Atherosclerosis and Angina
Risk Factors and Epidemiology of Atherosclerosis
Tetiana Povshedna
Learning Objectives
By the end of this chapter, you will be able to
- Identify the main modifiable and non-modifiable risk factors for the development of atherosclerosis.
- Describe the key epidemiological trends in the global burden of cardiovascular disease.
- Explain the role of public health measures in decreasing the burden of atherosclerosis.
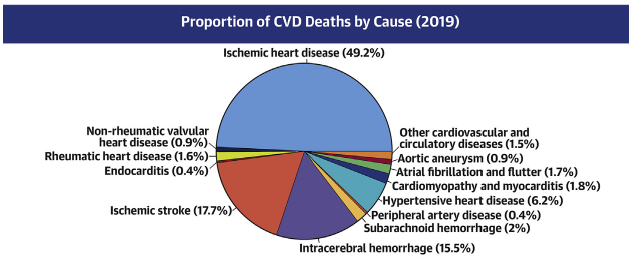
In 2019, cardiovascular disease accounted for 1/3 (17.9 million) deaths in the world, with the majority of them (85%) resulting from ischemic heart disease and stroke. These two acute types of cardiovascular disease are caused by occlusion of blood vessels in the heart/brain, which cuts off blood supply to these regions. The most common underlying reason of this blood flow restriction is atherosclerosis.
Atherosclerosis is a chronic inflammatory process that involves the accumulation of lipid particles within the vessel walls across the vascular tree (primarily heart, brain, lower limb), which results in acute atherosclerotic cardiovascular disease (ASCVD) events, such as heart attack and stroke.
Certain risk factors have been identified as associated with increased susceptibility to the development of atherosclerosis.
Generally, risk factors can be divided into 2 groups:
- Modifiable – the ones that can be changed/minimized by targeted interventions
- Non-modifiable – the ones that cannot be changed but should be accounted for when estimating the risk of ASCVD
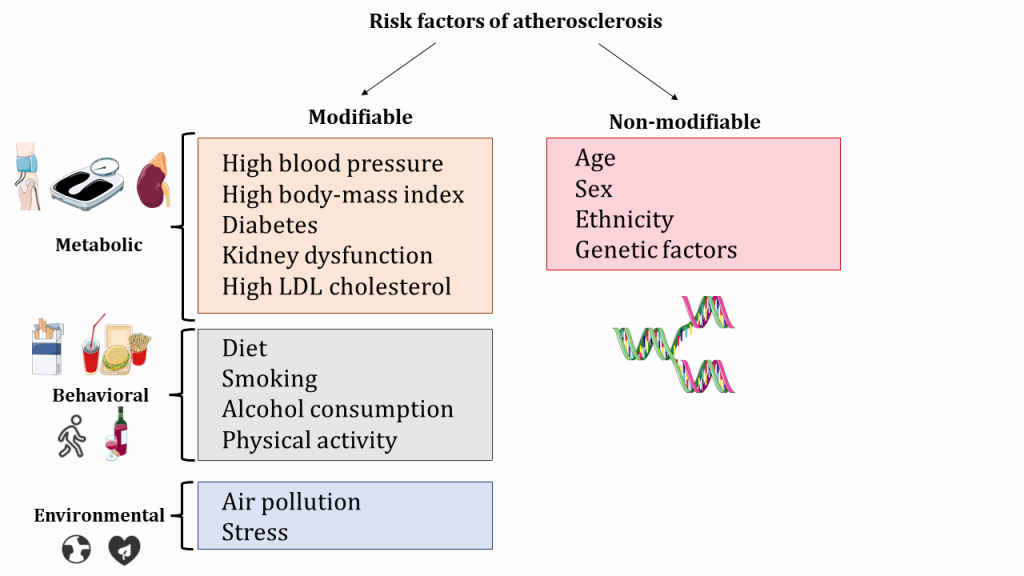
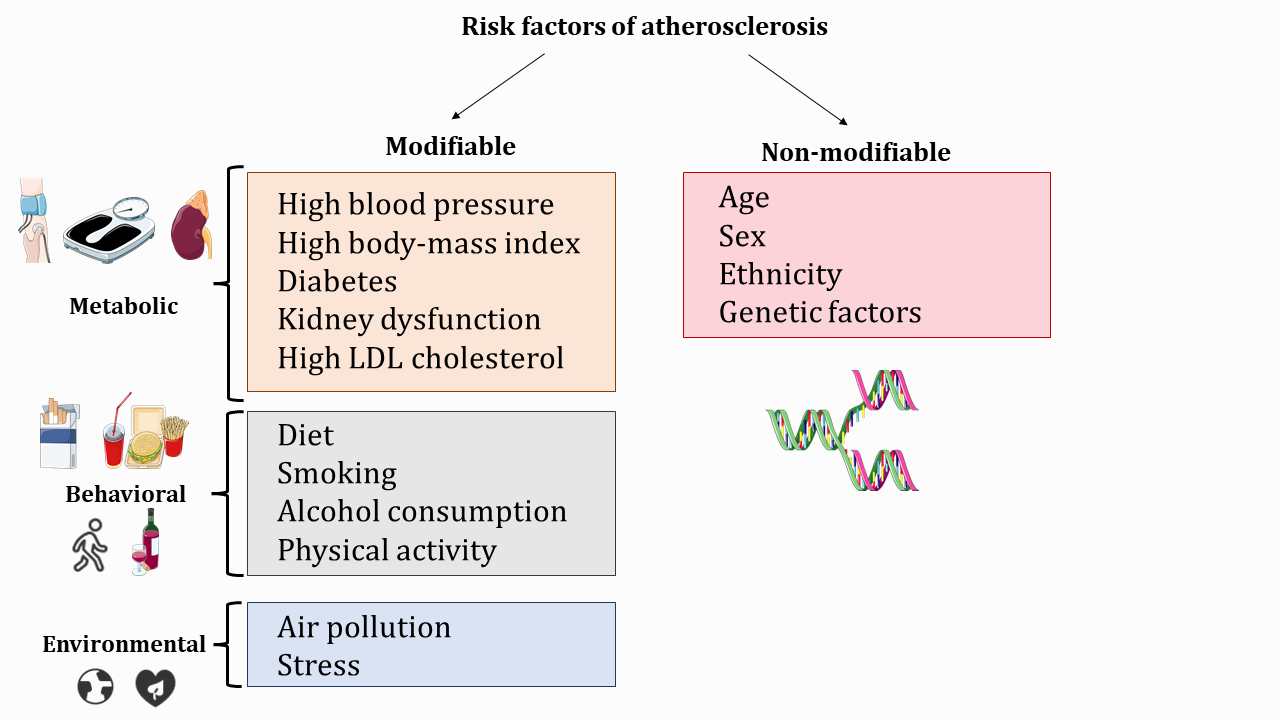
Non-modifiable factors include:
