Chapter 2 Innate and Adaptive Immunity: From Cell Defense to Tissue Repair
Section 2: White Blood Cells – Types and Roles
Zoë Soon
Hematopoiesis: Formation of Blood Cells
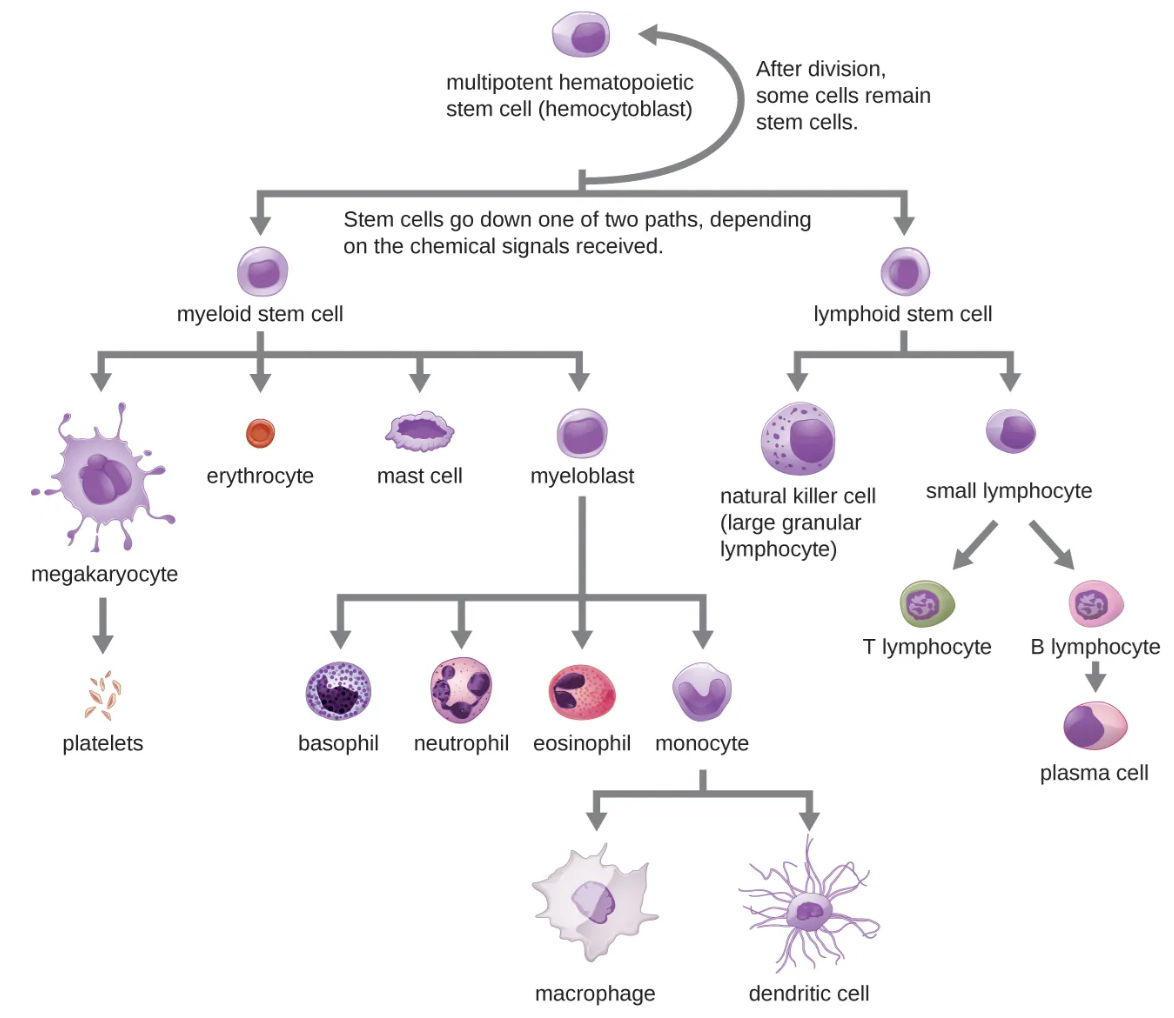
Hematopoiesis is the formation of blood cells. Production begins at day 7 of the embryonic life in the yolk sac, migrates to the liver and spleen at week 7, and moves to the bone marrow at ~week 20. The pluripotent stem cells giving rise to all blood cell types are called hemocytoblasts. Their daughter cells differentiate into erythrocytes (RBCs), megakaryocytes (platelet precursors), and leukocytes (WBCs).
Red Blood Cells (Erythrocytes)
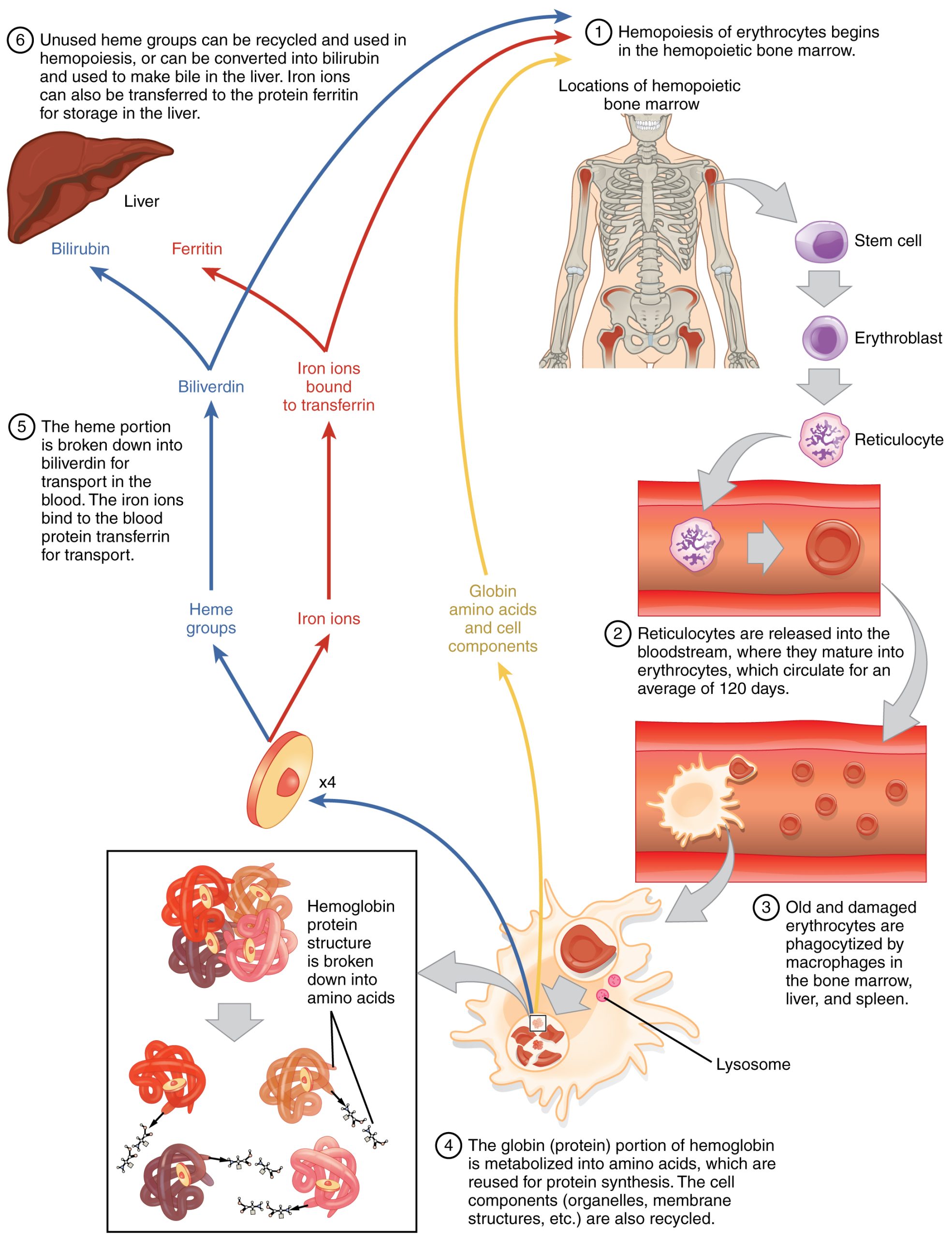
Erythropoiesis is the production of RBCs. Developing erythroblasts become increasingly packed with hemoglobin. At the normoblast stage, they lose their nucleus, become reticulocytes, enter the bloodstream 2-3 days later and mature into erythrocytes over the following 2 days. Main function: use hemoglobin to transport 98.5% of the oxygen and ~23% of the carbon dioxide in blood. Lifespan ~120 days; aged cells are recycled by macrophages in the liver, bone marrow, and spleen.
