Atherosclerosis and Angina
Prevention, Diagnosis and Treatment of Atherosclerosis
Tetiana Povshedna
Learning Objectives
By the end of this chapter you will be able to:
- Describe the actions toward primary and secondary prevention of atherosclerosis.
- Describe the common diagnosis and treatment strategies of atherosclerosis.
- Describe the role of interprofessional health teams in diagnosis and management of atherosclerosis.
Prevention efforts to minimize the global health impacts of atherosclerosis include primary and secondary prevention.
Secondary prevention includes actions to facilitate early diagnosis of existing diseases and prevent further disease progression/manifestations (lipid-lowering medication, anti-hypertensive medication, diagnostic tests to assess heart function)
It is important to recognize that atherosclerosis initiation can occur early in life, and the disease can be asymptomatic for decades before progressing and manifesting as an acute cardiovascular event.
This is why the prevention of atherosclerosis is a lifelong effort.
Primary Prevention
Primary prevention strategies involve lifestyle considerations that aim to minimize the impact of modifiable risk factors. It is especially important to minimize the effect of these factors in childhood and adolescence because higher cumulative exposure to risk factors (e.g. decades of adherence to a high-fat diet, smoking, and sedentary lifestyle) can result in a higher incidence of ASCVD later in life. Therefore, the ideal primary prevention of atherosclerosis would involve adherence of a healthy lifestyle since childhood. Still, health behavior modifications for the prevention of atherosclerosis provide benefits regardless of age and atherosclerosis stage.
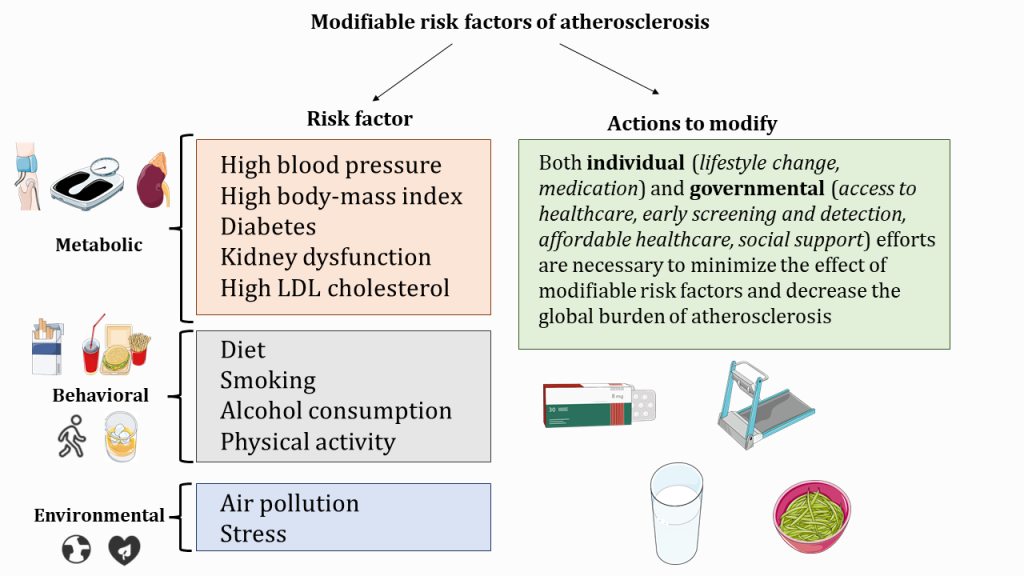
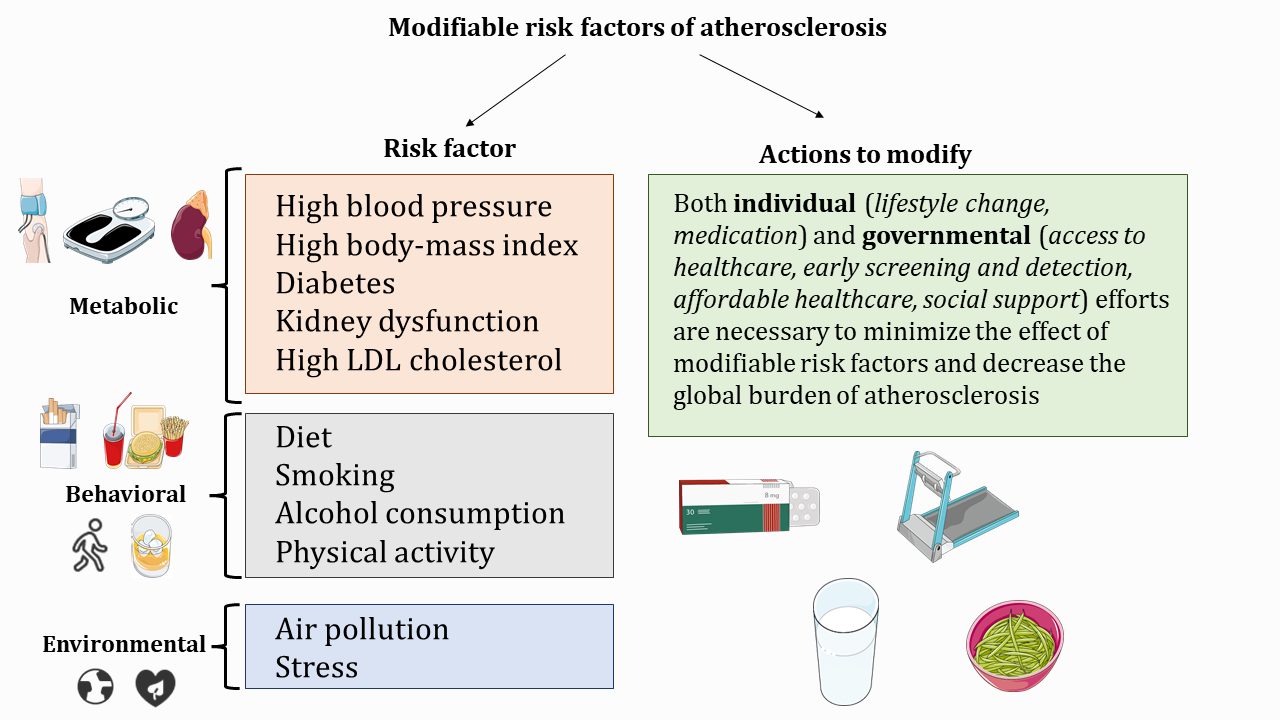
It’s important to recognize that modifiable risk factors, even though distinct, often co-exist and can exacerbate each other. On the other hand, certain lifestyle changes can affect multiple modifiable risk factors, “breaking down” the vicious circle of metabolic imbalance and atherosclerosis risk.
The interplay between modifiable risk factors in the context of atherosclerosis
Various modifiable risk factors can potentiate each other and thus increase the total risk of atherosclerosis progression and ASCVD.
Similarly, lifestyle and medical interventions towards one of the risk factors can modify and weaken the effect of other factors.
For example:
- Low rates of physical activity and poor diet are major behavioural risk factors that lead to caloric imbalance, higher rates of obesity, and type 2 diabetes (metabolic risk factors)
