Autoimmunity
Celiac Disease
Celiac Disease
Dylan Mann and Morgan Alford
Learning Objectives
By the end of this section, you will be able to:
- Define Celiac disease.
- Describe autoimmune processes underlying Celiac disease.
- Explain how genetic and environmental factors impact on the pathogenesis of Celiac disease.
- Distinguish between Celiac disease and other autoimmune diseases of the gut.
Introduction
Celiac disease is a common autoimmune condition, affecting approximately 1 in 100 people worldwide. It is characterized by an autoimmune response triggered by consumption of gluten, a protein that is in food products containing wheat, barley, and rye.
Mechanism
Gluten is one of the few chronically consumed proteins that is digested incompletely. Gliadin, a metabolic byproduct of gluten digestion, is bound by secretory IgAin the small intestine. Under normal conditions, IgA protects gut epithelial cells from pathogens by marking the pathogens for destruction by the immune system. However, in the case of celiac disease, IgA facilitates the transport of gliadin into the lamina propria . There, gliadin is deaminated by tissue transglutaminase (ttg). Then, deaminated gliadin is phagocytosed by intestinal macrophages, broken down into small peptides and presented on MHC II. When presented on MHC II, helper T cells(CD4+ T cells) can bind and be activated by deaminated gliadin epitopes, resulting in the production of inflammatory cytokines. The resulting inflammation can damage the epithelium of the small intestine. Simultaneously, B cells may be stimulated to produce anti-gliadin IgA and anti-endomysial IgA, or endomysial antibodies (EMAs), which can interfere with the activity of transglutaminase. The cytokines produced by helper (CD4+) T cells can also recruit cytotoxic (CD8+) T cells , which can worsen epithelial cell damage. As epithelium is destroyed, it becomes possible for more gliadin to enter the lamina propria, propagating the autoimmune process.
Genetic Predisposition and the Environment
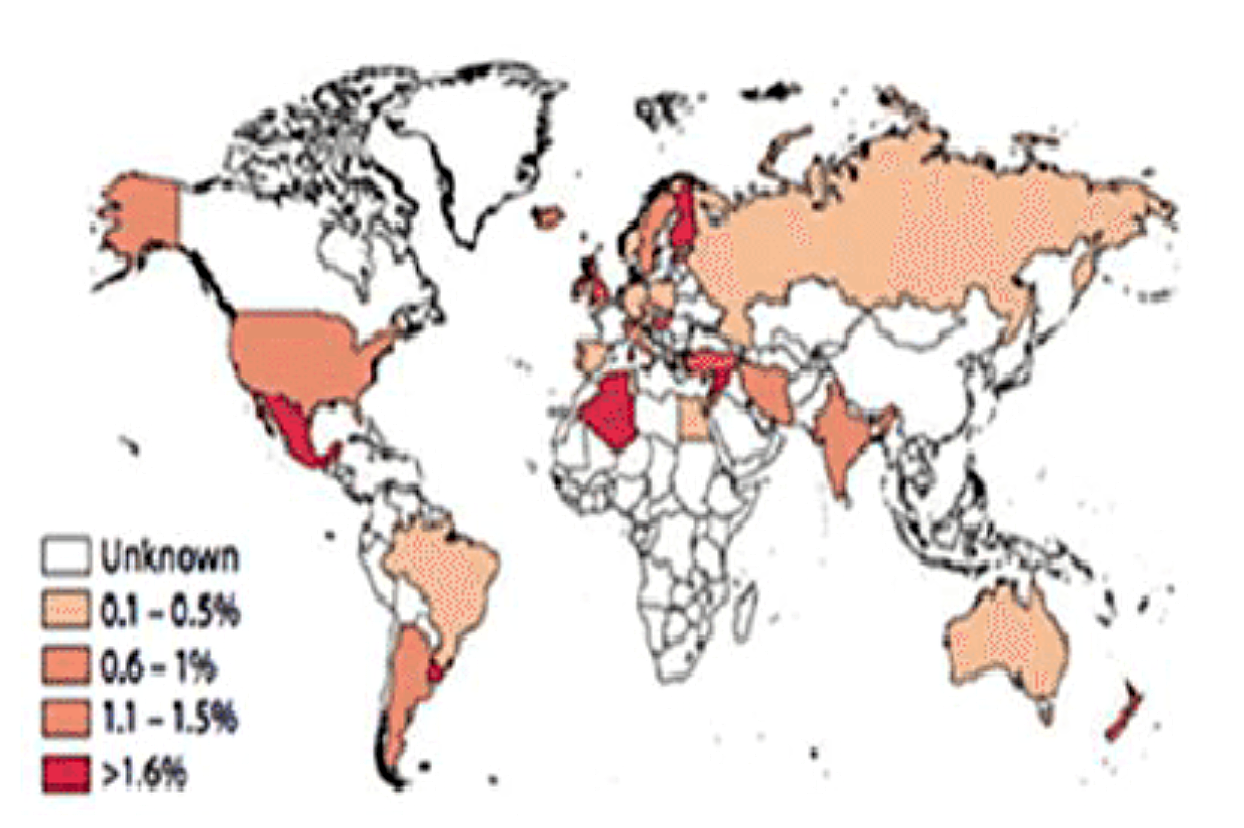
Although Celiac disease, like most autoimmune diseases, is influenced by environmental factors there are genes that are associated with the condition. For example, certain alleles of the human leukocyte antigen (HLA) gene, which encodes MHC proteins, are common in patients with celiac disease. More specifically, HLA-DQ2 and HLA-DQ8 are risk factors for celiac disease. Interestingly, the extent to which other genes are expressed can influence celiac pathology. For example, the receptor TFR, which is necessary for transporting gliadin complexes across the intestinal epithelium, is overexpressed in people with celiac disease. Numerous environmental factors influence celiac pathology as well, as demonstrated by uneven geographic distribution of the disease, which implies that different lifestyles and climates may impact manifestation. For example, the hygiene hypothesis proposes that decreased exposure to bacterial antigens as an infant may trigger future autoimmunity. In the case of celiacs, the prevalence of H. pylori is found to be significantly less than the rest of the population. Current data implies that Celiac disease is most prevalent in Europe and Oceania, and least prevalent in South America. While the unequal distribution of celiac disease of ongoing debate, it may be caused by any combination of weather, bacterial populations, hygiene standards, and diet.
