Chapter 1 Introduction to Pathophysiology; Cellular Responses to Stress, Injury, and Aging
Section 4 Cellular Change in Disease
Zoë Soon
Biopsies allow for the microscopic analysis of cells and tissues – known as cell morphology or the study of structure, shape, and arrangement of cells. This is essential for detecting signs of disease and determining the cause and extent of disease progression. Each of the 200+ human cell types has a typical diameter, shape, and set of organelles within the normal, healthy range.
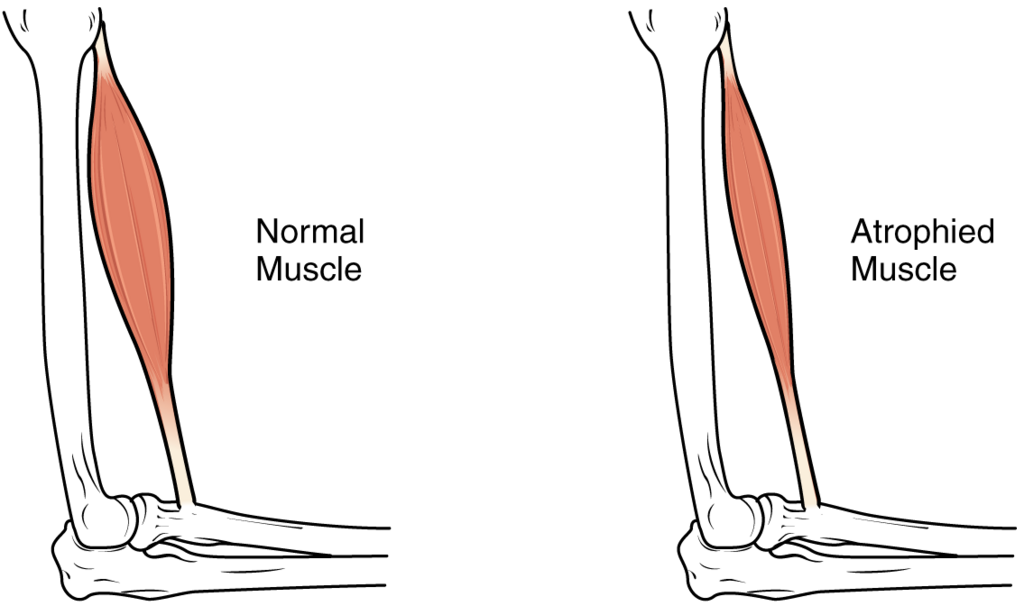
Atrophy
Atrophy is the shrinkage of cells below their normal size. The prefix a- means ‘without’ and tropy means ‘growth’. At least seven causes of skeletal muscle atrophy have been identified:
- Bed rest: Muscles not used due to prolong immobility begin to shrink – a ‘use it or lose it’ phenomenon.
- Casting: Restraint of a limb (e.g., when a bone is broken) prevents muscle use, leading to atrophy visible when the cast is removed.
- Low-gravity environments: Astronauts experience muscle atrophy because their muscles are nor required to generate as much force in microgravity.
- Reduced neural input: Nerve damage such as in spinal cord injuries (e.g., paraplegia or quadriplegia) severs the neural connections to muscles, which then atrophy without stimulation.
- Poor nutrition / starvation: Without adequate dietary nutrients, cells lack the building blocks for growth and maintenance.
- Ischemia: Poor blood flow (from the Greek ischein ‘hold back’ + haima ‘blood’) means reduced nutrient and oxygen delivery, coupled with lowered waste removal, impairs cell function and maintenance.
- Reduced hormones: With aging, the body produces less estrogen, testosterone, and growth hormone, leading to reduced cellular stimulation and noticeable atrophy of muscle, bone, and other tissues.
Hypertrophy: Physiologic vs. Pathologic
Hypertrophy is the opposite of atrophy – it refers to an increase in cell size. The prefix hyper- means ‘more’.
