Chapter 1 Introduction to Pathophysiology; Cellular Responses to Stress, Injury, and Aging
Section 9 Four Types of Necrosis
Zoë Soon
When cells undergo necrosis, the resulting tissue damage ahs a characteristic appearance that depends on the cause and location of the injury. There are four main types of necrosis, each name for what the affected tissue looks like.
1. Liquefaction Necrosis
In liquefaction necrosis, dead cells liquefy into a soupy, fluid-filled mass. This occurs because lytic enzymes release from the lysosomes of dying cells break down proteins and other cellular components. Liquefaction necrosis most commonly results from infection and follows this progression:
- Cells die and release hydrolytic enzymes that digest surrounding tissue.
- Macrophages arrive and release cytokines to recruit additional white blood cells, including neutrophils (also phagocytes), to the area.
- Phagocytes engulf debris and if present, the infecting agent (e.g., bacteria, virus, fungi).
- If the bacteria resist phagocytosis, the infection persists and may require antibiotics. (Viral and fungal infections require antiviral and antifungal medications respectively).
- A fluid-filled space or abscess may form, particularly in closed tissue such as beneath the skin (e.g., from a splinter carrying bacteria). Treatment may include lancing the abscess to release fluid and deliver antibiotic therapy.
- If the wound is open, the battle between bacteria and phagocytes may produce pus – a protein-rich fluid containing dead cells and cell debris.
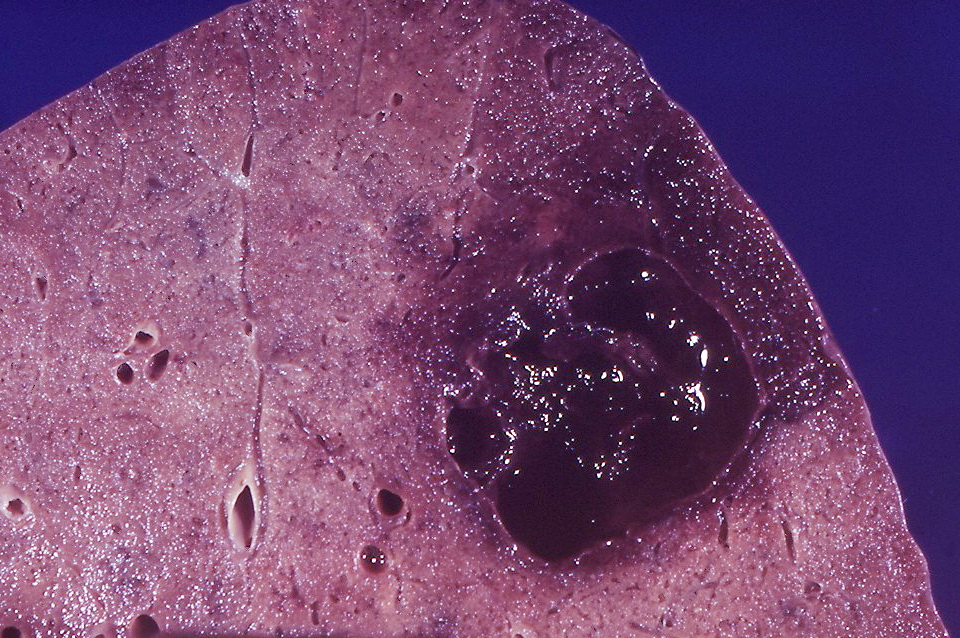
Special Case: Liquefaction Necrosis in the Brain
Although liquefaction necrosis is typically caused by infection, the brain is a notable exception: hypoxia in the brain also causes liquefaction necrosis rather than the coagulative necrosis induced by hypoxia in other organs. The reason is not fully understood, but it may be related to the brain’s lower connective tissue content.
A bacterial infection of the brain can similarly cause liquefaction necrosis, potentially forming a fluid-filled abscess visible on brain imaging.
