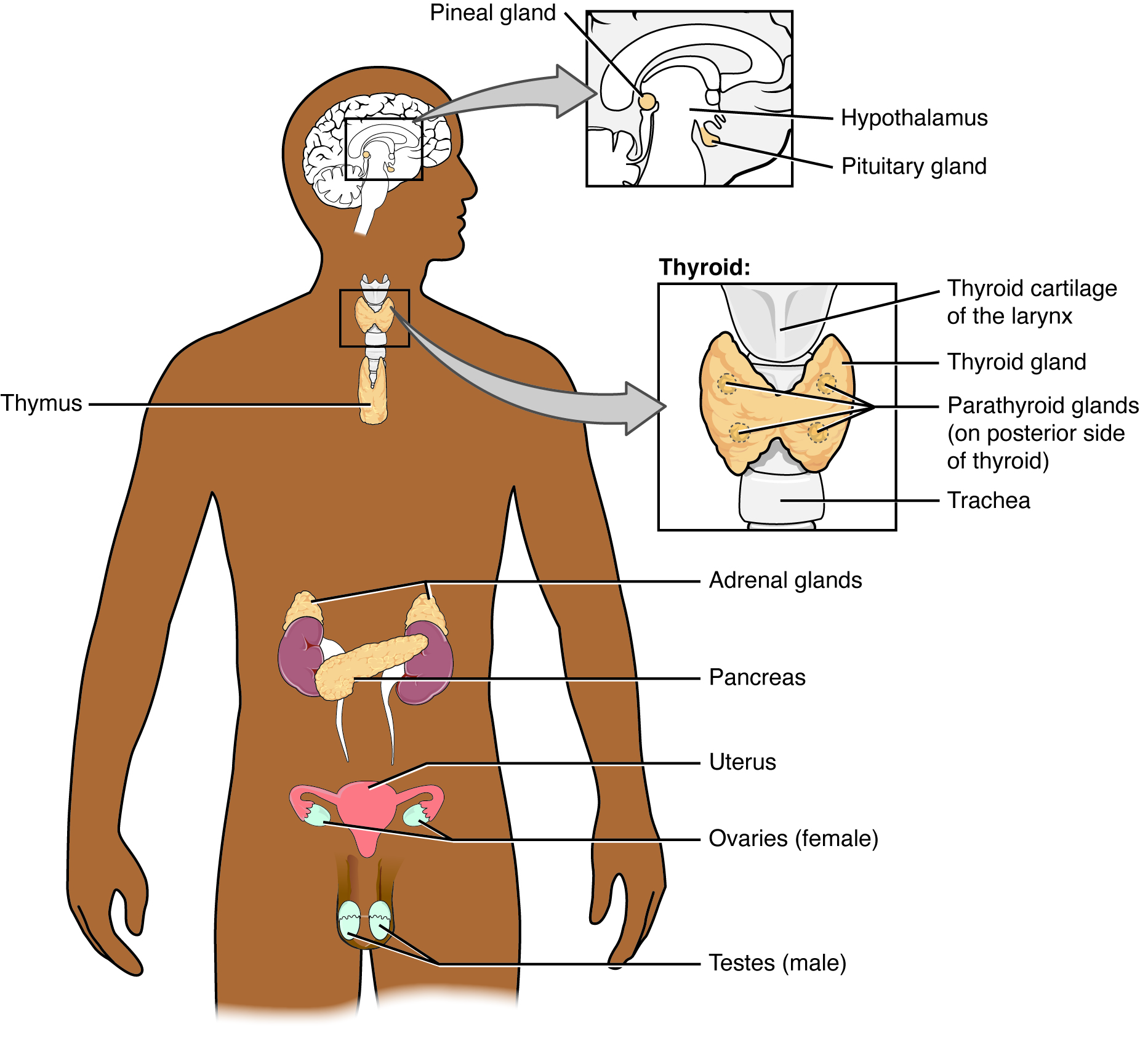
Endocrine System Endocrine glands and cells are located throughout the body and play an important role in homeostasis. 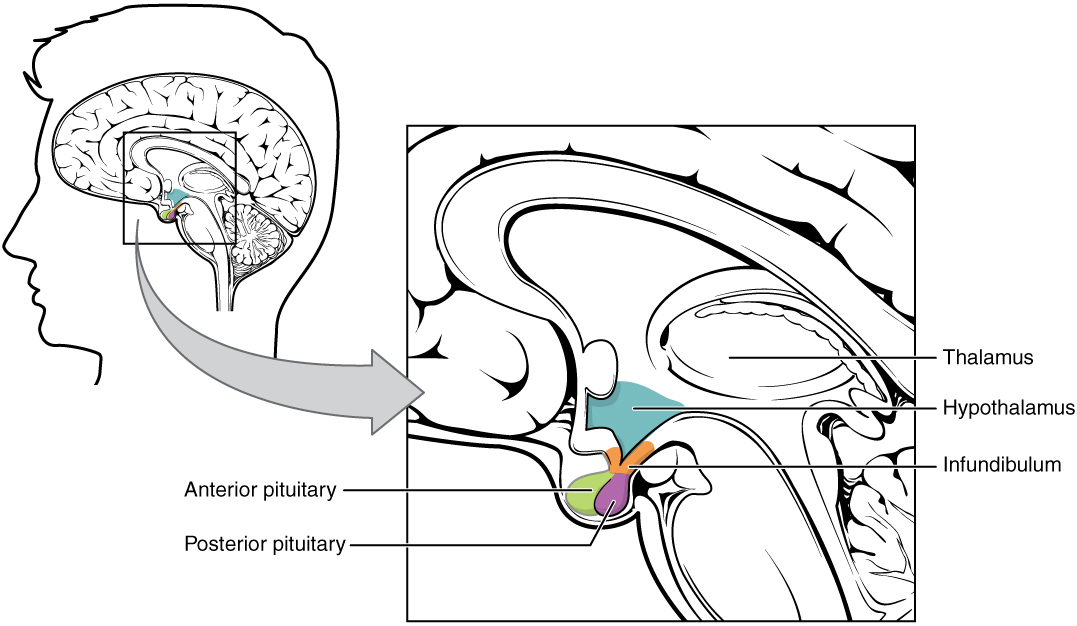
The hypothalamus region lies inferior and anterior to the thalamus. It connects to the pituitary gland by the stalk-like infundibulum. The pituitary gland consists of an anterior and posterior lobe, with each lobe secreting different hormones in response to signals from the hypothalamus. 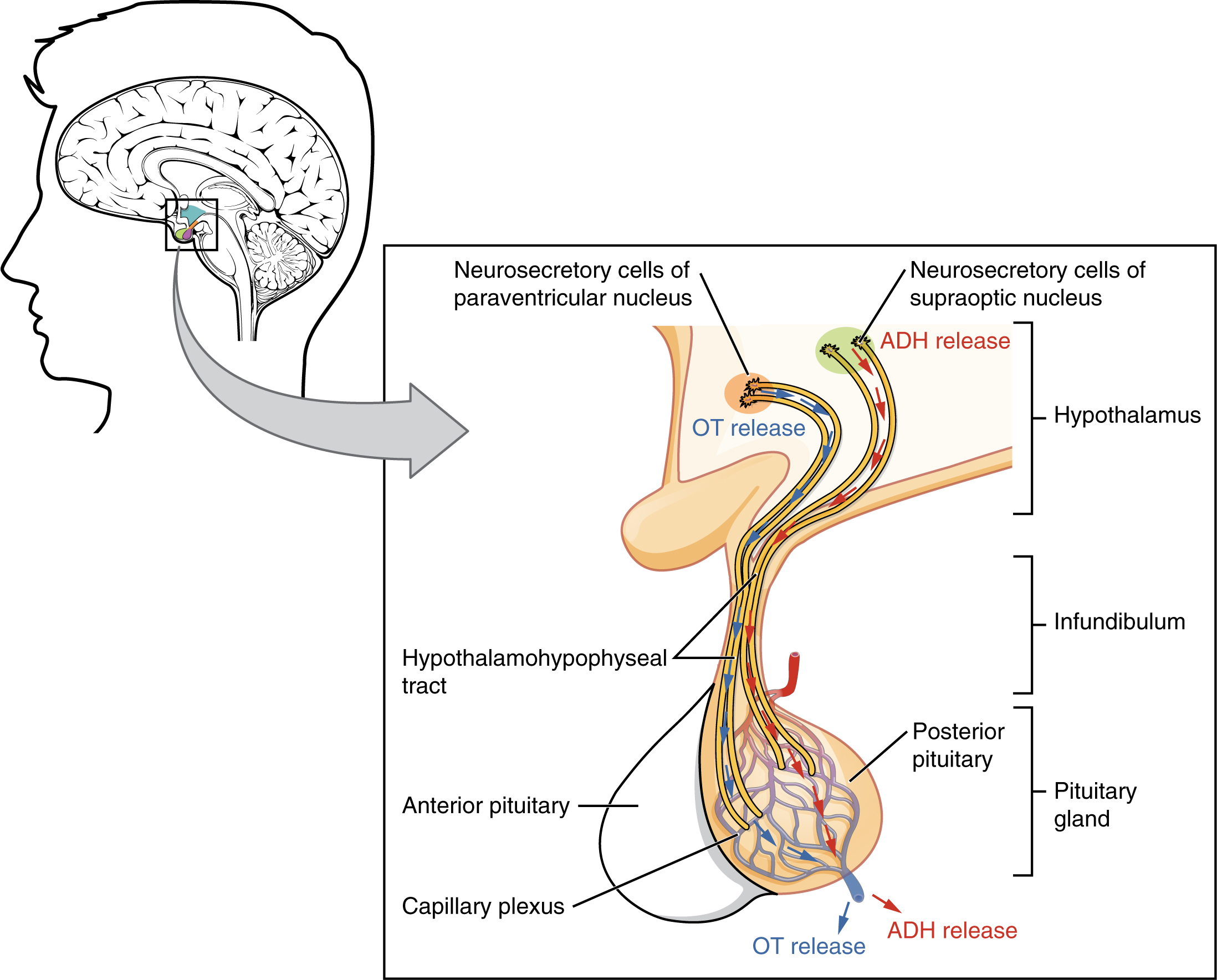
Neurosecretory cells in the hypothalamus release oxytocin (OT) or ADH into the posterior lobe of the pituitary gland. These hormones are stored or released into the blood via the capillary plexus. 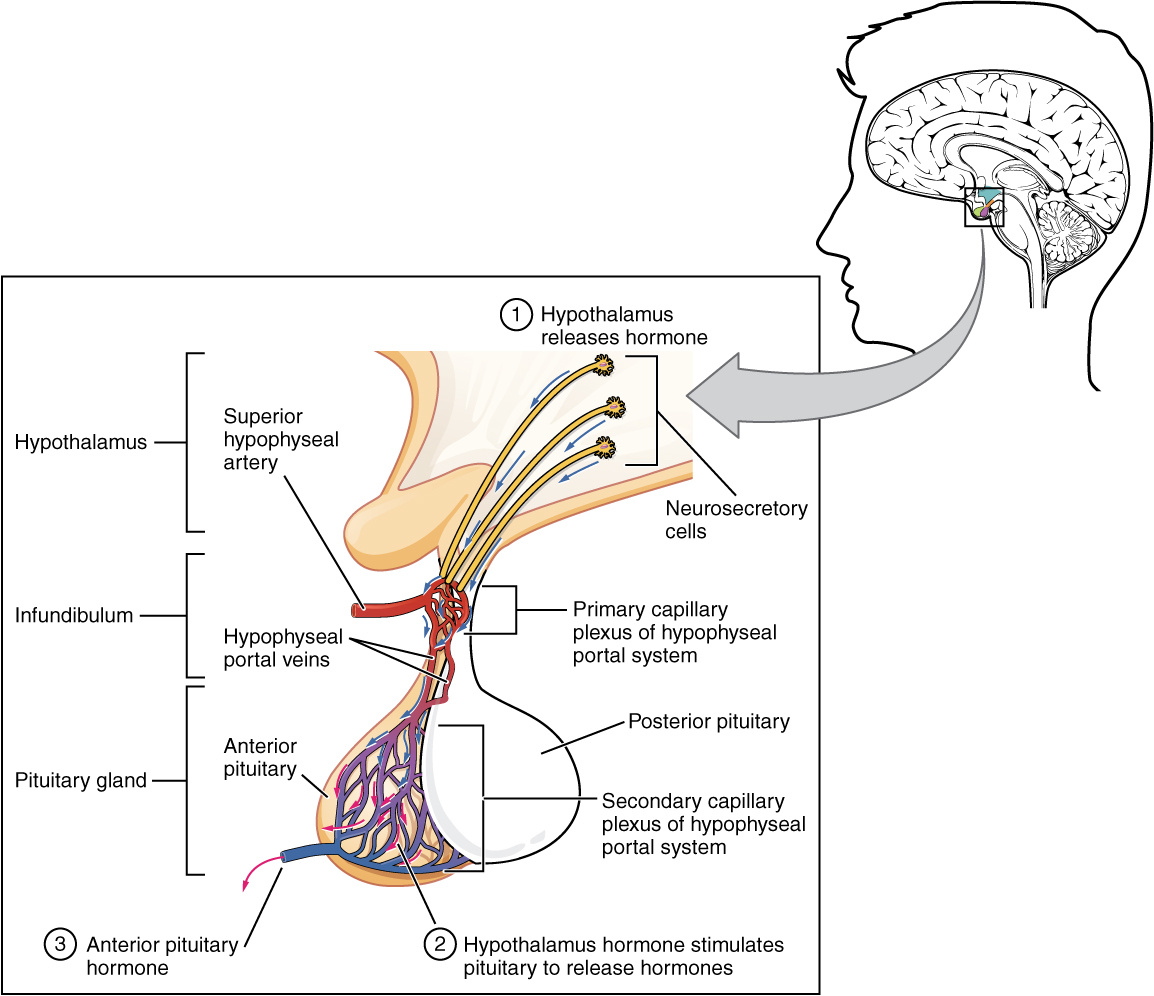
The anterior pituitary manufactures seven hormones. The hypothalamus produces separate hormones that stimulate or inhibit hormone production in the anterior pituitary. Hormones from the hypothalamus reach the anterior pituitary via the hypophyseal portal system. 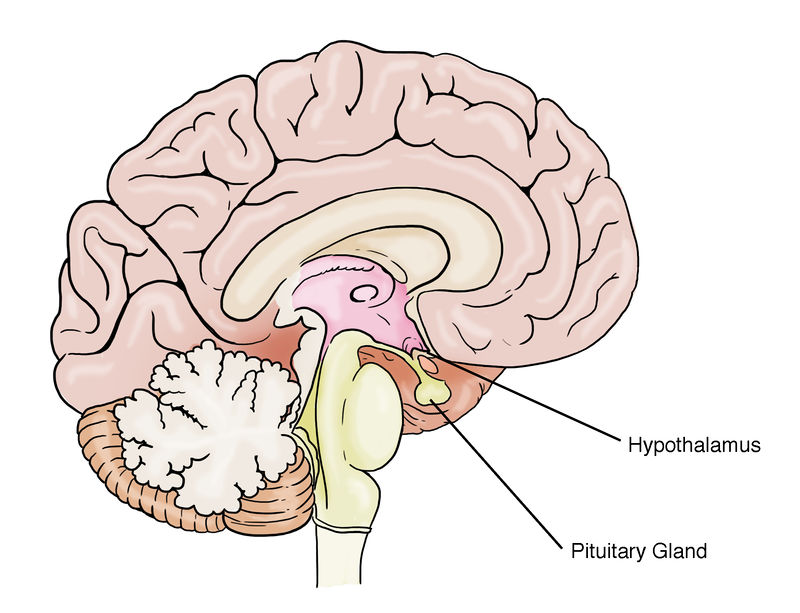