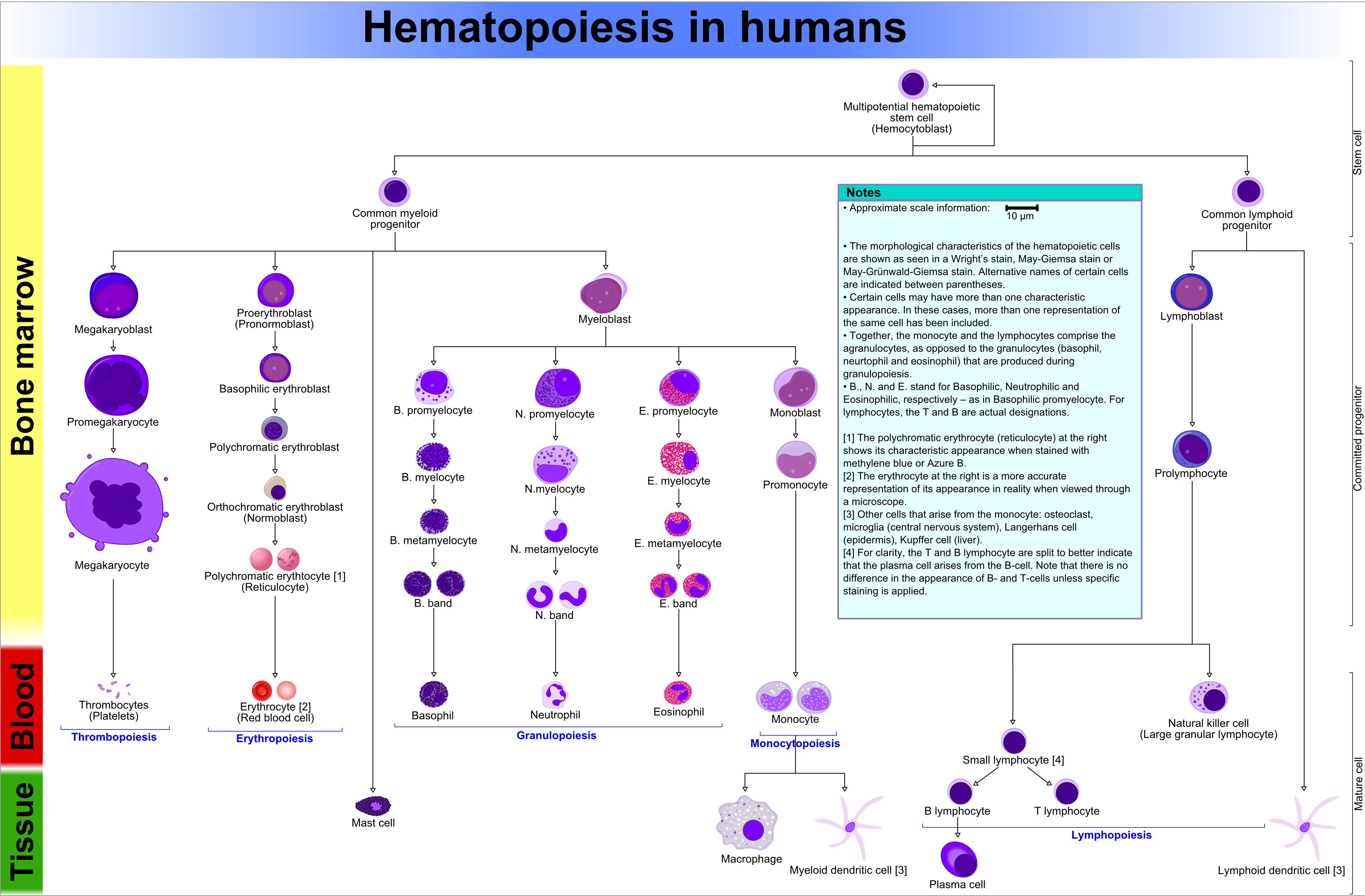
![Erythropoiesis: begins with hemocytoblasts producing proerythroblasts that mature into erythroblasts → normoblasts reticulocytes erythrocytes. [1] In this diagram, the reticulocyte on the right shows characteristics when stained with methylene blue. [2] The erythrocyte on the right represents its appearance under a light microscope.](https://pressbooks.bccampus.ca/pathophysiology/wp-content/uploads/sites/1961/2026/06/Hematopoiesis_human_diagram-cropped.png)
[1] In this diagram, the reticulocyte on the right shows characteristics when stained with methylene blue.
[2] The erythrocyte on the right represents its appearance under a light microscope.
Erythropoiesis is regulated by erythropoietin (EPO) hormone, secreted by the kidneys in response to low blood-oxygen levels, growth hormone (GH), thyroxine, and testosterone. In an adult, 2-3 million RBCs are produced per second and RBC production requires B vitamins, folate, amino acids and iron.
Diagnostic Blood Tests
Blood Count Terminology
| Retic count | Proportion of RBCs that are reticulocytes (normal: 1-2%).
Low retic count (e.g., 0.5%) indicates reduced erythropoiesis. |
| Hematocrit | Percentage of blood volume made up of formed elements.
Females ~42%; Males ~46% (testosterone stimulates RBC production). |
| Leukopenia | Reduced WBC production. |
| Thrombocytopenia | Reduced platelet production. |
| Neutrophilia | Elevated neutrophil count – common with bacterial infections. |
| Neutropenia | Decreased neutrophil count – caused by severe infection, nutritional deficiency, congenital defects, autoimmune disease, or cancer. |
| Eosinophilia | Elevated eosinophil count – caused by helminth infections, allergies, or autoimmune diseases. |
| Lymphocytosis | Elevated NK, T, and P lymphocytes count – occurs with viral infections. |
Platelets (Thrombocytes)
Megakaryocytes fragment into ~1,000 anuclear platelets (thrombocytes). Despite lacking a nucleus, platelet contain ~300 chemicals involved in hemostasis (blood clotting) and are essential for innate defense and preventing excessive bleeding.
