Neuromuscular Control of Motion
Pathophysiology of Neuromuscular Control: CNS Issues in White Matter (Multiple Sclerosis)
Mena Burr and Jennifer Kong
Learning Objectives
By the end of this section, you will be able to:
- Explain the pathophysiology and histopathology of MS.
- Correlate the signs and symptoms of MS with your understanding of the pathophysiology of MS.
- Describe the diagnosis of MS.
- Describe the treatment of MS.
Multiple Sclerosis (MS) is the most common non-trauma cause of nervous system related disability in young adults, with the typical age of diagnosis being between 20-40 years old. It is a disease of the central nervous system (CNS) in which the ability of neurons to transmit neural signals breaks down. As a result, the body cannot interpret and respond to environmental stimuli as effectively. Since MS can affect various parts of the CNS, it can have a wide variety of symptoms, ranging from motor, sensory, or cognitive deficits. Usually, patients initially experience unpredictable episodes of symptoms before progressing to more persistent and permanent states of disability.
Pathophysiology of MS
The pathophysiological hallmark of MS is the formation of demyelinating lesions in the central nervous system (an area with loss of myelin and relative preservation of axons). Since the role of myelin is to increase the speed of neuronal action potentials, the breakdown of myelin in MS results in slower or potentially absent signals. Some of the most commonly affected sites are the optic nerves (esp optic chiasm and tract), white matter serving the cortex (subcortical), areas around the ventricles of the brain (periventricular), and grey matter below the cortex (deep grey nuclei).
While the exact cause of MS is not completely understood, it is considered an immune mediated disease influenced by both genetic and environmental factors. It is thought that a breakdown of the blood brain barrier (BBB) occurs, which promotes the infiltration of reactive immune cells such as T cells, B cells, and myeloid cells into the CNS tissue. These immune cells produce antibodies that mark myelin as foreign, causing inflammation and the destruction of the myelin. This inflammatory component of MS likely may explain the on and off nature of symptoms that most patients initially experience (this type of MS is called relapsing-remitting MS).
Through the demyelination around axons, scarring and fibrosis also occurs. This is where the name of the disease comes from; sclerosis means hardening or scarring of tissue. Multiple scars are found in the white matter of the brain and spinal cord. Although new myelin may be formed in these lesions, this remyelination is often limited and variable between patients.
In addition to neuronal conduction, myelin also functions to protect and nourish axons. Thus, prolonged areas of demyelination can eventually lead axonal loss as well, causing irreversible clinical and cognitive deficits (this type of MS is called progressive MS). However, for unknown reasons, a small subset of patients experience a progressive style MS right from disease onset.
Histopathology of MS
MS lesions can be designated as active, inactive, or mixed active/inactive. This differentiation is based on the distribution of inflammatory cells around the plaque and the existence of demyelination. Histological and immunohistological stains can be used for identifying these lesions. For example, myelin can be seen with special stains (e.g. Luxol fast blue, Klüver-Barerra-Stains) while cell morphology can be seen with hematoxylin and eosin stains. Moreover, inflammatory cells such as macrophages can be seen with immunohistochemical markers (e.g. CD68). Thus, a combination of the pre-mentioned stains can help illuminate the loss of myelin in neurons caused by macrophages.
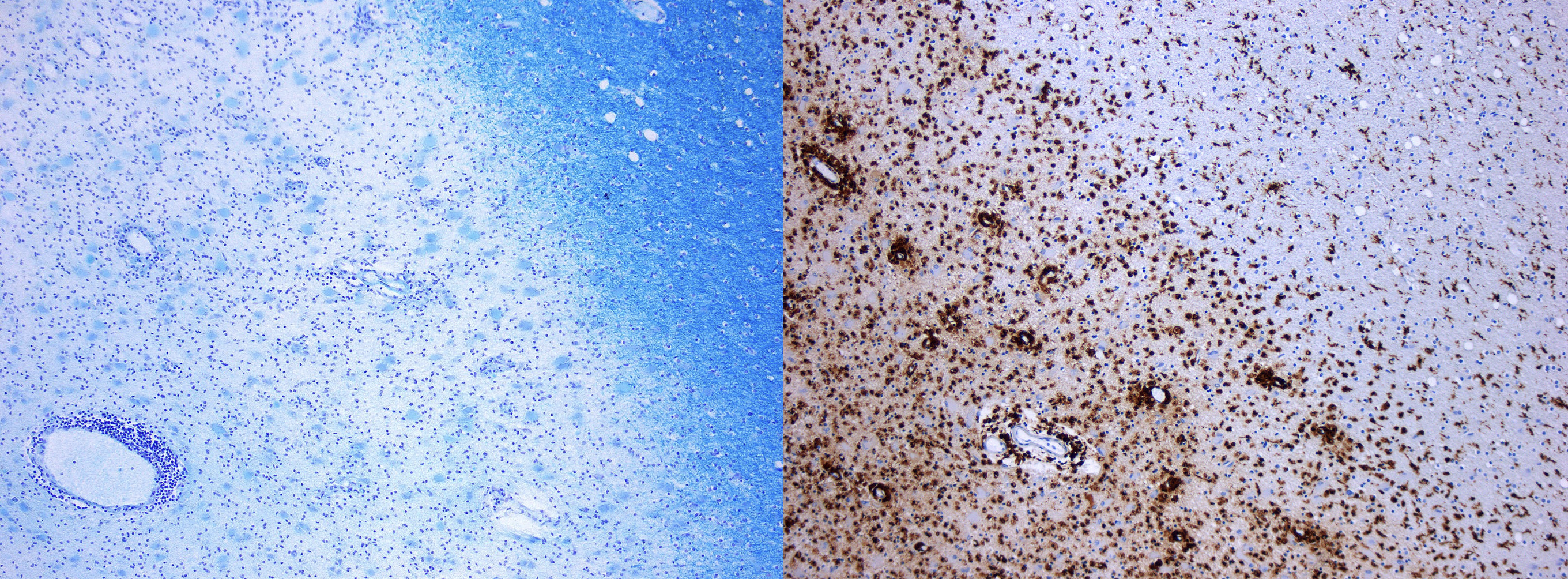
It should be noted that the presence of inflammatory cells within the plaques varies depending on the lesion’s stage. While active lesions tend to contain many macrophages, inactive/chronic lesions often contain few or none. Thus, stains such as CD68 may help determine lesion stage.