2. Coagulative Necrosis
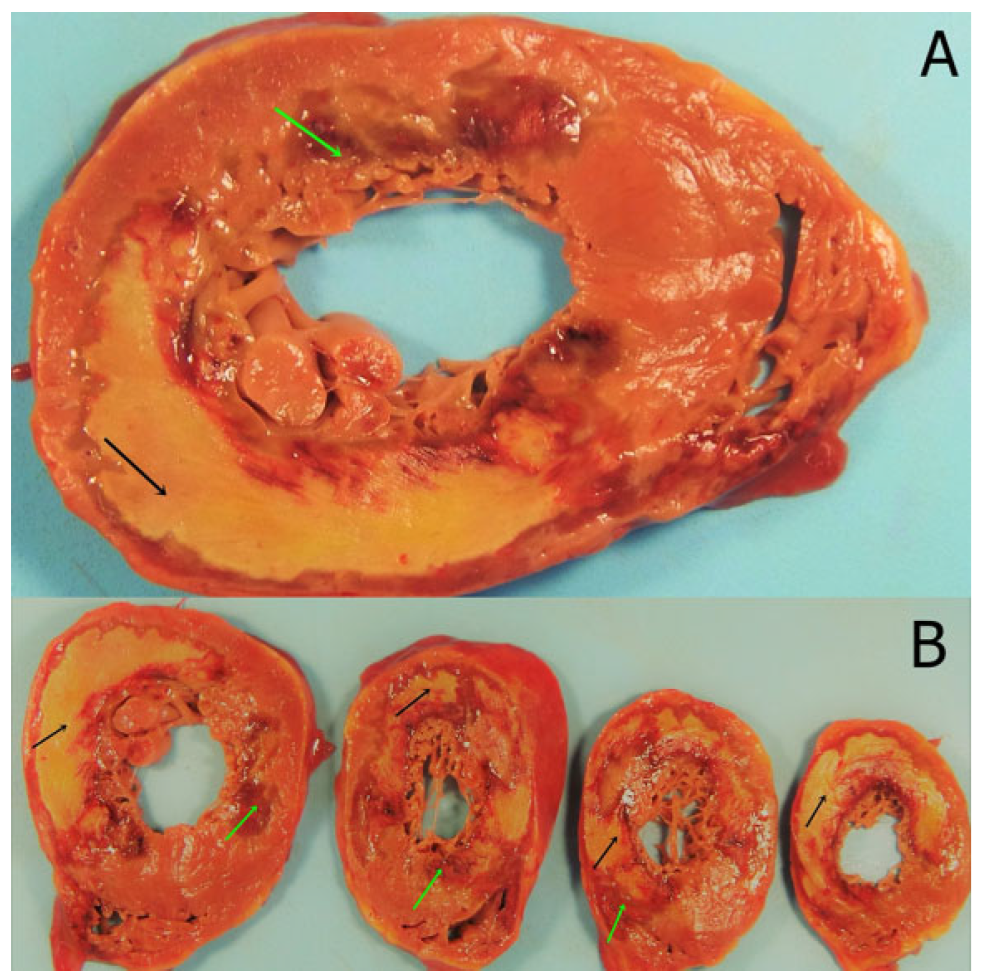
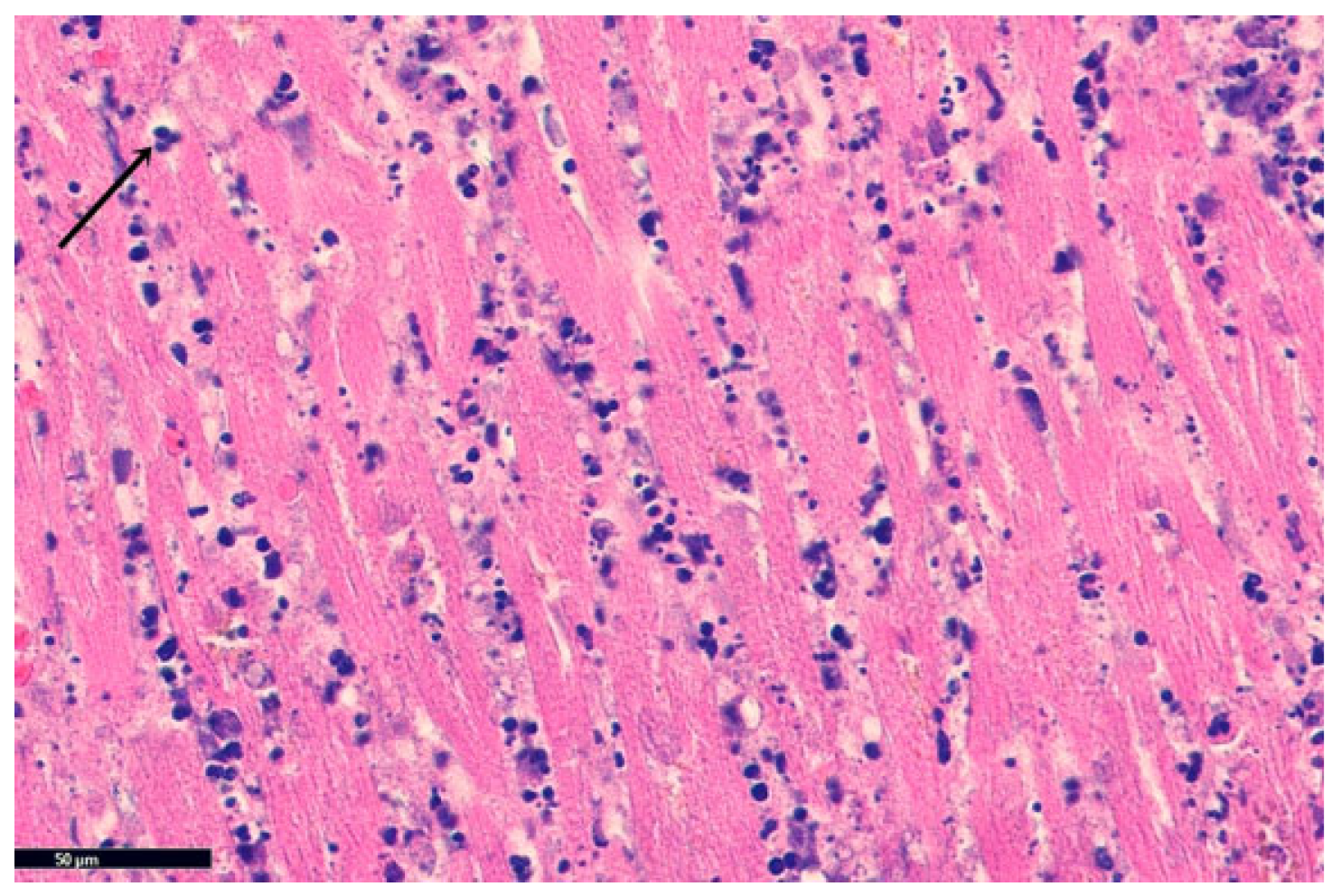
Coagulative necrosis is the most common type and typically results from ischemia (in any organ other than the brain). During ischemia, cells switch to anaerobic metabolism, generating large amounts of lactic acid. This acidic environment denatures proteins – including the lytic enzymes that otherwise liquefy the tissue. As a result, the dead tissue takes on a firm, pale yellow, cheese-like appearance.
Because the lytic enzymes are themselves denatured, the tissue is not dissolved into soup – it retains its structural outline (at least temporarily) while the cells within are dead. This is commonly seen in ischemic kidney tissue and in the heart following a myocardial infarction (heart attack).
Some bacterial infections can cause coagulative necrosis rather than liquefactive necrosis, particularly when bacterial toxins induce ischemia. Similarly viral infections can also induce coagulative necrosis when they cause severe hypoxia in tissues.