Location of the hypothalamus and pituitary gland. 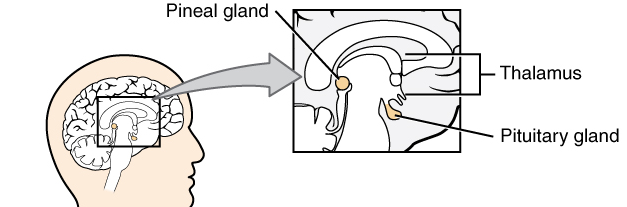
The pineal gland is located in the posterior aspect of the hypothalamus. 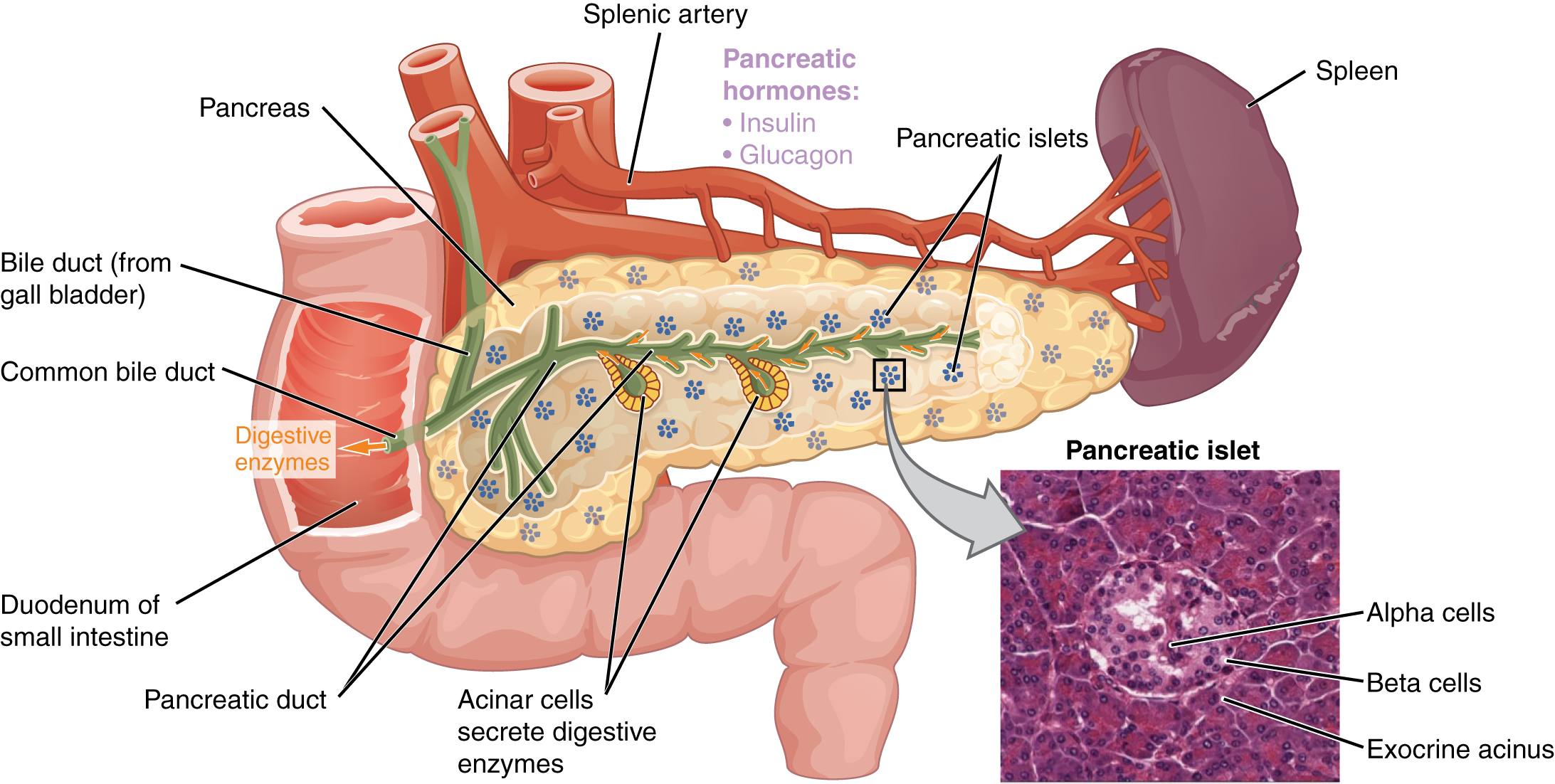
The pancreatic exocrine function involves the acinar cells secreting digestive enzymes that are transported into the small intestine by the pancreatic duct. Its endocrine function consists of the secretion of insulin (produced by beta cells) and glucagon (produced by alpha cells) within the pancreatic islets. These two hormones regulate the rate of glucose metabolism in the body. The micrograph reveals pancreatic islets. LM × 760. (Micrograph provided by the Regents of University of Michigan Medical School © 2012) 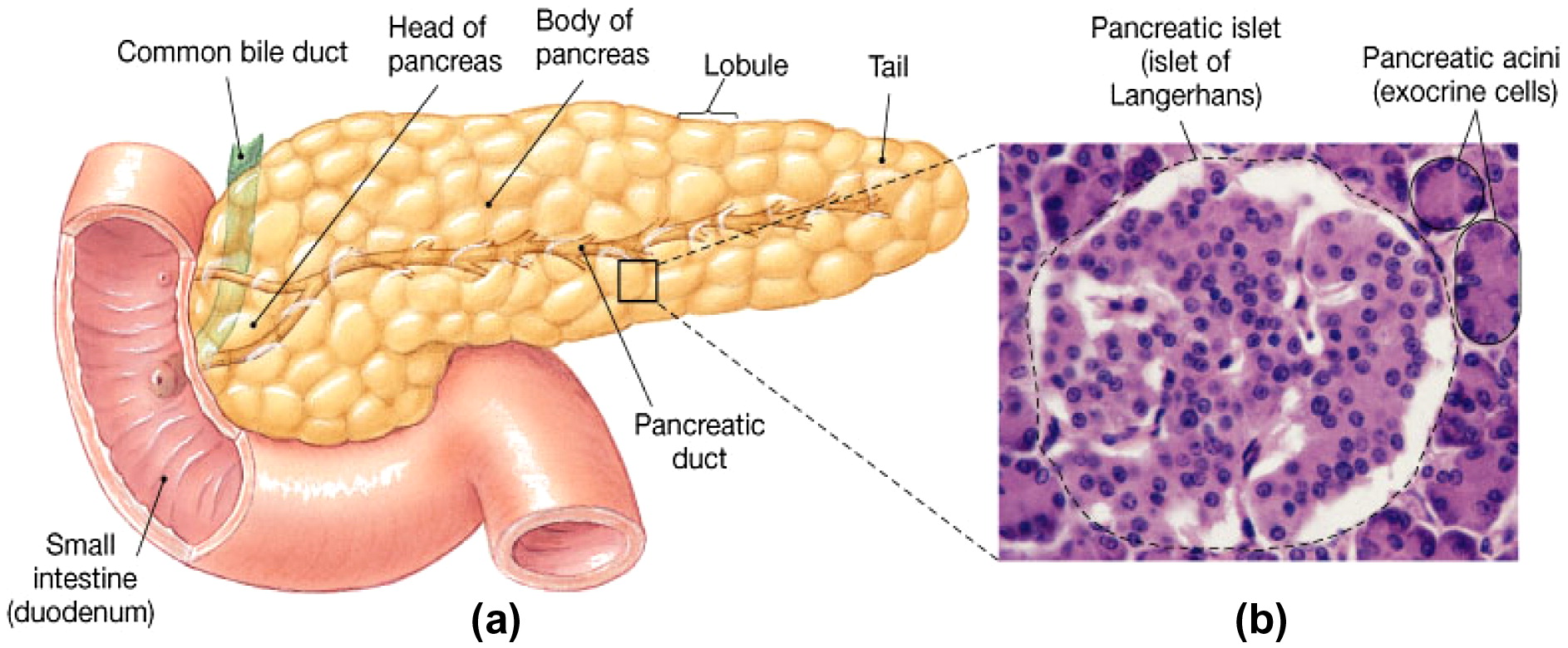
Histological structure of pancreas (Longnecker, 2014) 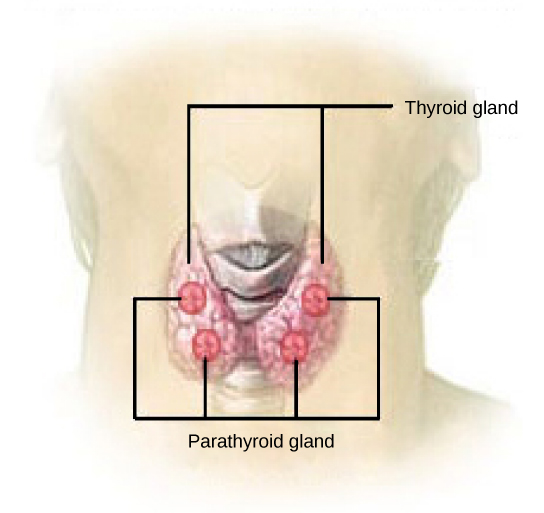
The parathyroid glands are located on the posterior of the thyroid gland. 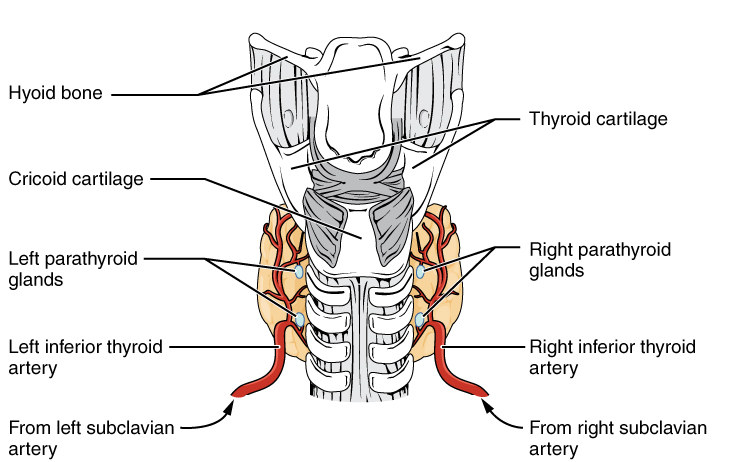
Posterior view of the thyroid gland. 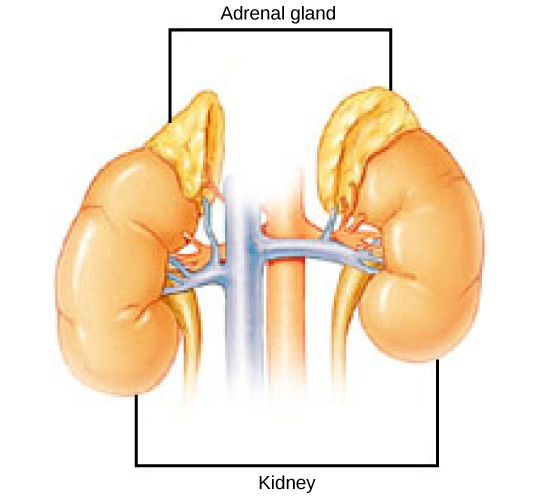