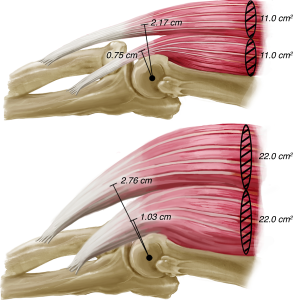
| Physiologic Hypertrophy | Normal, healthy cell growth in response to increased demand. Example: skeletal muscle hypertrophy during exercise training, as cells produce more contractile proteins (myosin, actin) and increase in diameter and strength. |
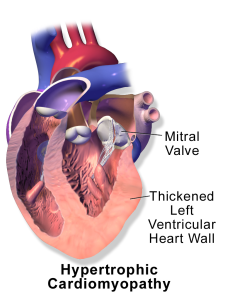
| Pathologic Hypertrophy | Cell enlargement caused by disease. Example: in heart disease and hypertension, the heart’s ventricular muscle must work harder to pump blood through damaged or narrowed vessels, leading to ventricular wall hypertrophy. Unlike physiologic hypertrophy, this change is detrimental – the heart’s shape becomes less efficient at pumping blood, signalling deterioration. |
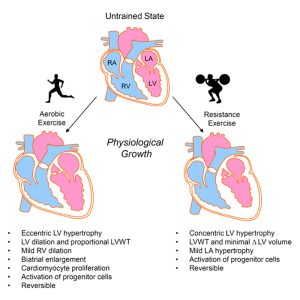
Athlete’s Heart: Exercise-Induced Cardiac Remodeling
Both resistance and cardiovascular training cause beneficial cardiac remodeling, but in distinct ways:
Resistance training: Ventricular wall thickness increases (without major increase in fill volume), helping the heart generate more pressure to pump blood through compressed vessels during weightlifting.
Cardiovascular (aerobic training): Both wall thickness and fill volume increase, allowing the heart to send larger volumes of blood per beat – reducing the need for a rapid heart rate during long-duration events like marathons.
In both forms of training, progenitor cells are activated, meaning hyperplasia (increased cell number through cell division) in addition to the cellular hypertrophy is contributing to heart enlargement (physiologic cardiac hypertrophy). Importantly, both adaptions are reversible – if training stops, the cellular changes reverse.
Hyperplasia
Hyperplasia refers to an increase in cell number due to mitosis (cell division). The suffix -plasis, comes from the Greek word meaning ‘formation’. As with hypertrophy, hyperplasia can be physiologic or pathologic.
| Physiologic Hyperplasia | Normal growth occurring, for example, during childhood development (from embryo through to adulthood), or during pregnancy (growth of the uterus, breasts, and other supportive tissues). |
| Pathologic Hyperplasia | Usually caused by a disease creating a hormonal imbalance that drives excess cell division. It can also lead to the formation of a benign tumor, which may be surgically removed if it causes clinical manifestations. |
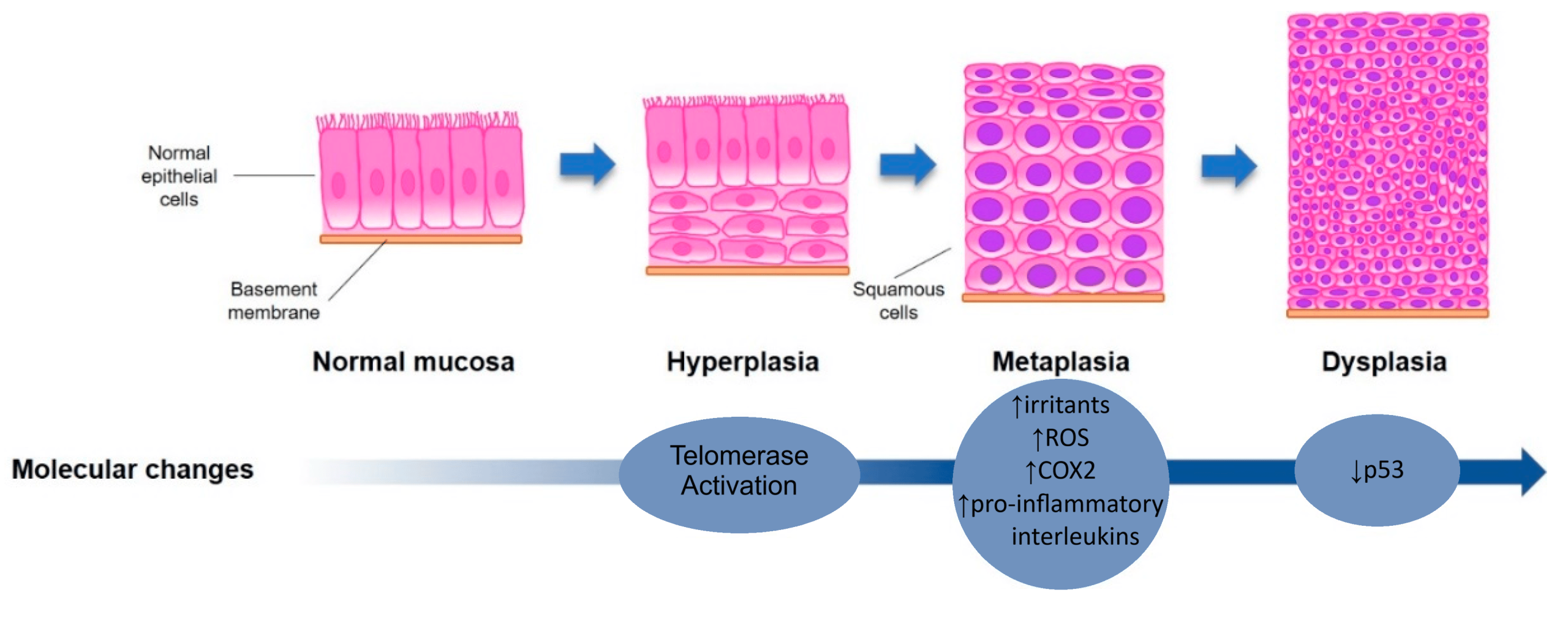
Metaplasia
Metaplasia (from Greek: ‘change form’) occurs when one cell type replaces another in response to chronic irritation, producing a more resilient but less functional tissue.