- Age – the risk of atherosclerosis naturally increases with age as the vascular tree is exposed to risk factors for a longer time;
- Sex– men and women experience ASCVD differently (before the age of 80, men are more likely to have a heart attack compared to women, but the trend reverses after 80 y.o.; at the same time, women are more likely to experience a stroke compared to men, even in younger age groups). This observation can be partially explained by different exposure of men vs women to some of the modifiable atherosclerosis risk factors (e.g. in some populations men are more likely to smoke, develop type 2 diabetes, and hypertension compared to women) or inherent differences between the sexes (hormones). However, a lot of cardiovascular events in younger women (15-20%) occur in the absence of known risk factors, which warrants future research.
- Ethnicity – some ethnicities experience a higher burden of type 2 diabetes and hypertension, which might affect increase their risk of ASCVD compared to the general population;
- Genetic factors – history of a cardiovascular event (heart attack/stroke in parents or siblings) increases individual risk of atherosclerosis and should be accounted for by healthcare providers
Perspective for future atherosclerosis research
Even though non-modifiable risk factors cannot be changed, they should be considered as independent variables in atherosclerosis research (data for men vs women, as well as different ethnicities, should be analyzed separately; this will allow for the identification of sex/ethnicity-specific trends or risk factors of atherosclerosis that, ultimately, can inform prevention and treatment strategies).