The location of the adrenal glands on top of the kidneys is shown. - Organs with Secondary Endocrine Functions – Heart, Thymus, Adipose Tissue, Digestive Tract, Kidneys, Gonads
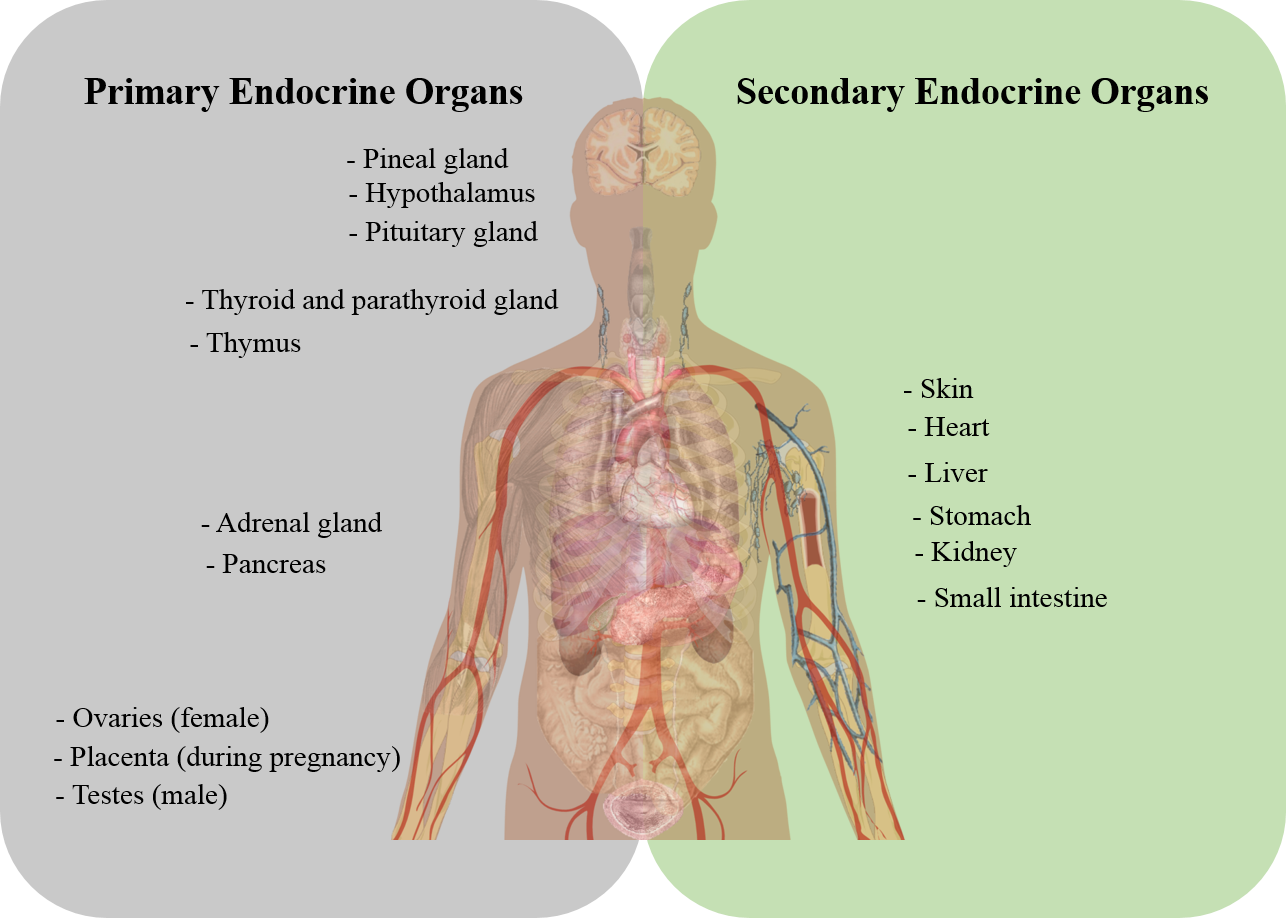
primary and secondary endocrine organs
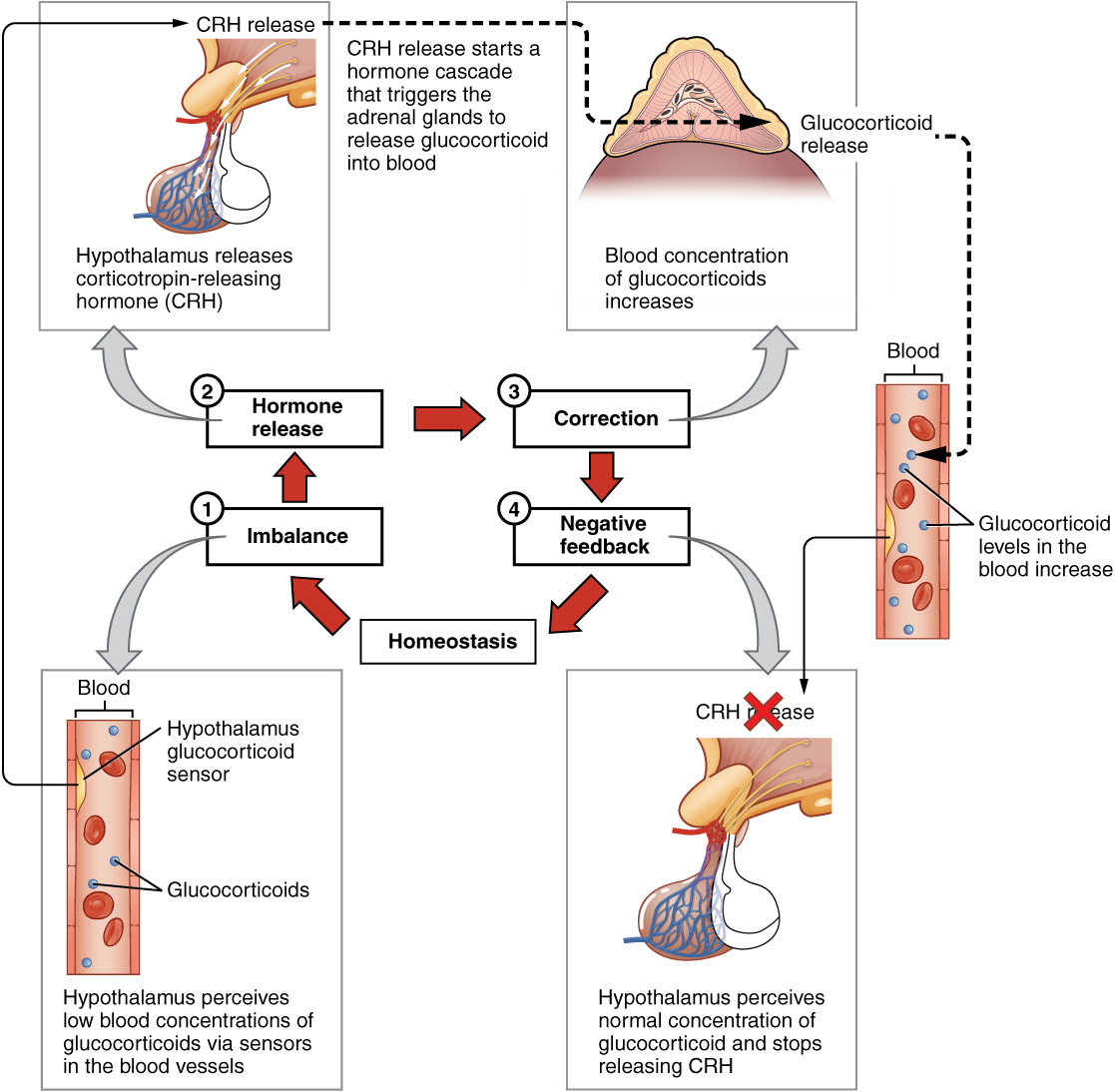
Typical Pattern of Hormone Regulation – Negative Feedback Loop
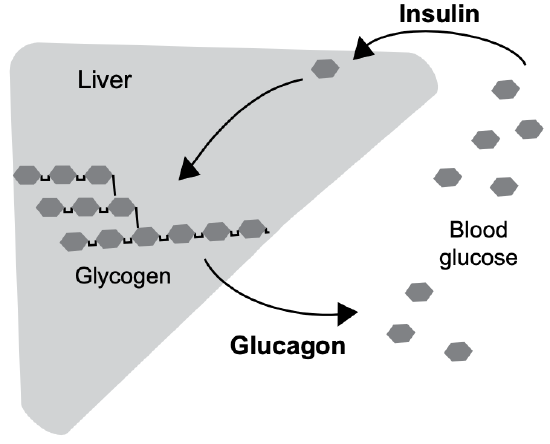
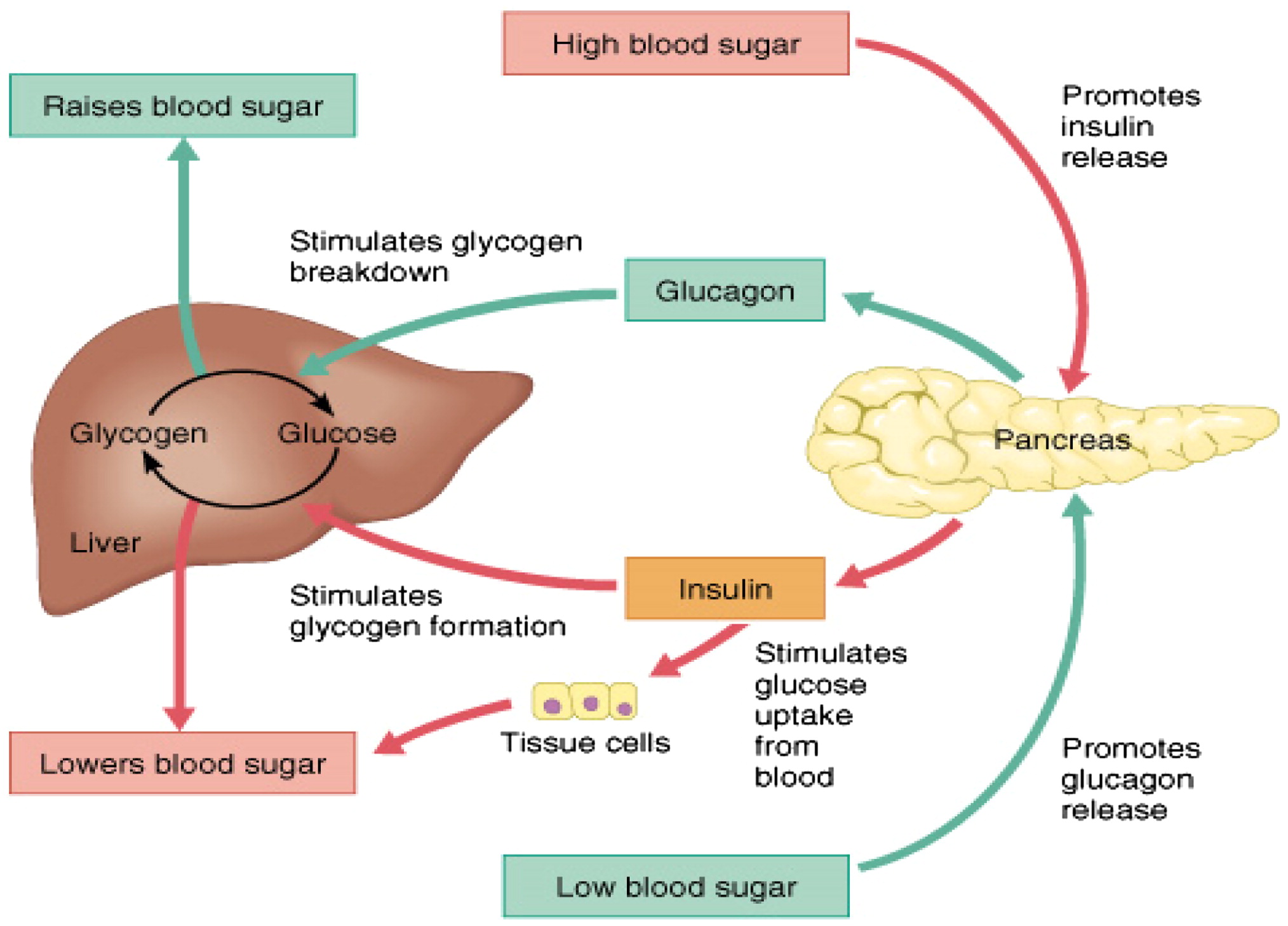
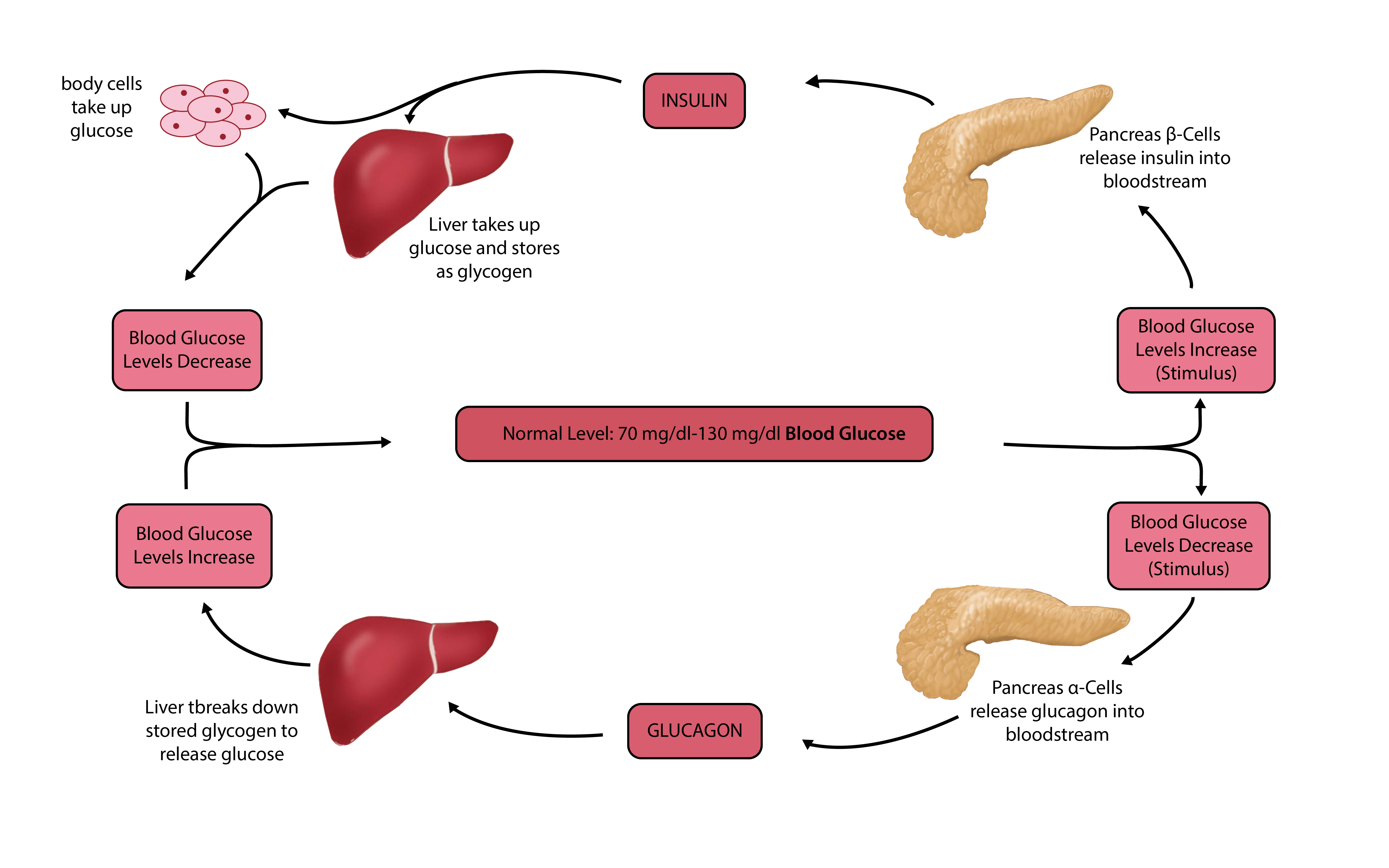
Glucagon and Insulin
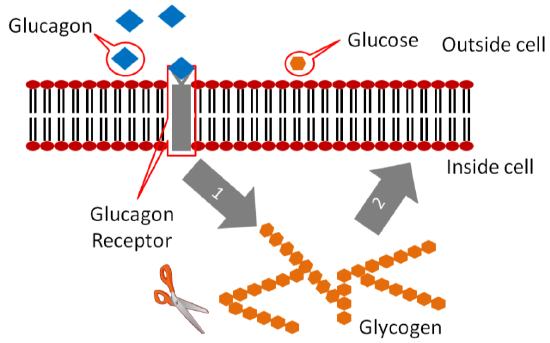
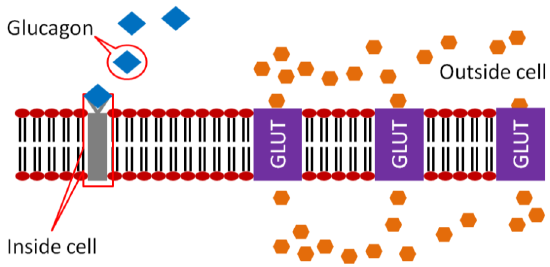
- Insulin Receptors, Glut4 channels
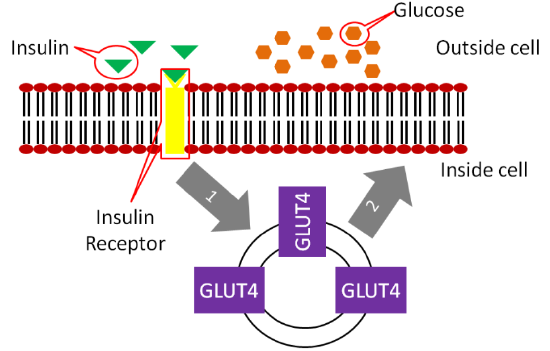
1) 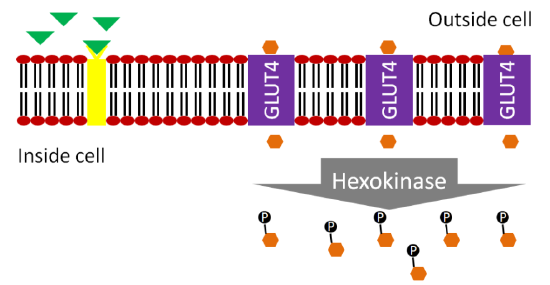
Response of muscle and adipose cells to insulin; 1) binding of insulin to its receptor, 2) movement of GLUT4 vesicles to the cell surface. - Type I Diabetes
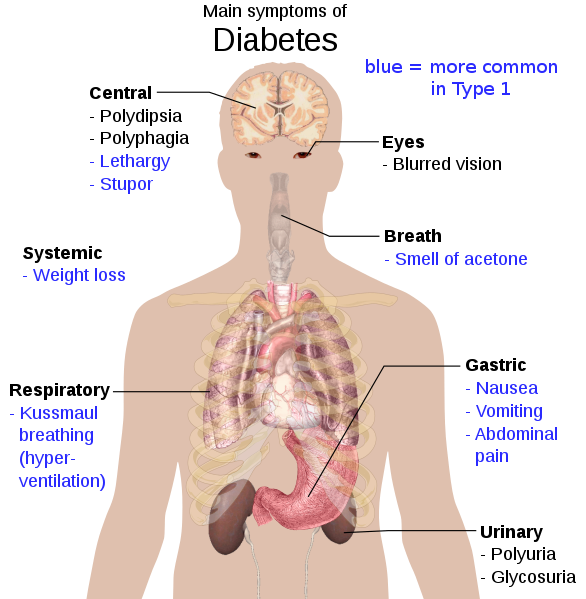
Overview of the most significant possible symptoms of diabetes. 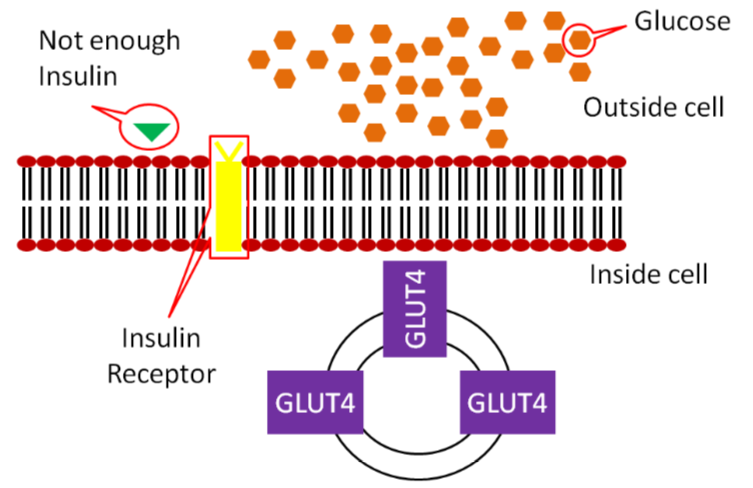
In type 1 diabetes, little to no insulin is produced; thus, insufficient insulin binds to the receptor. 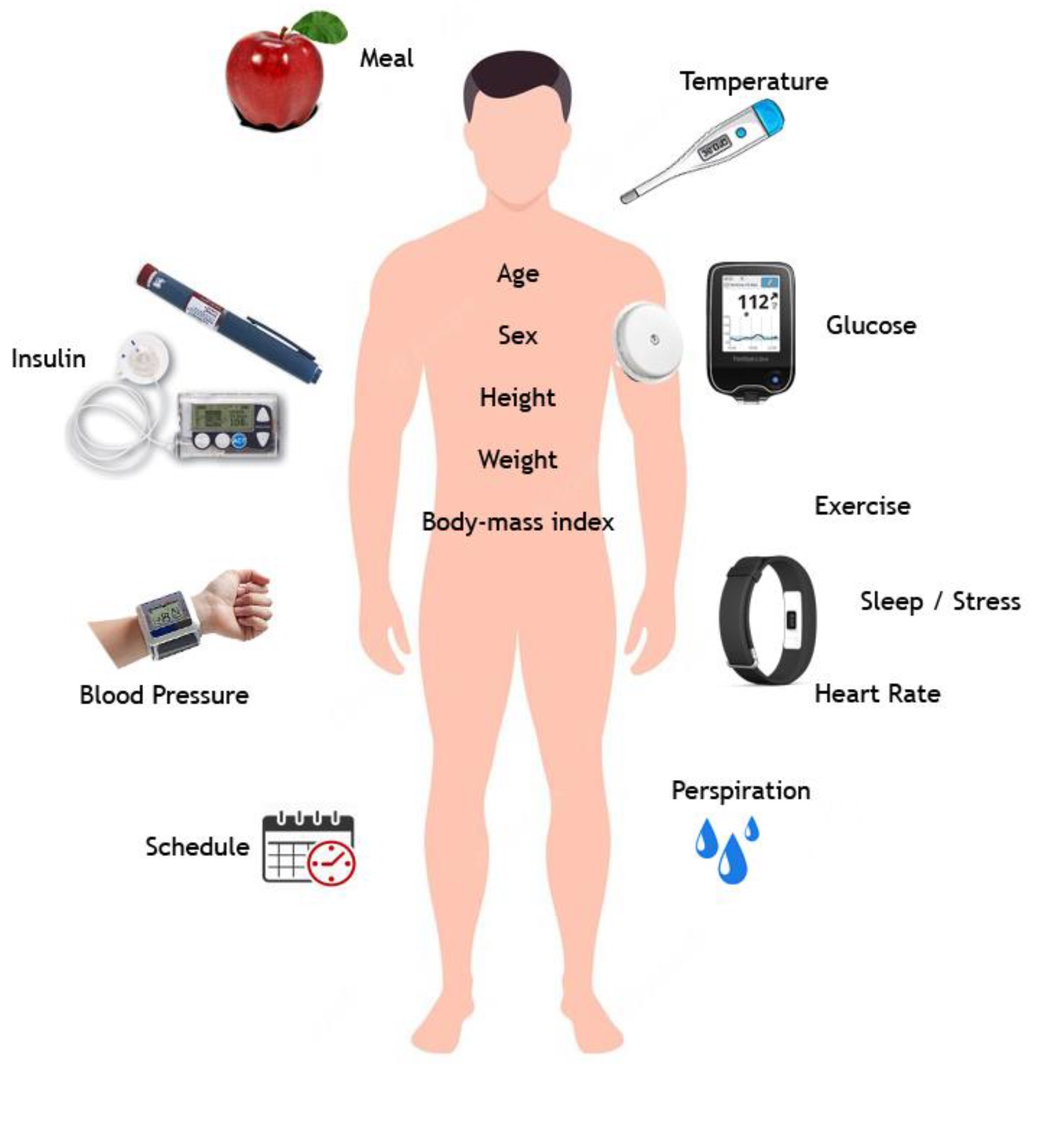