Examples: Smoker’s Trachea
Under normal conditions, the trachea (windpipe) is lined with simple pseudostratified columnar ciliated epithelial cells and mucus-secreting Goblet cells. Cilia sweep mucus and trapped pathogens upward to be swallowed and eliminated.
In a long-term smoker, this tissue is perpetually damaged by smoke and remodels itself into stratified squamous epithelium with no cilia and fewer Goblet cells. This new tissue is more resistant to smoke, but far less functional: mucus production decreases and cilia are absent, requiring the smoker to rely on coughing to clear the airway – the well-known ‘smoker’s cough’. Metaplasia is thought to be reversible if the irritant is removed.
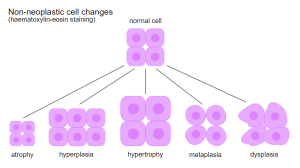
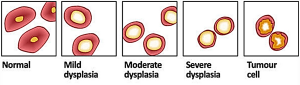
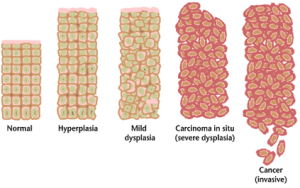
Dysplasia, Anaplasia, and Neoplasia
| Dysplasia | Literally ‘bad growth’ (dys- = bad). Cell shapes change and cells become less functional and de-differentiated (more immature). Dysplastic cells are considered pre-cancerous. If the irritant is removed and normal gene expression resumes, dysplastic cells may revert to normal. |
| Anaplasia | Completely de-differentiated, non-functional cells that have entered a state of uncontrollable, continuous cell division. Anaplastic cells are often immortal. |
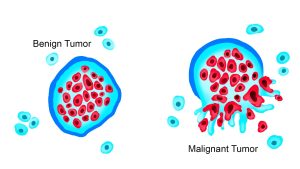
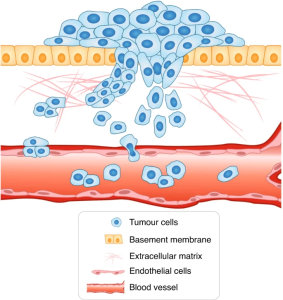
| Neoplasia | A ‘new growth’ or tumor produced by the accumulation of anaplastic cells Can be benign (non-cancerous, confined within the basement membrane) or malignant (cancerous, capable of breaching the basement membrane, spreading through blood or lymph vessels and infiltrating other tissues. |
| Carcinoma in situ | A pre-malignant state in which the basement membrane remains intact. Most carcinomas in situ eventually progress to become malignant. |
The typical sequence of changes is: Normal → Dysplasia (reversible if the irritant is removed) → Anaplasia → Neoplasm (benign or malignant). If malignant cancerous cells breach the basement membrane, they can enter blood or lymph vessels, spread to distant sites, form secondary cancers, and if untreated, cause multi-organ failure.
Causes of Dysplasia and Cancer: Three Examples
1. Smoking and Lung Cancer
Smoking causes persistent irritation to cells within the respiratory tract and is the leading cause of lung cancer. It is also a risk factor for several other cancers.