White Blood Cell Lineages
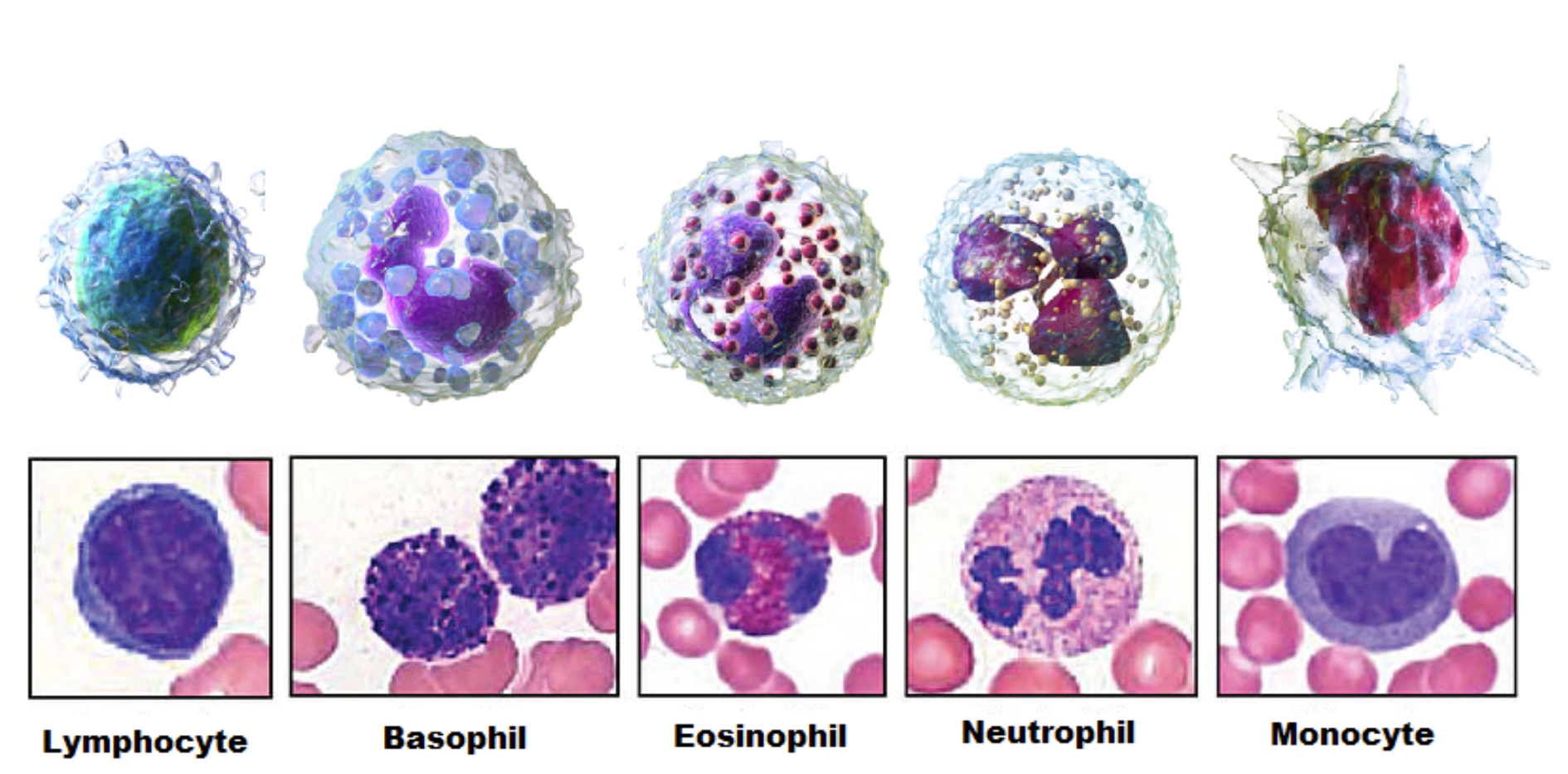
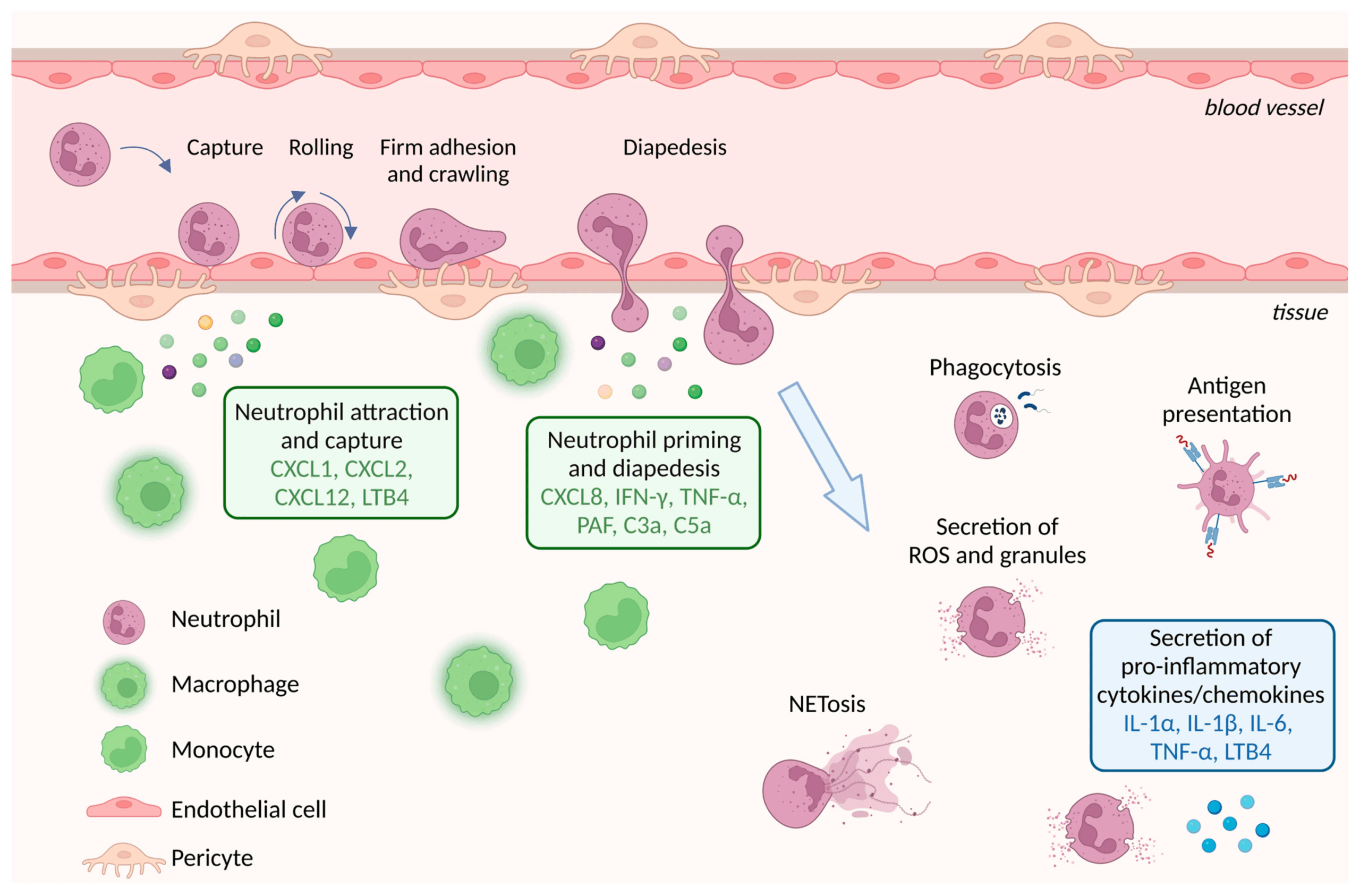
WBCs are classified as either granulocytes (containing large granules, readily visible with light microscope); also called polymorphonuclear leukocytes (PMNs) or agranulocytes (containing smaller granules). Granulocytes include: neutrophils, eosinophils, mast cells, and basophils. Agranulocytes include: monocytes, macrophages, dendritic cells, Natural Killer lymphocytes (NK cells), T lymphocytes (T cells), and B lymphocytes (B cells). All WBCs perform amoeboid movement and diapedesis (emigration from blood vessels into tissue – also termed extravasation or transmigration.
