How Data Should be Restructured: Population Catchment Approach
Respect for the principles articulated in the previous section (see ‘Principles of Data Reorganization for Rural Health’) leads to new opportunities for designing new systems with novel technologies. In the context of rural healthcare services, Schuurman et al. developed a GIS model based on travel time to healthcare facilities to define true geographical catchments around rural hospitals.18 Specifically, they utilized a GIS network analysis based on vectors to create catchment models that accurately depict and map the availability of hospital-based healthcare services in rural and remote regions of BC. This tool allows for modelling where various services, like rural maternity care or ICU, can be assessed. Additionally, this catchment tool estimates the percentage of the population that can be reached within specific travel times and those that cannot.
Similarly, researchers in Australia used GIS to analyze the distribution of maternity services across rural and remote Australia.19 Like Schuurman, they conducted a network analysis to define a health facility catchment as the surrounding geographic region that can be reached by road within a one-hour drive time. The study revealed that rural health facilities located 1 to 2 hours away from a C-section facility were more likely to offer birthing services than those closer to C-section facilities, regardless of the characteristics of the population living within those catchments.19 This raises the question of why health service systems do not support non-C-section birthing services, when outcomes are better than having no local services at all.
Building on these models, the following assumptions and consequent data strategies form the foundation for a population catchment approach for rural BC:
- The population catchment is geographically defined by proximity to the point-of-care. In urban areas, health facilities are central, easily accessible, and numerous to accommodate dense populations. Individuals living in urban settings often have several options for health facilities within close proximity and may select their location of care based on other factors, such as wait times or specialty, rather than simply proximity. In comparison, rural communities in BC are typically served by a single health centre or hospital with most of the population situated relatively close by the health facility. This is because rural regions in BC are composed of distinct population clusters between mountains and dense forest patches. Due to this isolated and dispersed geography, BC is well suited to be organized into distinct, geographically defined population-based catchments surrounding each rural health service point.
- One hour of travel time by car to a care centre is a reasonable distance to work with as a standard measure since there is recognition of this standard travel time in the literature related to rural maternity care and trauma care outcomes.21, 22
- The population of the catchment, based on residency, is definable through address, including using postal codes and census data.
- Health service utilization data for the defined population is the first layer of outcomes and can be related to the quality of local services. It is likely that some residents of rural catchments will travel further away to access basic services for family or personal reasons, but the majority of residents should access care based on location unless there are significant barriers such as racism, inequity, or quality of care issues. If utilization patterns are unusual in the catchment then further analysis might be justified.
- Population catchments can be linked to health outcomes through BC health data resources like Population Data BC and Perinatal Services BC using the home address (postal codes) of patients.
- The definition of a population denominator within the catchment framework provides a tool for comparison between rural communities. The establishment of a level playing field based on population and the need for services creates the potential for evidence-based systematic planning and quality improvement. This is particularly relevant to a time of system renewal and transformation such as we are currently experiencing across the province.
Rural populations should be linked to the services reached by creating hospital population catchments based on 1-hr travel times
Using the assumptions outlined above, RHSRNbc has created a GIS Catchment Tool, using ArcGIS, to map the areas located within a one-hour drive time from all 45 rural hospitals, forming a catchment boundary for these communities. The following image demonstrates the catchment map and overview for Fort Nelson, a northern community in BC (Figure 2).