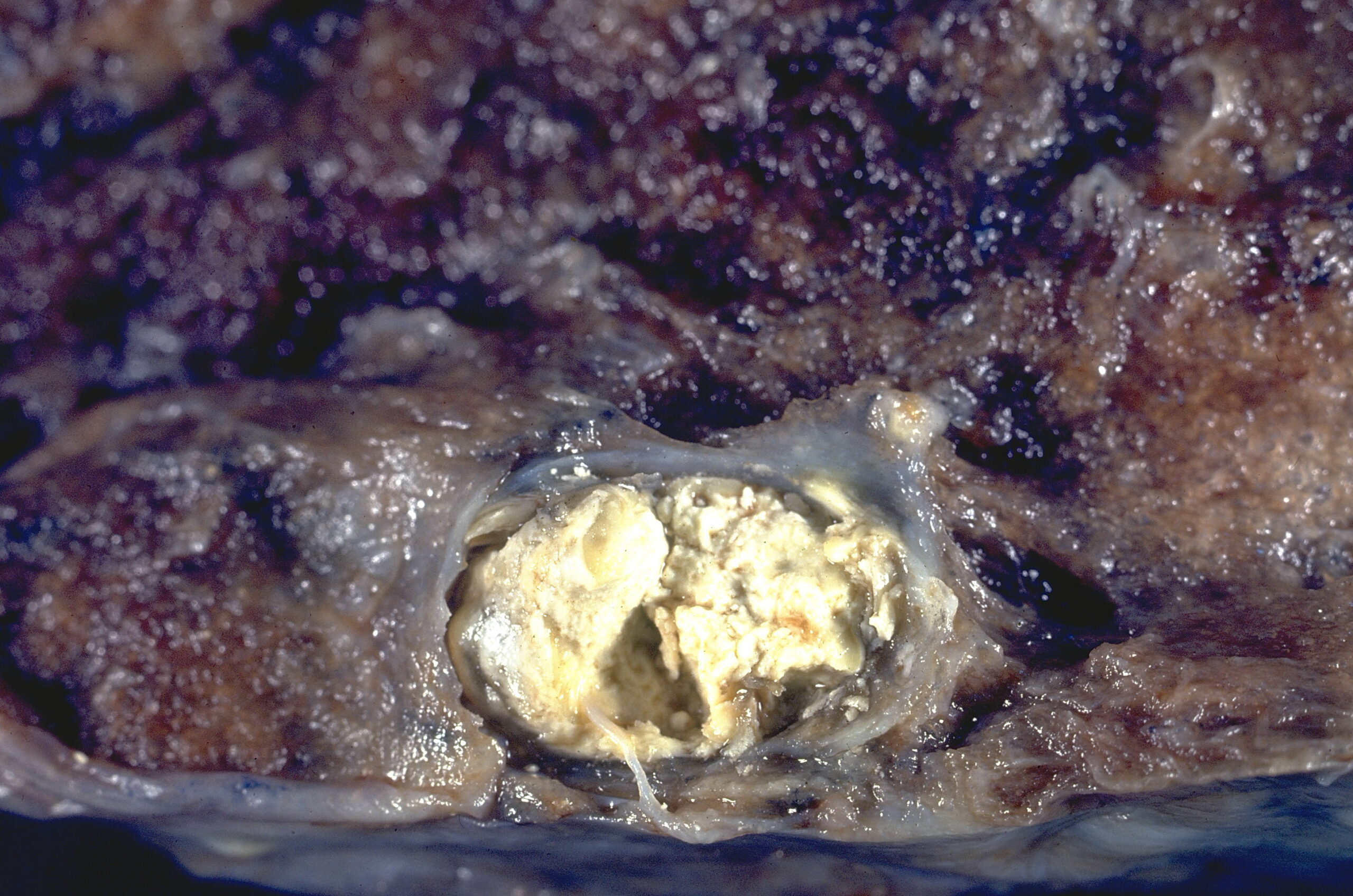
3. Caseous Necrosis
Caseous necrosis is caused by particular types of infection rather than ischemia. Instead of dying as a result of hypoxia, cell death is induced by specific bacteria and fungal infections and the ensuing response by white blood cells.
The most common example is tuberculosis (TB) – a serious respiratory disease caused by the bacterium Mycobacterium tuberculosis and spread by respiratory droplets. Certain fungal respiratory infections (e.g., histoplasmosis, cryptococcosis, and coccidioidomycosis) can also result in caseous necrosis.