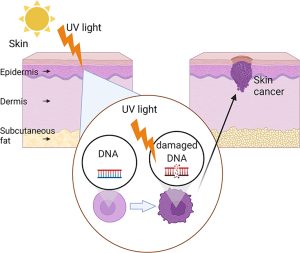
2. UV Light and Skin Cancer
Ultraviolet (UV) light causes DNA mutations in skin cells and is the leading risk facto for the most common forms of skin cancer, including basal cell carcinoma, squamous cell carcinoma and melanoma
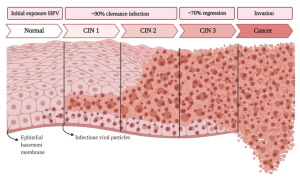
3. Human Papilloma Virus (HPV) and Cervical Cancer
Several strains of Human Papilloma Virus (HPV) are known oncoviruses (viruses that can cause cancer). Some HPV strains are risk factors for cervical cancer, penile cancer and cancers of the mouth, throat, anus, and vagina; other stains cause genital or skin warts. HPV is transmitted skin-to-skin contact, including sexually.
HPV Vaccination and Cervical Screening in Canada
In Canada, the HPV vaccine is available for youth and is ideally given prior to sexual activity – when the risk of viral exposure is lowest. Early detection of cervical cancer is critical for a better prognosis and the following screening protocol is recommended:
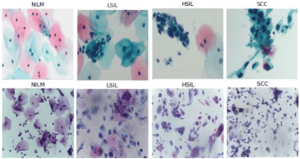
Pap smear (Papanicolaou test): Cervical cells are scraped and examined under a microscope for abnormal morphology. Recommended every 2-3 years after an individual becomes sexually active (as per physician recommendation). Named after Dr. Georgios Papanikolaou, who developed this test in 1923.
HPV testing: An emerging approach adds Primary HPV testing (a highly sensitive DNA test for high-risk HPV stains) as a first step, followed by the Pap smear (cytology), and then colposcopy (a specificity test) when abnormal cells are detected. Colposcopy utilizes a lighted magnifying instrument, allowing the physician to examine the cervix, vagina and vulva for abnormal areas which can be biopsied and sent to the lab for testing.
Media Attributions
- fig-3-full © Vigotsky AD, Contreras B, Beardsley C. is licensed under a CC BY (Attribution) license
- Private: Atrophy is licensed under a CC BY (Attribution) license
- Exercise-induced_cardiac_growth_-_Cardiac_remodeling_from_Aerobic_and_Resistance_exercise © Kyle Fulghum, Bradford G. Hill is licensed under a CC BY-NC-SA (Attribution NonCommercial ShareAlike) license
- Blausen_0166_Cardiomyopathy_Hypertrophic © Blausen Medical Communications is licensed under a CC BY (Attribution) license
- Non-neoplastic_changes.svg © Dennis Hansen is licensed under a CC BY (Attribution) license
- 5971147bf2f20018315cd3b0_figure-2[1]crop
- Tumor_Types_MTK © WolfpackBME is licensed under a CC BY-NC-SA (Attribution NonCommercial ShareAlike) license
- Cancer_progression_from_NIH is licensed under a Public Domain license
- Metastasis © Novikov, N.M., Zolotaryova, S.Y., Gautreau, A.M. et al is licensed under a CC BY (Attribution) license
- Metaplasia-Dysplasia-Lung-Modified-ZS © Ashraf-Uz-Zaman, M.; Bhalerao, A.; Mikelis, C.M.; Cucullo, L.; German, N.A. adapted by Zoë Soon is licensed under a CC BY-NC-SA (Attribution NonCommercial ShareAlike) license
- UV skin cancer © Breen I and Richmond J is licensed under a CC BY (Attribution) license
- HPVcervicalcancer © Causin, R.L.; Freitas, A.J.A.d.; Trovo Hidalgo Filho, C.M.; Reis, R.d.; Reis, R.M.; Marques, M.M.C. is licensed under a CC BY (Attribution) license
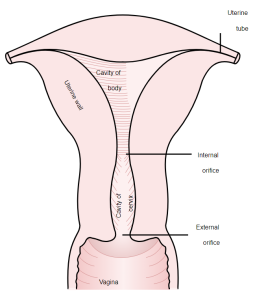
- Cervix © Henry Vandyke Carter - Henry Gray (1918) is licensed under a Public Domain license
- Pap Test © Karasu Benyes, Y.; Welch, E.C.; Singhal, A.; Ou, J.; Tripathi, A. A is licensed under a CC BY (Attribution) license

{kind=link}