1103 Chapter 11. The Muscular System
11.4 Axial Muscles of the Abdominal Wall, and Thorax
Learning Objectives
By the end of this section, you will be able to:
It is a complex job to balance the body on two feet and walk upright. The muscles of the vertebral column, thorax, and abdominal wall extend, flex, and stabilize different parts of the body’s trunk. The deep muscles of the core of the body help maintain posture as well as carry out other functions. The brain sends out electrical impulses to these various muscle groups to control posture by alternate contraction and relaxation. This is necessary so that no single muscle group becomes fatigued too quickly. If any one group fails to function, body posture will be compromised.
Muscles of the Abdomen
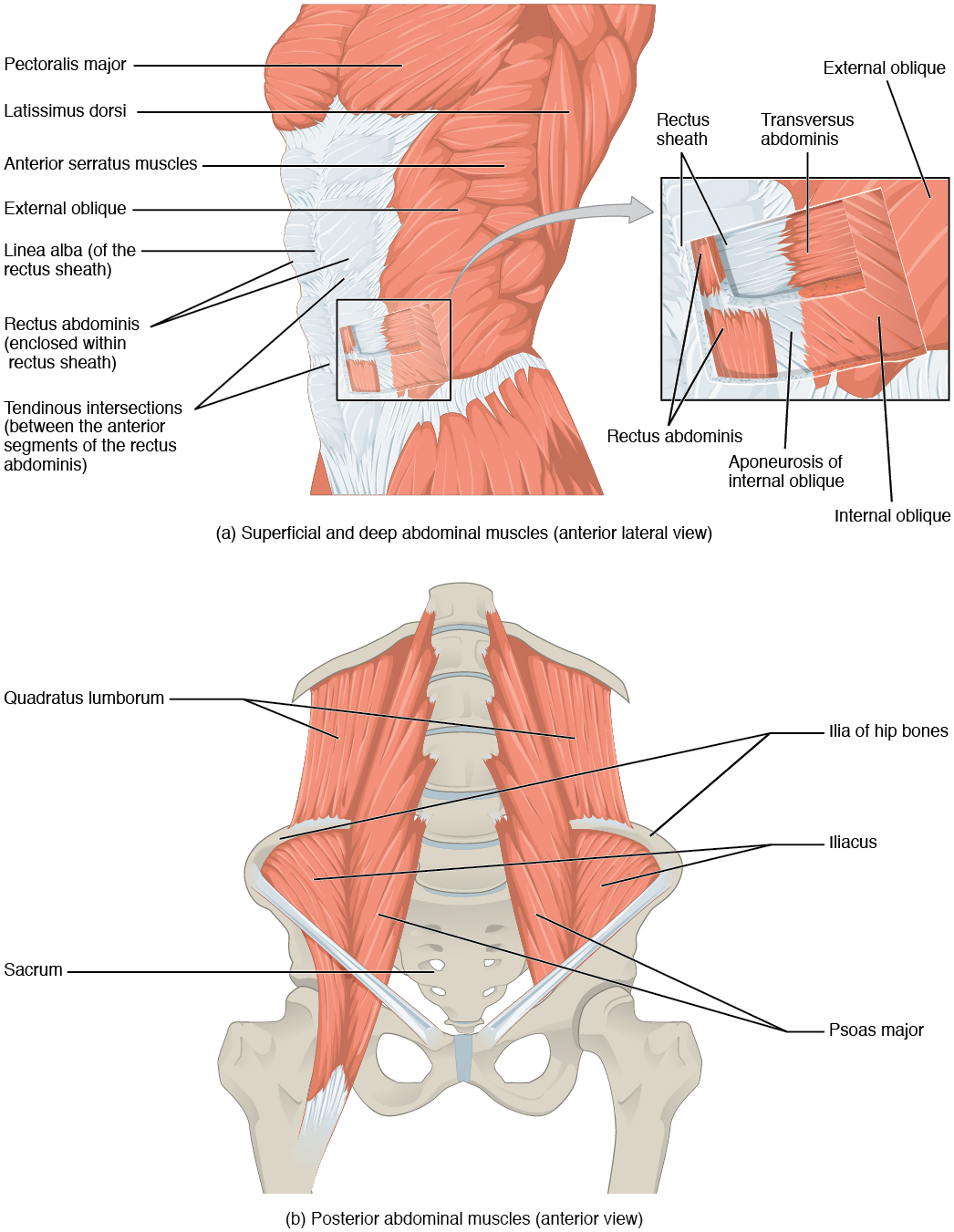
There are four pairs of abdominal muscles that cover the anterior and lateral abdominal region and meet at the anterior midline. These muscles of the anterolateral abdominal wall can be divided into four groups: the external obliques, the internal obliques, the transversus abdominis, and the rectus abdominis (Figure 1 and Table 6).