MS Pathology with Common Signs and Symptoms
Patients often have many complaints of problems with sensory and/or motor control long before an official diagnosis. Because demyelination can occur in any white matter in the CNS (i.e. brain and spinal cord), signs and symptoms can be separated from each geographically and temporally. For example, a patient may have issues with vision of right eye (sensory) and then problems with controlling the left foot (motor) two months later. Below is a table of some common signs and symptoms reported in MS. Please note that this is not an exhaustive list.
| Area of demyelination | Sign or Symptom |
| the optic nerve (cranial nerve II) | blurry vision or partial or complete loss of vision in one eye |
| white matter serving the cerebral cortex | depression, mood disturbances, fatigue, and cognitive deficits such as slowed thinking |
| spinal cord | Sensory: unusual sensations like tingling or numbness, often on one side of the body
Motor: numbness, movement issues like loss of balance and/or coordination. Autonomic functions: bladder or bowel impairments and sexual dysfunction |
| brainstem, cerebellum, and cranial nerves | Sensory: unusual sensation affecting the face, vertigo
Motor: weakness of facial muscles, difficulty swallowing, slurred speech |
| oculomotor nerve (cranial nerve III) | sensory: prolonged double vision
motor: non-consensual eye movements, |
Signs and symptoms of MS and location of demyelination
Diagnosis of MS
The diagnosis of MS is largely based on the signs and symptoms. Moreover, it is also required that there be multiple lesions that vary in time and space, and to exclude other conditions with similar symptoms. In other words, the lesions must be in various stages and various locations within the CNS. This can be determined using tests such as magnetic resonance imaging (MRI) of the brain and spinal cord, cerebral spinal fluid (CSF) analysis, or measuring electricity flowing in nerves (evoked potentials).
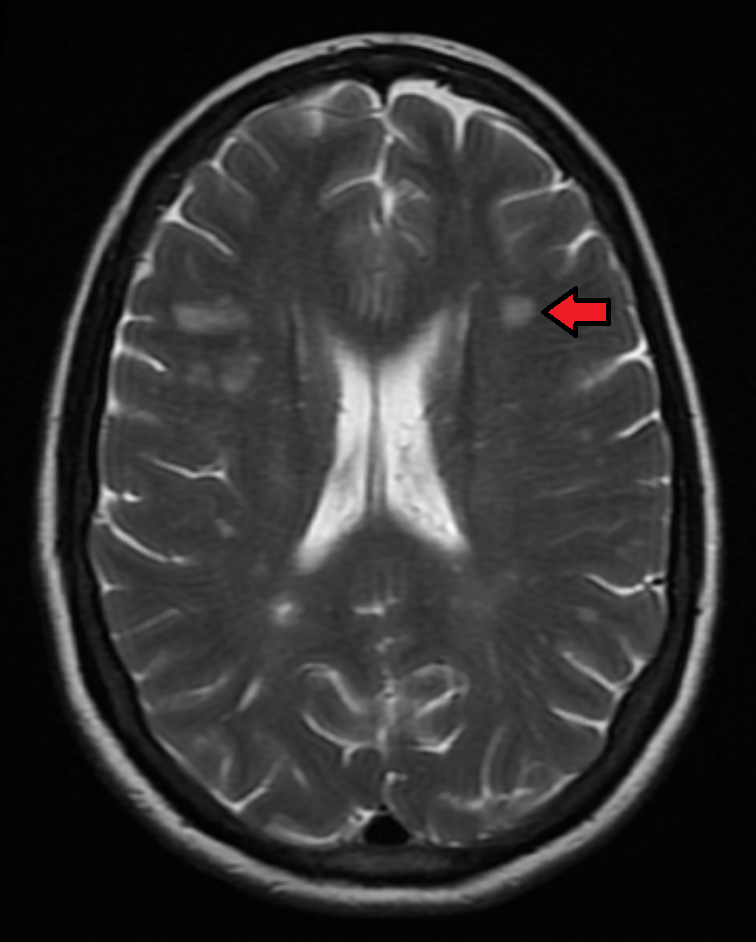
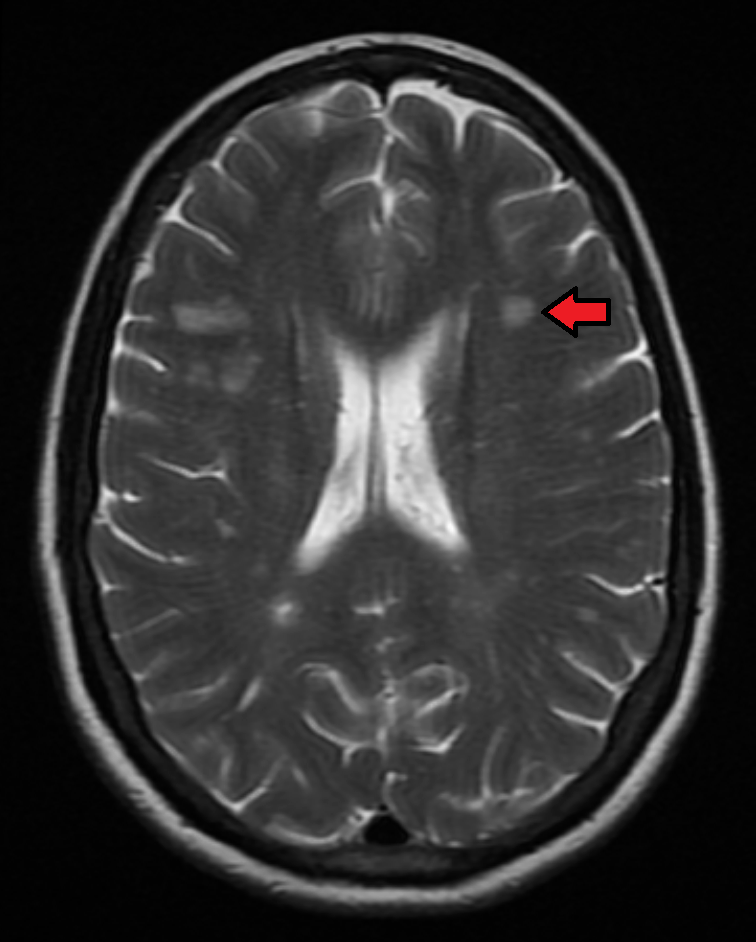
MRI of CNS
Through MRI, a contrast agent called gadolinium is used to highlight lesions with active demyelination. The McDonald criteria is the most commonly used criteria to diagnose MS, combining both clinical assessment of symptoms and the additional tests mentioned. In order to diagnose MS using this criteria, a patient must have a least one symptomatic episode, as well as an MRI scan showing lesions at various stages and locations in the CNS.
