Diabetes Mellitus
Anatomy of the Pancreas and Glucose Homeostasis
J. Gordon Betts; Kelly A. Young; James A. Wise; Eddie Johnson; Brandon Poe; Dean H. Kruse; Oksana Korol; Jody E. Johnson; Mark Womble; and Peter DeSaix
Learning Objectives
By the end of this section, you will be able to:
- Describe the location and structure of the pancreas, and the morphology and function of the pancreatic islets.
- Compare and contrast the functions of insulin and glucagon.
The pancreas is a long, slender organ, most of which is located posterior to the bottom half of the stomach, as shown in the figure below. Although it is primarily an exocrine gland, secreting a variety of digestive enzymes, the pancreas also has endocrine function. Pancreatic islets—clusters of cells formerly known as the islets of Langerhans—secrete the hormones glucagon, insulin, somatostatin, and pancreatic polypeptide (PP).
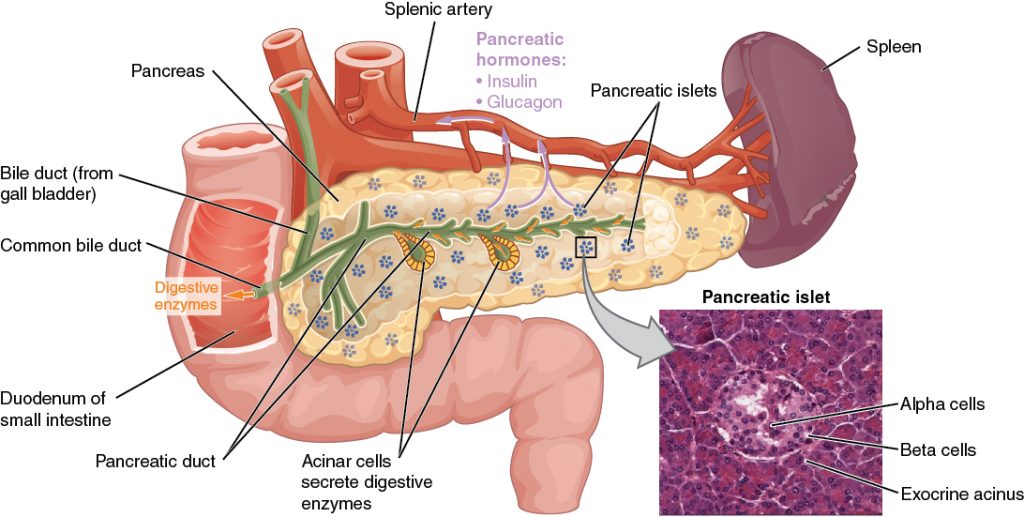
Cells and Secretions of the Pancreatic Islets
The pancreatic islets each contain four varieties of cells:
- Alpha (α) cell produces the hormone glucagon and makes up approximately 20 percent of each islet. Low blood glucose levels stimulate glucagon release.
- Beta (β) cell produces the hormone insulin and makes up approximately 75 percent of each islet. Elevated blood glucose levels stimulate the release of insulin.
- Delta (δ) cell accounts for four percent of the islet cells and secretes the hormone somatostatin. Recall that somatostatin is also released by the hypothalamus (as GHIH), stomach and intestines. Pancreatic somatostatin inhibits the release of both glucagon and insulin.
- PP cell accounts for about one percent of islet cells and secretes the pancreatic polypeptide (PP) hormone. This hormone is thought to play a role in appetite, as well as in the regulation of pancreatic exocrine and endocrine secretions. PP release following a meal may reduce further food consumption; however, it is also released in response to fasting.
