Chapter 2 Innate and Adaptive Immunity: From Cell Defense to Tissue Repair
Section 14: Wound Healing
Zoë Soon
Any break in skin in a wound. All wounds progress through four phases:
| 1. Hemostasis | Cellular damage triggers cytokine release attracting macrophages, neutrophils, platelets, and mast cells.
Platelet plug and fibrin mesh form to stop bleeding and contain the area. |
| 2. Inflammation | Macrophages and neutrophils remove pathogens and debris.
Pro-inflammatory mediators (histamine, prostaglandin, bradykinin) induce vasodilation, increased capillary permeability and trigger nociceptors producing the 4 cardinal signs of inflammation (redness, warmth, swelling, and pain). |
| 3. Granulation and Proliferation | Activated cells (fibroblasts, macrophages, epithelial and endothelial cells) release growth factors stimulating angiogenesis and formation of granulation tissue (pink, moist, fragile, highly vascular).
Fibroblasts produce collagen that crosslink and contracts across the wound to strengthen repair. Stem cells undergo mitosis to replace lost cells. |
| 4. Remodeling | Collagen-rich scar tissue may gradually be replaced by epithelial cells over time.
Extent of remodeling depends on wound dimensions, patient age, health, and genetics. |

Three Categories of Wound Healing
| Primary (1st) Intention | Minimal-gap, uninfected wounds (e.g., clean surgical incisions).
Edges approximated with sutures, staples, or adhesive closures. Criteria: clean, fresh (within 4-8 hours), free of debris, and necrosis. Results in minimal scarring and loss of functional tissue. |
| Secondary (2nd) Intention | Larger, deeper, or infected wounds where suturing is not feasible.
Heals from the base outward; cleaned and dressed to prevent infection. Results in more granulation tissue, more collagen, greater scare formation and reduced functional structures (fewer hair follicles, glands, sensory nerved endings, melanocytes). |
| Tertiary (3rd) Intention | A wound healing by 2nd intention is purposely interrupted during granulation to close it mechanically (skin grafts, sutures, staples) after initial treatment of infection and edema.
In this type of process, debridement may also have been required prior to closing the wound mechanically. |
Burn Wounds
Burns can be thermal, electrical, or chemical, affecting skin, respiratory tract (smoke inhalation), or digestive tract (chemical ingestion). Severity depends on cause, temperature/strength/concentration, duration, body area, and site. Older adults, infants, and children are more vulnerable to deeper burns due to thinner skin.
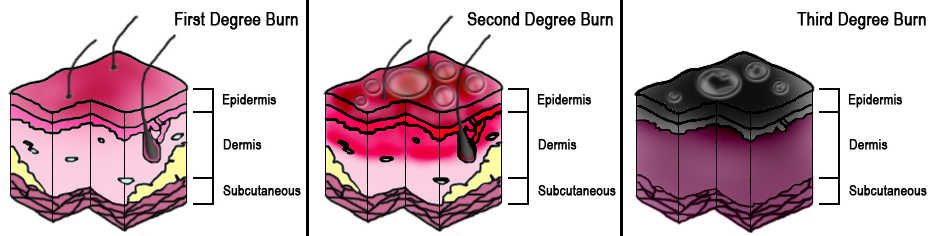
| Partial-thickness (1st degree) | Involves part of the epidermis only.
Inflammation; possible blister formation. Includes sunburns. Burn blisters should not be punctured – reduces infection risk and speeds healing. |
| Partial-thickness (2nd degree) | Involves epidermis and part of the dermis. Inflammation and blisters present. |
| Full-thickness (3rd degree) | Involves epidermis, dermis, and hypodermis (and possibly deeper tissue).
Eschar (dead tissue) is present. May require escharotomy to relieve pressure. |