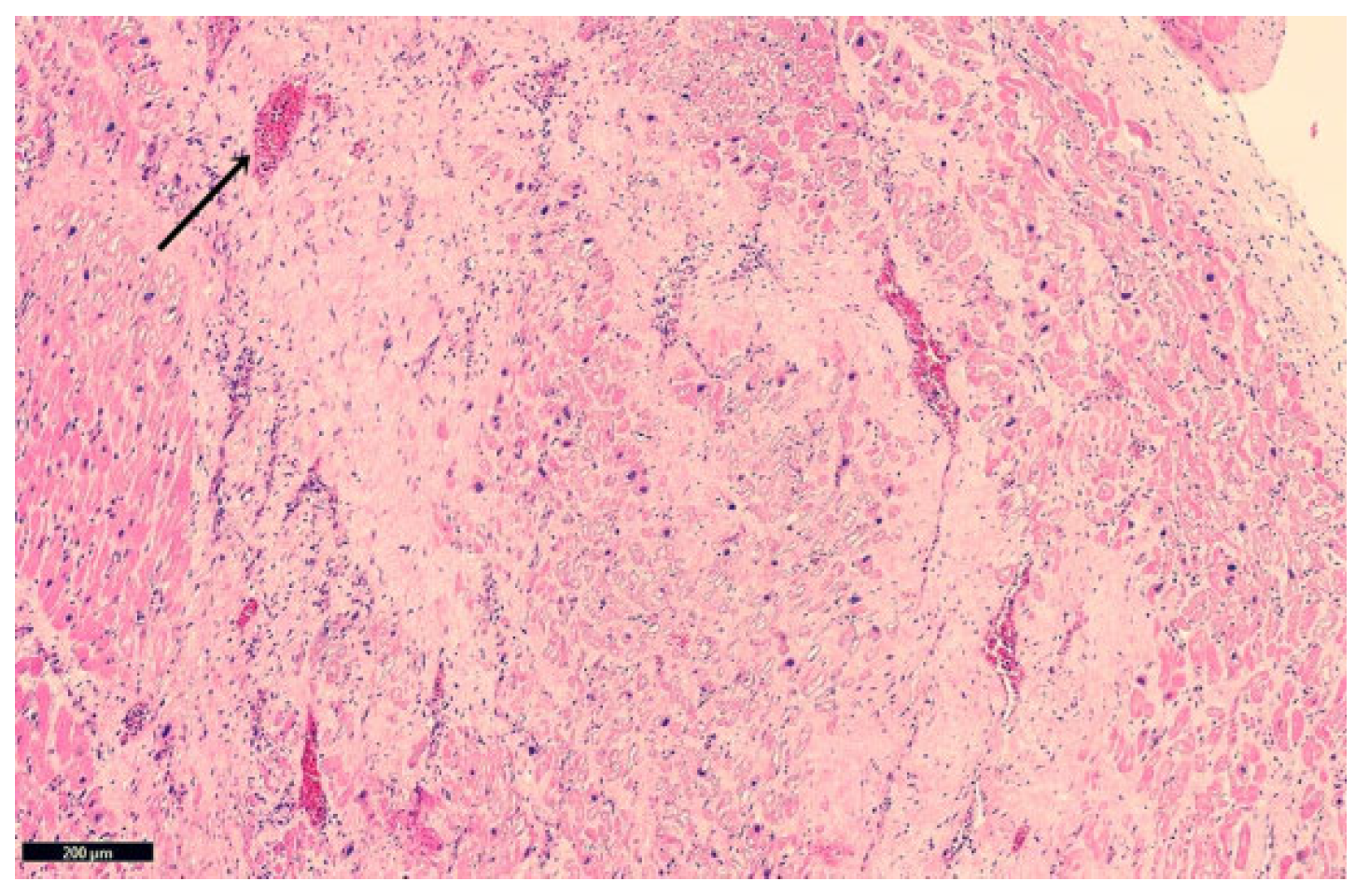
In these respiratory infections, the killing of lung cells attracts white blood cells, including macrophages to the area. The macrophages promptly wall off the infected area and release digestive chemicals causing the affected cells to disintegrate. The dead tissue has a cheese-like appearance, a necrotic zone that becomes enclosed within a granuloma (an aggregation of macrophages). When fully walled off (often with a rim of calcium), this is called a Ghon focus. The contained tissue has a soft, crumbly, cheese-like appearance, hence the name ‘caseous’ (from the Latin word for cheese).
