Emphysema
Pathophysiology of Emphysema
Jennifer Kong
Learning Objectives
At the end of this section, you will be able to:
- Outline the physiological cause of emphysema as a disease of repeated injury, inflammation and remodelling.
- Define the role of alpha-1-antitrypsin (AAT) in health and its role during the development of emphysema.
- Identify key features of emphysema in lung tissue on a gross and histological level.
- Explain how chronic inflammation and remodelling during emphysema leads to exhalation being an active process.
Causes of Emphysema
| Modifiable causes | Non-modifiable causes |
| Chronic inhalation of foreign particulate (e.g. air pollution, second hand smoke, working with fine dust or powders) | A rare, inheritable alpha-1-anti-trypsin deficiency |
| Chronic infection/inflammation of the lungs – especially in childhood |
Pathophysiology of Emphysema
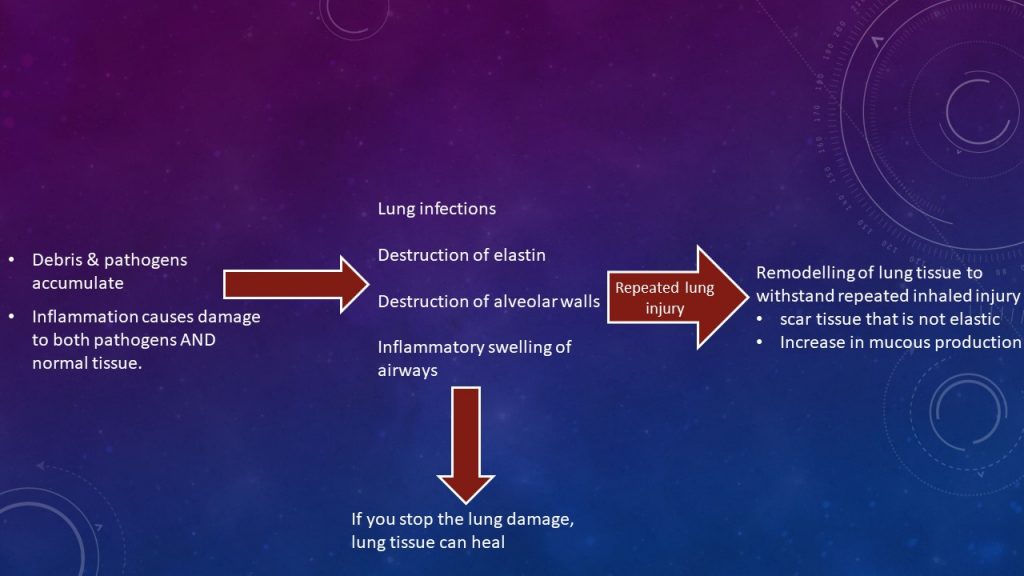
Regardless of the cause, emphysema is caused by repeated injury and inflammatory response in the lung tissue. As part of the inflammatory response, leukocytes – especially neutrophils – are recruited to the site of injury. Neutrophils release enzymes which degrade proteins in the irritant/pathogen. Such enzymes (i.e. proteases such as trypsin, elastase) can also degrade one’s own tissue’s proteins if it weren’t for the special protein alpha-1-antitrypsin (AAT) that deactivates any proteases approaching normal cells – akin to a protective forcefield. AAT is predominantly made in the liver, circulates continuously in the blood, and accumulates in lungs since lungs are exposed to pathogens (and hence, possible infection) with each breath.
But what happens if one frequently inhales harmful irritants? The acute inflammatory process works as needed, but the lungs run out of AAT. Rather, AAT is consumed by the frequent inflammatory response, faster than the liver can make it and circulate. As a result, the proteases released by neutrophils during inflammation will go uninhibited: digesting the proteins in both the irritant/pathogen AND the lungs. As a result, the lungs get damaged by its own cells – causing more of an inflammatory response and so forth. The result: loss of lung tissue and remodeling of airways to a non-elastic tissue (since proteases repeatedly digest the lung’s natural elastin). The loss of lung tissue particularly alveolar walls is noticed microscopically and by gross inspection in that the fine holes/bubbles in lung tissue are larger, distorted blebs as airspaces from digested alveoli coalesce to form a single larger air space. Similarly, alveoli & airways, particularly bronchioles, are remodeled due to chronic inflammation, becoming inelastic. This is particularly noticeable in the airways as the airways have narrowed and lost its ability to stay open during exhalation (i.e. airways collapse). At the same time, alveoli, with their larger than normal airspace, can’t recoil to a smaller volume during exhalation due to their remodeled inelastic nature. The end effect is that air is “trapped” inside lungs because the elastic-driving force of exhalation has been lost to remodeling.