Variables related to Type 1 Diabetes Mellitus (DM1) in an Internet of Medical Things context. - Type II Diabetes
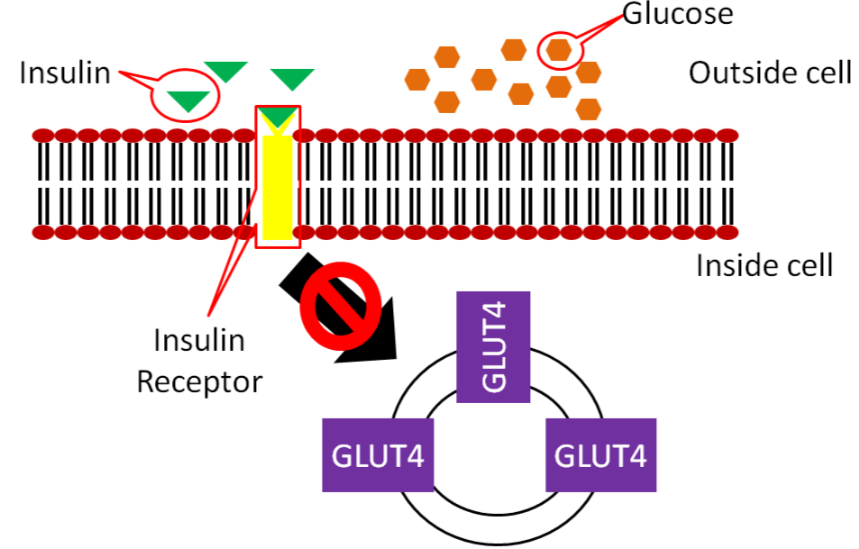
In Type 2 diabetes, the body produces enough insulin, but the person’s body resists it. In Type 2 diabetics, insulin binding to its receptor does not cause enough GLUT4 to move to the surface of the muscle and adipose cells, thus not enough glucose is taken up. 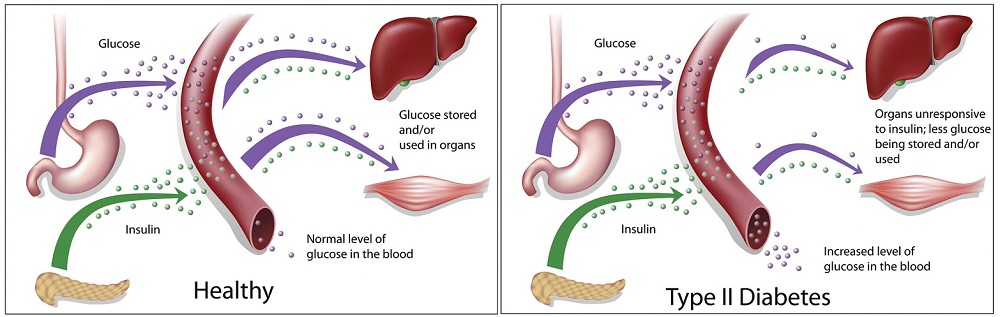
Type 2 diabetes is a metabolic disease characterized by high blood glucose levels. 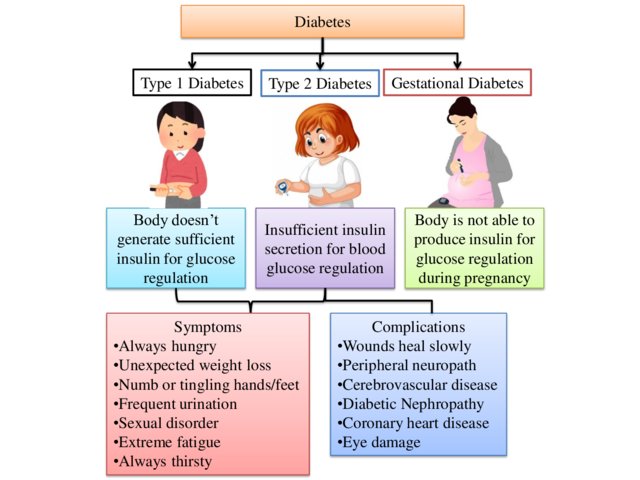
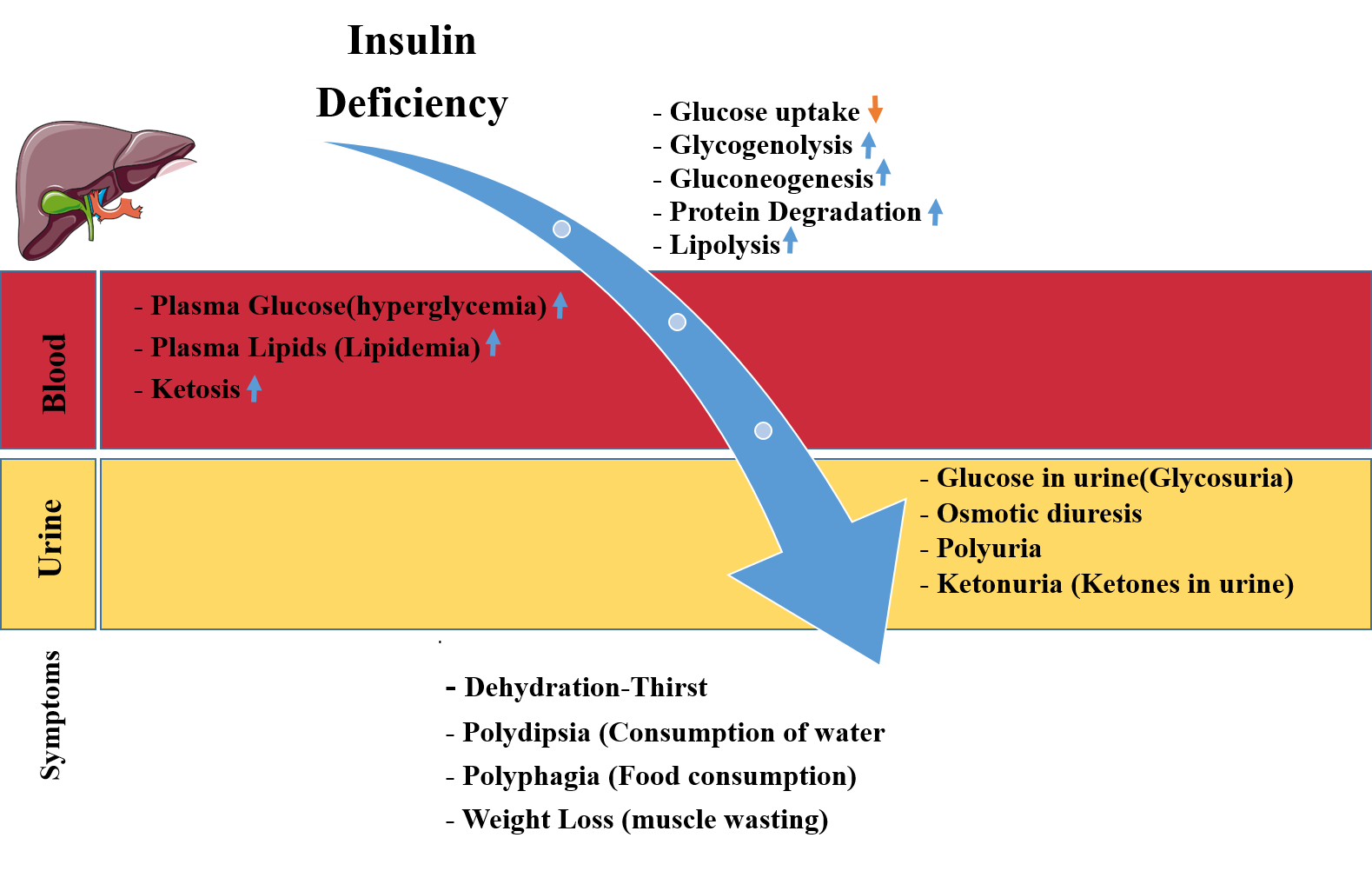
Different types of diabetes and their symptoms. - Signs of Diabetes Mellitus – Polydipsia, Polyphagia, Polyuria, Hyperglycemia, Glucosuria, Ketonemia, Ketonuria, lipidemia
- Gestational Diabetes
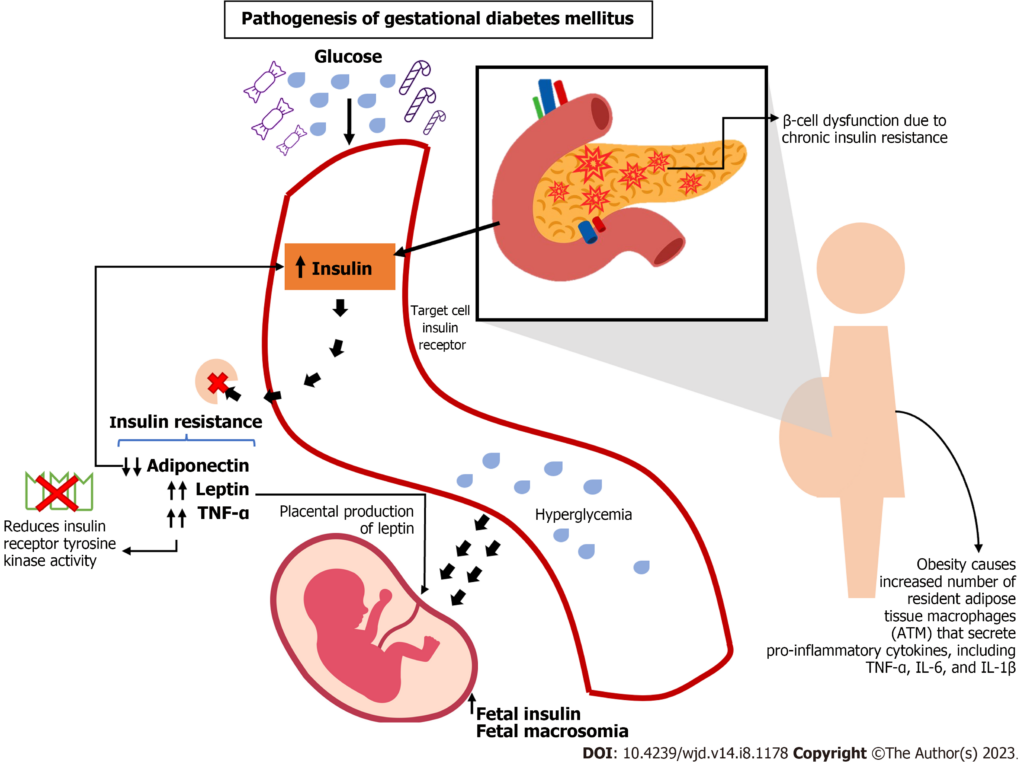
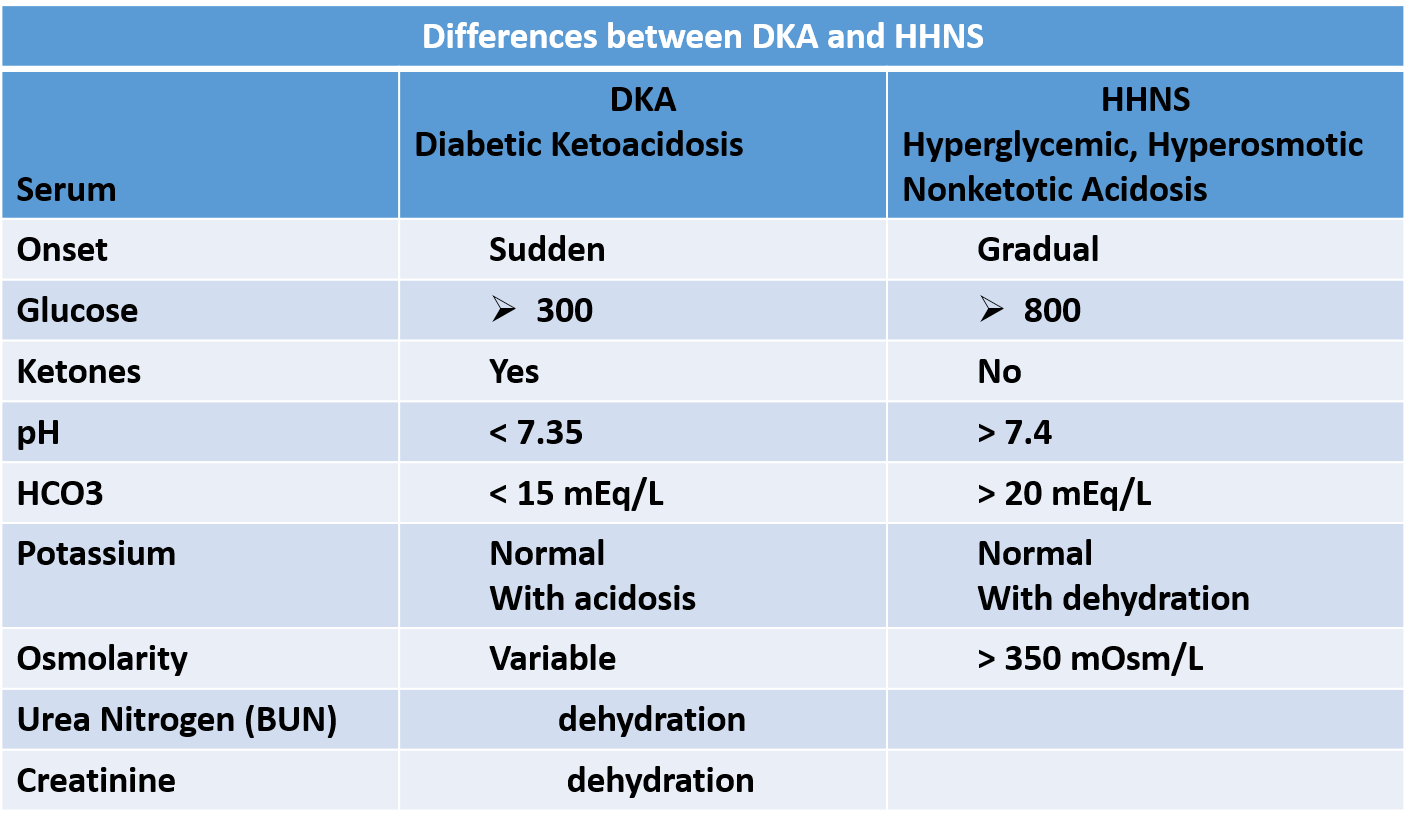
This image provides an overview of the underlying mechanisms and processes involved in developing gestational diabetes mellitus. TNF: Tumor necrosis factor; IL: Interleukin; ATM: Adipose tissue macrophages. - Diabetic Ketoacidosis