| Muscles of the Abdomen (Table 6) | |||||
|---|---|---|---|---|---|
| Movement | Target | Target motion direction | Prime mover | Origin | Insertion |
| Twisting at waist; also bending to the side | Vertebral column | Supination; lateral flexion | External obliques; internal obliques | Ribs 5–12; ilium | Ribs 7–10; linea alba; ilium |
| Squeezing abdomen during forceful exhalations, defecation, urination, and childbirth | Abdominal cavity | Compression | Transversus abdominus | Ilium; ribs 5–10 | Sternum; linea alba; pubis |
| Sitting up | Vertebral column | Flexion | Rectus abdominis | Pubis | Sternum; ribs 5 and 7 |
| Bending to the side | Vertebral column | Lateral flexion | Quadratus lumborum | Ilium; ribs 5–10 | Rib 12; vertebrae L1–L4 |
There are three flat skeletal muscles in the antero-lateral wall of the abdomen. The external oblique, closest to the surface, extend inferiorly and medially, in the direction of sliding one’s four fingers into pants pockets. Perpendicular to it is the intermediate internal oblique, extending superiorly and medially, the direction the thumbs usually go when the other fingers are in the pants pocket. The deep muscle, the transversus abdominis, is arranged transversely around the abdomen, similar to the front of a belt on a pair of pants. This arrangement of three bands of muscles in different orientations allows various movements and rotations of the trunk. The three layers of muscle also help to protect the internal abdominal organs in an area where there is no bone.
The linea alba is a white, fibrous band that is made of the bilateral rectus sheaths that join at the anterior midline of the body. These enclose the rectus abdominis muscles (a pair of long, linear muscles, commonly called the “sit-up” muscles) that originate at the pubic crest and symphysis, and extend the length of the body’s trunk. Each muscle is segmented by three transverse bands of collagen fibers called the tendinous intersections. This results in the look of “six-pack abs,” as each segment hypertrophies on individuals at the gym who do many sit-ups.
The posterior abdominal wall is formed by the lumbar vertebrae, parts of the ilia of the hip bones, psoas major and iliacus muscles, and quadratus lumborum muscle. This part of the core plays a key role in stabilizing the rest of the body and maintaining posture.
Muscles of the Thorax
The muscles of the chest serve to facilitate breathing by changing the size of the thoracic cavity (Table 7). When you inhale, your chest rises because the cavity expands. Alternately, when you exhale, your chest falls because the thoracic cavity decreases in size.