- Levels of LDL and HDL in the blood (metabolic risk factors) are affected by physical activity, diet, smoking (behavioural interventions), and body-mass index (metabolic risk factor)
- High body-mass index (metabolic risk factor) affects blood pressure, glucose metabolism, systemic inflammation, and cardiac structure and function (metabolic risk factors)
- Kidney function (metabolic risk factor) can be affected by hypertension and diabetes (metabolic risk factor)
Thus, a complex approach to modifiable risk factors, which includes recognition of their interplay, is necessary for effective primary prevention of atherosclerosis that, ideally, would address multiple modifiable risk factors.
In practice, primary prevention can include both individual efforts (lifestyle considerations regardless of age), and treatment strategies addressing modifiable risk factors.
The decision about prevention efforts is usually based on the risk assessment – a holistic assessment of a patient in the context of atherosclerosis. The image below, which includes laboratory tests, physical examination, and medical/family history collection.
Healthcare professionals can also utilize risk calculators – clinical tools that integrate most of the known risk factors for atherosclerosis and can help guide clinical decision-making by providing estimates of 10-year risk of heart attack or other ASCVD outcomes.
Based on the risk assessment, patients are stratified as low, intermediate, or high risk in the context of primary prevention of atherosclerosis.
Primary atherosclerosis prevention: key recommendations from the Canadian Cardiovascular Society
- For those at low risk: medications generally not recommended; focus on health behaviour modifications (smoking cessation, diet, exercise)
- For those at intermediate and high risk: health behaviour modifications + lipid-lowering medication (details might vary for different risk groups)
Summary of recommended health behaviour modifications:
- Diet: Mediterranean dietary pattern, Portfolio dietary pattern, Dietary Approaches to Stop Hypertension (DASH) dietary pattern, plant-based dietary pattern, dietary patters high in nuts, legumes, olive oil, fruits, vegetables, total fibre, and whole grains
- Exercise: at least 150 minutes of vigorous aerobic activity per week + muscle- and bone-strengthening activities at least 2 days per week
Diagnosis and Secondary Prevention
Secondary prevention efforts involve interprofessional health teams that work together to optimally manage patients with existing atherosclerosis with or without history of cardiovascular events (heart attack, stroke, etc) to prevent further disease progression and exacerbation.