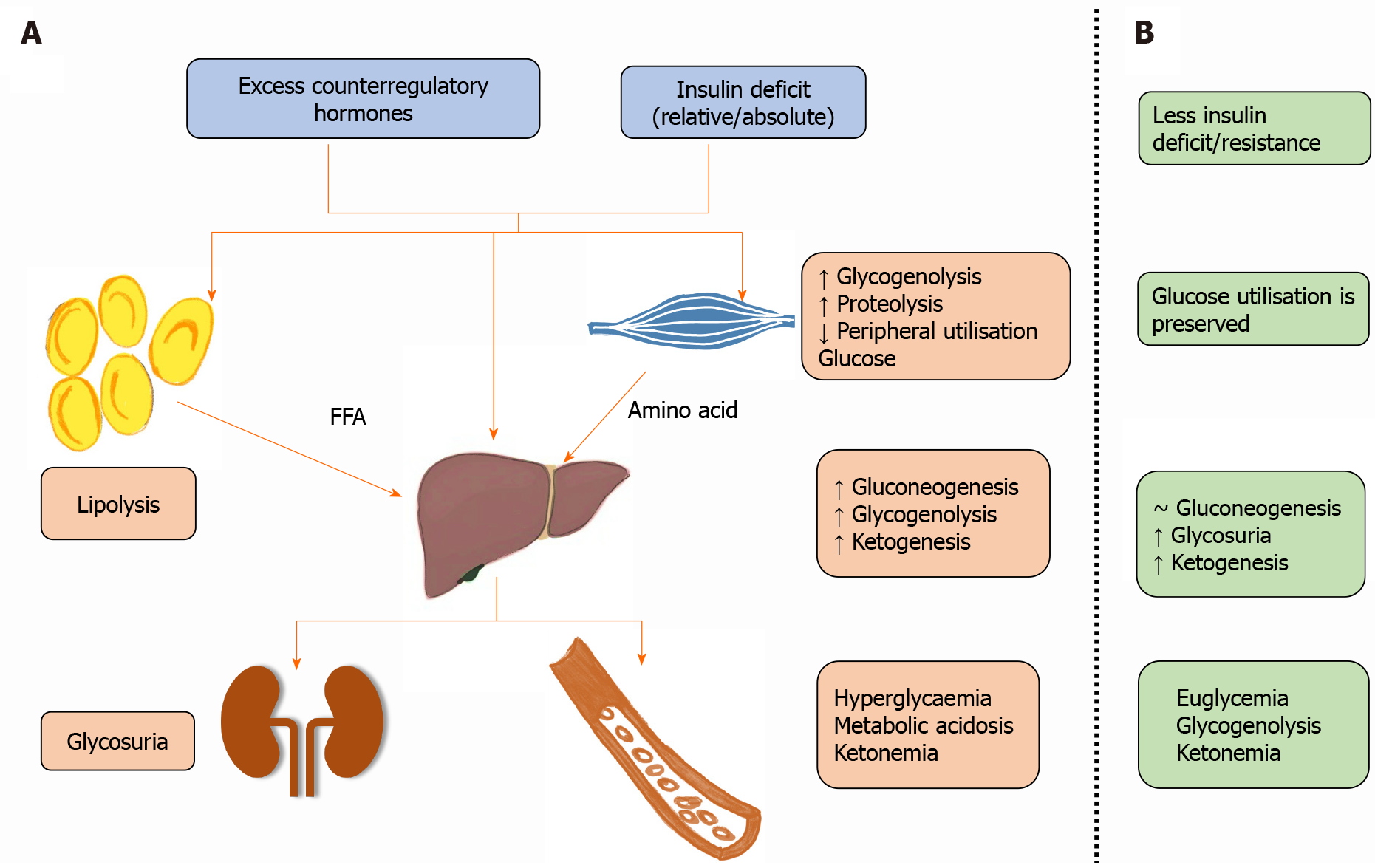
Ketone bodies (beta-hydroxybutyrate, acetoacetate, and acetone) are responsible for metabolic acidosis, while hyperglycemia through glycosuria and osmotic diuresis causes dehydration and hypovolemia. A: Pathophysiology of diabetic ketoacidosis; B: Pathophysiology of euglycemic diabetic ketoacidosis. FFA: Free fatty acids; ↑: Increase; ↓: Decrease; ~: No change. 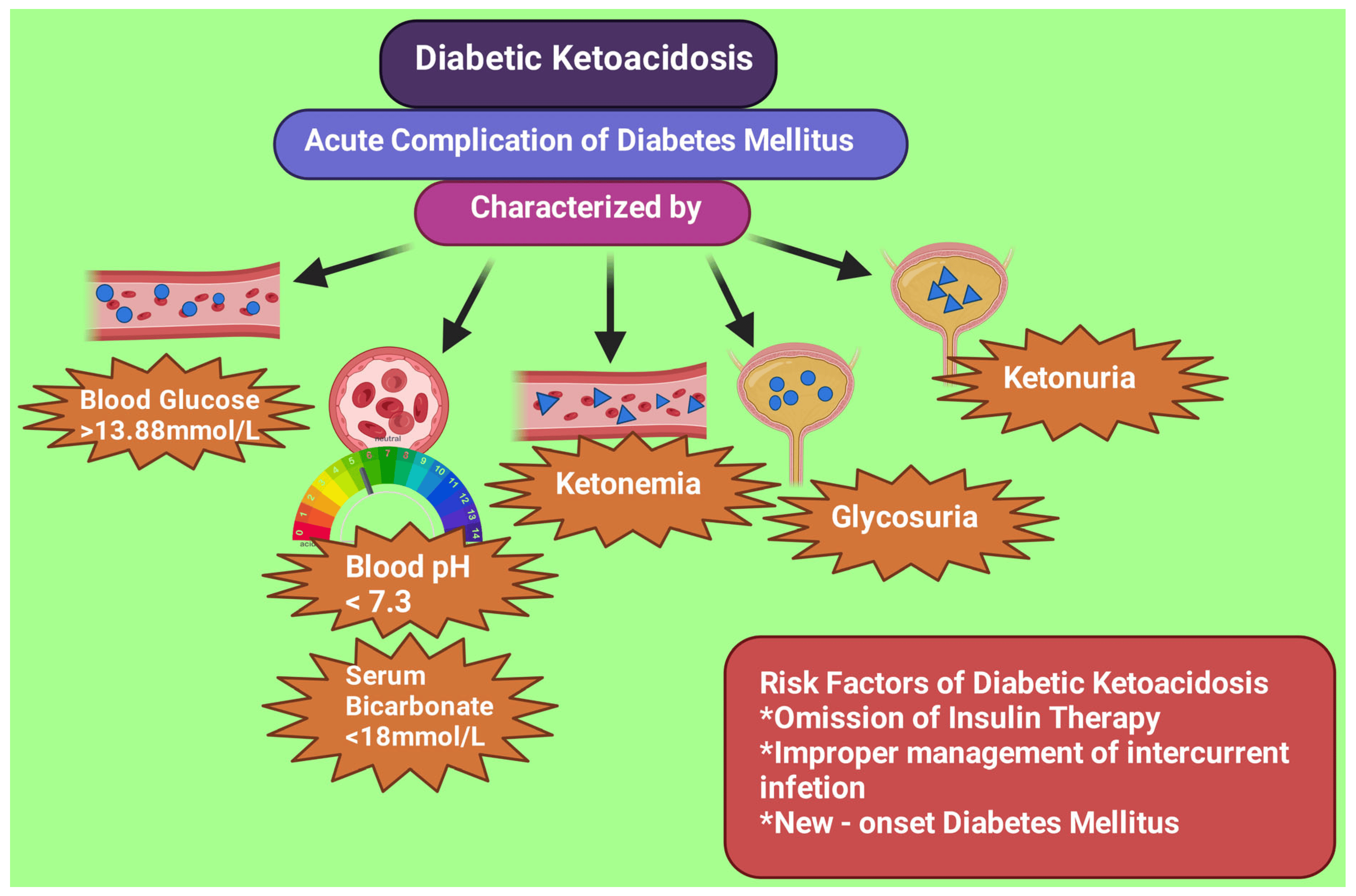
Biochemical characteristics and risk factors of diabetic ketoacidosis. - Insulin/Hypoglycemic Shock
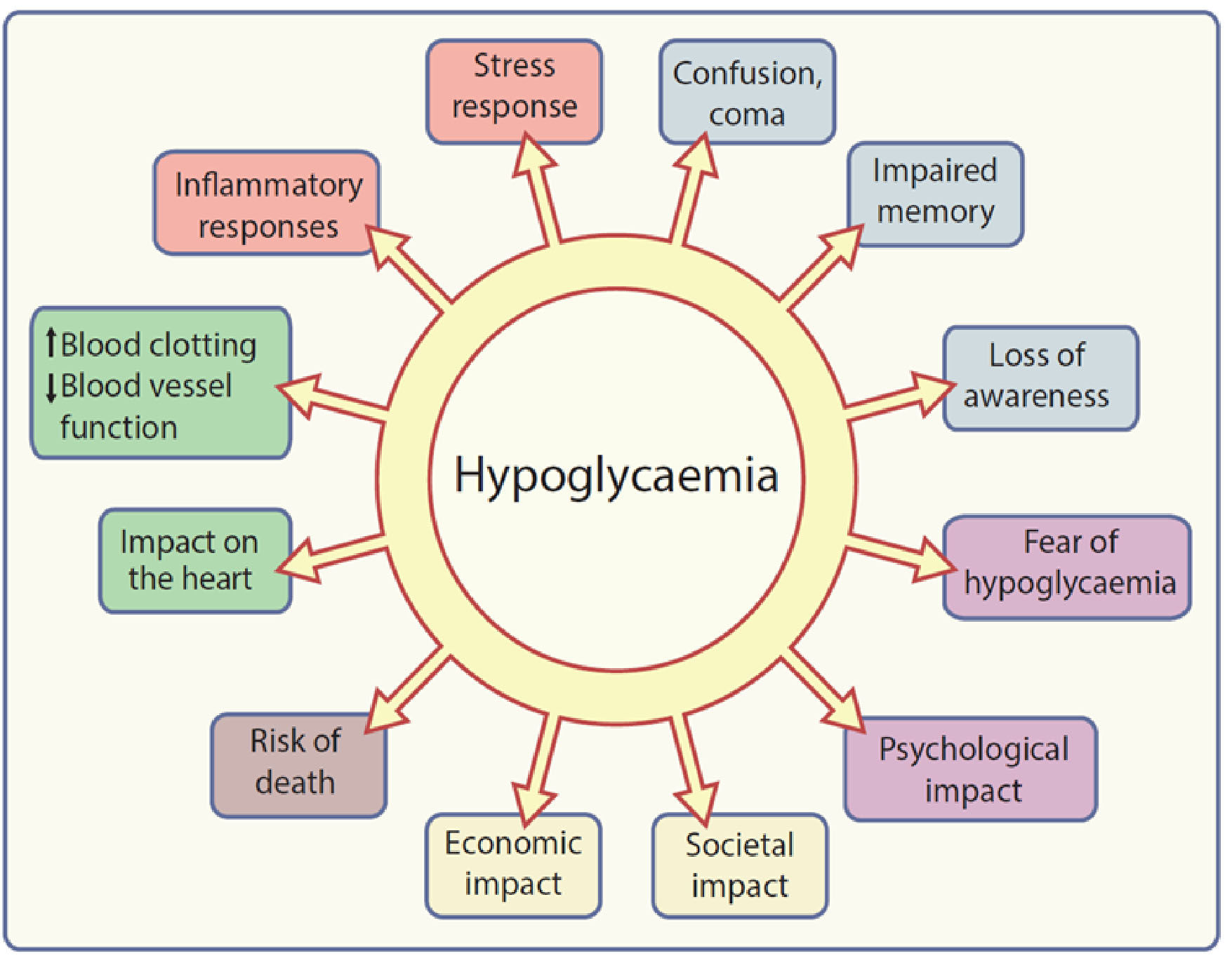
graphical summary of the potential consequences of hypoglycaemia. Elements of the stress response to a hypoglycaemic episode are shown in orange text boxes; other colours indicate different classes of possible consequences of hypoglycaemic episodes and of hypoglycaemia itself (blue, neurological/cognitive; purple, psychological; yellow, socioeconomic; brown, mortality; green, cardiovascular). 