The danger of TB lies in its ability to persist in latency. Live bacteria can remain viable inside the Ghon focus for years or even decades. If the person later becomes immunocompromised (due to aging, HIV, or another illness), the bacteria, can reactivate causing progressive lung destruction, form expanding cavities, and even spread through the bloodstream to other organ.
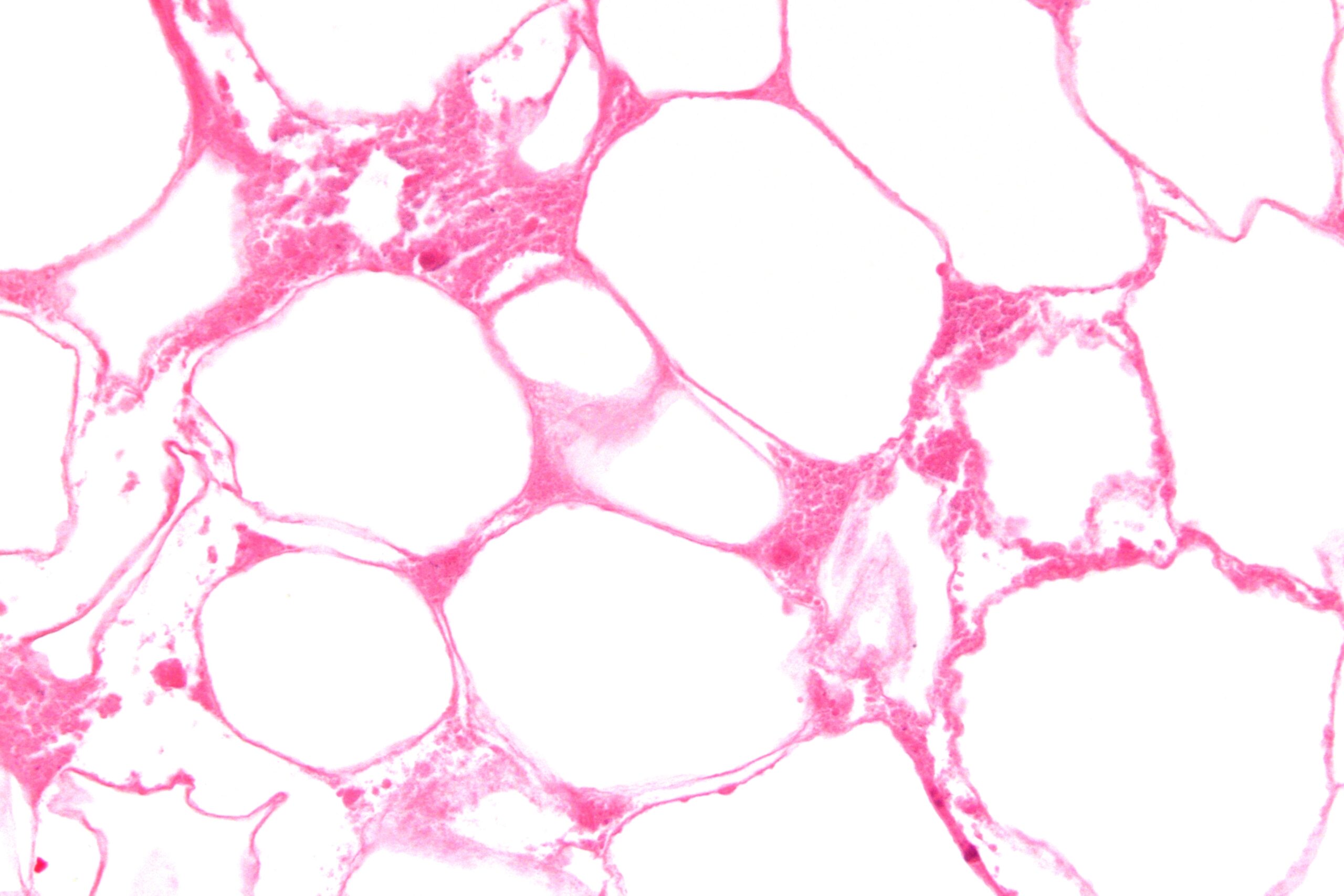
4. Fat Necrosis
Fat necrosis is rare and occurs specifically in fatty tissues such as the pancreas or breast tissue. When cells in these tissues die, lipase (an enzyme that breaks down triglycerides) is released. Lipase cleaves triglycerides into glycerol and fatty acid chains. The freed fatty acids then bind to calcium, forming a chalky, soap-like residue. This white, chalky deposit is the hallmark of fat necrosis.