CSF Analysis
Cerebral spinal fluid is collected by an invasive procedure known as lumbar puncture. Because CSF circulates around both the brain and spinal cord, this CSF sample can show the presence of antibodies, which are abnormally present during MS.
Evoked Potential Tests
Evoked potential tests measure the electricity of the nervous system upon a stimulus (visual or electrical). While being stimulated (e.g. watching a visual pattern or by electrical stimulation via electrodes), electrical impulses are applied to the affected limbs and electrodes measure the speed the electricity travels down the nerves.
Treatment of MS
There is no cure for multiple sclerosis. Some people have mild symptoms where no treatment is necessary and others have flare ups with periods of remission. However, when MS affects health and activities of daily living, treatment focuses on reducing the inflammatory and circulating antibodies associated with MS.
Corticosteroids are prescribed to reduce inflammation, particularly the inflammatory process which is attacking the myelin.
Plasma exchange (plasmapheresis) occurs when MS has a bout of new, severe symptoms which don’t respond to corticosteroids. Plasmapheresis involves separating whole blood into blood cells (e.g. red and white blood cells) and the watery plasma where antibodies are found. After antibody removal, the plasma is mixed back with the blood cells and put back into circulation.
Monoclonal antibodies are synthetic antibodies made to directly interfere with the B cells to prevent their formation of the offending antibodies that cause demyelination.
Review Questions
References
Huang WJ, Chen WW, Zhang X. Multiple sclerosis: Pathology, diagnosis and treatments. Exp Ther Med. 2017 Jun;13(6):3163-3166. doi: 10.3892/etm.2017.4410. Epub 2017 Apr 28. PMID: 28588671; PMCID: PMC5450788.
https://www.mayoclinic.org/diseases-conditions/multiple-sclerosis/diagnosis-treatment/drc-20350274
Media Attributions
- MS histo © Marvin 101 is licensed under a CC BY-SA (Attribution ShareAlike) license
- MS MRI © James Heilmen is licensed under a CC BY-SA (Attribution ShareAlike) license

{kind=link}
{kind=link}