The putative neural mechanism of hypoglycemic and sympathoinhibitory responses to acupuncture. GABA, γ-aminobutyric acid; 5HT, 5- hydroxytryptamine or serotonin; NO, nitric oxide; IML, intermediolateral column of the spinal cord; DM, diabetes mellitus. - Hyperglycemic, Hyperosmotic Nonketotic Acidosis/Coma (HHNK)
- Chronic Complications of Diabetes
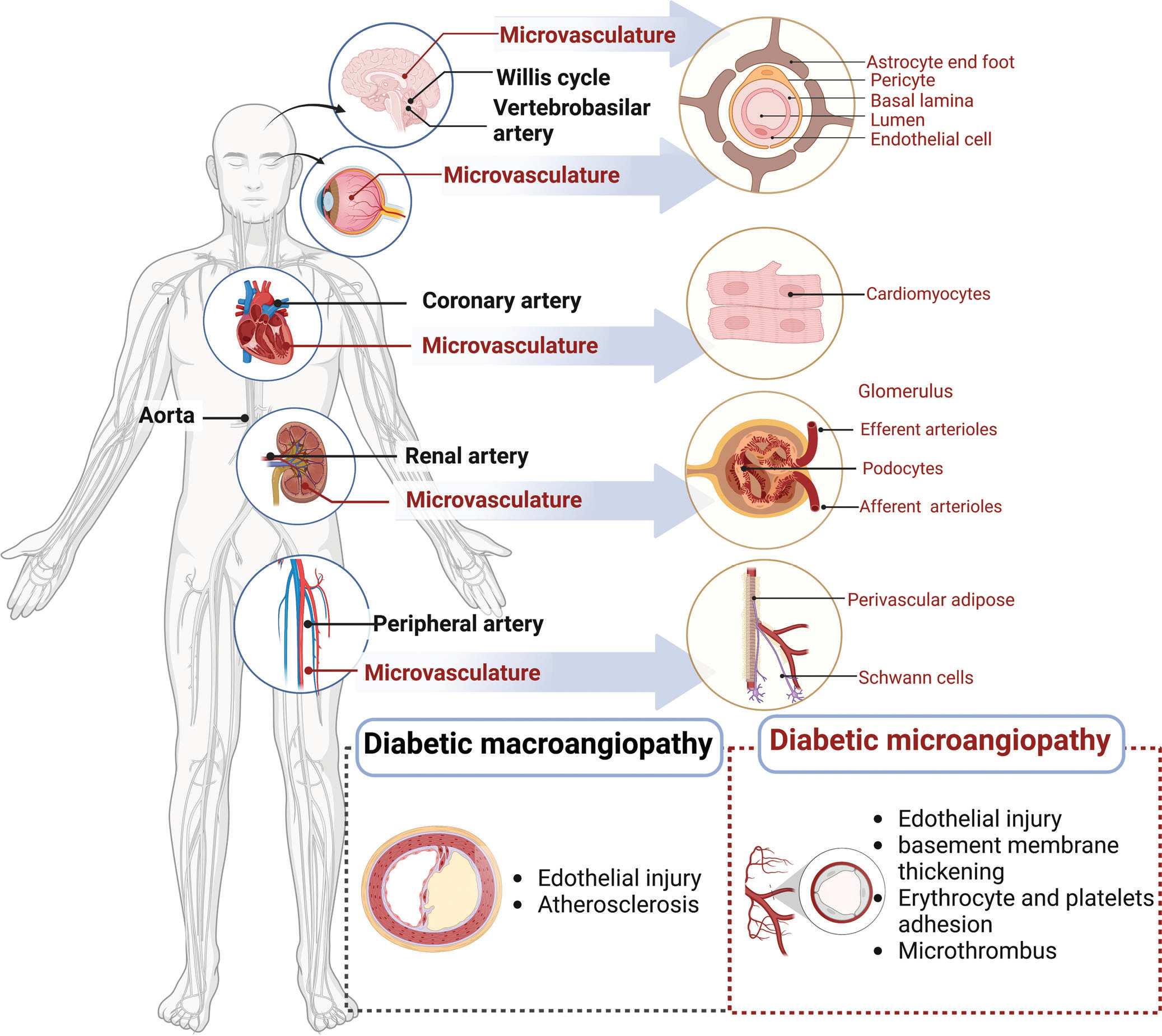
Diabetic vascular diseases. Schematic overview of panvasculopathy in diabetes mellitus. Diabetic panvasculopathy involves the cardiac, cerebral, renal, ophthalmic, and peripheral systems. The macrovascular lesions are in black text. The microvascular lesions are in red. The microvascular system varies in different organs, which affects vascular function - Atherosclerosis, Arteriosclerosis → Stroke
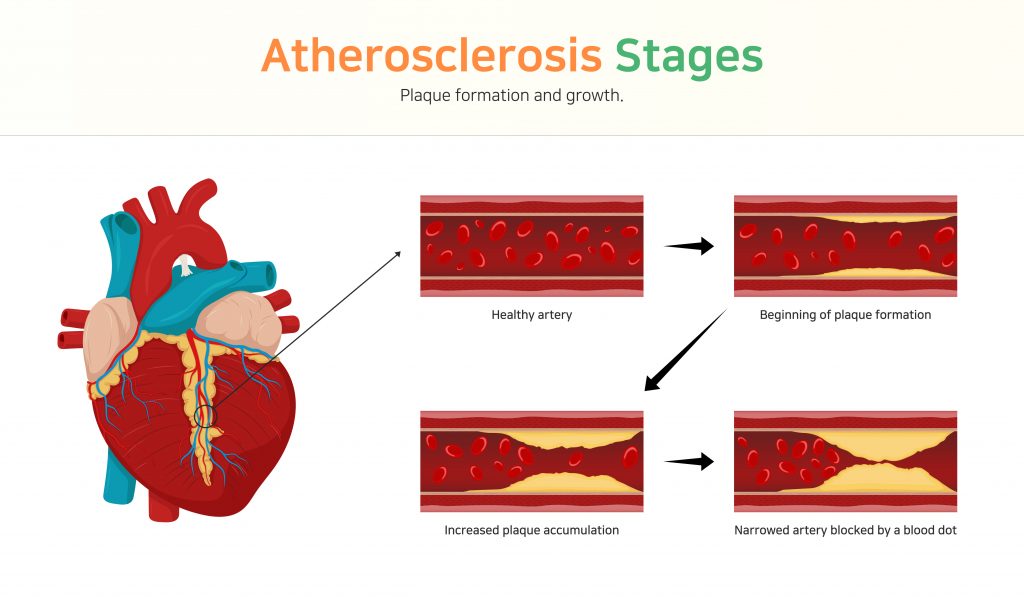
Stages of Atherosclerosis - Peripheral Artery Disease → gangrene

Gangrene Foot - Coronary Artery Disease → Myocardial Infarction
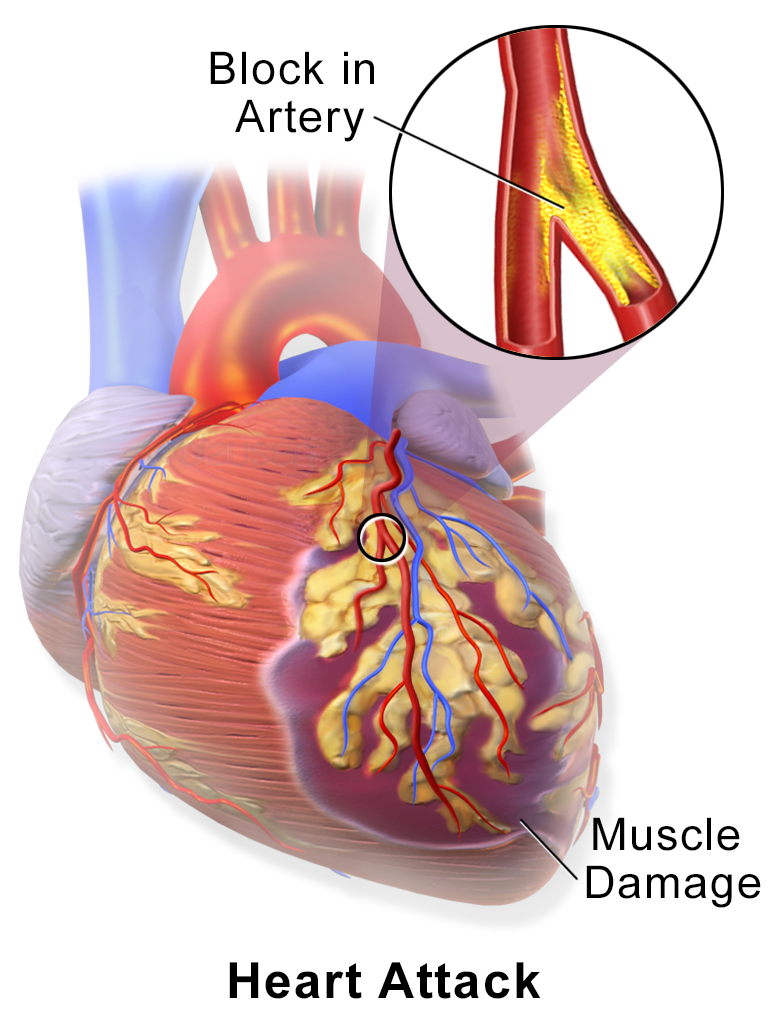
Myocardial Infarction or Heart Attack 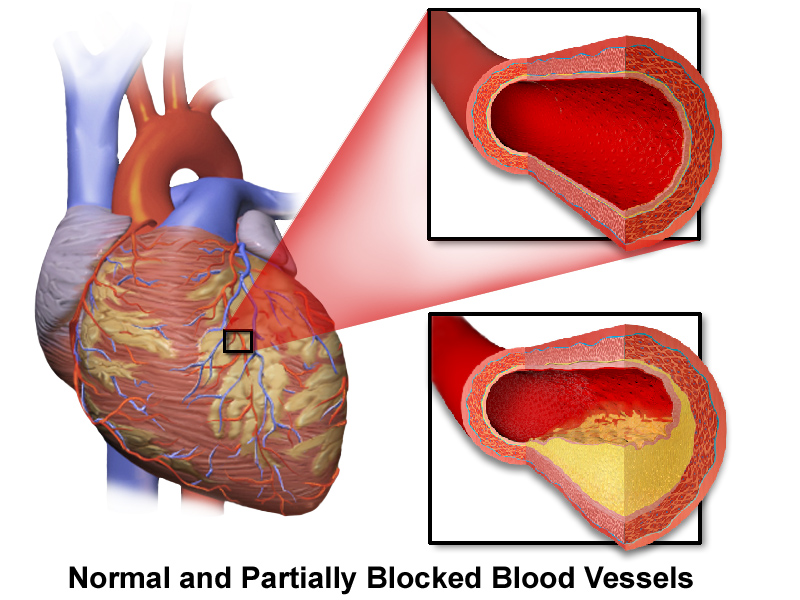
Coronary Artery Disease. Illustration of the heart with normal and partially-blocked vessels. 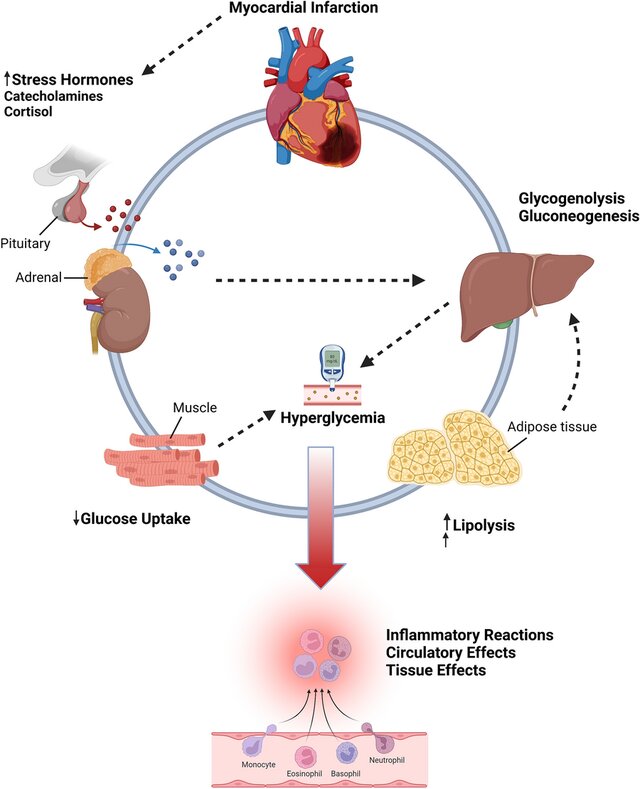
Cardiovascular effects of hyperglycemia during the acute phase of myocardial infarction
- Microangiopathy → Retinopathy, Tissue Necrosis, Neuropathy, Ischemia
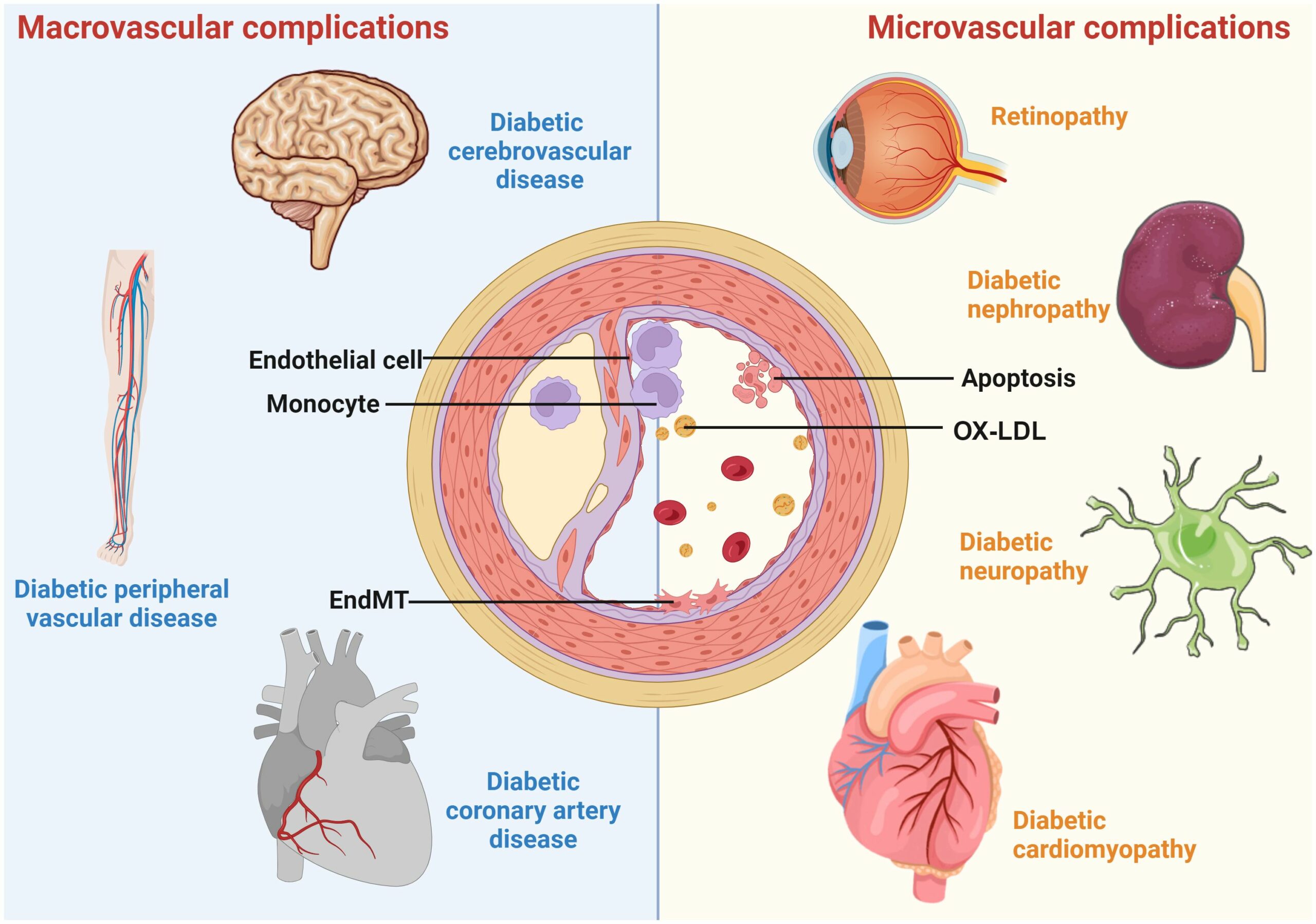
A schematic overview of diabetic vascular complications. Diabetic vascular complications include macrovascular complications (diabetic coronary artery disease, cerebrovascular disease, and peripheral vascular disease) and microvascular complications (diabetic retinopathy, nephropathy, cardiomyopathy, and neuropathy). Continued exposure to risk factors causes endothelial dysfunction, leading to lipid retention in the endothelium. Monocytes differentiate into macrophages, internalize modified lipoproteins, and form foam cells. Activated foam cells induce inflammation by secreting cytokines through several downstream signals. In addition, endothelial cells undergo EndMT, cell death, etc., further exacerbating the atherosclerotic process.
