Evaluating Community Risks & Strengthening Emergency Preparedness
What is Emergency Preparedness?
According to the World Health Organization (WHO), the aim of emergency preparedness is to “strengthen the capacity of governments, organizations, institutions and communities to withstand a disaster or emergency situation.”17 This includes natural hazards and infectious disease outbreaks including COVID-19. Adequate emergency preparedness enhances resilience against climate change-driven environmental disruptions and mitigates the health impacts for BC’s rural population which makes up about 17.8% of the total population.2,18,19
Climate Change-Driven Natural Disasters in Rural British Columbia
Identifying the likelihood and severity of natural disasters is a fundamental step to emergency preparedness. This entails community- and region-specific risk assessments based on geographic data.20 For example, the Canadian Centre for Climate Modelling and Analysis Regional Climate Model (CanRCM4) is a tool that illustrates regional climate projections analysis for mitigation and adaptation planning.21 Based on geographical characteristics of BC, some of the most prominent threats include forest fires and floods, which is why they are recursed to several times as examples throughout this learning hub.
Forest Fires

Forest fires are expected to increase in frequency and severity across BC. Land area burned from the record-breaking 2017 wildfire season was 40% greater than the previous record in 1958, with approximately 65,000 people evacuated and many more exposed to the hazardous smoke.22,23 Environment and Climate Change Canada and the University of Victoria jointly reported that anthropogenic climate change amplifies the risk of wildfires in BC and increases burned areas by 7 to 11 times. With progressing climate change, it is predicted that wildfires will continue to intensify. In 2018, more than 1.3 million hectares of land were destroyed, immediately surpassing 2017’s record.22,24
Forest fires can have both short- and long-term health consequences, such as inflammation of the respiratory system, impaired lung development in children, and psychiatric disorders.25 Simultaneous presentation of these health conditions can put significant pressure on local health care providers. The increasing incidence and associated costs therefore make wildfire management an important aspect of health services adaptation.22
The City of Rossland, which is located in the Kootenay Rockies Region, is vulnerable to wildfires, especially during dry summers. This community has received $255,000 through the Fall 2019 Community Innovation Grant by the Columbia Basin Trust to expand public education on forest fires, including training community leaders and hosting FireSmart events, for the FireSmart Community Recognition Program.26,27 FireSmart BC is based on the national FireSmart program to build wildfire resilience through seven main disciplines, such as education, emergency planning, and interagency cooperation.28,29 An increasing number of BC’s communities are now being recognized as FireSmart, with more than 20 added in 2019 alone.30