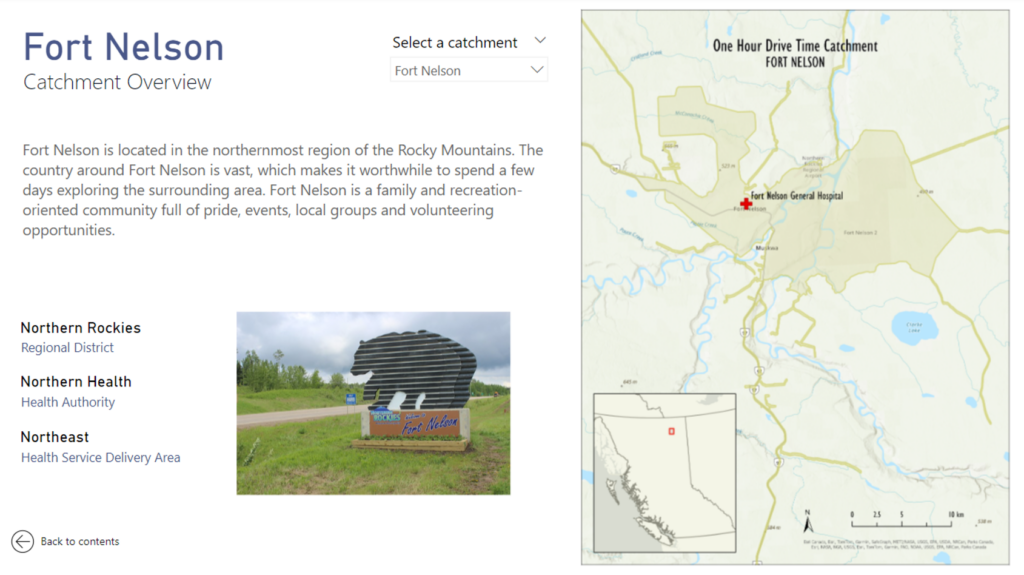
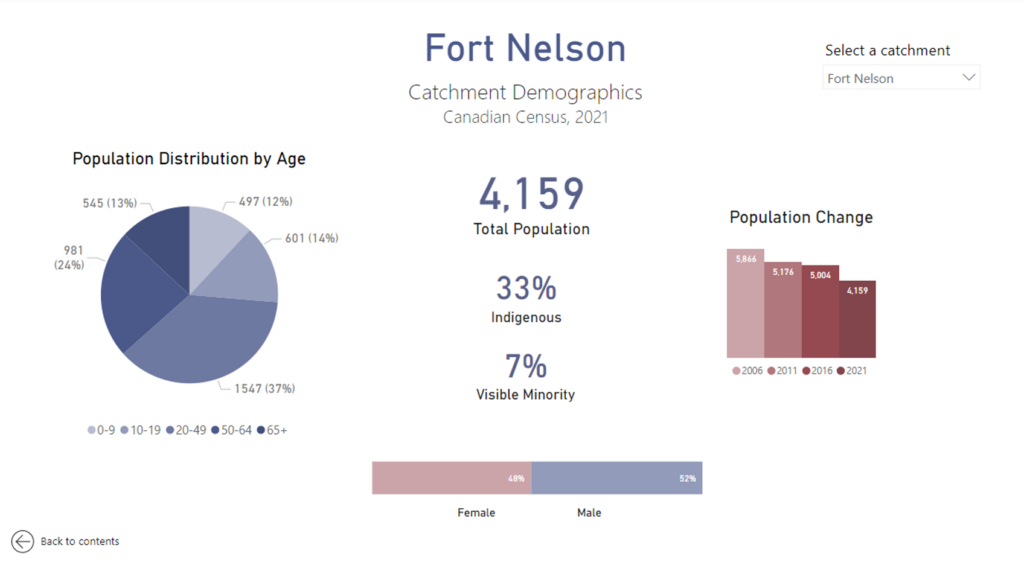
The physical catchment boundary (as depicted by the map above) is then overlaid with the corresponding census data to calculate the population size. The use of census data provides access to relatively stable demographic data that is standardized across all communities. Moreover, since the census is updated at regular intervals of five years, it is possible to keep track of longitudinal population characteristics. These data can include specific demographic data such as a population age distribution and the proportion of the catchment population that is Indigenous, in order to provide a better understanding of what the specific population health needs may be (Figure 3).