- Peripheral Artery Disease → gangrene
- Diabetic Macular Edema
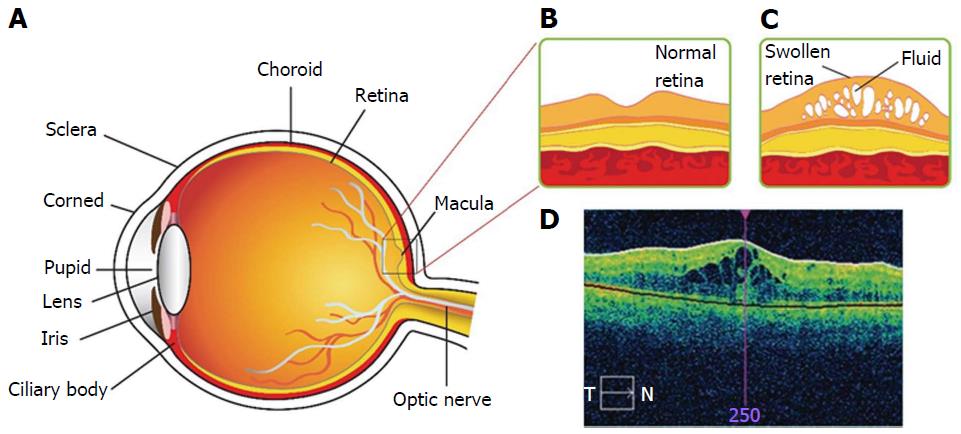
Diabetic macular edema. A: Structure of human eye; B: Expanded representation of macula region for normal eye; C: Expanded representation of macula region for diabetic macular edema (DME); D: Optical coherence tomography image for DME. - Diabetic Sugar Cataracts
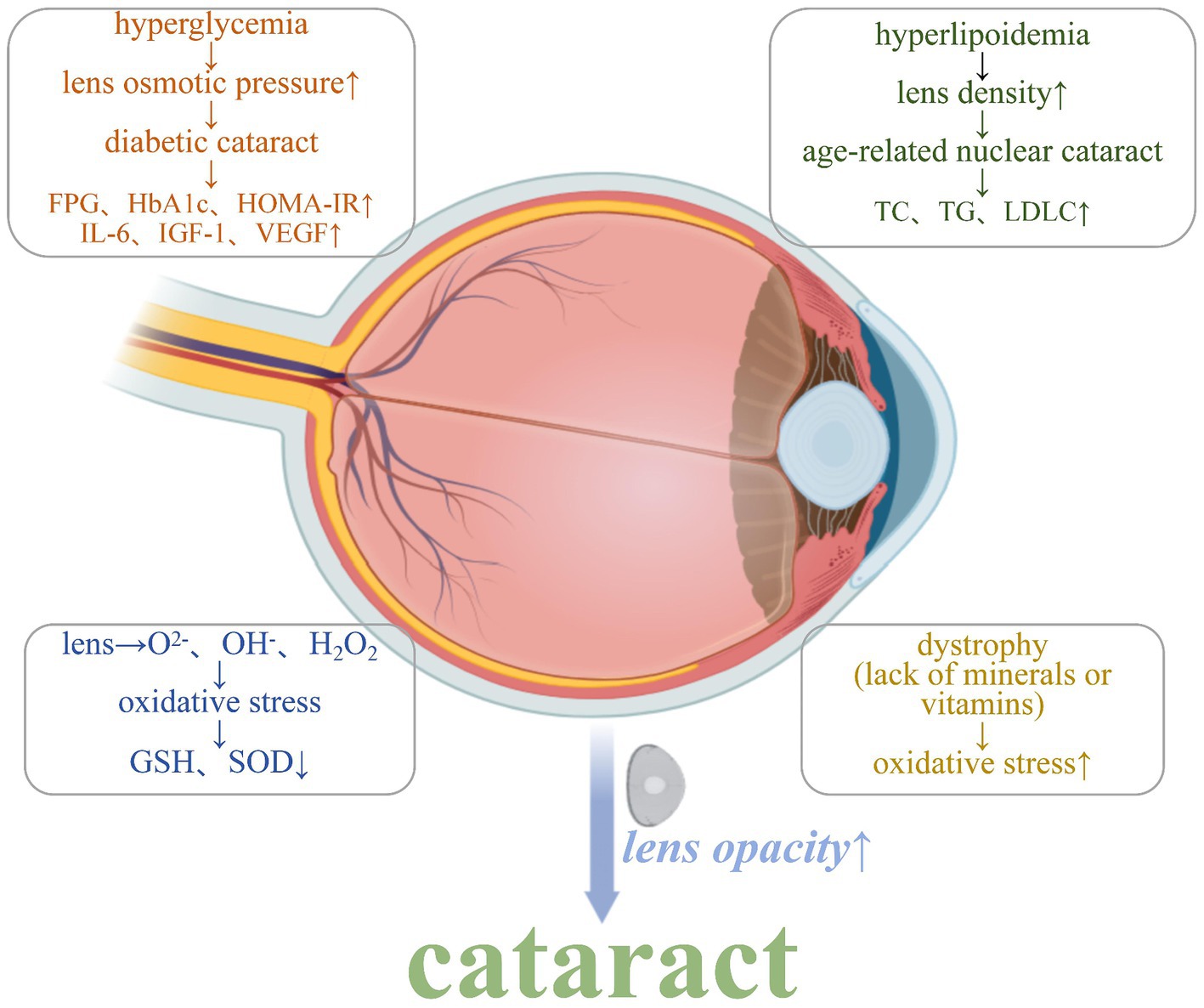
Mechanisms that induce cataract development. 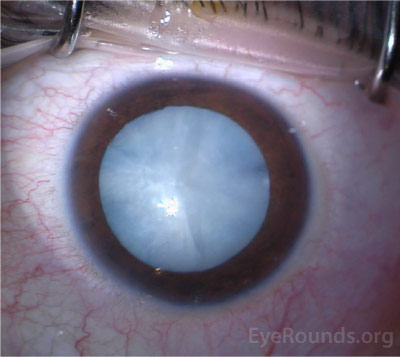
An image of the right eye captured from an intraoperative recording demonstrates the dense white cataract related to diabetes. - Diabetic NEphrosclerosis
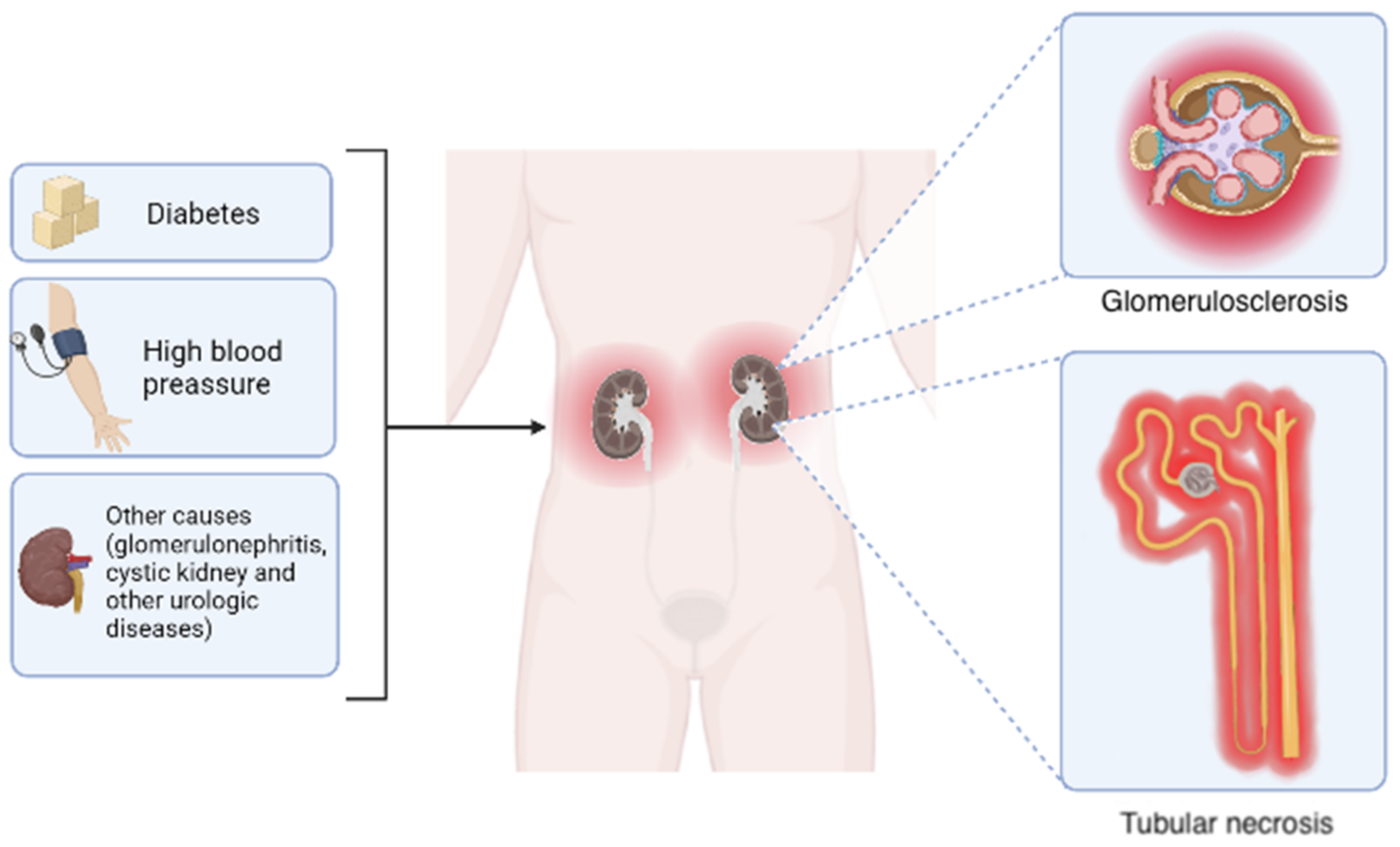
Primary causes and morphological outcomes of chronic kidney disease. Although the leading causes of chronic kidney disease include diabetes and hypertension, other disorders such as glomerulonephritis, cystic kidney disease, and diverse urologic diseases also contribute in a minor proportion. Regardless of the etiology, the progressive reduction in glomerular filtration rate occurs accompanied by two common histological changes: glomerular sclerosis and tubular necrosis. 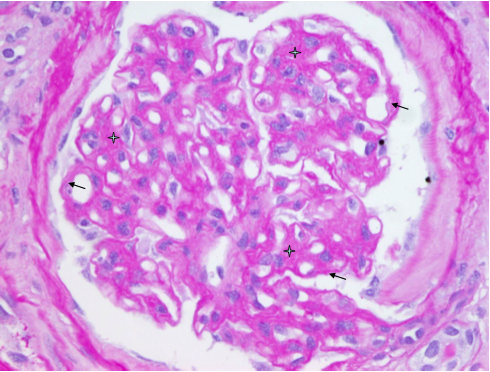
Diabetic nephropathy. Class II b diabetic nephropathy. Diffuse expansion of mesangium (star) and diffuse thickening of the glomerular basement membrane (arrow). PAS stain, X400. 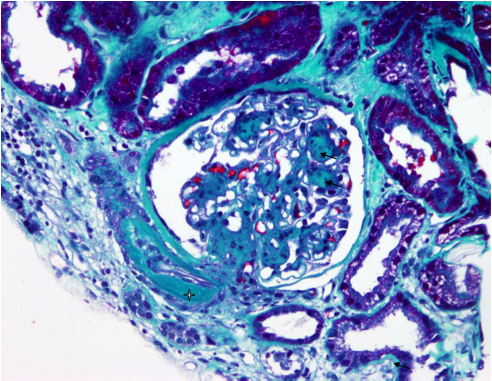
Diabetic nephropathy. Class III diabetic nephropathy. Sclerotic nodule (Kimmelstiel–Wilson) in nodular diabetic nephropathy (arrow). Mallory stain, X 100. 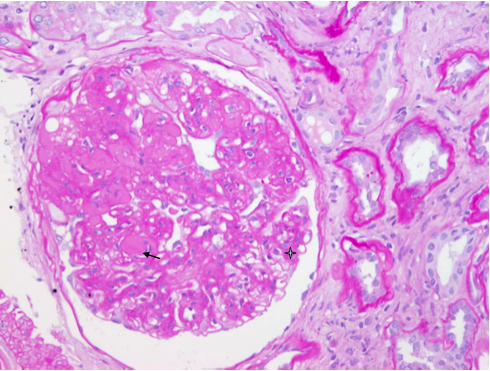
Diabetic nephropathy. Fibrin cap (arrow) is characteristic for diabetic nephropathy. It is caused by insudation and accumulation of glycosilated plasma proteins between the glomerular endothelium and the glomerular basement membrane. Diffuse expansion of mesangium is designated by four point star. PAS stain, X 200. - Hypertension
Hypertension (High Blood Pressure) 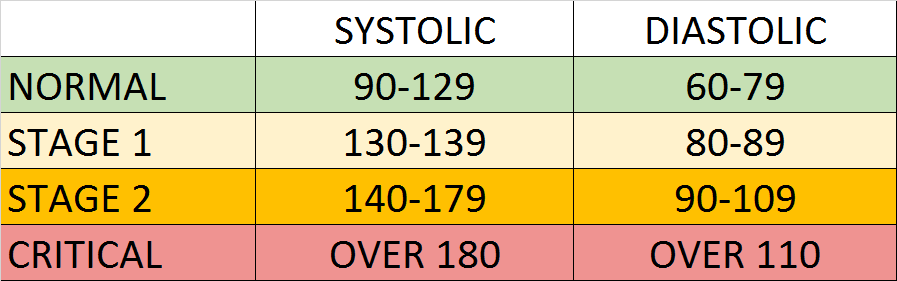
Hypertension ranges chart 
grade 2 arterial hypertension - Congestive Heart Failure
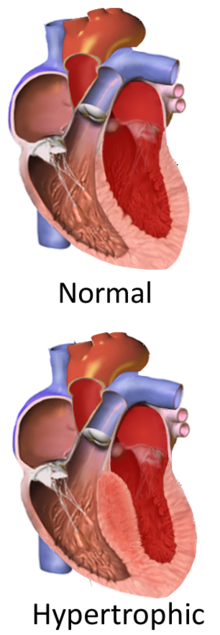
congestive heart Vs Normal Heart. Thickened ventricular septum - Urinary Tract Infections
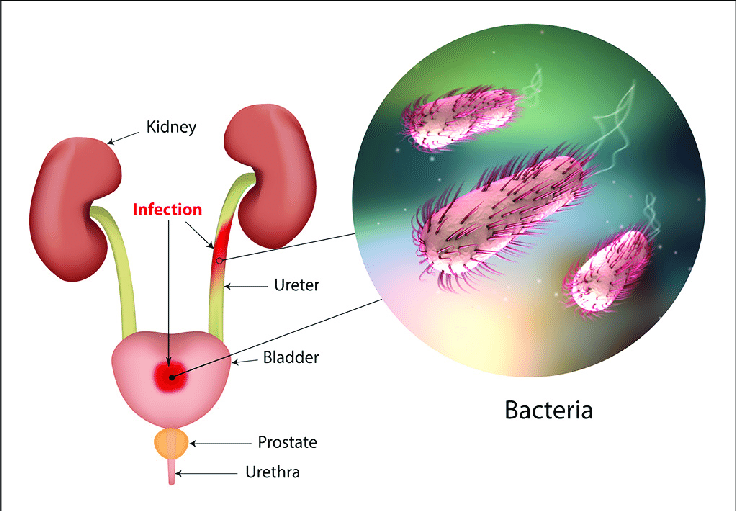
The urinary tract and sites of infection. - Gingivitis,

Gingivitis. Gingivitis before (top) and after (bottom) a thorough mechanical debridement of the teeth. - Foot ulcers