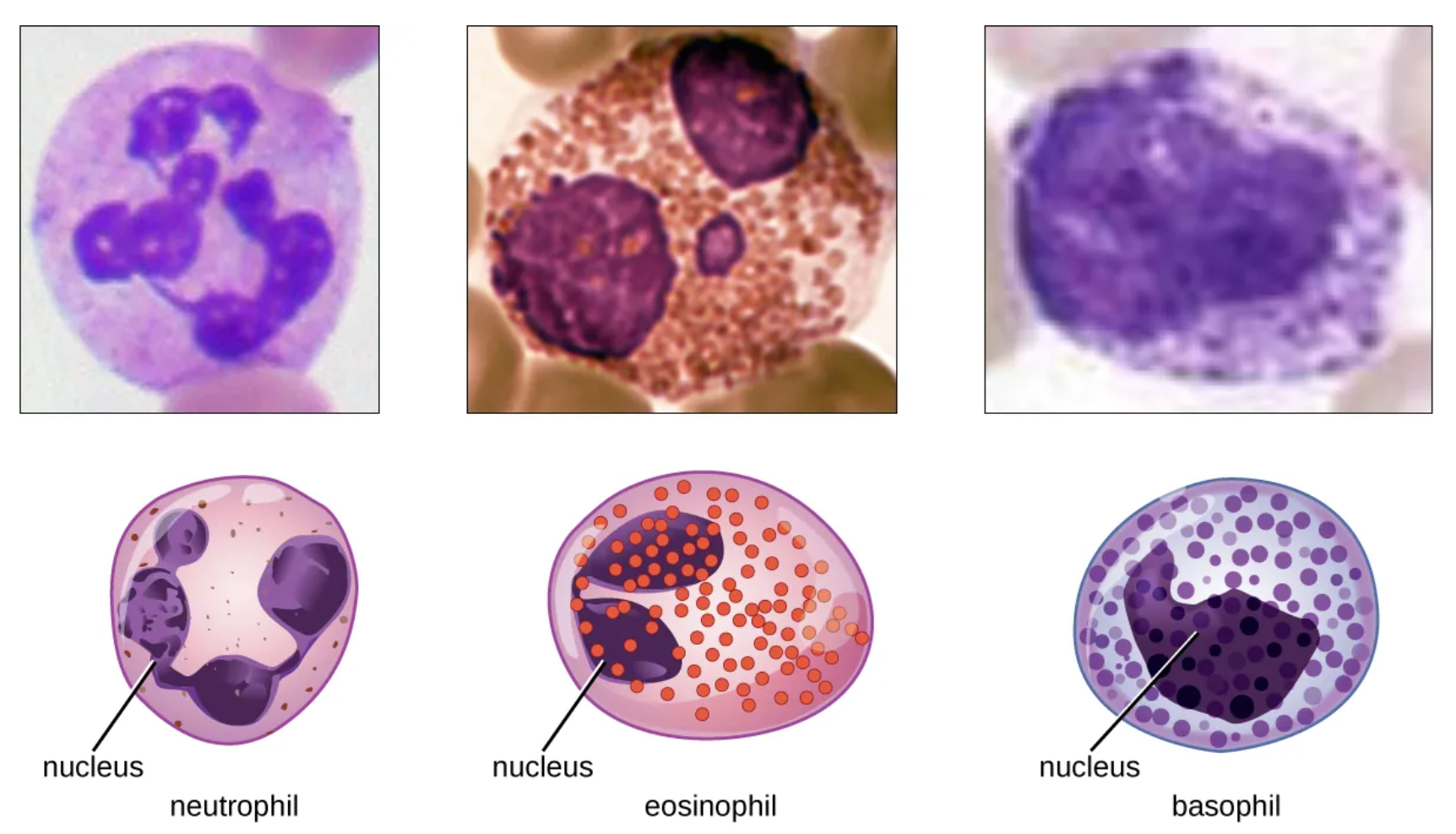
Granulocytes (Polymorphonuclear Leukocytes, PMNs)
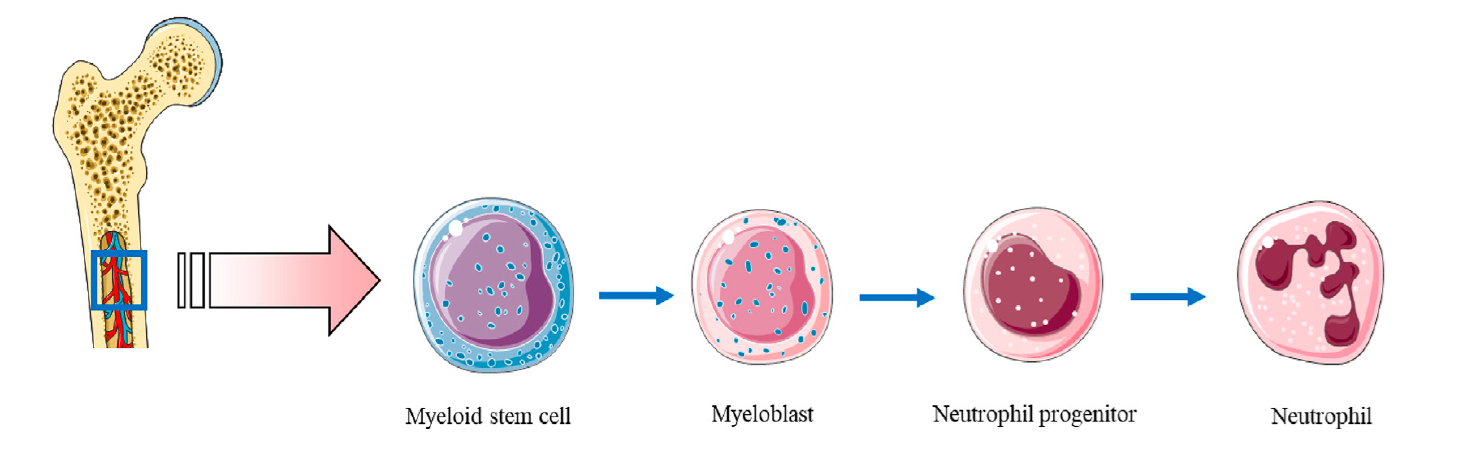
| Neutrophils | Immature band cells mature into neutrophils.