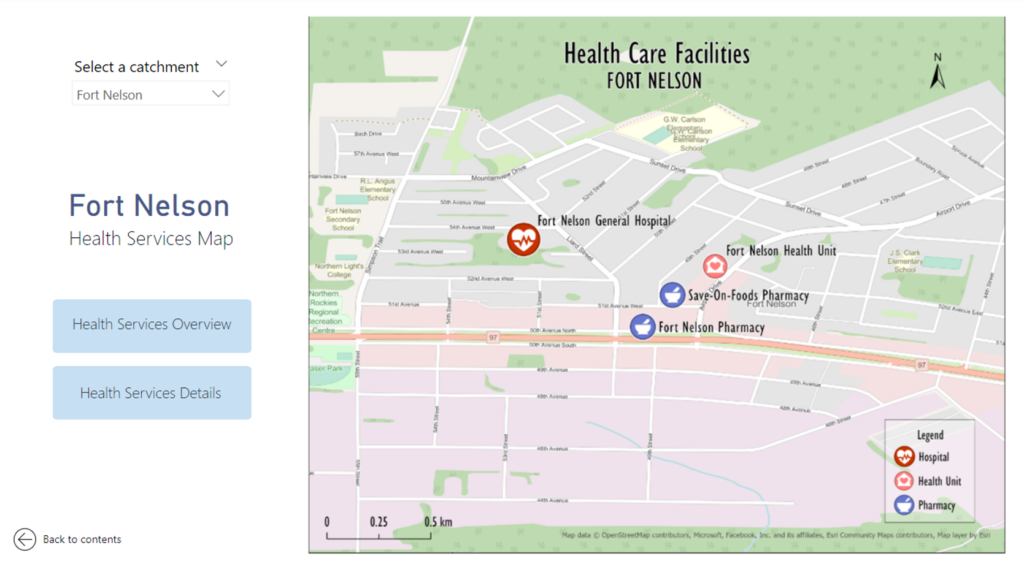
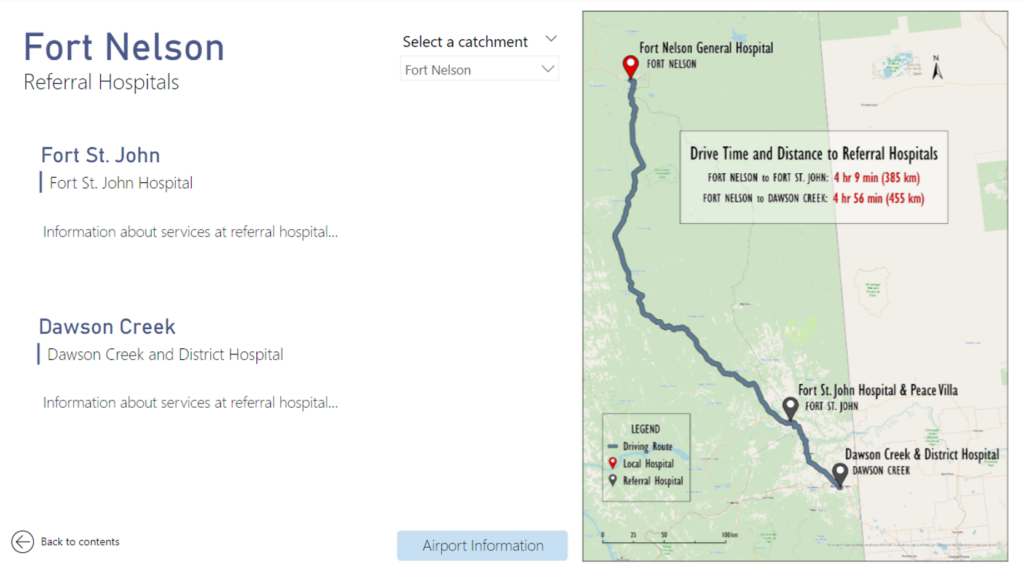
Using this catchment approach, each rural community in BC can be organized into a similar community profile. In addition to population demographics, community profiles can also include information on the local services available (Figure 4), and the community’s relationship with the nearest referral centre (Figure 5).
The strength of defining a catchment based on one-hour drive times from a healthcare facility is that it highlights the direct needs of the population (demand), which can then be matched with the appropriate and sustainable level of services (supply). Moreover, the census and hospitalization data can be linked using postal codes, which would provide healthcare planners with a much more accurate understanding of who is accessing health services and more importantly, who is not. When health services planning is solely based on historical utilization data, it assumes that everyone who needs healthcare services is able to access those services, which is not always the case.20 Combining census data with hospitalization outcomes will help determine the proportion of the catchment population that is not accessing services, and prompt appropriate initiatives to ensure that healthcare is being accessed equitably by everyone in the catchment.
Models like these have applicability for a wide variety of healthcare policy and planning. Establishing a catchment profile for each community in the province, and ensuring that it is updated based on availability of external data, can also be a tool to aid in ecosystem disruption planning. Developing projections and scenario-based analyses for disruptions like the COVID-19 pandemic can better equip rural communities to respond effectively, particularly when they have access to community-specific and relevant data.