Floods
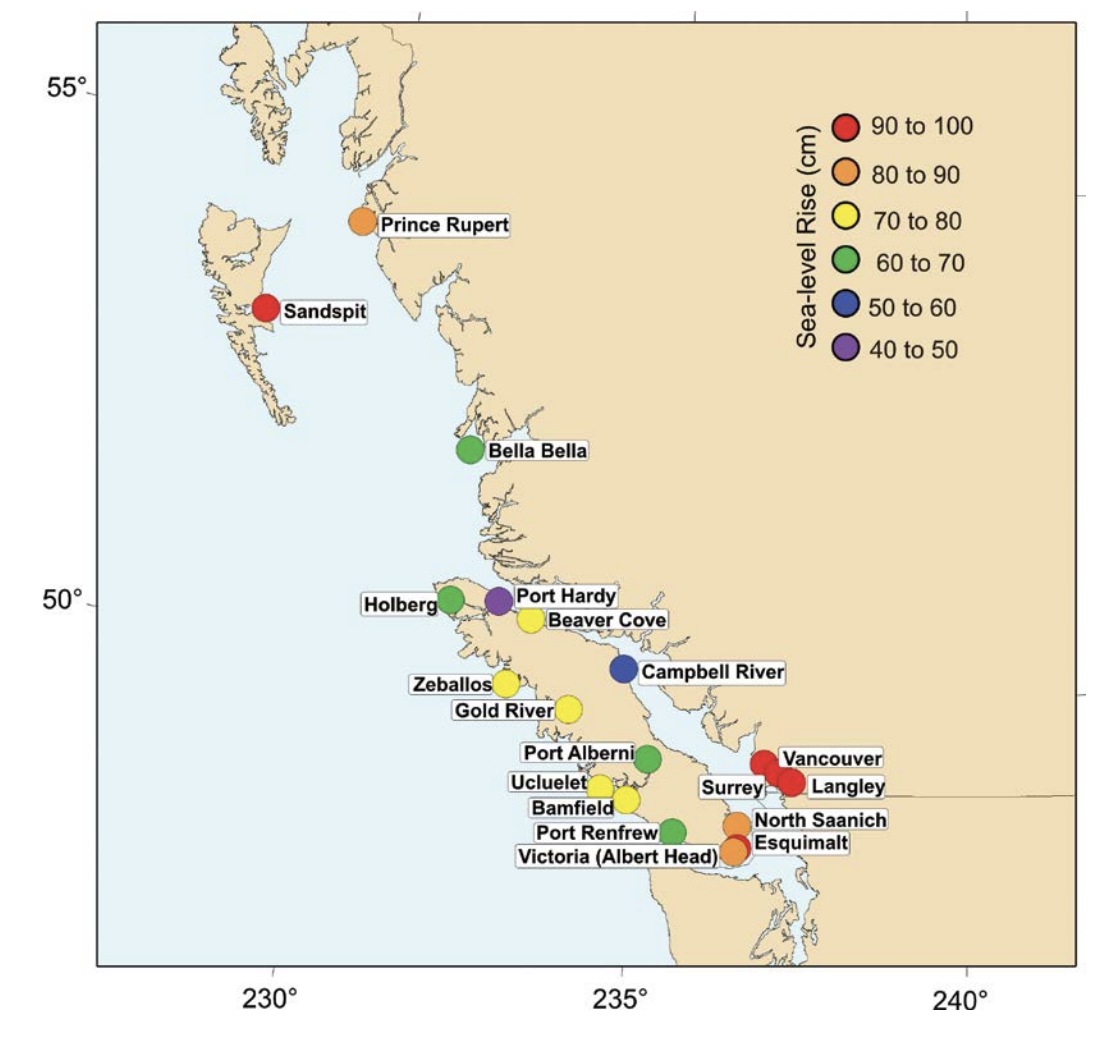
coast of B.C. by the year 2100. Natural
Resources Canada (2016).
In addition, coastal regions face increased risk of storm surges and floods, as BC contains more than 27,200 km of shoreline on the Pacific Ocean. This poses the threat of immediate environmental and health emergencies in affected rural communities.31 To aid in flood preparations based on detailed, region-specific information, Natural Resource Canada provides CanCoast which is an ArcGIS geospatial database for coastal hazard risk analysis and adaptation planning. It combines factors such as sea level, wave height, and ground ice content to derive coastal sensitivities in the face of climate change.31,32
The City of Courtenay in the Comox Valley District is located on Vancouver Island, and floods are Courtenay’s main climate vulnerability. This rural community has developed independent risk assessment and management strategies, such as the Integrated Rainwater Management Plan for stormwater pipes, catch basins, wetlands, and rivers. They have been awarded $150,000 in 2019 through the BC Community Emergency Preparedness Fund for flood risks assessments and response planning. Aqua Dams and manhole blocking systems were also implemented to physically contain and manage rainwater flow.31,33,34

With projections of increased natural disasters in BC, lack of emergency preparedness can leave communities uninhabitable and cause severe physical and mental health disruptions. Emergency preparedness strategies, provincial guidelines, and toolkits aid in strengthening climate resilience for rural health services. The following section will explore these in further detail.
Rural community adaptation to the challenges of climate change and ecosystem disruption should be built on a strong local foundation addressing climate hazards, resources, and opportunities for a strategic response
Emergency Preparedness Adaptation for Health Services
Addressing acute health outcomes of climate events should entail evidence-based assessments of community-specific vulnerabilities. This includes exposure to disasters, socioeconomic status, prevalent health conditions, population demographics, and available public services.35,36 A report on Community Health and Climate Change (2020) mapped community-level health vulnerability index to four hazards of climate change: summer temperatures, wildfire smoke events, ground level ozone pollution, and coastal and river flooding. The vulnerability index was formulated based on three elements: exposure, sensitivity, and adaptive capacity. Currently, results from the study are only available for Vancouver Coastal and Fraser Health regions.35 Development of such resources for the rest of the province will underpin the development of rural health services adaptation strategies.