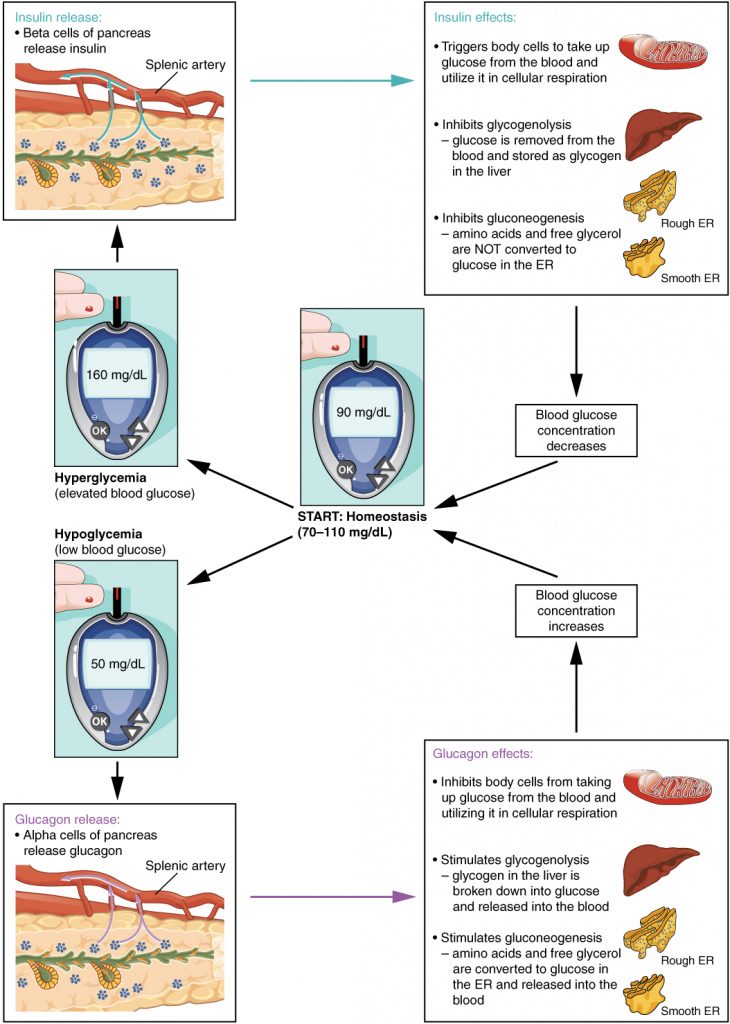
Regulation of Blood Glucose Levels by Insulin and Glucagon
Glucose is required for ATP production in the process of cellular respiration and is the preferred fuel for all body cells. The body derives glucose from the breakdown of the carbohydrate-containing foods and drinks we consume. Glucose not immediately taken up by cells for fuel can be stored by the liver and muscles as glycogen, or converted to triglycerides and stored in the adipose tissue. Hormones regulate both the storage and the utilization of glucose as required. Cells in the pancreas sense glucose levels, and subsequently secrete glucagon or insulin to maintain normal levels.
For example, it is expected that high blood glucose levels (hyperglycemia) will occur after a meal. When an influx of blood glucose occurs, specific endocrine cells in the pancreas are the first to detect excess glucose in the bloodstream. Pancreatic beta cells then respond to the increased blood glucose by releasing the peptide hormone insulin into the bloodstream. Once bound to cell surface insulin receptors, insulin stimulates cells of the body to increase the number of glucose transporters present in their plasma membranes. This allows cells to uptake more glucose. Insulin also signals skeletal muscle fibers, fat cells (adipocytes), and liver cells to take up the excess glucose, removing it from the bloodstream. As glucose concentration in the bloodstream drops, this decrease is detected by pancreatic beta cells and stimulates a negative feedback loop, inhibiting insulin production and secretion. This prevents blood sugar levels from continuing to drop below the normal range.
Glucagon
The cells in the pancreatic islets also sense the decrease in blood glucose levels, such as during periods of fasting or during prolonged exercise. In response, the alpha cells of the pancreas secrete the hormone glucagon, which has several effects:
- It stimulates the liver to convert its stores of glycogen back into glucose (glycogenolysis). The glucose is then released into the circulation for use by body cells.
- It stimulates the liver to take up amino acids from the blood and convert them into glucose (gluconeogenesis).