∗ Real-World Story: Frostbite on Mount Everest – Beck Weathers
In 1996, climber Beck Weathers was left for dead near the summit of Mount Everest. That day was filled with a tragic series of events. During the last day in the final push for the summit, as the climbers ascended from Camp IV, Beck lost his vision and was no longer able to navigate the steep and treacherous terrain. While waiting for the climbing party to return from summitting, Beck became severely hypothermic and the hypoxic conditions of being high altitude led to difficulties in maintaining consciousness. A storm had blown in as the climbing party was attempting the final ascent to the summit. While waiting, Beck slipped into a hypothermic coma for several hours and miraculously awoke and managed to walk back down to Camp IV by himself. On rejoining climbers in the camp, he appeared near death. Little did he know that storm and plunging temperatures would claim 8 lives that day.
During extreme cold exposure at high altitude, the body vasoconstricts blood vessels in the skin – sacrificing the skin’s circulation to protect vital internal organs. Beck had lost a glove in the storm and the hours that went by before being able to descend resulted in Beck’s nose, cheeks, and hands being deprived of blood flow, oxygen and nutrients for too long. His hands reportedly looked like porcelain and his nose and cheeks had turned black. After the highest-altitude medical evacuation ever performed by a helicopter at the time (a risky challenge due to the thinness of the air), Beck required amputation of all four fingers and thumb of the left hand as well as his nose due to lost circulation in those tissues. Reconstructive surgery of his nose was performed using tissue from his ear and forehead.
The events of May 1996 are captured in the riveting movie ‘Everest’ as well as several books, including “Into Thin Air by Jon Krakauer, “Left for Dead: My Journey Home from Everest by Beck Weathers, “The Climb: Tragic Ambitions on Everest” by Anatoli Boukreev.
Media Attributions
- Private: Aspergillosis,_angioinvasive_(3679097189) © Yale Rosen is licensed under a CC BY-SA (Attribution ShareAlike) license
- Myocardial Infaction Coagulative Necrosis © Ghafoor, Mariam; Kamal, Maria; Nadeem, Urooba; Husain, Aliya is licensed under a CC BY-NC-ND (Attribution NonCommercial NoDerivatives) license
- Myocardial Infaction Coagulative Necrosis H&E stain © Ghafoor, Mariam; Kamal, Maria; Nadeem, Urooba; Husain, Aliya is licensed under a CC BY-NC-ND (Attribution NonCommercial NoDerivatives) license
- Normal Myocardiomyocytes H&E stain © Guo, Xiao-Fu & Yang, Xiang-Jun is licensed under a CC BY (Attribution) license
- Myocardial Infaction Granuloma H&E stain © Ghafoor, Mariam; Kamal, Maria; Nadeem, Urooba; Husain, Aliya is licensed under a CC BY-NC-ND (Attribution NonCommercial NoDerivatives) license
- Private: Tuberculosis_-_Sub-pleural_primary_(Ghon)_focus_(6596011395) © Yale Rosen is licensed under a CC BY-SA (Attribution ShareAlike) license
- Private: Fat_necrosis_-_very_high_mag © Nephron is licensed under a CC BY-SA (Attribution ShareAlike) license

{kind=link}