Histopathology of Emphysema
Critical thinking Exercise
Before viewing histopathologist Jon’s video, consider what you already know about emphysema and what you would expect to see histologically. Privately record your answers to these questions before viewing the video
- In the histology chapter, you learned there are certain epithelial types you see within lung tissue. Which cell type would form the alveolar wall? The airways?
- What do you expect to see with respects to alveolar size, knowing there is destruction & remodeling?
- What do you think those enlarged airspaces, easily visible with the naked eye, will look like microscopically?
- What do you think the overall pattern of the emphysema tissue sample be? Will it be a predictable, homogeneous pattern?
- What do you think cigarette residue within lung tissue will look like microscopically?
- How would you observe the remodeling of lung tissue into inelastic connective tissue?
Histopathology of Emphysema by Jonathan Bush, licensed under All rights reserved
Section Review
- Due to chronic injury and/or insufficiency of alpha-1-antitrypsin in the lung, the inflammatory process destroys both the inhaled irritant AND normal healthy lung tissue. As a result, there is loss of lung tissue, particularly evident in alveolar walls, and remodeling of lung tissue to thicker, stiffer, less compliant properties.
- Because the lungs have lost their elasticity through remodeling, airways are narrowed and collapsible, especially during exhalation, resulting in an incomplete exhalation of the normal expiratory volume. The end result is some air being ‘trapped’ in the alveoli and thus lungs with each breath.
- Exhalation becomes progressively more difficult as the elastic recoil of healthy lung tissue is lost and the airways become narrowed and more likely to collapse. As a result, exhalation changes from a passive process to an active effort.
- Repeated inflammation causes loss of alveolar tissue. Thus causing expansion of alveolar air spaces with less area for gas exchange. These coalesced air spaces are visible histologically.
- Emphysema lung tissue may retain some of the inhaled irritants, thus changing the colour of lung tissue.
Review Questions
1. Fill in the blanks.During inflammatory processes, _____ are recruited to the site of injury/infection and begin releasing enzymes to degrade the irritants or pathogens. Alpha-1-antitrypsin is made in the _____ and circulates continuously in the _____, where it can accumulate in the lungs. Alpha-1-antitrypsin is responsible for deactivating _____ that are released by immune cells during inflammation. These enzymes can also degrade _____ lung tissue if they are unregulated.
2. Which of the following statements are true? Select all that apply.
- AAT is released from the liver after inflammation occurs, and is responsible for preventing damage to healthy tissue.
- Extensive tissue remodelling occurs in response to an acute inflammatory event, where inelastic scar tissue prevents proper functioning of the alveoli.
- AAT helps to regulate inflammatory-mediated damage to healthy lung tissue in acute events, but can run out in cases where there is frequent exposure to irritants or pathogens that cause an immune response.
- If the exposure to lung irritants stops, lung tissue is able to heal.
3. Describe some differences you can expect in the gross appearance of emphysema lung tissue versus healthy lung tissue.
4. List 3 ways in which breathing for a lung with emphysema will be more difficult than for a healthy lung. Recall the pathophysiology of emphysema, and relate that to the clinical picture.
Answer Key
- Leukocytes/neutrophils,liver, blood, proteases,normal/healthy
- AAT helps to regulate inflammatory-mediated damage to healthy lung tissue in acute events, but can run out in cases where there is frequent exposure to irritants or pathogens that cause an immune response.
- Example answer: Depending on the cause of emphysema, the lung tissue may have noticeable pigmentation (e.g. due to repeated smoke inhalation, cigarette tar). Some black spots are normal in lung due to everyday inhalation of pollutants, but the lung of a lifetime smoker with emphysema may appear nearly completely black. A lung with emphysema will have a “shaggy” appearance: there will be large holes where the walls between alveoli (air sacks) have been destroyed and the air spaces coalesced, and these large holes can be seen with the naked eye. There will also be noticeable thickening of the walls of the larger airways compared to healthy lung tissue.
- Example answer:
i) Due to tissue remodelling, the lungs lose elasticity which leads to narrowed and collapsible airways (having trouble staying open, particularly during exhalation). ii) The alveoli, which also become inelastic through tissue remodelling, are unable to recoil during exhalation which “traps” air inside of the lungs and causes incomplete exhalations.
iii) Many of the alveoli, which are responsible for the actual gas exchange in the lungs, have been destroyed and their air spaces have coalesced. This leaves less area for gas exchange to occur.
Media Attributions
- emphysema patho © Jennifer Kong is licensed under a CC BY (Attribution) license
A general term for an enzyme that the breaks down proteins into smaller polypeptides or amino acids.
A protease inhibitor that protects tissues from proteases released by inflammatory cells