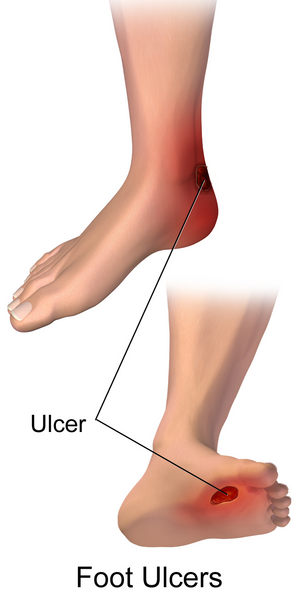
Diabetes Foot Ulcers - Fungal infections

Human tongue infected with oral candidiasis - Bladder incontinence, impotence
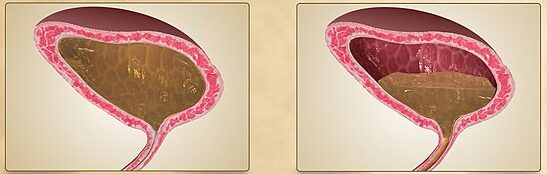
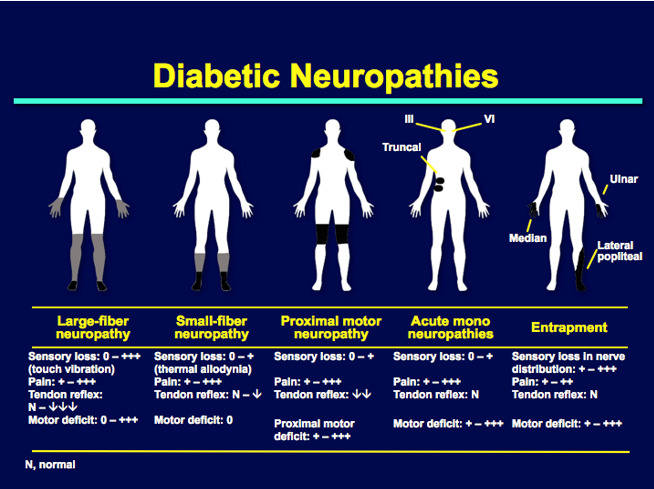
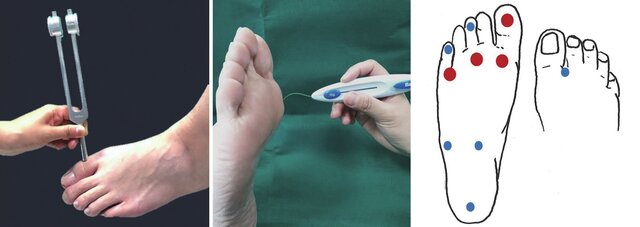
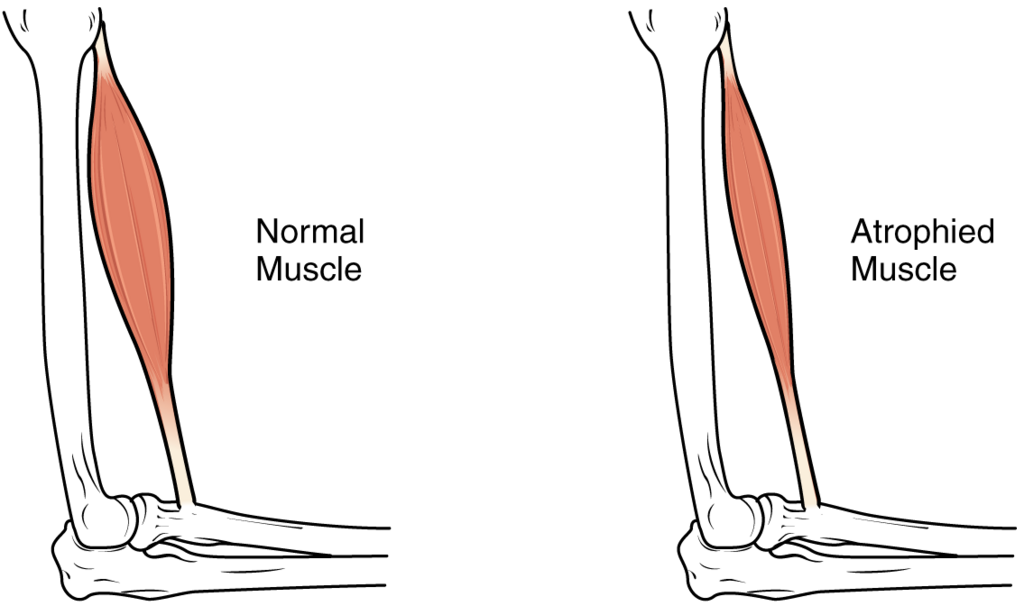
normal urinary bladder(L) and overactive urinary bladder(R). - Decreased senssation, muscle wasting
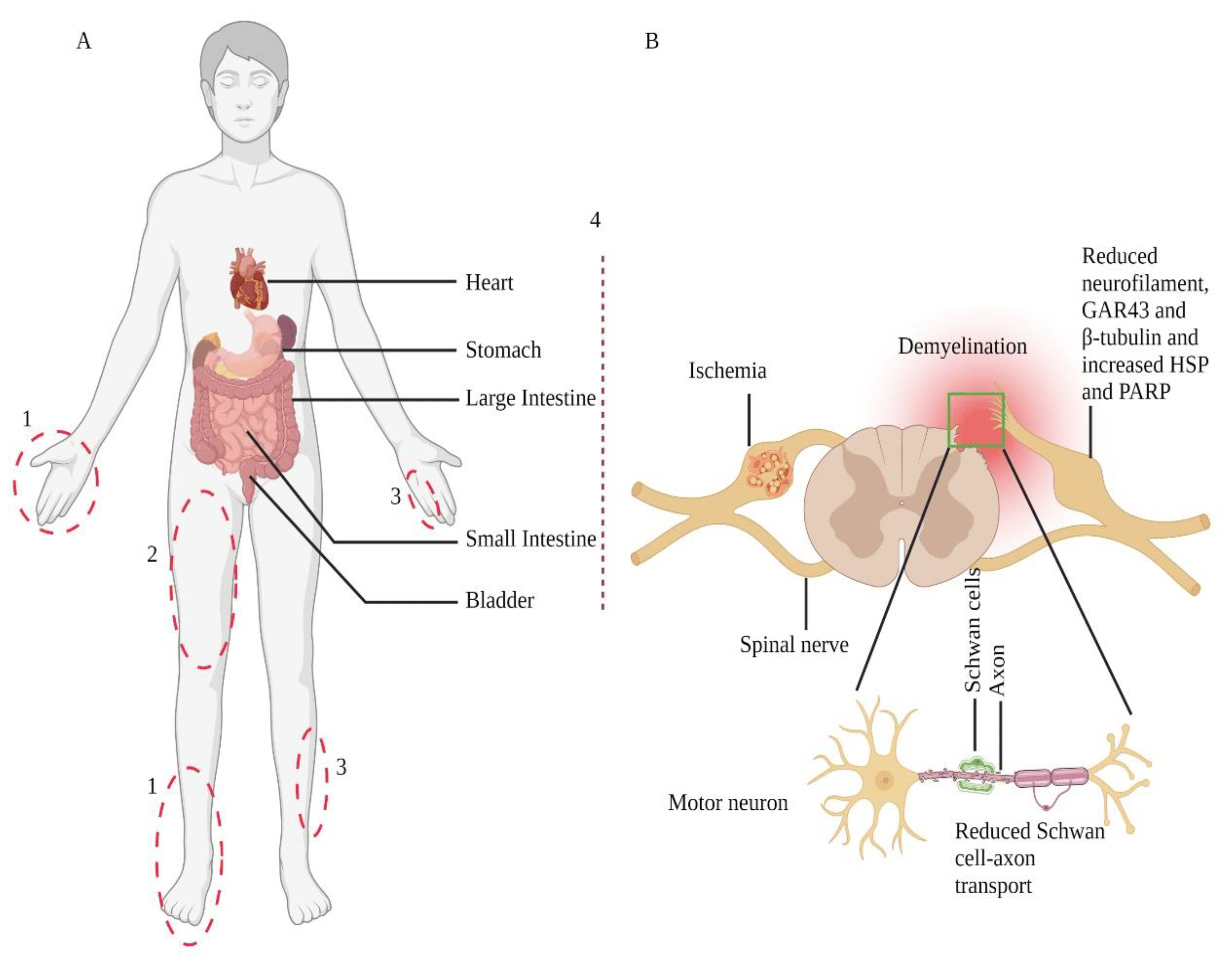
Nerve injury-prone areas and alteration of the peripheral nervous system in diabetic neuropathy. Diabetic neuropathy primarily affects distal sensory systems (1), eventually causing radiculopathy (2), mononeuropathy (3), and autonomic neuropathy or treatment-induced neuropathy (4) (part A). Sensory neurons transmit their terminal information from the periphery to the dorsal horn of the spinal cord (part B); contrarily, spinal cord-residing motor neurons relay information to the periphery. The Schwan cells myelinate axons and play a crucial role in preserving axonal functions. Therefore, in response to cellular injuries, such as diabetes, damaged Schwan cells or axons lead to neuronal cell body damage. These changes also include Schwan cell-axon transport, change in protein expression, demyelination, and degeneration.
- Atherosclerosis, Arteriosclerosis → Stroke
Media Attributions
- The-normal-synchronous-relationships-between-sleep-and-daytime-activity-and-cortisol
- Antibody © Fvasconcellos is licensed under a Public Domain license
- Paracetamol_acetaminophen_500_mg_pills © Michelle Tribe is licensed under a CC BY (Attribution) license
- Macrophages_and_helper_T-cells © Abutler05 adapted by Portiaa McGonigal is licensed under a CC BY-SA (Attribution ShareAlike) license
- NeutrophilerAktion.svg © Mario Schubert is licensed under a Public Domain license
- Dendritic_cell
- Mast_cells
- Cancer_progression_from_NIH
- Metastasis
- Metaplasia, Dysplasia Lung © Ashraf-Uz-Zaman, M.; Bhalerao, A.; Mikelis, C.M.; Cucullo, L.; German, N.A. is licensed under a CC BY-SA (Attribution ShareAlike) license
- Equipment_-_Endoscopy_-_Smart-Servier
- Histology_Lab © Baitaal is licensed under a CC BY-SA (Attribution ShareAlike) license
- cytokines © National Institute of Allergy and Infectious Disease adapted by Portiaa McGonigal is licensed under a CC BY (Attribution) license
- Killer_T_cells

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}