Epidemiological studies should represent the diversity of the global population, include young people, and account for socio-demographic factors (financial stability, employment status, mental health, stress levels)
Modifiable risk factors can be further divided into 3 groups:
- Metabolic
- High blood pressure
- High body-mass index
- Diabetes
- Kidney dysfunction
- High LDL cholesterol
2. Behavioural
- Diet
- Smoking
- Alcohol consumption
- Low physical activity
3. Environmental
- Air pollution
- Stress
All these factors can be addressed/changed by targeted health behaviour interventions, which will be discussed further in the “Prevention, diagnosis, and treatment of atherosclerosis” section of this chapter.
Stress and Metabolic Health
When trying to understand and identify factors that predict clinical outcomes, it is important to take a holistic look at health and consider not only biological (laboratory/clinical/genetic) variables, but also socio-demographic factors that affect health and aging. The rise in cardiovascular mortality despite advances in healthcare and treatment might reflect an increase in common metabolic disorders over the past 30 years. These include common risk factors for atherosclerosis – liver disease, obesity, and diabetes (a 24% increase in men and women combined). Multiple studies have shown that stress (including childhood adversity) has an adverse impact on metabolic health and can result in 1.1-1.4 times higher risk of obesity, diabetes, and liver disease, as well as accelerated progression of existing metabolic conditions. Factors examined in the studies include home and work-related stress as well as socioeconomic disadvantage, including in childhood.
Thus, not only individual but also governmental efforts (access to healthcare, social protection and support programs, and working conditions) are important for reducing the global burden of atherosclerosis and its consequences.
From: Kivimäki, M., Bartolomucci, A. & Kawachi, I. The multiple roles of life stress in metabolic disorders. Nat Rev Endocrinol (2022). https://doi.org/10.1038/s41574-022-00746-8
Section Review
Atherosclerosis, a leading cause of mortality globally, remains a concern despite advancements in research and treatment approaches. Currently, the majority of cardiovascular deaths occur in low/middle-income countries, which highlights the importance of effective primary and secondary prevention strategies, access to healthcare, education, and other social determinants of health. Multiple risk factors have been identified as associated with atherosclerosis. While modifiable factors (diet, smoking, physical activity, etc) can be changed by behavioural interventions, non-modifiable factors (sex, genetics, ethnicity) should be considered in research and treatment strategies.
References
- https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds)
- https://www.thelancet.com/journals/langlo/article/PIIS2214-109X(20)30117-0/fulltext#section-3d6acba1-acea-4be2-8dc9-b7e14e5b6583
- https://www.sciencedirect.com/science/article/pii/S0735109720377755?via%3Dihub
- https://www.mdpi.com/1422-0067/23/6/3346
- https://www.nature.com/articles/s41574-022-00746-8
Review Questions
1. Acute manifestations of atherosclerosis cannot be prevented.
- True
- False
2. Finish the following sentence. Modifiable risk factors of atherosclerosis include:
Select all that apply.
- Physical activity level
- Sex
- Ethnicity
- Body-mass index
3. Finish the following sentence. Non-modifiable risk factors of atherosclerosis include:
Select all that apply.
- Lipid metabolism parameters
- Diabetes
- Stress levels
- Genetic factors
- Sex
4. Fill in the blanks.
The most common acute outcomes of atherosclerosis are _____ attack and _____.
Answer Key
- False
- Physical activity level, body-mass index
- Genetic factors, sex
- Heart, stroke
Media Attributions
- Global burden of atherosclerosis © Gregory A. Roth is licensed under a CC BY (Attribution) license
- Risk factors of atherosclerosis © Tetiana Povshedna is licensed under a CC BY (Attribution) license
acute atherosclerotic cardiovascular disease
elevated blood pressure

{kind=link}