- It stimulates lipolysis, the breakdown of stored triglycerides into free fatty acids and glycerol. Some of the free glycerol released into the bloodstream travels to the liver, where it is converted into glucose. This is also a form of gluconeogenesis.
Together, these actions increase blood glucose levels. The activity of glucagon is regulated through a negative feedback mechanism, where rising blood glucose levels inhibit further glucagon production and secretion.
Insulin
The primary function of insulin is to facilitate the uptake of glucose into body cells. Some tissues/cells, despite the presence of insulin receptors, do not require insulin to uptake glucose. This is the case of the brain, liver, kidneys and lining of small intestines. However, many body tissues require the presence of insulin to facilitate their uptake of glucose from the bloodstream. These main ones are the skeletal muscle and the adipose tissue.
The presence of food in the intestine triggers the release of gastrointestinal tract hormones such as glucose-dependent insulinotropic peptide (GIP) (previously known as gastric inhibitory peptide) and glucagon-like peptide 1 (GLP-1). This is the initial trigger for insulin production and secretion by the pancreatic beta cells. Once nutrient absorption occurs, the resulting surge in blood glucose levels further stimulates insulin secretion, as described above.
Insulin activates a tyrosine kinase receptor, triggering the phosphorylation of many substrates within the cell. These multiple biochemical reactions converge to support the movement of intracellular vesicles containing glucose transporters to the cell membrane. Therefore, insulin triggers the rapid movement of a pool of glucose transporter vesicles to the cell membrane, where they fuse and expose the glucose transporters to the extracellular fluid. The transporters then move glucose by facilitated diffusion into the cell interior. In the absence of insulin, these transport proteins are normally recycled slowly between the cell membrane and cytoplasm.

Insulin also reduces blood glucose levels by stimulating glycolysis, the metabolism of glucose for generation of ATP. Moreover, it stimulates the liver to convert excess glucose into glycogen for storage, and it inhibits enzymes involved in glycogenolysis and gluconeogenesis. Finally, insulin promotes triglyceride and protein synthesis, while inhibiting the breakdown of fat (lipolysis). The secretion of insulin is regulated through a negative feedback mechanism. As blood glucose levels decrease, insulin release is inhibited. The pancreatic hormones and their main effect in glucose homeostasis are summarized in the table below.
| Hormones of the Pancreas | ||
|---|---|---|
| Associated hormones | Chemical class | Effect |
| Insulin (beta cells) | Protein | Reduces blood glucose levels |
| Glucagon (alpha cells) | Protein | Increases blood glucose levels |
| Somatostatin (delta cells) | Protein | Inhibits insulin and glucagon release |
| Pancreatic polypeptide (PP cells) | Protein | Role in appetite |
Review Questions
Adaptation
This chapter is adapted from the following text:
Endocrine Pancreas in Anatomy and Physiology by OSCRiceUniversity is licensed under a Creative Commons Attribution 4.0 International License
Media Attributions
- 1820_The_Pancreas © OSCRiceUniversity is licensed under a CC BY (Attribution) license
- 1822_The_Homostatic_Regulation_of_Blood_Glucose_Levels © OSCRiceUniversity is licensed under a CC BY (Attribution) license
- insulin and glucose © Sarah Perkins is licensed under a CC BY-ND (Attribution NoDerivatives) license
organ with both exocrine and endocrine functions located posterior to the stomach that is important for digestion and the regulation of blood glucose
specialized clusters of pancreatic cells that have endocrine functions; also called islets of Langerhans
pancreatic islet cell type that produces the hormone glucagon
pancreatic islet cell type that produces the hormone insulin
minor cell type in the pancreas that secretes the hormone somatostatin
minor cell type in the pancreas that secretes the hormone pancreatic polypeptide
pancreatic hormone that stimulates the catabolism of glycogen to glucose, thereby increasing blood glucose levels
pancreatic hormone that enhances the cellular uptake and utilization of glucose, thereby decreasing blood glucose levels