Climate disasters result in sudden surges of hospital admissions and patient visits.37,38 In these circumstances, geographic isolation and limited transportation infrastructure make it hard for rural communities to depend on centralized health services for support. Rural emergency preparedness must recognize this limitation and focus on maximizing local services capacity. For example, rural communities have experienced greater increases in the number of nurse practitioners compared to nurses and physicians as a result of the Nurse Practitioners for British Columbia (NP4BC) program implemented in 2012.39 These nurse practitioners have served as local resources and have filled gaps in primary health services within rural populations. This suggests that allocating a broader scope of practice to nurse practitioners in rural BC will be a practical adaptation strategy centred on building local services capacity. Ultimately, this will enable communities to better respond to spikes in acute conditions, and maintain continuity of care, especially for patients requiring treatment for chronic illnesses such as chemotherapy for cancer, dialysis for renal failures, and mental health therapies.40,41
Investigating the adaptive capacity of hospitals is also crucial for disaster management. Historically, simulation models in general healthcare have aided resource allocation and hospital designs.42-44 For rural emergency preparedness, the focus of simulation models should be on optimizing fewer than 100 beds and less frequently functioning operating rooms.39 Other considerations include low staffing, limited life-support devices, and greater distance to nearby hospitals.45,46 However, simulations in this context are more challenging because disaster response capability depends on multiple factors for which data is not readily available or up-to-date, such as the accurate number of patients accessing health services in a given region. Further, the extent of hospital or transportation damage that determine post-disaster healthcare capacity is often unpredictable. Developing rural-specific simulation models that take these into account is an important future task for climate adaptation.
Furthermore, volunteerism can supplement rural emergency preparedness. The United Nations Office for Disaster Risk Reduction (UNDRR)’s Sendai Framework emphasized the role of volunteers in providing pragmatic guidance and collective participation in disaster management.47 This is especially powerful in rural and Indigenous communities with a strong sense of unity. A series of case studies concluded that Indigenous values, such as unity, hospitality, and strong relationships are cultural enablers of volunteerism, and that altruism in Indigenous communities is necessary for long-term adaptive capacities.48 Volunteering also serves as a method of therapeutic healing by allowing community volunteers to become active players in their own recoveries, rather than passive victims. Positive impact on self-image and community cohesion have additional long-term implications, such as tighter-knit communities and increased engagement in public concerns.49
The Disaster Psychosocial Services (DPS) Program is an example of a volunteer-based emergency service. Professional and paraprofessional volunteers from organizations such as the BC Association for Social Workers, Police Victim Services of BC, and Canadian Association for Spiritual Care are deployed to the communities to provide emotional, psychological, and practical social support. The program also offers psychological first aid training to communities’ first responders to enhance local emergency response capacity, thereby increasing community mental health and resilience.50
Dr. Eliseo Orrantia discusses the impact of team-based care models in responding to crises and how this model could help respond to the threats of climate change (4:17)
Emergency Preparedness for Infectious Diseases
In early 2020, the COVID-19 pandemic highlighted a need for rural community preparedness to respond to infectious disease outbreaks. As climate change becomes more extreme, changes to the transmission of and exposure to infectious diseases such as COVID-19 have become inevitable.51 A warmer climate has already changed the distribution and incidence of vector-borne diseases. For example, the occurrence of Lyme disease in Canada has increased as a result of temperature-driven expansion to tick ranges.52 Emergency preparedness for infectious disease is critical for future rural health services planning.

The United States’ Center for Disease Control and Prevention (CDC) recommends that communities prepare for an infectious disease outbreak by assessing their susceptibility to the potential infectious diseases as well as their community’s social vulnerability index which includes factors such as housing, transportation, socioeconomic status, race and ethnicity, and language.53 In disease-specific susceptibility assessments, communities should account for some of the distinct features of the disease, including its modes of transmission and its effect on the most at-risk population. According to the CDC, some actions communities and health service planners can take in the development of an infectious disease emergency response plan include:
- Develop a response plan that is adjusted to meet the needs of the populations served, such as the elderly, people with disabilities, and substance users.
- Develop plans in collaboration with other health care providers and jurisdictions.
- Plan for effective and efficient supply chain management.
- Develop appropriate measures for the safe and fast transport of rural residents to urban centres in case a higher level of care is required.
- Increase availability and quality of telehealth services to reduce risk of infection.
- Health care providers should work to foster trust and credibility within the community when sharing the response plan and related information on infectious diseases by:
- Assuring that messaging is culturally appropriate.
- Assuring that messaging is accessible and shared in a manner appropriate for people with disabilities.
- Providing translation in multiple languages as necessary.53
Much can be learned from COVID-19 responses for developing sustainable infectious disease emergency preparedness measures that meet the needs of rural communities. In BC, a collaborative framework was developed in 2020 by the provincial government, in collaboration with the FNHA, the Northern Health Authority, and the Provincial Health Services Authority, which ensures that the healthcare needs of rural communities are met during crises such as the COVID-19 pandemic.54 The Framework includes measures to meet the immediate needs of communities, as well as to promote sustainable transformation of the emergency response capacities of rural communities in post-pandemic conditions.
