Diabetes Mellitus
Gestational Diabetes
Jennifer Kong
Learning Objectives
By the end of this section, you will be able to:
- Identify some risk factors of developing gestational diabetes mellitus.
- Identify the manifestations of gestational mellitus.
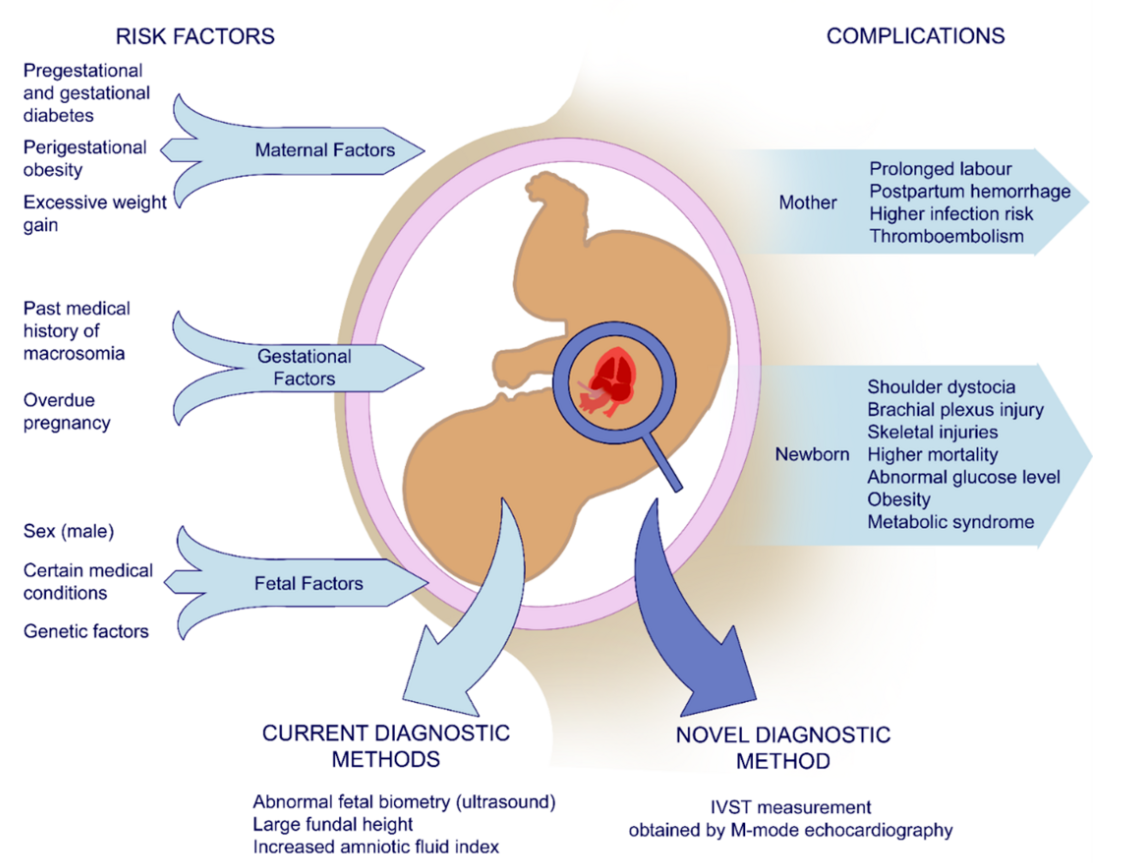
Gestational diabetes mellitus is similar to T2DM, except that it is associated with pregnancy. As such, it often resolves shortly before or after birth. As the fetus grows, its demands for tissue growth causes a similar increased demand for both insulin and circulating nutrients. In conjunction with hormones associated with pregnancy, the mother’s cells can’t use its own insulin effectively causing a temporary insulin resistance. In fact, all pregnant women have some level of insulin resistance during late pregnancy, but not necessarily diagnosable gestational diabetes. Thus, many of the mother’s symptoms overlap T2DM: hyperglycemia, polyuria, polydipsia (thirst), and polyphagia (hunger).
There is an association between gestational diabetes and pregnancy-induced high blood pressure (gestational hypertension). The mechanism is not well understood. However, if the mother already has diabetes-induced changes in microvasculature, the risk of developing gestational hypertension is greater.
The baby receives all of the mother’s nutrients and insulin. Because insulin is an anabolic hormone (i.e. builds tissues), babies of mothers with gestational diabetes will tend to be larger than average. Because of the high amount of circulating insulin in utero, the baby may have sudden hypoglycemia upon birth as that insulin makes the tissues take up the circulating glucose even though maternal supply has been cut off.
Pregnancy is the biggest risk factor for gestational diabetes. However, if the mother has risk factors for T2DM as well, the mother is more likely to develop gestational diabetes.
Section Review
Gestational diabetes is caused by pregnancy which causes an abundance of insulin and nutrients circulating in the maternal blood. As such, maternal tissues become resistant to insulin – akin to a temporary form of T2DM which resolves in the mother upon birth. Maternal symptoms would be excessive thirst and urination. The baby exposed to high levels of nutrient and insulin may be large and have temporary hypoglycemia (due to maternal hyperinsulinemia).
Review Questions
1. Pregnancy is a risk factor for gestational diabetes mellitus and is developed in the fetus.
- True
- False
2. Fill in the blanks.
Some possible clinical manifestations for gestational diabetes mellitus are _____.
3. Which of the following can occur as a clinical manifestation of gestational diabetes mellitus?
- Baby is greater than 9 lb during delivery
- Baby is likely to develop T1DM later in life
- All of the above
Answer Key
- False
- Higher than normal sugar, sugar/glucose in urine, high blood pressure
- Baby is greater than 9 lb during delivery
Media Attributions
- gestational diabetes © Szmyd et al. is licensed under a CC BY (Attribution) license

{kind=link}