Diagnoses
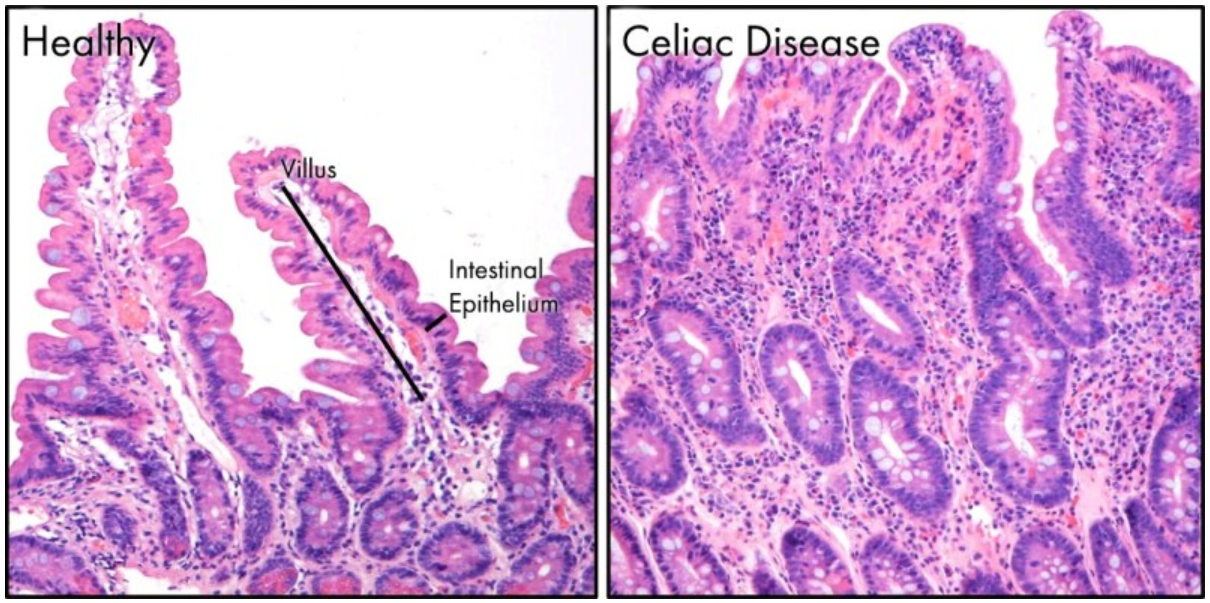
A non-invasive way to screen for Celiac disease is to perform serology to determine titres of anti-gliadin IgA and EMA. However, because anti-gliadin IgA is not uniformly expressed in celiacs or non-celiacs, this test lacks specificity. It can be used as a tool to suggest Celiac disease prevalence or rule out other autoimmune diseases. A definitive diagnosis can be made following biopsy of the duodenum; the first part of the small intestine. A biopsy of a person with celiac disease would show a damaged duodenum, with destroyed villi, and abnormally long crypts.
Symptoms and Treatment
Review Questions
Media Attributions
- World Prevalence of Celiac Disease © Mohammadi et al. is licensed under a CC BY (Attribution) license
- healthy vs celiac villi © Sharon F. Daley; Muhammad Haseeb. is licensed under a CC BY-NC-ND (Attribution NonCommercial NoDerivatives) license
inappropriate immune response to host cells or self-antigens
antibody crucial for mucosal immunity
The layer of cells that covers all internal and external surfaces of the body
Connective tissue found under the thin layer of surface epithelium covering a mucous membrane
large phagocytic cell that engulfs foreign particles and pathogens
protein found on the surface of antigen-presenting cells that signals to immune cells whether the cell is healthy/normal or is infected/cancerous; it provides the appropriate template into which antigens can be loaded for recognition by lymphocytes
cell of the adaptive immune system that binds APCs via MHC II molecules and stimulates B cells or secretes cytokines to initiate the immune response
small proteins released by cells; allow for communication between the cells involved in the same type of immune response/reaction
lymphocytes that mature in the bone marrow and differentiate into antibody-secreting plasma cells
adaptive immune cell that directly kills infected cells via perforin and granzymes, and releases cytokines to enhance the immune response
genes part of the major histocompatibility complex
Gram-negative, flagellated, helical bacterium that may cause stomach infection
Scientific examination or study of blood serum
Eextraction of sample cells or tissues for examination to determine the presence or extent of a disease. The tissue is examined under a microscope by a pathologist for histological changes