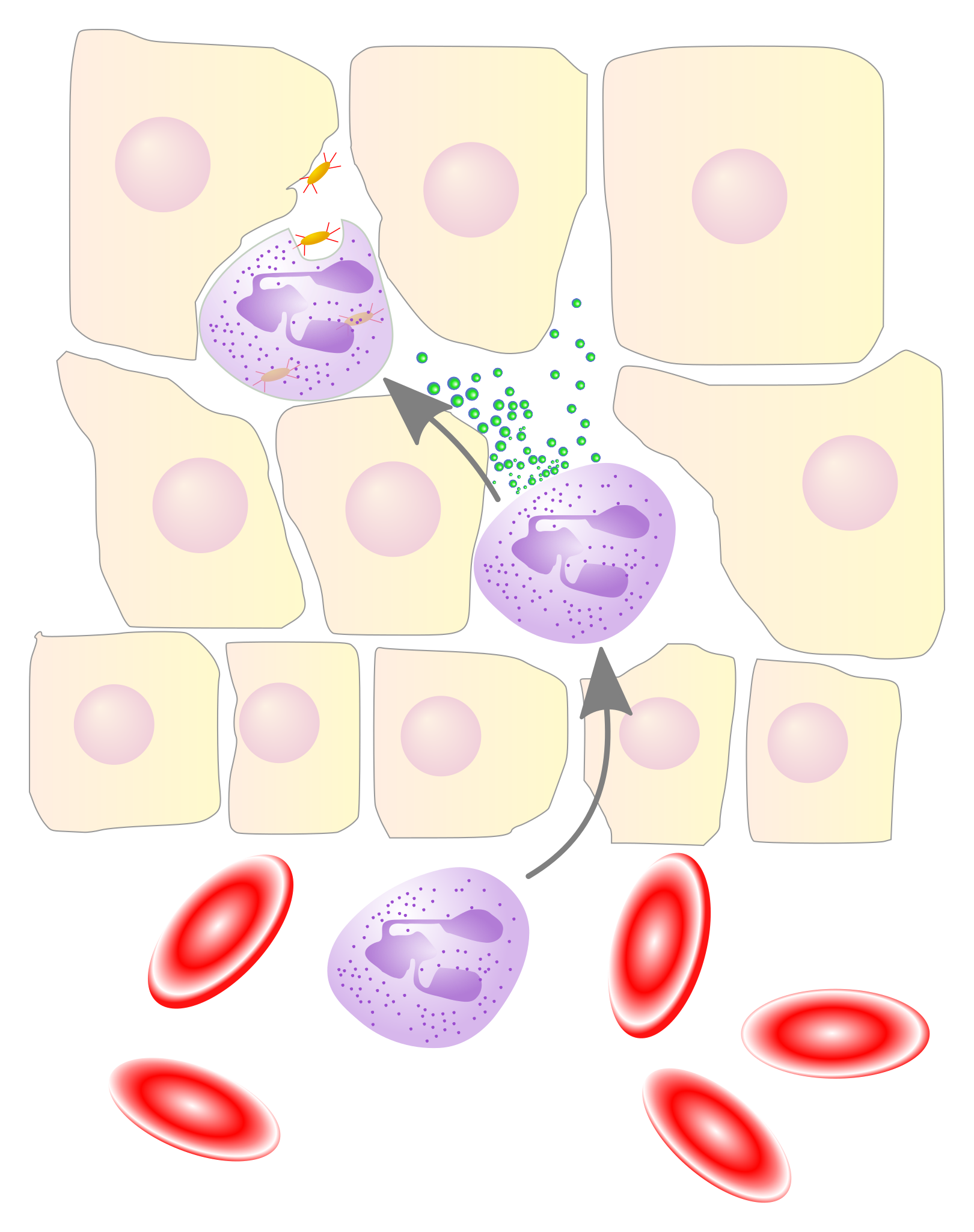
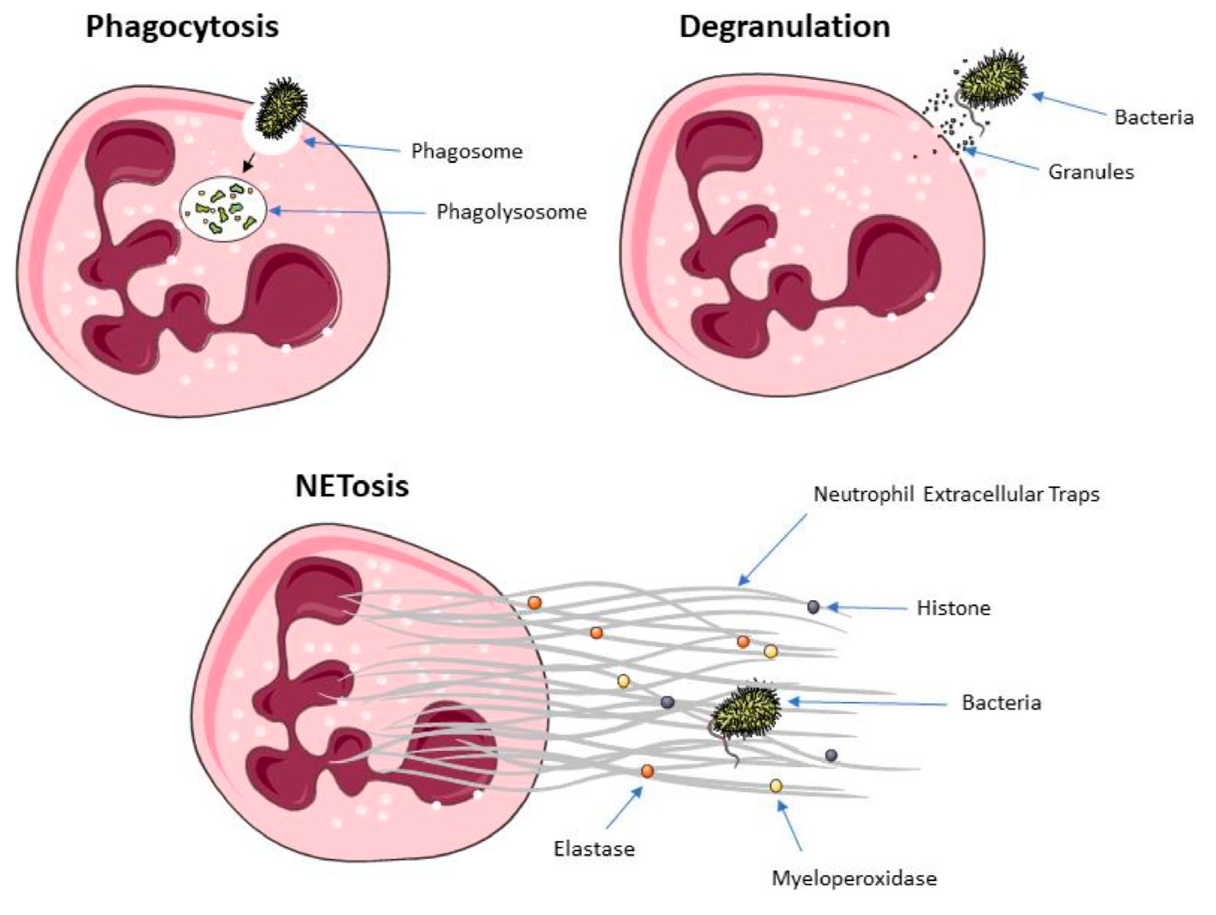
Most abundant WBC (50-70%). 2-5 lobed nucleus; stain neutral pink with H&E stain. First responders to sites of damage. Phagocytose bacteria and utilize extensive lysosomes. Neutrophil Oxidative Bursts exocytose highly toxic, unstable Reactive Oxygen Species (ROS) from secretory vesicles that damage bacterial cell walls. Neutrophil granules release lactoferrin (sequesters iron, depriving bacteria of required resource) Neutrophils release defensin and proteases (degrade pathogen) Can also release NETs (Neutrophil Extracellular Traps – webs of chromatin fibers and toxic enzymes) to trap and destroy microbes extracellularly. Active lifespan: 24-48 hours. |
| Eosinophils | Stain red with acidic eosin dye; ~2-3% of WBCs. Arrive 2-3 hours after neutrophils.