Please note: Some healthcare systems (including British Columbia) classify disease prevention as primary, secondary, and tertiary. In this case, primary prevention refers to efforts towards preventing the occurrence of the disease, secondary – efforts towards early diagnosis, and tertiary – efforts towards improvement of quality of life and reduction of symptoms in those with a diagnosed condition.
Learn more: https://www.healthlinkbc.ca/healthy-eating-physical-activity/conditions/physical-activity-and-disease-prevention
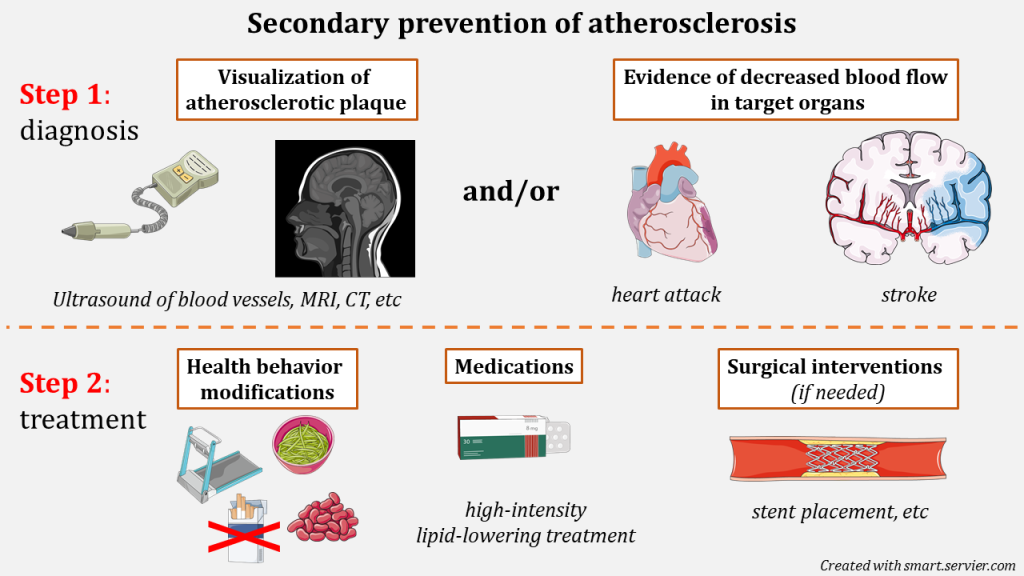
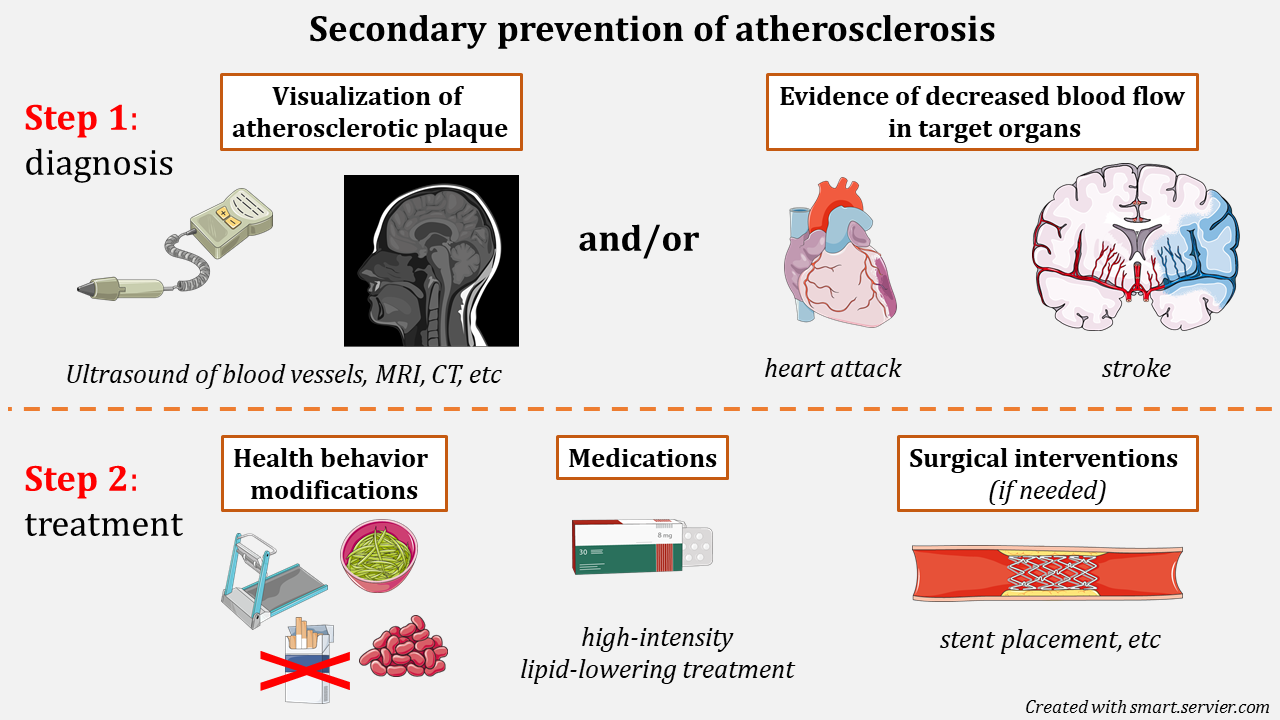
Diagnosis of atherosclerosis generally involves:
- direct visualization of atherosclerotic plaques ( via ultrasound, computer tomography, or other imaging techniques)
- definitive evidence of ischemia in target organs ( evidence of heart muscle damage as a result of heart attack, etc)
As a general approach, patients with diagnosed atherosclerosis benefit from health behaviour modifications and high-intensity lipid-lowering therapy.
