Chapter 2 Innate and Adaptive Immunity: From Cell Defense to Tissue Repair
Section 4: The Inflammatory Response
Zoë Soon
Inflammation is a protective response triggered by any type of cellular damage or irritation – cuts, burns, infections, sprains, ischemia, chemicals, foreign objects, extreme heat or cold. It facilitates removal of harmful agents, limits damage, and sets the stage for healing.
How Inflammatory Is Initiated
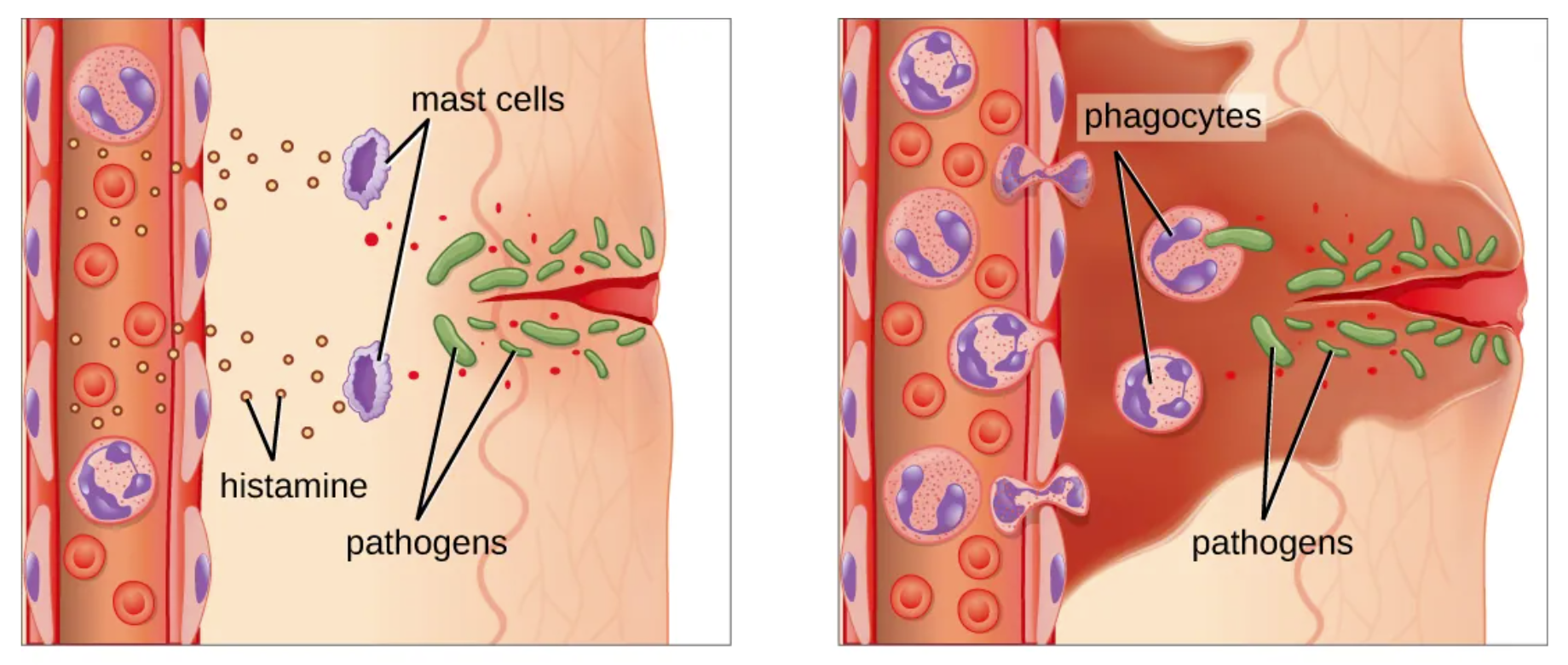
When cells are damaged they release contents (ADP, K+, proteins, enzymes) and cytokines that activate macrophages and mast cells. Macrophages phagocytose debris and pathogens and release chemokines to recruit other WBCs. Mast cells degranulate, releasing histamine, bradykinin, and prostaglandin, which cause:
- Vasodilation: local blood vessels dilate, increasing blood flow to the area.
- Increased capillary permeability: plasma fluid (exudate) leaks from capillaries into the damaged tissue bed.
- WBC diapedesis: endothelial cells of the blood vessel walls express adhesion molecules facilitating rolling, adhesion, and transmigration of WBCs into tissue.