| Muscles of the Thorax (Table 7) | |||||
|---|---|---|---|---|---|
| Movement | Target | Target motion direction | Prime mover | Origin | Insertion |
| Inhalation; exhalation | Thoracic cavity | Compression; expansion | Diaphragm | Sternum; ribs 6–12; lumbar vertebrae | Central tendon |
| Inhalation;exhalation | Ribs | Elevation (expands thoracic cavity) | External intercostals | Rib superior to each intercostal muscle | Rib inferior to each intercostal muscle |
| Forced exhalation | Ribs | Movement along superior/inferior axis to bring ribs closer together | Internal intercostals | Rib inferior to each intercostal muscle | Rib superior to each intercostal muscle |
The Diaphragm
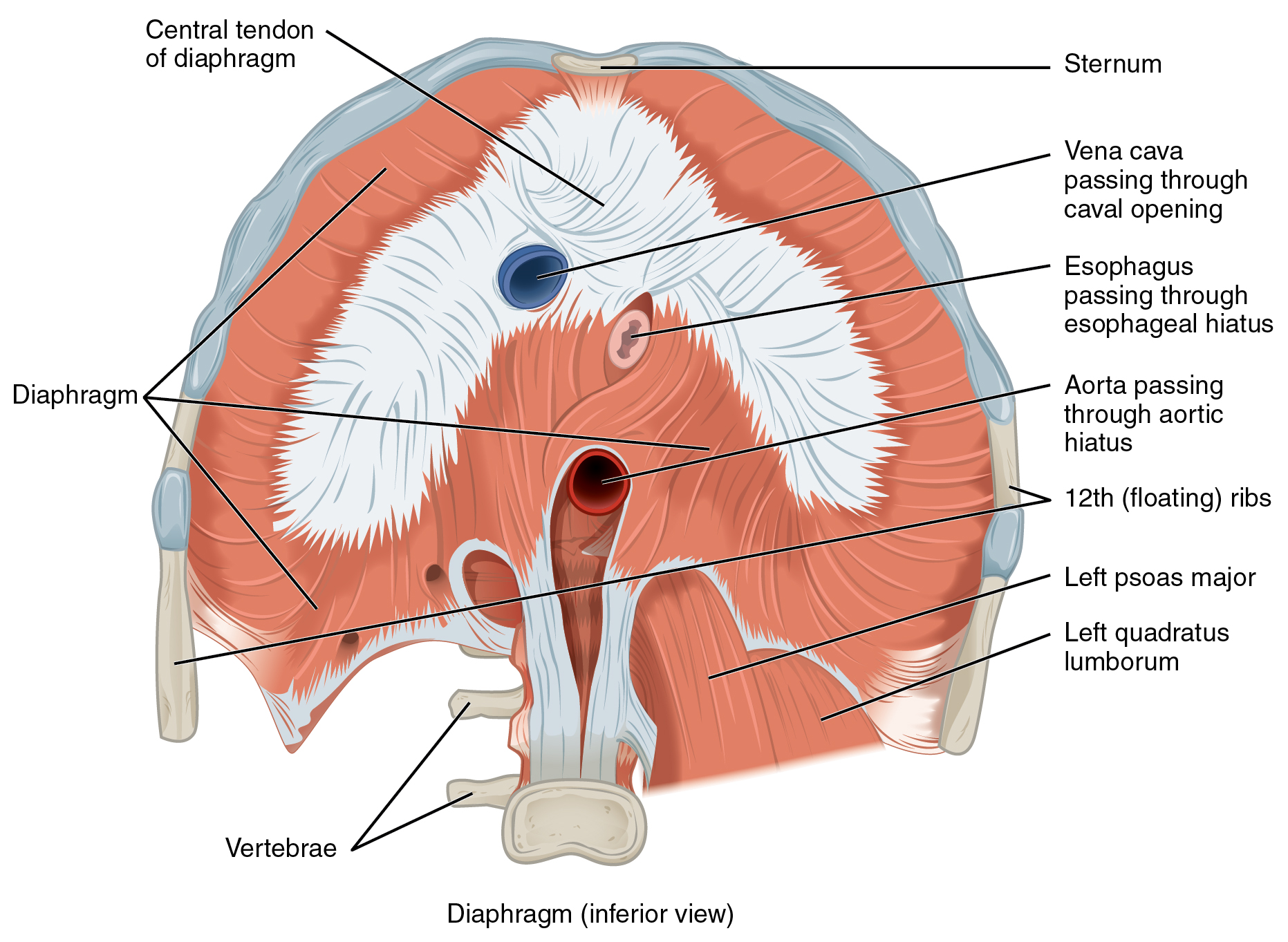
The change in volume of the thoracic cavity during breathing is due to the alternate contraction and relaxation of the diaphragm (Figure 2). It separates the thoracic and abdominal cavities, and is dome-shaped at rest. The superior surface of the diaphragm is convex, creating the elevated floor of the thoracic cavity. The inferior surface is concave, creating the curved roof of the abdominal cavity.
Defecating, urination, and even childbirth involve cooperation between the diaphragm and abdominal muscles (this cooperation is referred to as the “Valsalva maneuver”). You hold your breath by a steady contraction of the diaphragm; this stabilizes the volume and pressure of the peritoneal cavity. When the abdominal muscles contract, the pressure cannot push the diaphragm up, so it increases pressure on the intestinal tract (defecation), urinary tract (urination), or reproductive tract (childbirth).
The inferior surface of the pericardial sac and the inferior surfaces of the pleural membranes (parietal pleura) fuse onto the central tendon of the diaphragm. To the sides of the tendon are the skeletal muscle portions of the diaphragm, which insert into the tendon while having a number of origins including the xiphoid process of the sternum anteriorly, the inferior six ribs and their cartilages laterally, and the lumbar vertebrae and 12th ribs posteriorly.
The diaphragm also includes three openings for the passage of structures between the thorax and the abdomen. The inferior vena cava passes through the caval opening, and the esophagus and attached nerves pass through the esophageal hiatus. The aorta, thoracic duct, and azygous vein pass through the aortic hiatus of the posterior diaphragm.