Phagocytose debris and pathogens. Exocytose toxins ROS, Eosinophil Cationic Protein (ECP), and Major Basic Protein (MBP) to kill organisms too large to phagocytose (e.g., helminths). Release cytokines to stimulate mast cell and basophil inflammatory response. Release growth factors (e.g., VEGF, vascular endothelial growth factor) to support healing. Release RNases to destroy viruses. Play a role in allergies and asthma |
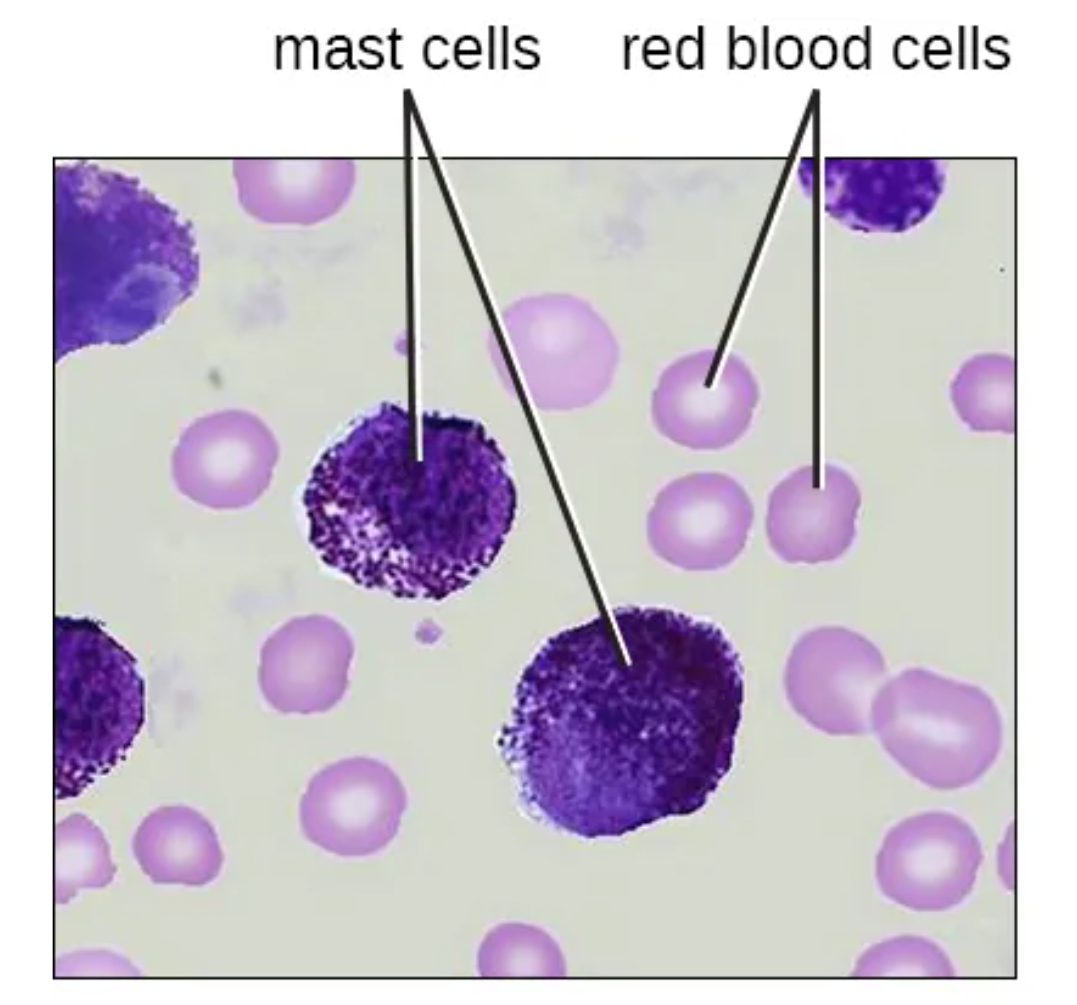
| Mast cells | Tissue-resident cells, most prevalent in skin dermis, lung mucosa, and GI tract mucosa.
Contain granules with heparin (anticoagulant) and histamine. Activated by cellular injury; degranulate releasing pro-inflammatory mediators (histamine, bradykinins, prostaglandins, leukotrienes). |
| Basophils | Circulating counterpart to mast cells. Both contain heparin and histamine granules and fulfill similar pro-inflammatory roles. Basophils circulate the bloodstream rather than residing in tissue. |
*ROS = Reactive Oxygen Species, such as superoxide, O2•− and hydroxyl radical HO• are free radicals with unpaired electrons that damage DNA, lipids and proteins.

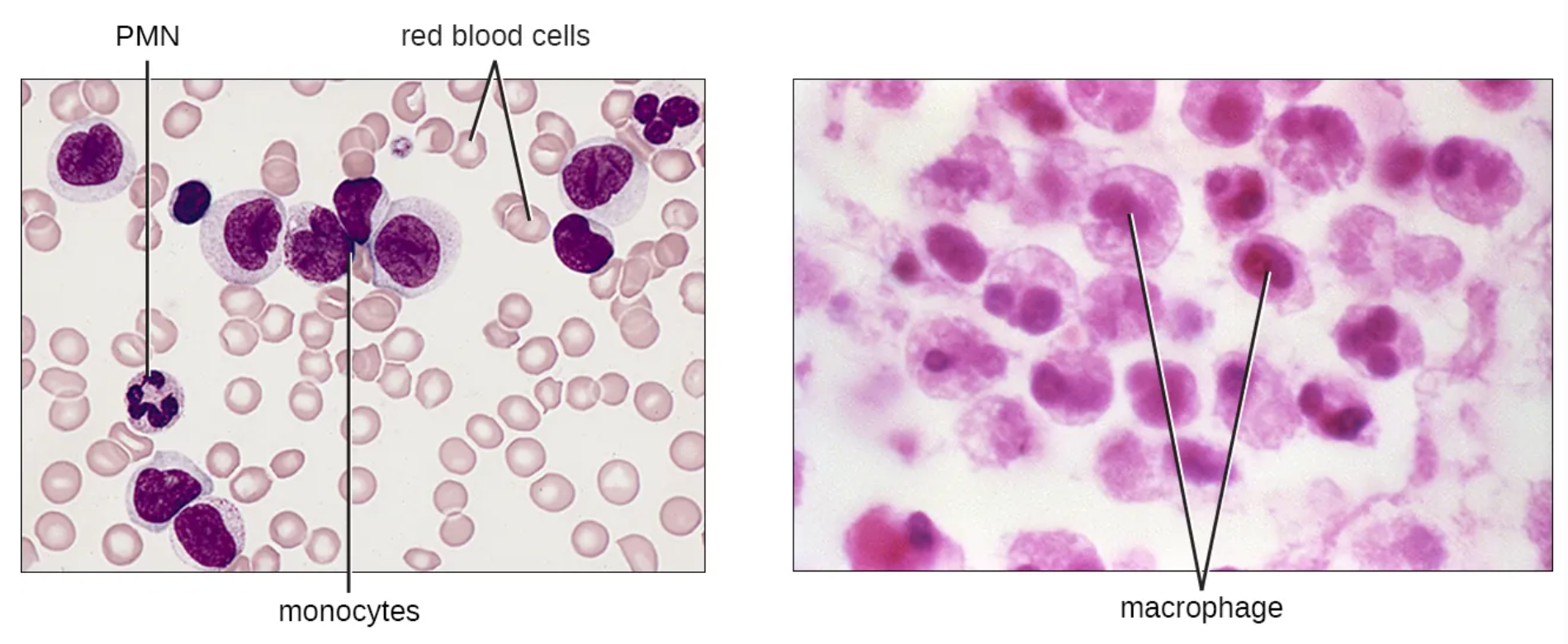
Agranulocytes: Monocytes, Macrophages, and Dendritic Cells
Monocytes are immature macrophages that mature within 1-3 days into fixed macrophages, free macrophages, or dendritic cells. Despite being immature, monocytes can phagocytose bacteria, secrete cytokines, and act as Antigen Presenting Cells (APCs).
| Fixed macrophages | Patrol tissue beds for debris, cancerous cells, and pathogens. Tissue-specific names: microglia (brain), dust cells (lung alveoli), Kupffer/stellate cells (liver), histiocytes (vertebrae), Langerhans cells (skin).