The leaked exudate contains fibrinogen, complement proteins, C-reactive proteins, and platelets. Fibrin mesh and clots help contain the damaged area. Chemokines recruit neutrophils, monocytes, macrophages, dendritic cells, eosinophils, and basophils. WBCs also secrete growth factors to stimulate tissue repair once the area is cleared.
Two Phases of Inflammation
| Vascular phase | Vasodilation and increased capillary permeability occur within local blood vessels. |
| Cellular phase | Emigration (diapedesis/transmigration) of WBCs from blood into the tissue bed occurs. |
The Five Signs of Inflammation
| Redness | Hyperemia (increased blood flow) to the area due to vasodilation. |
| Warmth | Blood (37°C) is slightly warmer than surface tissues; increased perfusion warms the area. |
| Swelling | Exudate accumulates in interstitial spaces due to increased capillary permeability.
When substantial this is called edema. |
| Pain | Nociceptors (pain sensory receptors) are stimulated by prostaglandins, bradykinin, leukotriene, leaked blood, extracellular ATP, and exudate pressure.
Histamine activates a nociceptor subtype producing itching. |
| Loss of Function (sometimes) | Swelling or pain impedes joint or muscle movement.
Exudate in lung alveoli or interstitial spaces impairs gas exchange. Swelling in the esophagus impairs swallowing. |
Vasoactive Compounds in Inflammation
Several key pro-inflammatory mediators are classified as vasoactive compounds (they all change blood vessel diameter):
- Histamine: Nitrogenous compound released by mast cells, basophils, and platelets.
- Bradykinin: Peptide activated by enzymatic cleavage of its kininogen precursor.
- Prostaglandin: Lipid mediator released by mast cells, basophils, macrophages, and activated platelets.
- Leukotrienes: Lipid mediators produced by mast cells, basophils, neutrophils, monocytes, and eosinophils. A potent bronchoconstrictor in asthma; also a vasodilator increasing capillary permeability.
All four compounds induce vasodilation, increase capillary permeability, cause bronchoconstriction, stimulate mucus production and trigger WBC chemotaxis.
Bradykinin, prostaglandin, and leukotriene also stimulate nociceptors, contributing to the pain of inflammation. Histamine stimulates itch (pruritus) especially during allergic reactions.
Side note: Interestingly, itch and pain do share overlapping neuronal pathways and sharp pressure can temporarily override the itch sensation. However, the withdrawal neural reflex arc for pain differs from the scratching reflex for itch (which can damage the skin).
Four Types of Exudate
| Serous | Watery, containing some proteins and WBCs. Found in unruptured burn blisters. |
| Fibrinous | Thick, sticky, contains fibrin; associate with severe injuries and infections.
Linked to increased scar tissue formation. |
| Purulent | Thick, yellow-green; contains WBCs and microorganisms.
Seen in bacterially-infected abscesses and acne. Contains pus – a protein-rich fluid of dead cells and debris. |
| Hemorrhagic | Contains blood from damaged blood vessels. |

Systemic Effects of Inflammation
Pro-inflammatory cytokines circulate the whole body, causing systemic effects; mild fever, malaise, fatigue, headache, loss of appetite, and – particularly in the elderly – decreased mental function.
When Inflammation Goes Wrong: Too Little or Too Much
Too little inflammation: In immunosuppressive diseases, insufficient inflammation allows prolonged tissue damage, infection, and potentially permanent tissue loss.
Too much inflammation: Chronic conditions such as atherosclerosis, diabetes, osteoarthritis, autoimmune diseases, allergies, and asthma drive prolonged inflammatory responses. Excessive WBC activity leads to cycles of tissue destruction and healing, causing progressive damage.
Systemic Inflammatory Response Syndrome (SIRS): A potentially fatal condition caused by a “cytokine storm”, a massive pro-inflammatory cytokine release. Results in systemic vasodilation and increased capillary permeability → hypotension and circulatory shock. Most frequently caused by sepsis (dysregulated immune response to infection).
Fever of Unknown Origin (FUO): Thought to be caused by inflammatory responses to undetectable cellular damage – from infections, trauma, cancer, heart attacks, blood clots, inflammatory diseases, or drug reactions.
Media Attributions
- Mast Cells Inflammation © Nina Parker, Mark Schneegurt, Anh-Hue Thi Tu, Philip Lister, Brian M. Forster is licensed under a CC BY-NC-SA (Attribution NonCommercial ShareAlike) license
- Private: Swollen_eye_with_conjunctivitis © Tanalai, Wikipedia Commons is licensed under a CC BY (Attribution) license

{kind=link}