The Intercostal Muscles
There are three sets of muscles, called intercostal muscles, which span each of the intercostal spaces. The principal role of the intercostal muscles is to assist in breathing by changing the dimensions of the rib cage (Figure 3).
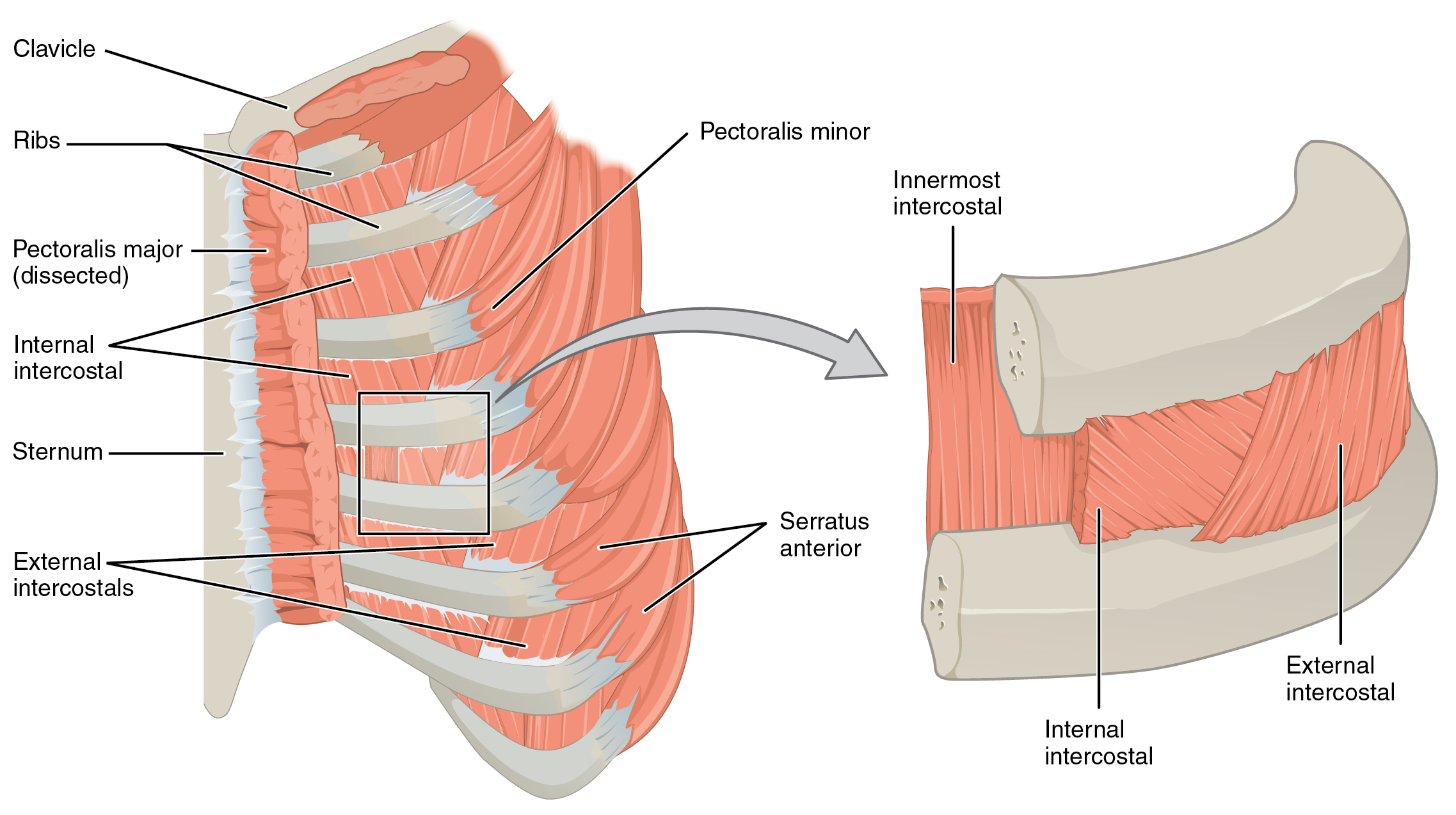
The 11 pairs of superficial external intercostal muscles aid in inspiration of air during breathing because when they contract, they raise the rib cage, which expands it. The 11 pairs of internal intercostal muscles, just under the externals, are used for expiration because they draw the ribs together to constrict the rib cage. The innermost intercostal muscles are the deepest, and they act as synergists for the action of the internal intercostals.