Splenic red pulp macrophages and liver macrophages recycle millions of RBCs daily in process called erythrophagocytosis. |
| Free macrophages | Circulate the bloodstream; enter tissue beds via diapedesis to remove bacteria, cellular debris, and aged neutrophils. |
| Dendritic cells | Reside in tissues exposed to microbes (skin, mucosa). Once activated, migrate to lymph nodes to function as APCs, stimulating T and B lymphocytes. |
Agranulocytes play important roles in phagocytosing bacteria, as well as secreting cytokines (glycoprotein messengers) to induce inflammation and recruit immune cells to the infected or damaged area. Additionally they release growth factors to promote tissue repair.
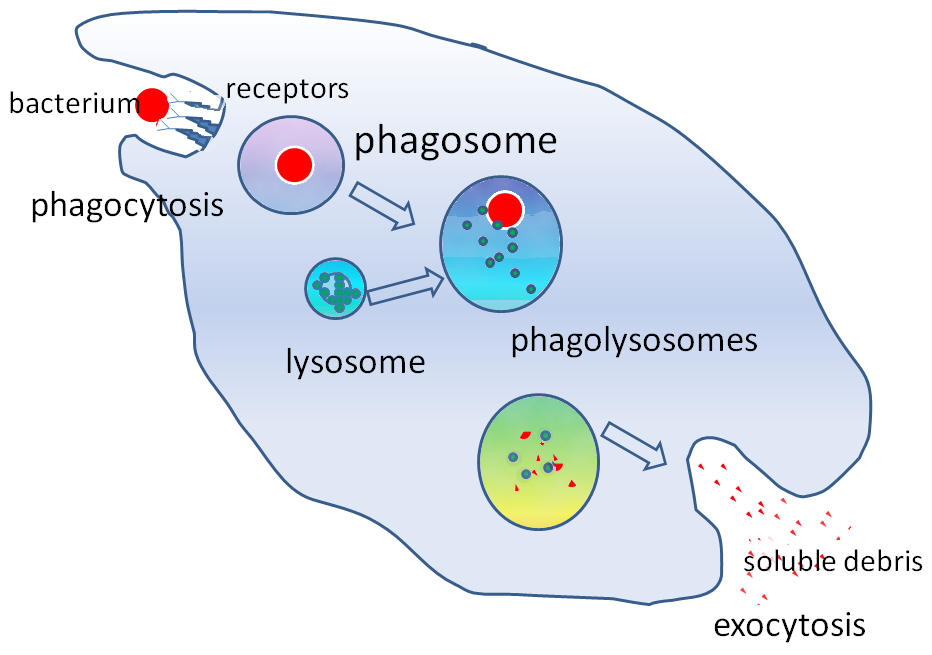
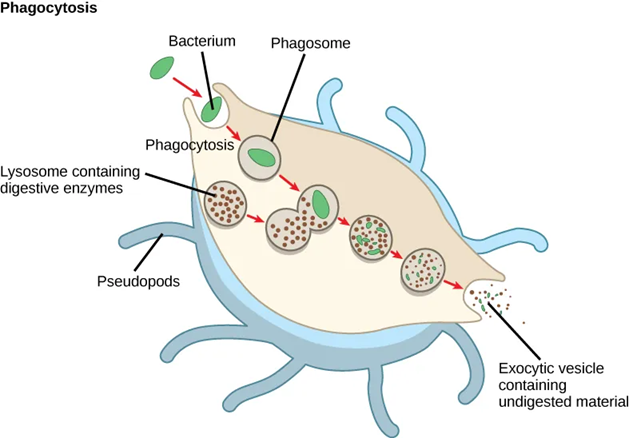
Steps of Phagocytosis
Phagocytes (neutrophils, monocytes, macrophages, dendritic cells, eosinophils) remove cellular debris and are able to provide non-specific defence by destroying pathogens through seven ordered steps:
- Activation: Pro-inflammatory cytokines activate the phagocyte, enabling pathogen recognition and production of antimicrobial ROS.
- Chemotaxis: Activated phagocytes follow chemokine gradients to the site of infection or injury.
- Recognition and Adherence: Opsonins (antibodies, lectin, complement proteins) coating the pathogen facilitate phagocyte binding when direct adherence is blocked (e.g., by a bacterial slime capsule).
- Ingestion: The phagocyte extends pseudopods that encircle the pathogen, forming an internal vesicle called a phagosome.
- Killing and Recycling: The phagosome fuses with a lysosome → phagolysosome. Lytic enzymes kill the pathogen and digest its components for recycling, display, or expulsion.
- Antigen Display: Pathogen antigens are coupled to MHC (Major Histocompatibility Complex) molecules and displayed on the phagocyte’s surface to activate T and B cells.
- Expulsion: Undigested components are expelled from the cell as waste via exocytosis.
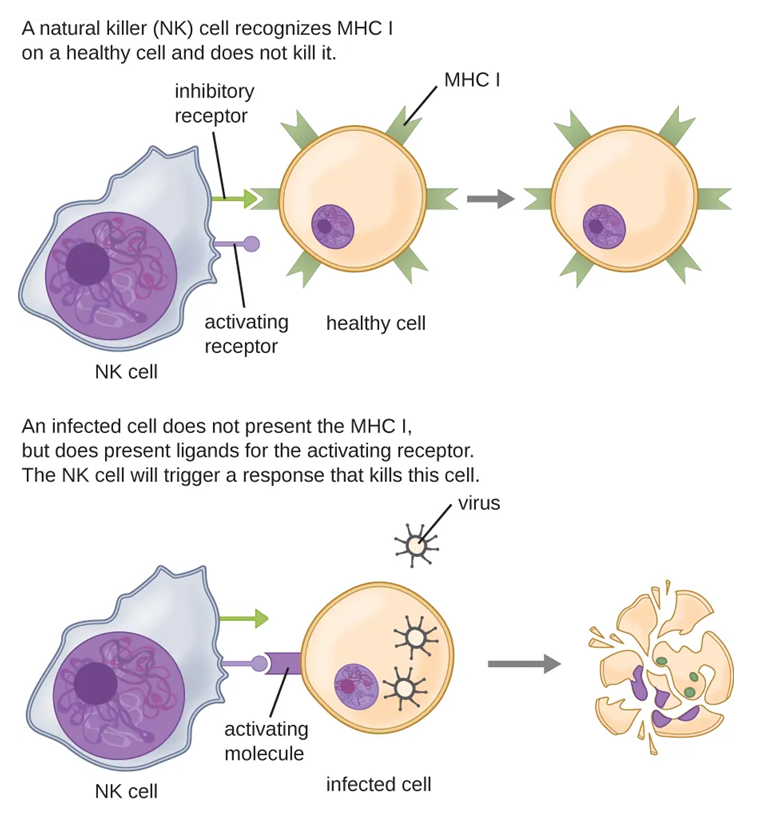
Agranulocytes: Natural Killer (NK) Cells
Natural Killer (NK ) cells are lymphocytes providing non-specific defense. NK lymphocytes are cytotoxic (able to kill other cells) and make up 5-20% of lymphocytes. NK cells recognize and destroy damaged, abnormal, cancerous, virally-or bacterially-infected cells, and extracellular pathogens.