Systemic Complications of Severe Burns
Dehydration: Large wounds allow significant water evaporation. Controlled by dressings or skin grafting.
Edema: Widespread capillary permeability causes extensive swelling and decreased blood volume.
Hypovolemic shock: Due to dehydration and edema → insufficient blood pumped → organ hypoxia → organ failure. Signs: hypotension, acidosis (from anaerobic respiration producing lactic acid). Pathway: massive inflammation → vasodilation → hypotension → hypoxia → organ failure → death.
Anemia: Caused by blood loss from trauma or burns.
Respiratory problems: Smoke inhalation → bronchiole inflammation → swelling, bronchoconstriction, and impaired gas exchange.
Infection / Sepsis: Large wounds are highly susceptible to infection and sepsis (infection → systemic vasodilation → septic shock → hypotension → organ failure → death). Prophylactic antibiotics are given to reduce chance of infection.
Hypermetabolism: Increased metabolic demands during healing require adequate nutrients, water, and electrolytes.
Contractures and Adhesions: Scar tissue can form contractures and adhesions that restrict mobility. Treatment can involve physiotherapy during rehabilitation to reduce loss of range of motion associated with scarring.
Factors Affecting Wound Healing
| Oxygenation | Poor oxygenation lowers cellular activity and mitotic rates, delaying healing. |
| Age | Older adults heal more slowly due to lower cellular activity. Adult females tend to heal faster than adult males. |
| Infection | Prolongs inflammation and delays healing. |
| Foreign material | Dirt, thorns, splinters, and debris delay healing, especially if not removed. |
| Underlying illness | Diabetes, cancer, and other systemic diseases delay healing. |
| Obesity | Chronic inflammation and reduced vascularity may delay healing. |
| Glucocorticoid Use | Slows healing due to immunosuppressive and catabolic effects. |
| NSAIDs / COX-2 drugs | Can increase scarring. |
| Chemotherapy | Reduces WBC proliferation, cell division, and angiogenesis – all delaying healing. |
| Nutrition deficits | Reduce proteins, carbohydrates, fats, vitamins, and minerals required for cellular activity and division. |
| Alcohol | Slows cellular activity, delaying healing |
| Smoking | Causes vasoconstriction, reducing oxygen and WBC delivery to the wound. |
Problems Associated with Scarring
| Loss of function | Scar tissue lacks hair follicles, sweat and sebaceous glands, and sensory nerve endings.
Non-regenerative tissues (heart, kidney, pancreas, brain, spinal cord, teeth, articular cartilage, eyes, ears) lose functional cells permanently. |
| Non-elasticity | Inelastic scar tissue limits range of motion.
Large burn wounds can cause contractures. Physiotherapy and surgery can partially offset this. |
| Adhesions | Bands of scar tissue between internal organs prevent normal movement (e.g., intestinal twisting and blockage). |
| Keloids | Raised hypertrophic scar tissue from excessive collagen production.
Strong genetic predisposition; more common in individuals with darker skin and on the upper chest and back. Reducible through surgery, laser, cryotherapy, or corticosteroid injection. |
| Ulceration | Scars impairing blood supply cause further tissue damage.
Very rarely, chronic wound scars can become cancerous ulcers. |



Media Attributions
- Private: tissue_healing © OpenStax College is licensed under a CC BY (Attribution) license
- Private: Burn_Degree_Diagram © Persian Poet Gal is licensed under a CC BY (Attribution) license
- Sunburn © Phil Kates is licensed under a CC BY-SA (Attribution ShareAlike) license
- 2nd Degree Burn © Erik Hmn is licensed under a CC BY-SA (Attribution ShareAlike) license
- Private: Skin_Graft_on_Ankle_after_Third_Degree_Burns © Giftrapped is licensed under a CC BY-SA (Attribution ShareAlike) license
- Private: Perihepatic_adhesions_2 © Hic et nunc is licensed under a Public Domain license
- Private: Keloid,_Post_Surgical © Dr. Michael H. Tirgan is licensed under a CC BY-SA (Attribution ShareAlike) license
- Private: Ear_Keloid-_Auricular_Keloid © Dr. Michael H. Tirgan is licensed under a CC BY-SA (Attribution ShareAlike) license

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}