Chapter 2 Innate and Adaptive Immunity: From Cell Defense to Tissue Repair
Section 13: Anti-Inflammatory, Analgesic, and Antipyretic Therapies
Zoë Soon
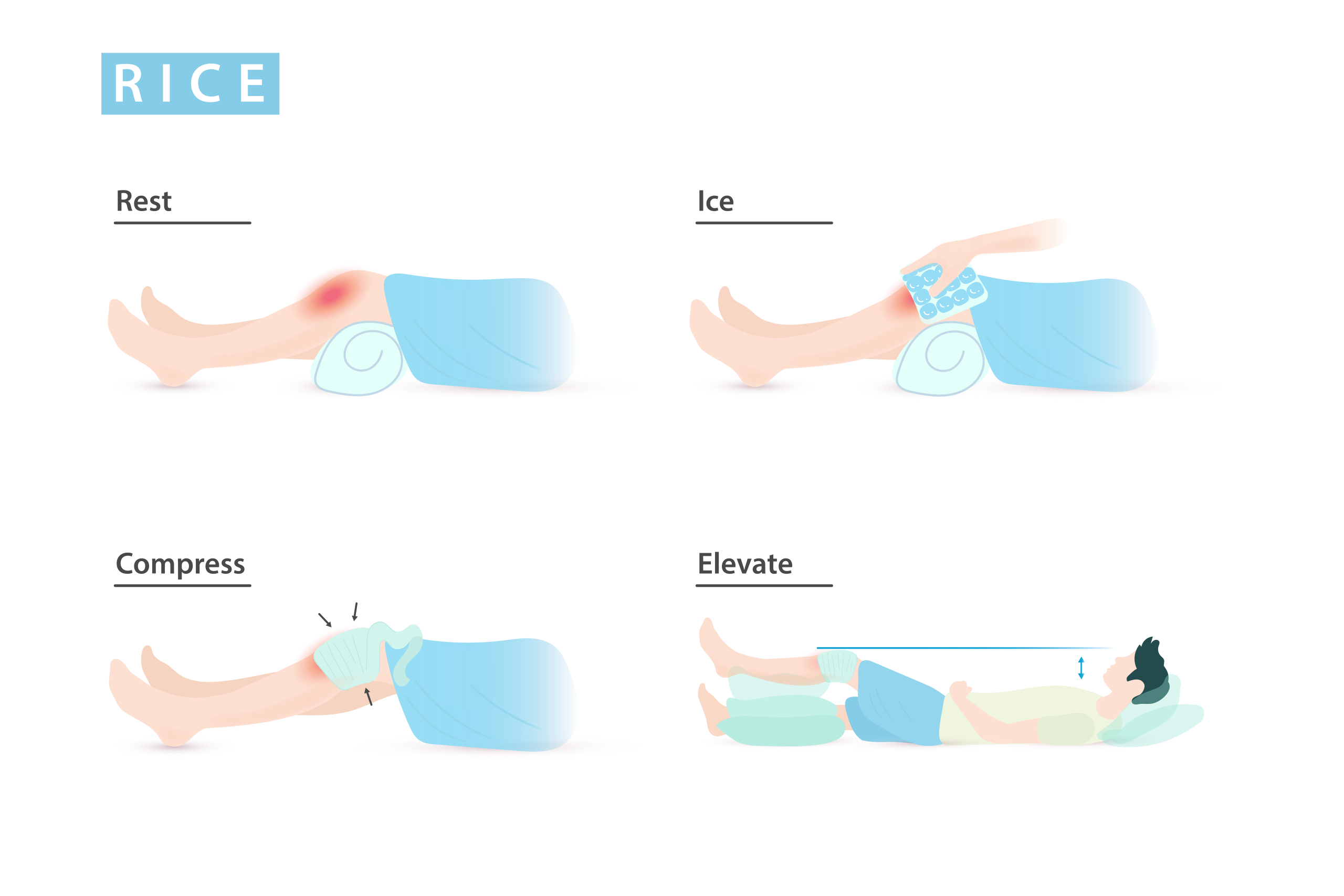
PRICE Therapy
PRICE is a non-pharmacological first-line approach to inflammation and pain from minor injuries:
| P = Protection | Protect the damaged area from further injury (e.g., splint, cast, crutches) |
| R = Rest | Reduces blood flow, limiting inflammation.