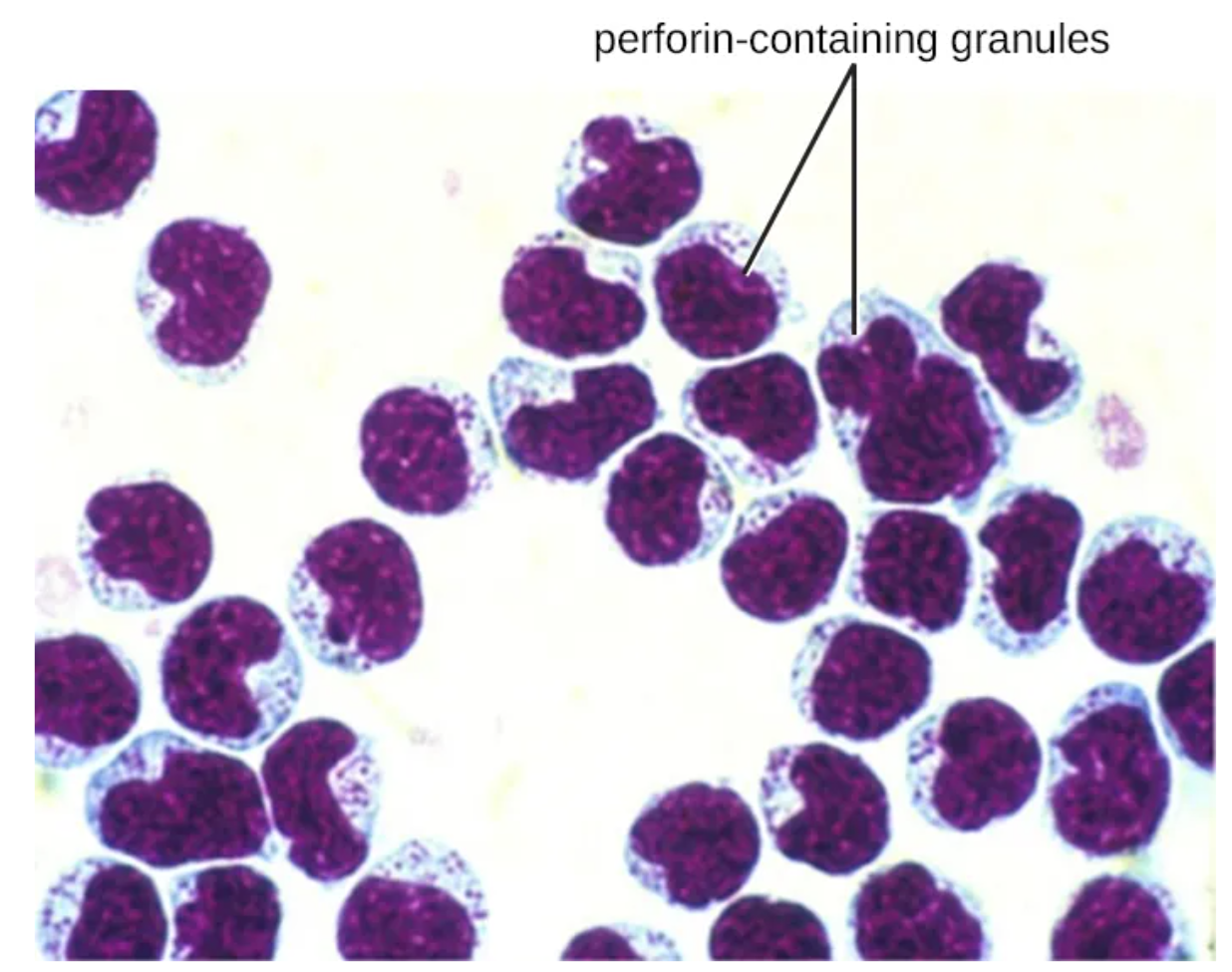
NK cells contain granules of perforin (pore-forming proteins) and granzymes (proteases) that are degranulated near a target cell. Perforin creates portals in the target membrane that if released in high concentration without granzyme can cause a cell to leak in fluid and lyse; though often granzyme are released at the same time and quickly enter the pores and induce apoptosis. Crucially, NK cells prefer inducing apoptosis in virally-infected cells rather than lysing them – preventing newly formed virions from escaping into surrounding tissue.
NK cells also release alpha-defensins (damaging bacterial cell walls, fungi, and enveloped viruses) and pro-inflammatory cytokines to activate other WBCs. Together with macrophages, NK cells recycle senescent cells (cells that have stopped replicating and are at risk of DNA damage due to age).
Clinical Note: Cancer and Immune Evasion
Cancerous cells or pathogens that evade NK cells can spread through tissue, blood, or lymph, potentially creating damage in multiple locations. Understanding how pathogens and cancers evade innate immunity is a major area of current research.
Media Attributions
- Hemopoiesis © Nina Parker, Mark Schneegurt, Anh-Hue Thi Tu, Philip Lister, Brian M. Forster is licensed under a CC BY-NC-SA (Attribution NonCommercial ShareAlike) license
- Hematopoiesis_(human)_diagram cropped © A. Rad is licensed under a CC BY-SA (Attribution ShareAlike) license
- 1905_Erythrocyte_Life_Cycle © Open Stax Anatomy and Physiology is licensed under a CC BY (Attribution) license
- WBC key © Leukocytes by Suzanne Wakim licensed CC BY 4.0 adapted from: White Blood Cells, CC BY 3.0, Blausen.com staff (2014). "Medical gallery of Blausen Medical 2014". WikiJournal of Medicine 1 (2). DOI:10.15347/wjm/2014.010. ISSN 2002-4436. Leukocyte Key by OpenStax College, CC BY 3.0 via Wikimedia Commons is licensed under a CC BY-NC-SA (Attribution NonCommercial ShareAlike) license
- Blood Cells © Mary Ann Clark, Matthew Douglas, Jung Choi is licensed under a CC BY-NC-SA (Attribution NonCommercial ShareAlike) license
- Neutrophil production © Gierlikowska, B., Gierlikowki, W., Stachura, A., Demkow, U. is licensed under a CC BY (Attribution) license
- Private: Neutrophil Granulocyte © Laboratoires Servier is licensed under a CC BY-SA (Attribution ShareAlike) license
- Private: NeutrophilerAktion.svg © Mario Schubert is licensed under a Public Domain license
- Neutrophil activity © Gierlikowska, B., Gierlikowki, W., Stachura, A., Demkow, U. is licensed under a CC BY (Attribution) license
- neutrophils-12-01981-g003 © Tsioumpekou, M., Krijgsman, D., Leusen, J. H. W., & Olofsen, P. A. (2023). The Role of Cytokines in Neutrophil Development, Tissue Homing, Function and Plasticity in Health and Disease. Cells, 12(15), 1981. is licensed under a CC BY (Attribution) license
- 3 granulocytes © Nina Parker, Mark Schneegurt, Anh-Hue Thi Tu, Philip Lister, Brian M. Forster (Image Credit: “neutrophil” micrograph: modification of work by Ed Uthman) is licensed under a CC BY-NC-SA (Attribution NonCommercial ShareAlike) license
- Mast Cells © Nina Parker, Mark Schneegurt, Anh-Hue Thi Tu, Philip Lister, Brian M. Forster is licensed under a CC BY-NC-SA (Attribution NonCommercial ShareAlike) license
- monocytes © Nina Parker, Mark Schneegurt, Anh-Hue Thi Tu, Philip Lister, Brian M. Forster (Image credit left: modification of work by Armed Forces Institute of Pathology; credit right: modification of work by Centers for Disease Control and Prevention) is licensed under a CC BY-NC-SA (Attribution NonCommercial ShareAlike) license
- Private: phagocytosis © By GrahamColm at English Wikipedia, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=6811745 is licensed under a CC BY-SA (Attribution ShareAlike) license
- Macrophage Phagocytosis © Mary Ann Clark, Matthew Douglas, Jung Choi is licensed under a CC BY-NC-SA (Attribution NonCommercial ShareAlike) license
- NK cell perforin granzyme © Nina Parker, Mark Schneegurt, Anh-Hue Thi Tu, Philip Lister, Brian M. Forster
- perforin granzyme © Nina Parker, Mark Schneegurt, Anh-Hue Thi Tu, Philip Lister, Brian M. Forster (Image credit: modification of work by Rolstad B) is licensed under a CC BY-NC-SA (Attribution NonCommercial ShareAlike) license

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}