However, the location and characteristics of atherosclerotic plaque may warrant additional medical treatments/surgical interventions.
Overall, prevention of atherosclerosis is a complex task that involves both behavioural and societal changes.
Role of Interprofessional Health Teams in the Prevention and Treatment of Atherosclerosis
Listen to Andrea Glew, a cardiac sciences technologist, as she discusses the experiences of patients who obtain an EKG or a stress test.
Role of EKG and Stress Tests During Prevention and Treatment of Atherosclerosis by Andrea Glew, licensed under All Rights Reserved
Key Takeaways
EKG is a routine painless procedure that records electric impulses of the heart and provides information about heart blood supply and function. EKG can detect changes that occur as a result of reduced blood flow and heart damage – common symptoms of atherosclerosis. EKGs are often administered by cardiac technologists at the emergency departments where patients can present with signs and symptoms consistent with a heart attack. The EKG findings are then transferred to the physician/nurse for further assessment and decision-making.
The stress test is used to detect atherosclerosis outside of the emergency setting. The patient is connected to a cardiac monitor and is asked to walk on a treadmill. Certain changes detected by a heart monitor can occur as a result of increased heart rate and blood pressure, suggesting decreased blood flow to the heart. Often these changes can be missed by EKG administered at rest. A stress test can also help determine the degree of blood flow reduction/severity of atherosclerosis.
Section Review
While primary prevention of atherosclerosis focuses on changing/addressing modifiable risk factors (smoking, diet, exercise level, etc) to defer the onset of the disease, secondary prevention aims to delay the progression of diagnosed atherosclerosis. Secondary prevention methods include health behavior modifications (same as in primary prevention) and lipid-lowering medications (the dosage depends on the severity of atherosclerosis). Some advanced cases of atherosclerosis might require surgical interventions to renew the blood flow in obstructed vessels. Atherosclerosis diagnosis and management efforts involve interprofessional health teams that work together to design and help facilitate optimal prevention/treatment plans for each case of this lifelong condition.
Resources
https://www.onlinecjc.ca/article/S0828-282X(21)00165-3/fulltext
https://www.nature.com/articles/s41572-019-0106-z
Review Questions
Select all that apply.
- Dietary considerations
- Exercise considerations
- Smoking cessation
- Genetic testing
2. Secondary prevention involves actions aimed to treat patients with diagnosed atherosclerosis to minimize it’s future health impact.
- True
- False
3. Finish the following sentence. The most commonly used type of medications used in atherosclerosis prevention are:
- Lipid-lowering
- Glucose-lowering
- Anti-hypertensive
- Anti-inflammatory
4. Fill in the blank.
_____ is a routine procedure that helps assess heart function by recording its electric impulses.
5. Health behaviour modifications are the cornerstone of both primary and secondary atherosclerosis prevention strategies.
- True
- False
Answer Key
- Dietary considerations, exercise considerations, smoking cessation
- True
- Lipid-lowering
- EKG/ECG
- True
Media Attributions
- Modifiable risk factors of atherosclerosis © Tetiana Povshedna is licensed under a CC BY-NC (Attribution NonCommercial) license
- Secondary prevention © Tetiana Povshedna is licensed under a CC BY-NC (Attribution NonCommercial) license
acute atherosclerotic cardiovascular disease
insufficient blood flow to the tissues

{kind=link}
{kind=link}