Temporary rest is recommended; prolonged rest however may delay functional recovery. |
| I = Ice | Induces vasoconstriction, reducing exudate leakage and swelling.
Also depresses nerve activity, reducing pain. |
| C = Compression | Stops external bleeding and limits exudate accumulation and swelling. |
| E = Elevation | Drains excess fluid away from the damaged area, reducing swelling. |
*For muscle or joint injuries, alternating warm and cold compresses is often advised – heat improves circulation to remove excess fluid, pain-causing chemicals and cellular waste; cold reduces acute swelling and depresses nociceptors. Adequate nutrition and hydration support optimal healing.
Pharmacological Treatments: How They Work
Mast cells and basophils convert phospholipids → arachidonic acid → prostaglandins using cyclooxygenase enzymes (COX-1 and COX-2). Prostaglandins stimulate nociceptors to induce pain and also trigger blood vessels to vasodilate and increase in permeability as part of the inflammatory response. Many analgesics and most anti-inflammatory drugs therefore target this pathway:
| ASA (Aspirin) – NSAID | Blocks COX-1 and COX-2 → reduces production of many different prostaglandins
Pros: Reduces pro-inflammatory prostaglandins → reduces inflammation, pain, and fever. Cons of long-term use:
At low doses, sometimes prescribed to reduce clotting risk. Caution: Never give to children/teenagers with viral infection – risk of Reye’s syndrome (potentially fatal liver and brain damage). |
| Acetaminophen (Tylenol) | Blocks part of the COX-2 downstream pathway, reducing prostaglandin E2 → reduces fever and pain, but not inflammation.
Must be taken as directed to avoid liver and kidney damage. Can be an allergen. |
| NSAIDs (Ibuprofen, Advil) | Block COX-1 and COX-2 (less COX-1 blockade than ASA) → reduce pro-inflammatory prostaglandins → decrease inflammation, fever, and pain.
Not linked to Reye’s syndrome, less gastric irritation, and less effect on platelet function than ASA. |
| COX-2 Selective Drugs (Celecoxib) | Preferentially block COX-2, targeting pro-inflammatory prostaglandins while sparing COX-1 (which produces protective gastric prostaglandins). An effective analgesic, anti-inflammatory and anti-pyretic.
Fewer side effects than ASA. |
| Glucocorticoids (Corticosteroids) | Immunosuppressive and anti-inflammatory: reduce WBC migration, proliferation, and activity; decrease production of pro-inflammatory mediators, vasodilation, capillary permeability, and swelling.
Not analgesics or antipyretics. Side effects:
|


Narcotics vs. Non-Narcotics: An Important Distinction
The drugs above (ASA, acetaminophen, NSAIDs, glucocorticoids) are not narcotics (opioids such as morphine, heroin, fentanyl). Non-narcotic analgesics do not induce narcosis (sleep), are not linked with physical dependence, and do not carry the risks of addiction, increasing tolerance, sedation, depressed heart and breathing rates, or potentially fatal substance abuse that characterize opioids. Narcotics are responsible for the ongoing opioid crisis in North America .
Media Attributions
- Private: RICE © Injurymap is licensed under a CC BY (Attribution) license
- Private: Paracetamol_acetaminophen_500_mg_pills © Michelle Tribe is licensed under a CC BY (Attribution) license
- Private: 512px-Dexamethasone_tablets © Mx. Granger is licensed under a Public Domain license

{kind=link}
{kind=link}